Embed Size (px)
Citation preview

1
Learning Objectives
Upon completion, participants should be able to:• Incorporate available tools to screen patients for IDU into
routine practice• Develop processes to mitigate infectious diseases risks of
IDU, including HCV/HIV testing, medication-assistedtherapy for opioid misuse, harm-reduction strategies, andPrEP
• Describe various resources to help rural primary careclinicians provide treatment to patients diagnosed withHCV and/or HIV

2
Age-Adjusted Rates of Death Related to POs and Heroin, 2000-2014
• Between 2000 and 2014,the rates of death from POoverdose nearly quadrupled
• In 2015, drug overdosesaccounted for 52,404 deaths inthe US, 63.1% (33,091)of which involved any typeof opioid
• In 2015, heroin-related deathrates were highest among 24-44 year olds (13.2/100,000),increasing 22.2% from 2014 to2015
Compton WM, et al. N Engl J Med. 2016;374:154-63; Rudd RA, et al. MMWR Morb Mortal Wkly Rep. 2016;65:1445-52.
0.7 0.6 0.7 0.7 0.6 0.7 0.7 0.81.0 1.1 1.0
1.4
1.9
2.7
3.4
1.5
1.9
2.62.9
3.43.7
4.64.8 4.8
5.0
5.4 5.45.1 5.1
5.9
0
1
2
3
4
5
6
7
200
0
200
1
200
2
200
3
200
4
200
5
200
6
200
7
200
8
200
9
201
0
201
1
201
2
201
3
201
4
No
. of
Ove
rdo
se D
eath
s p
er
100,
000
Po
pu
lati
on
Year
HeroinPOs
WA
OR
CA
NV
UT
AZ NM
CO
WY
TX
OK
KS
NE
SD
NDMT
ID
AK
HI
LA
AR
MO
IA
MN
WI
IL IN
MI
OH
MEVT
PA
NY
VAWV
KY
TN
ALMS
SC`
NC
GA
FL
NH
MA
RI
DE
MD
NJ
CT
Number and Age-Adjusted Rates of Drug Overdose Deaths by State, US, 2015
• From 2014 to 2015, thedeath rate from syntheticopioids other thanmethadone, whichincludes fentanyl,increased by 72.2%,and heroin death ratesincreased by 20.6%
• Natural/semisyntheticopioid death ratesincreased by 2.6%,whereas methadonedeath rates decreasedby 9.1%
CDC. Drug Overdose Death Data. www.cdc.gov; Rudd RA, et al. MMWR Morb Mortal Wkly Rep. 2016;65:1445-52.
2.8 to 11.011.1 to 13.513.6 to 16.016.1 to 18.518.6 to 21.021.0 to 41.5

3
AZ
WY
WA
OR
CA
NV
UT
NM
TX
OK
KS
SD
NDMT
ID
AK
HI
LA
AR
MO
IA
MN
WI
IL IN
MI
OH
MEVT
PA
NY
VAWV
KY
ALMS
SC`
NC
GA
FL
MA
DE
MD
NJNE
NH
RICT
Opioid Prescriptions: Where You Live Matters
CDC. Opioid Painkiller Prescribing. www.cdc.gov.
52-7172-82.182.2-9596-143
Number of painkillerprescriptions per 100 people
CO
TN
Number of Painkiller Prescriptions per 100 People
Number of Painkiller Prescriptions per 100 People
State Abbreviation
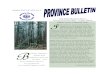
Opioid Prescribing, by Specialty, 2007-2012
• In 2012, rates of opioidprescribing were highest in painmedicine (48.6%), surgery(36.5%), and physicalmedicine/rehabilitation (35.5%)
• Although rates of opioidprescribing in primary carespecialty groups were low (4.8-7.5%), those dispensed opioidsaccounted for almost 50% of alldispensed opioid prescriptions
• Additionally, nonphysicianprescribers accounted for 11.2%of all dispensed opioids
Levy B, et al. Am J Prev Med. 2015;49:409-13.
-10%
15%
Per
cen
t C
han
ge
Fro
m B
asel
ine
in R
ate
of
Op
ioid
Rx/
Tota
l Rx
2005
10%
5%
0%
-5%
2007 2008 2009 2011 2012
Physical med and rehabPain medicineInternal medicineGeneral practiceNonphysician prescriberFamily practiceTotalSurgeryDentistryEmergency medicine
*Percentage change depicts the cumulative, absolute change away from 2007 rate for opioid prescriptions as a fraction of total prescriptions.

