Embed Size (px)
Citation preview
HIV Prevention 2.0
Charles Boucher MD. PhD

Prevention
A variety of methods exists to preventtransmission of HIVCircumcisionCondomsPost-exposure profylaxe (PEP)Treatment as preventionPre-exposure profylaxe (PREP)etc
Stop the HIV pandemic
Great enthiusiasm for decreasing thenumber of new HIV infections :Global goal UNAIDS: no new HIV infectionsthrough combining prevention approaches by2030 A big challenge !
Costs Prevention is not cheap Limited resources Are policy makers prepared to invest? PrEP cost effective when used by MSM with a high risk for infection (Nichols et al Lancet Infect Dis 2016, J Acquir Imm Def Syndr 2014)

Cost effective
Identify targeted strategies for different risk populations prevent a maxinum number of new infections at lowest costs

Sexual networks
https://www.k4health.org/sites/default/files/Poster%201_0.jpg
Prevention
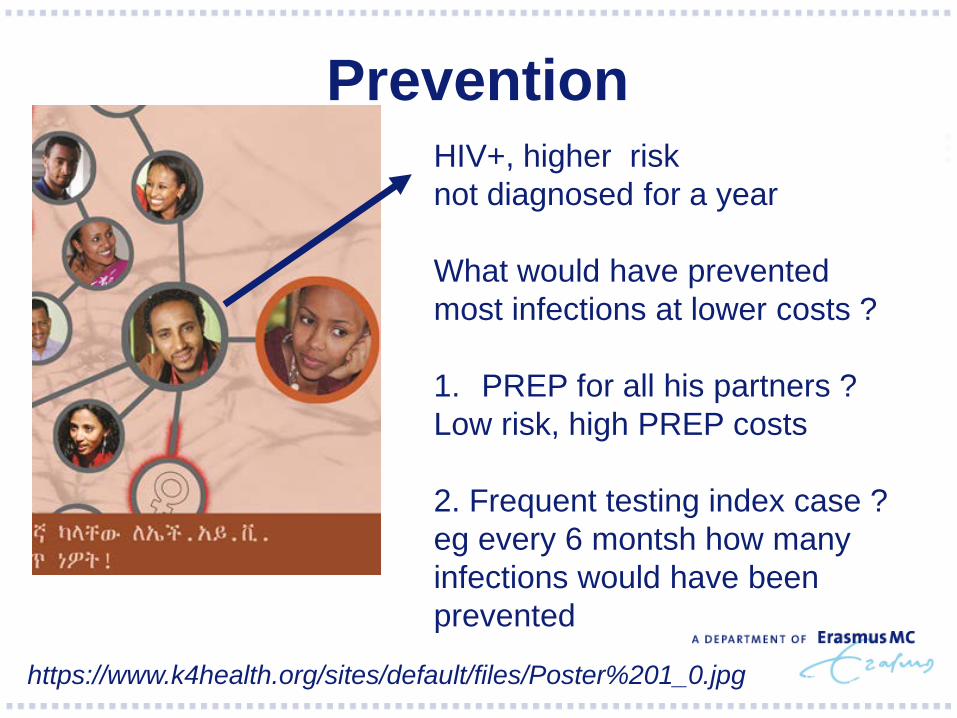
https://www.k4health.org/sites/default/files/Poster%201_0.jpg
HIV+, higher risk not diagnosed for a year
What would have preventedmost infections at lower costs ?
