Embed Size (px)
DESCRIPTION
HIV Research in International Settings. Wafaa El-Sadr, MD, MPH Columbia University. Overview of Presentation. Status of HIV epidemic HIV-related research where done and who is doing it Priority questions– implementation science Challenges and solutions Conclusions. - PowerPoint PPT Presentation
Citation preview

HIV Research in International Settings
Wafaa El-Sadr, MD, MPHColumbia University

Overview of Presentation
• Status of HIV epidemic• HIV-related research
– where done and who is doing it• Priority questions– implementation science• Challenges and solutions• Conclusions

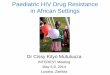
Total: 33.3 million [31.4 million – 35.3 million]
Western & Central Europe
820 000[720 000 – 910 000]
Middle East & North Africa460 000
[400 000 – 530 000]
Sub-Saharan Africa22.5 million
[20.9 million – 24.2 million]
Eastern Europe & Central Asia1.4 million
[1.3 million – 1.6 million]
South & South-East Asia4.1 million
[3.7 million – 4.6 million]
Oceania57 000
[50 000 – 64 000]
North America1.5 million
[1.2 million – 2.0 million]
Central & South America1.4 million
[1.2 million – 1.6 million]
East Asia770 000
[560 000 – 1.0 million]Caribbean240 000
[220 000 – 270 000]
Adults and children estimated to be living with HIV 2009
UNAIDS, 2010


Antiretroviral Therapy by Region--2001


Number of PLWH receiving ART in low- and middle-income countries, by region, 2002–2009
UNAIDS, 2010

Change in HIV Incidence
UNAIDS, 2010

HIV Treatment Coverage in Low & Middle Income Countries
WHO Towards Universal Access 2010

Coverage of HIV Prevention–Low Resource Countries, 2004-2009
Source: UNAIDS/WHO, 2010
0% 20% 40% 60% 80% 100%
HIV testing
Antiretroviral Drugs for PMTCT
Condom Use
Contraception for PMTCT
2004
9% 32%
9%
14%
2006/7
Male Circumcision
20% 61%
70%
10% 75%
47%
Unmet HIV Prevention Need
72%
Estimates of Coverage Unmet HIV Prevention Need
5%
15%
20%
2009
53%
39%
25%
30%
28%
Adapted Ward Cates


CROI 2011Oral Abstracts

Oral Posters

International Scholars

The study of methods to improve the uptake, implementation and translation of research findings into routine and common practices with the goal of improving program effectiveness and optimize efficiency
Know-DoEvidence to Program Gap
Implementation Science



Examples of Implementation Science Questions
Questions
Which TB/HIV integration model produces the best clinical and public health outcomes yet remains efficient and scalable?
What are specific strategies to increase adherence/retention in a particular program?
What is the balance of fixed and mobile clinics that will most effectively allow for rapid acceleration of task shifting and decentralization of HIV care and treatment services?
What is the essential package of laboratory monitoring needed for patients and how does it vary by stage of HIV disease
Adapted Padian et al, JAIDS 2011

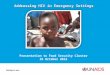
Countries with ICAP-Supported ProgramsTUNISIA
MOROCCO
SAHARA
ALGERIA
MAURITANIA
MALINIGER
LIBYA
CHAD
EGYPT
SUDAN
ETHIOPIA
DJIBOUTI
ERITREA
SOMALIAKENYA
TANZANIA
DEMOCRATIC
(ZAIRE)
CENTRAL
RWANDA
GABON
EQUATORIAL
ANGOLA
CONGO
NIGERIABENIN
DTVOIRE
SIERRA
SENEGAL
GHANA
THE
GUINEA
LIBERIACAMEROON
MALAWI
ZAMBIA
MOZAMBIQUE
MADAGASCARZIMBABWE
BOTSWANA
SWAZILANDLESOTHO
NAMIBIA
ANGOLA
WESTERN
UGANDA
OF THE CONGO
REPUBLIC
BURUNDI
GUINEAREP. OF
TOGOCOTE
BURKINAGUINEA
LEONE
GAMBIA
BISSAU
SOUTH
REPUBLIC
AFRICAN
THE
AFRICA
KYRGYZSTAN
TAJIKISTAN
KAZAKHSTAN
UZBEKISTAN
TURKMENISTAN

ICAP International Research Portfolio
• 40 active protocols • 9 countries • 4 studies with a
multi-country component
Country No. of studies
DRC 1
Ethiopia 1
Ivory Coast 4
Kenya 2
Mozambique 7
Rwanda 10
South Africa 2
Swaziland 6
Tanzania 5