4
Impact of Nonmedical Use of POs in Adolescence on the Risk of Future Heroin Use• Nonmedical use of POs increases the odds of riskier drug use,
including heroin, in younger cohorts• Prior use of nonmedical prescription opioids in adolescence is a
strong predictor of heroin use onset– Risk of heroin initiation was 13 times higher among individuals
who reported nonmedical prescription opioid use than thosewho had no history (95% CI, 10.73-16.04)
– Risk was highest among those who were first exposed tononmedical prescription opioids in early adolescence (10-12years of age) (HR, 15.42; 95% CI, 12.44-19.11)
Palamar JJ, et al. Drug Alcohol Depend. 2016;158:132-8; Cerda M, et al. J Pediatr. 2015;167:e1-2.
Incidence of Acute HCV Among Persons Aged ≤ 30 years, by Urbanicity and Year
(KY, TN, VA, WV, 2006-2012)
CDC. MMWR Morb Mortal Wkly Rep. 2015;64:453-8.*95% confidence interval
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
2006 2007 2008 2009 2010 2011 2012
No
. of
Cas
es p
er 1
00,0
00 P
op
ula
tio
n
Year
Non-urbanUrban
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
*

5
Newly Reported (Chronic or Acute) HCV Infection, NM, 2006-2012
Page K. Hepatitis C Epidemiology in New Mexico: The Role of Injection Drug Use. New Mexico Annual HIV & HCV Update Conference. Albuquerque, NM. April 30, 2015.
0
200
400
600
800
1000
1200
2006 2007 2008 2009 2010 2011 2012
Nu
mb
er o
f R
epo
rted
Cas
es
Year
Age 25-34
Age 55-64
< 1313-2425-3435-4445-5455-64≥ 65
2015 HIV Outbreak in Scott County, IN
• Scott County ranks 92nd out of 92 counties inmany social and health indicators
• Outbreak centered in the town of Austin, IN– Population: ~4,200– 19% of population living below the poverty line– 10% unemployment rate– 21% did not graduate high school– Before the outbreak, free HIV testing had
not been unavailable since 2013• Austin has only 1 PCP and the nearest
hospital/ED is 5 miles away in Scottsburg, IN
County Health Rankings. Scott County, IN. www.countyhealthrankings.org; Janowicz DM. Top Antivir Med. 2016;24:90-2; Peters PJ, et al. N Engl J Med. 2016;375:229-39.