1. PREP for all his partners ?Low risk, high PREP costs
2. Frequent testing index case ? eg every 6 montsh how manyinfections would have been prevented
Virological networks
When Individual A infects individual B theyhave intially an identical virus Virological : genetic distance of 0
Over time through evolution in both hoststhe viruses start to differentiate Analysis of sequences (resistance
genotyping)

Fylogenetics: HIV tree
Brenner et al. J Infect Dis 2007; 195: 951-9

Recent publications Proposed to use (real time) fylogenetic
analysis to understand the epidemic and torecommend specific interventions
Challenges fylogenetics
1. Reconstruction transmission network?Resik et al. AIDS hum retrovir 2007
2. Dense sampling required

Sexual networks
https://www.k4health.org/sites/default/files/Poster%201_0.jpg

Challenges fylogenitics1. Reconstruction transmission network?Resik et al. AIDS hum retrovir 2007
2. Dense sampling required Netherlands: 23% 2012

Challenges fylogenitics1. Reconstruction transmission network?Resik et al. AIDS hum retrovir 2007
2. Dense sampling required3. Timing of samples (ideally all recent
infections)
1. Sources of hiv infection among msm andimplication for prevention
2. Reconstruction transmission events network.
3. Dutch cohort 11863 msm, 1794 12 monthsinfected
4. Identified the source for 617 recent infections (1996-2010) by fylogeneticanalysis of chronic infections