Models for Improving Loss-to-follow-up in the Democratic of Congo (DRC)
Strengthening HIV Test Acceptance and Treatment Uptake Study (STATUS) Epidemiology of HIV-2 or HIV-1/HIV-2 infected patients in Ivory CoastHow to Optimize PMTCT Effectiveness (HOPE) Project in Ivory CoastAn Evaluation of Enhanced Tuberculosis Case-finding to Reduce Mortality Among Persons With Advanced HIV Presenting For HIV Care in Emergency Plan Countries (EMRG) Identifying Optimal Models of HIV Care approaches in sub-Saharan Africa
Development, implementation and evaluation of a comprehensive Prevention intervention in Care and Treatment Settings (PiCTS). Kenya, Tanzania
Establishment of sentinel cohorts of patients enrolled in HIV care and treatment services in Mozambique
Assessing enablers and barriers to the implementation of complex PMTCT regimens and ART in pregnancy in Mozambique
Evaluation of a symptom based flowchart for tuberculosis diagnosis in children in Mozambique
Quality of HIV counseling and testing in maternity in Mozambique
The role of Traditional Birth Attendants (TBA) in active defaulter tracing and adherence programs in MozambiqueMother-infant pair linkage using paper-tracking systems in Mozambique
Evaluate TB screening of pregnant women at two PMTCT sites in Gaza Province in MozambiqueQualitative study of ART adherence in Mozambique
Evaluation of a new patient tracking system on patient care and perceptions of care in MozambiqueSharing HIV/AIDS responsibility Efforts (SHARE) in Nigeria
Evaluating adherence to antiretroviral therapy among HIV care and treatment patients in Rwanda
Smear negative and extra pulmonary tuberculosis diagnosis and outcomes in Rwanda
Operating characteristics of a screening instrument for the detection of active tuberculosis in adult outpatients with HIV infection in Rwanda Evaluation of TB screening approaches for HIV-infected children in Rwanda
Estimating HIV incidence in two populations in Rwanda: High-risk women and female VCT clients- Project Ubuzima in Rwanda
Peer Educator for Adherence, Referral and Linkages Program Evaluation (PEARL study) in RwandaNational Pulmonary Tuberculosis Prevalence Survey in RwandaAssessing HIV Prevention, Care & Treatment at Sites Supported by Columbia University-International Center for AIDS Care and Treatment Programs (ICAP) in Rwanda
Evaluation of the quality of the national antiretroviral treatment program in Rwanda, 2004 - 2005Evaluation of access and utilization of PMTCT services in Rwanda BED and A1 Assay Validation Work, Kigali Incidence Study -- Project Ubuzima, Kigali, RwandaEvaluation of Access to and Acceptance of HIV Counseling and Testing Among Patients with Tuberculosis in Rwanda
Operating characteristics and effectiveness of a screening instrument for the detection of active tuberculosis in adult outpatients with HIV infection in the Eastern Cape, South Africa
Design, implementation and assessment of a nurse mentor training program in HIV care and treatment in Eastern Cape, South AfricaSwaziland HIV Incidence Measurement Survey (SHIMS)Swaziland National ART Program Evaluation: Treatment Outcomes and Cost-Effectiveness during 2004-2009Swaziland in-service HIV training assessment
Assessment of impact of the ART Program on people receiving Anti-Retroviral Therapy in Swaziland following six years of ART implementation in the country
Feasibility Pilot of the Evaluation of Expert Client Program: Swaziland National ART Program
Etiologic Survey for Genital Infections Among HIV-infected Adults Entering HIV Care: A Pilot Study in TanzaniaHIV Combination Prevention in TanzaniaNeonatal Circumcision Situation Assessment in Tanzania

A range of methodologies…
• Qualitative methods– Key informant interviews– Focus group discussions
• Quantitative methods– Group randomized studies– Cohort studies– Cross-sectional surveys
• Data collection – Questionnaires/interviews with patients and health workers– Data abstraction from routinely collected data– Site characteristics assessment tools

GCP Training
• Barriers – Non- Anglophone
investigators have difficulty completing GCP training
– Module content and examples are US focused and not relevant to international research
– Field internet connections hinder completion of web courses
• Suggestions– Consider translated
modules e.g. French and Portuguese
– Design modules with international focus appropriate for international investigators
– Adequate local training given at the time of study launch rather than required early in the process

The Protocol Approval Process
IN COUNTRY & NY REVIEW
Feedback&
Revision In-country
investigators ICAP-NY
investigators Local CDC Office
Feedback&
Revision
Feedback&
Revision
Feedback&
Revision
1 2 3 5 4
OGAC PHE Committee
Submitted via the local CDC office ADS
CDC Atlanta GAP ADS
Submitted via ICAP NY
Administrative approval for release of funds
LOCAL IRB
Local IRB approval Other in-country
approvals e.g. administrative approval from MOH
CU IRB
Submitted via RASCAL
CDC IRB
If CDC investigators are involved
• Multiple levels • Local and international

Multiple IRBs Review Processes
• Synchronizing reviews, comments and versions– If submissions are simultaneous, different IRBs will
provide feedback at different times – If submissions are done consecutively, the process
takes more time– Deciding which IRB to submit to first:
• For example, CU IRB usually gives more comments requiring protocol changes yet requires local IRB approval before they provide final approval

Field implementation of IRB requirements
• Getting timely approvals when there is national/MoH agenda and imperatives
• Adhering to required formats e.g. having the international PI name on the consent form, which may conflict with local requirements
• Using IRB stamped versions of tools – Running out of these forms

Local issues
• Local IRBs will usually approve first time protocols within reasonable time but– Renewals/modifications may take longer in some
countries – Some countries have several levels of approvals
which take more time
• Getting certified translators to fulfill IRB requirements can be difficult with some local dialects – Example: Changana and Macua in Mozambique

Example: PiCTS study
• Multi-country multi-site PHE: Kenya and Tanzania under ICAP, + Namibia
• Initial IRB submission done simultaneously in Oct 08 • IRB approval dates:
– Kenya local IRB Jan-09– CDC IRB Feb-09– CU IRB Feb-09– Tanzania
• Mainland IRB Apr-09 • Zanzibar IRB Jun-09
• Several rounds of revisions

Interpretation of IRB Non Human Subject Research (NHSR) determination
• Program evaluations can be considered NHSR even if they include interaction with human subjects (with no identifiable information) but
• the determination will say ‘no interaction with human subjects’
• Publication of program evaluations may require additional approval but
• This is not the case where there is no interaction with human subjects?
• How to deal with publications to share local lessons learned?


Conclusions• Substantial advances in tackling the HIV epidemic, but
many unanswered questions remain• Priority of pragmatic questions—implementation
science• Need to respond to the local circumstances and needs• Importance of considering the flow of approvals• Clearer definitions and interpretation of NHSR• Challenge of non-traditional research • Establishing responsive systems for support of
international research is a key priority