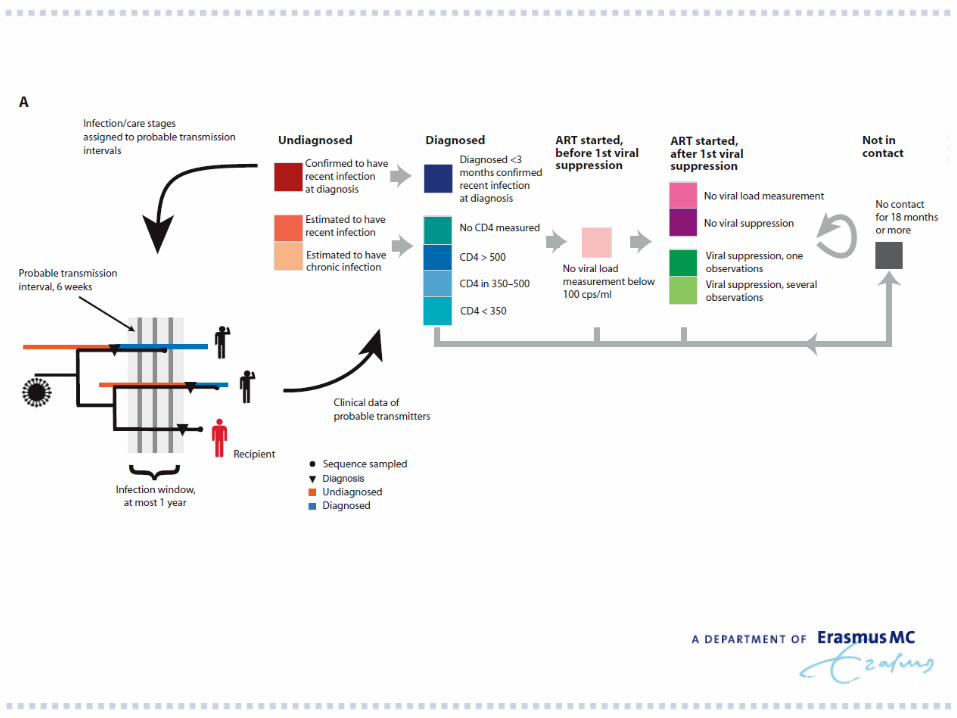

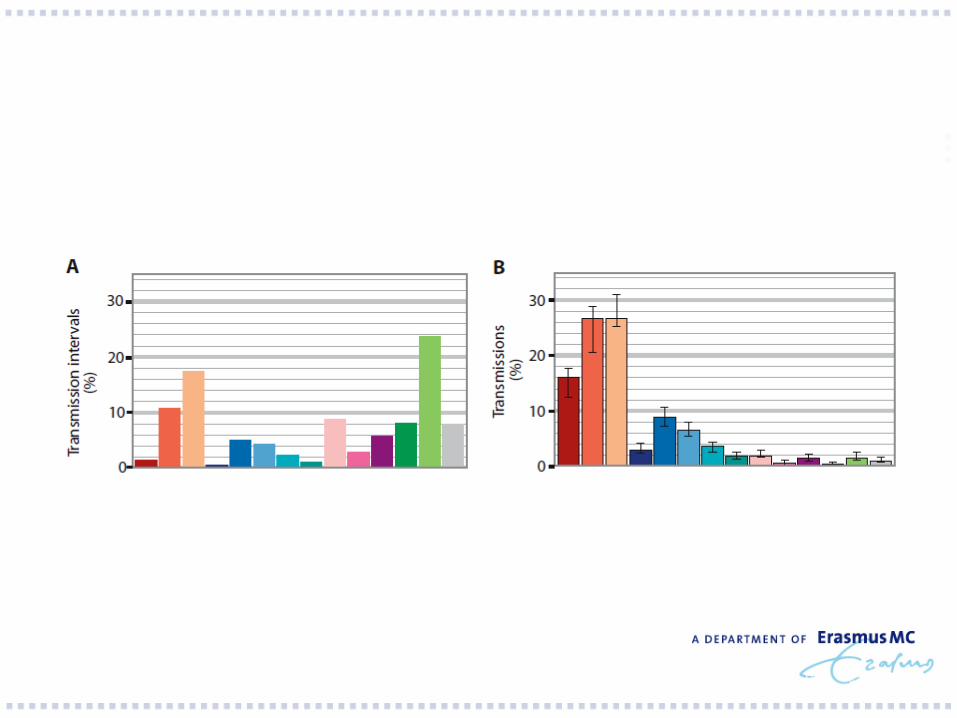
Sources for transmission
1. 71% from undiagnosed men2. 43% from men in first year of infection3. 6% from men started therapy4. 1% lost to follow up>18 months
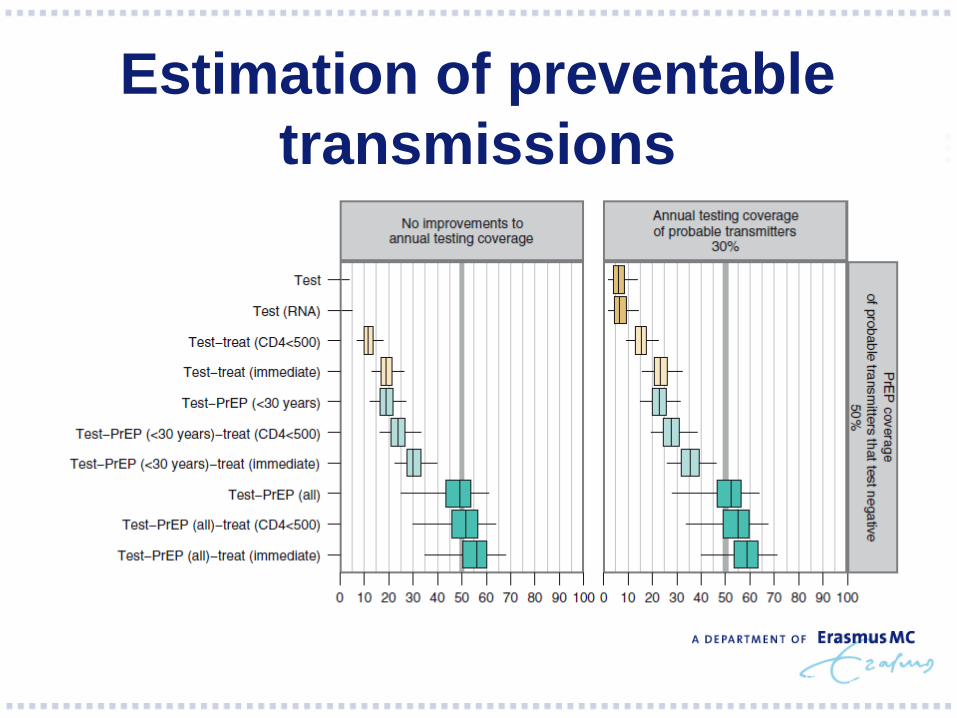
Estimation of preventable transmissions
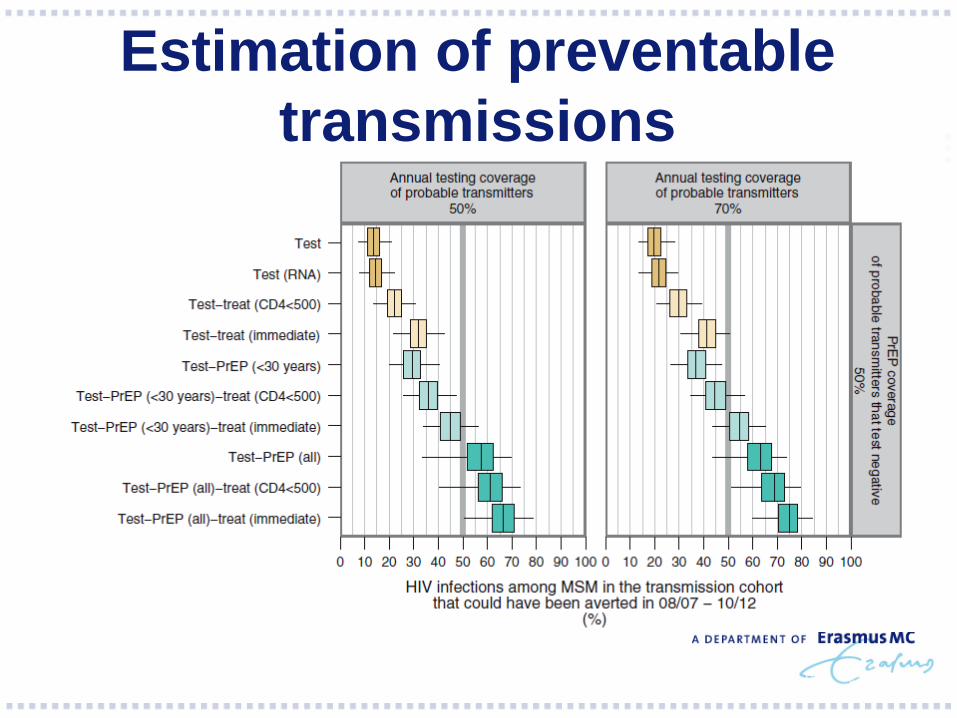
Estimation of preventable transmissions
Conclusions
1. Lack of substantial reductions is not due toineffective ART provision or inadequate retention
2. Rather due to frequent early transmission and continued low testing rate of men at risk of transmission
3. Increased annual testing and uptake of PREP in high risk MSM key role.


Dynamics french acute infections
1. 1999-2014 2. 1536 patients with primary infection3. Clinical, virological, geographical info 4. Objective: to characterise transmission
networks
Dynamics french acute infections
1. 86% Caucasian men (71% MSM)2. 983 (73% subtype B ) 209 CRF02-AG 3. 387 in clusterd: 156 dyads, 231 larger
clusters4. Genotype of reverse transcriptase
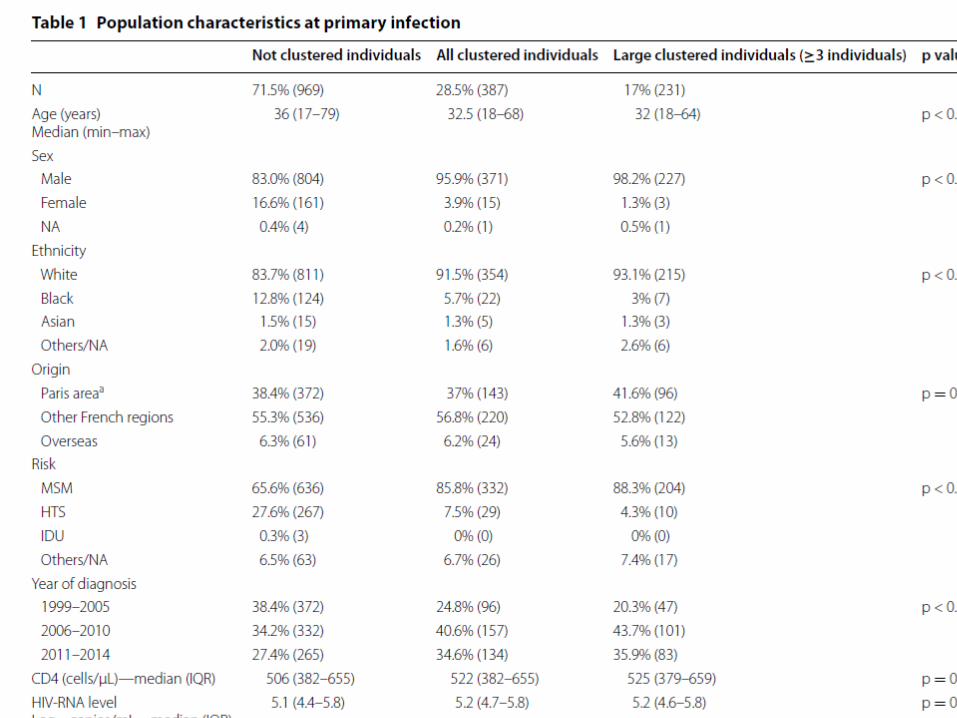
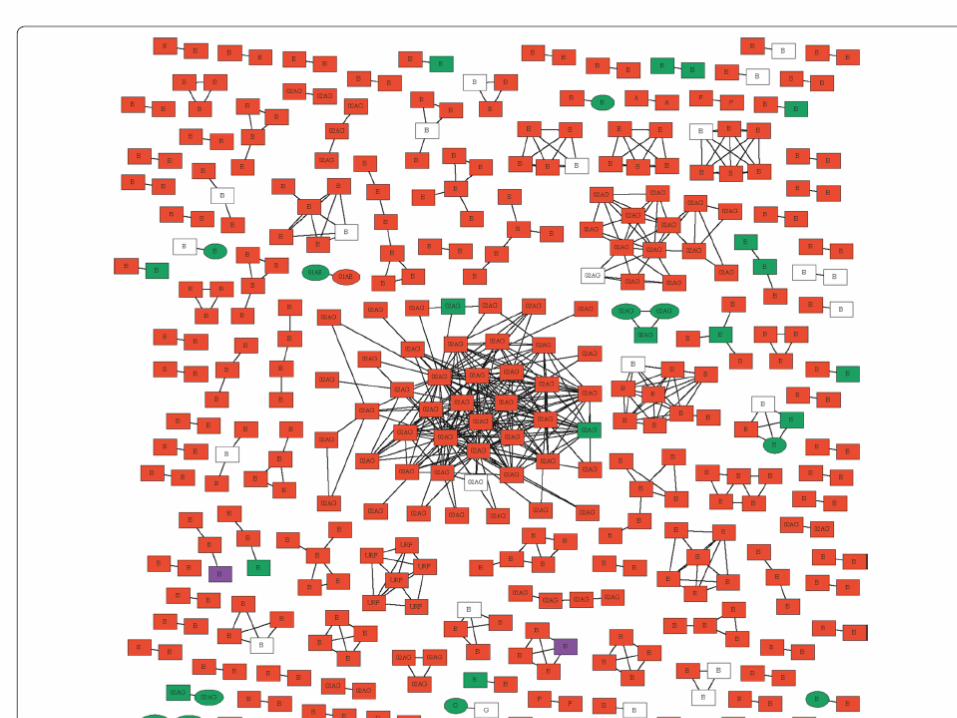
Clusters french acute infections
1. More likely men, younger, white2. Subtype CRF-AG3. More recent 4. Three clusters 9, 14 and 42 infections , all
white men and with geographicalconcentrations and during prolongedperiods


Intervention
1. Target all clustered individuals (223) before2010 would have prevented 60 of 143 onward transmissions,
2. Targeting individuals in intermediate or high density clusters (79) would have prevented 33 onward new infections.
Routine resistance genotyping for all new infections in British Columbia Analysed clusters, if >5 and followed over
growth chracteristics of clusters were shared with public health officials
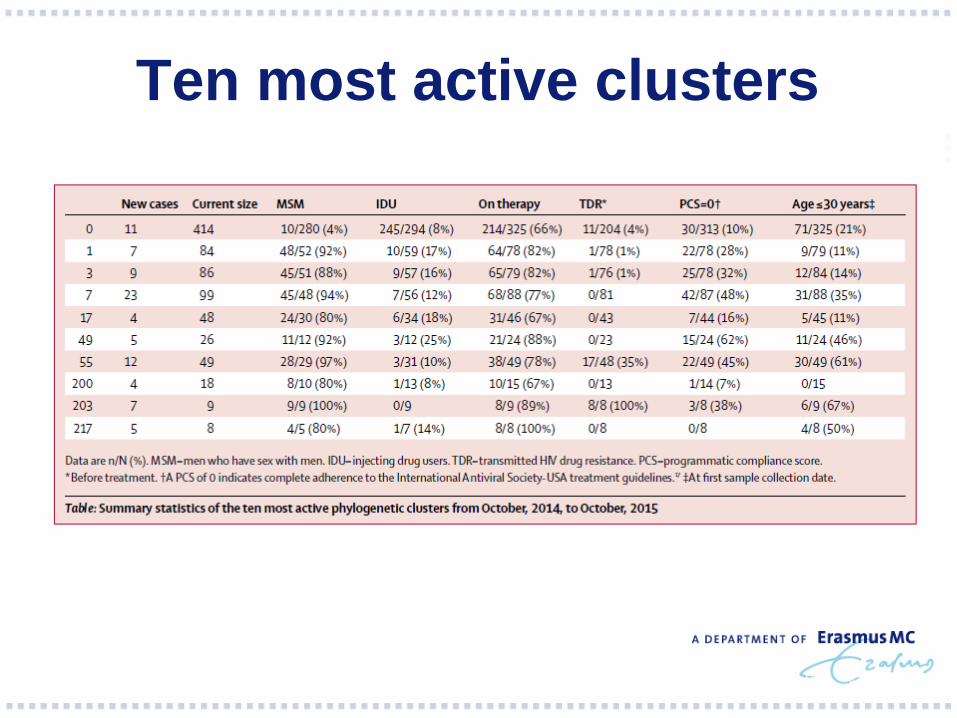
Ten most active clusters
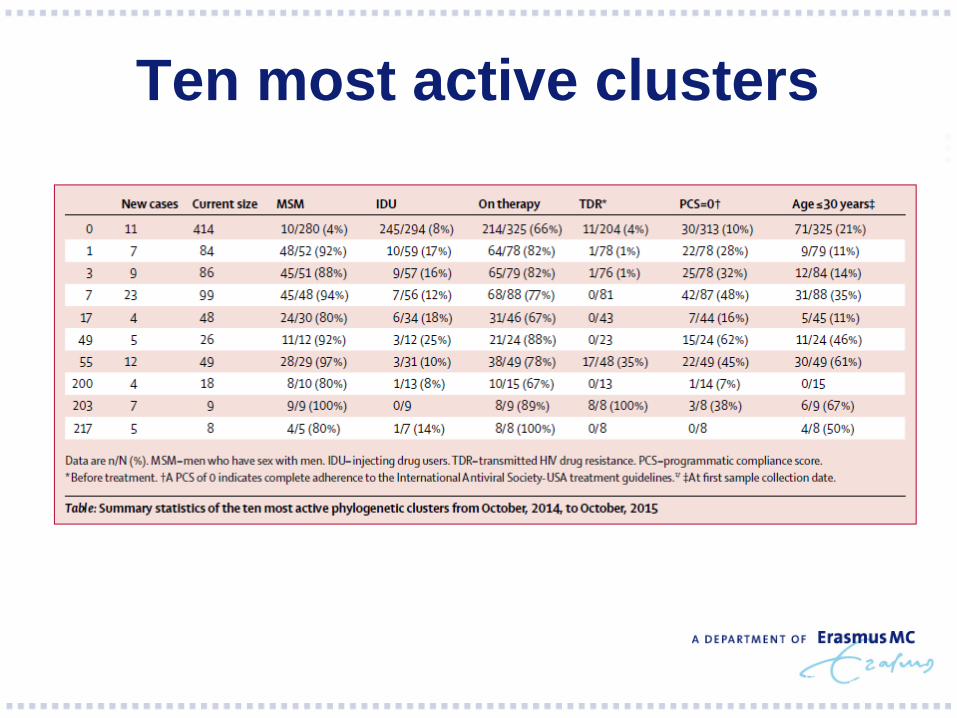
Ten most active clusters
Specific Interventions
Initiate treatment in index case and keep him/her in care (clinical guidelines, treatment as prevention) Trace contacts (counsel partners), test them
and treat them and keep them in care Search and destroy
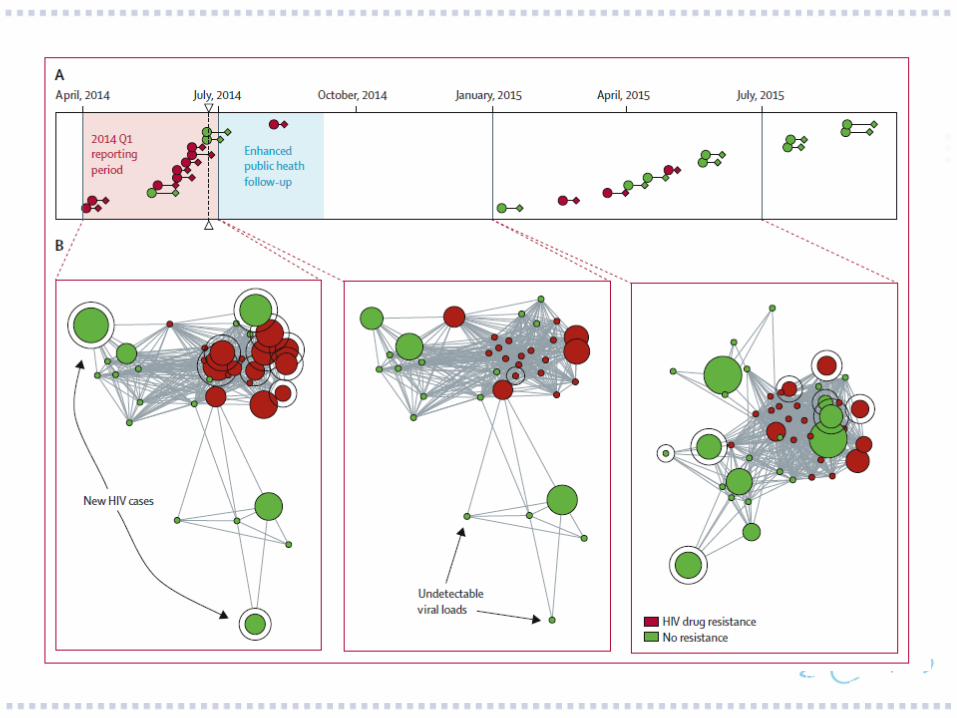
Cluster 55
An additional case with drug resistance in 2014, subsequently 10 new cases, 8 withdrug resistance. Enhanced public health follow up linkage to
care, initiation of therapy, partner notificationtesting partners linkage to care and initiationof therapy

Limitations & Challenges Ethical and legal considerations which differ
per country The more and the earlier patients are
diagnosed the easier it become to performcluster analysis (screening strategies) Similarly the more effect can be obtained
from partner identification, treatment andlinkage to care
Conclusion. To achieve zero new infections in 2030 is a
big challenge Contribution of HIV clinicians will be critical Close(r) collaboration between clinical and
public health community.