6
2015 Scott County Outbreak, Epidemiology
• In December 2014, multiple new cases of HIV were diagnosed in Scott County– All cases linked to IDU, specifically to the injection of oxymorphone
• As of May 2016, 191 confirmed cases of HIV– Median age: 34 years (18-60)a
– 58% male, 100% non-Hispanic whitea
– 92% coinfected with HCV (167/181)a
– 96% reported IDU (173/181)b
– 95% with annual income < $10,000a
– Multigenerational sharing of injection equipment
• 513 total contacts traced– 38% positivity rate among tested contacts– Nearly 5% prevalence in Austin
• > 300 individuals remain at riskConrad C, et al. MMWR Morb Mortal Wkly Rep. 2015;64:443-4;
ISDH. Scott County Public Health Emergency Declaration Extended. www.in.gov; Janowicz DM. Top Antivir Med. 2016;24:90-2; Peters PJ, et al. N Engl J Med. 2016;375:229-39.
aAs of April 2016bAs of November 2015
Epidemic Curve: Scott County, IN, Outbreak
Adams J. N Engl J Med. 2015;373:1379-80.
Co
un
t
25
0
20
15
10
5
18
7
1
5
3
8
14
11
22
17
999 9
5 5
3 3
5
1111 1 1 12 2 2
0000 0 0 0
4
0 0 0 0
15
Ma
r 1
5
8 M
ar
15
1 M
ar
15
22
Fe
b 1
5
15
Fe
b 1
5
8 F
eb
15
1 F
eb
15
25
Ja
n 1
5
18
Ja
n 1
5
11 J
an
15
4 J
an
15
28
De
c 1
42
1 D
ec
14
14
De
c 1
4
7 D
ec
14
30
No
v 1
4
23
No
v 1
4
16
No
v 1
4
0
2 A
ug
15
0
19
Ju
l 15
22
Ma
r 1
5
29
Ma
r 1
5
5 A
pr
15
12
Ap
r 1
5
19
Ap
r 1
52
6 A
pr
15
3 M
ay
15
10
Ma
y 1
51
7 M
ay
15
24
Ma
y 1
5
31
Ma
y 1
5
7 J
un
e 1
5
14
Ju
n 1
52
1 J
un
e 1
52
8 J
un
15
5 J
ul
15
0
12
Ju
l 15
0
26
Ju
l 15
9 A
ug
15
16 A
ug
15
23 A
ug
15
30 A
ug
15
6 S
ep
15
13
Se
pt
15
20
Se
pt
15

7
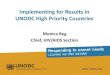
Counties Within the 95th Percentile of Most Vulnerable to Future HIV and/or HCV Outbreaks
Van Handel MM, et al. J Acquir Immune Defic Syndr. 2016;73:323-31.
Ranked IndexTop 200 counties
Challenges in Reaching Rural PWID
• Dispersed and hidden populations• Medically underserved• Gaps and lacks in services and providers• Poverty• Cultural differences• Stigma• Fear of mistreatment and criminalization• Shame
Slide courtesy of Dr. Patrick Milligan.

8
HCV and HIV Prevention Toolbox for PWID
Slide courtesy of Dr. Patrick Milligan.
Point of transmission
After exposure
Before exposure
• Change in injectingbehavior
• Clean injectingequipment
• Needles
• Ancillary equip
• Alcohol, bleach
HCV treatment
Prevent HCVreinfection
HIV treatment
• Drug treatment foropioid disorder
• HCV/HIV testing andcounselling
• PrEP for HIV prevention
• Reducing HCV/HIVtransmission inserodiscordant injectingand sexual partners
• Abstinence
Before Exposure: Screening for IDU in Primary Care
• Several evidence-based screening tools for drug use and opioid risk can beused in the primary care setting
NIH. Chart of Evidence-Based Screening Tools for Adults and Adolescents. www.drugabuse.gov;NIH. American Psychiatric Association Adapted NIDA Modified ASSIST Tools. www.drugabuse.gov.
Screening Tool Patient Age Group Method of Administration
Adult Adolescent Self-administered
Clinician-administered
Prescreens
CRAFFT (Part A) X X X
NIDA Drug Use Screening Tool: Quick Screen
X See APA Adapted NM ASSIST tools
See APA Adapted NM ASSIST tools
X
Opioid Risk Tool X X X
Full Screens
CAGE-AID X X
CRAFFT X X X
DAST-10 X X X
DAST-20: Adolescent Version X X X
NIDA Drug Use Screening Tool X X

9
MAT for Opioid Use Disorder
• MAT can reduce the incidence of HIV and HCV infections by 54% and> 60%, respectively, but barriers to its implementation are disproportionatelyhigher in rural areas
• The shortage of MAT providers and opioid treatment programs has improvedlargely in part to an increase in buprenorphine providers– Shortages still remain disproportionately high in rural areas– In 2011, 60% of small, non-metropolitan residents lived in “shortage” areas,
compared with 5% of metropolitan residents
• Patients often lack insurance, experience “onerous” treatment demands, feelstigma, can be pressured to end MAT therapy by providers, and lack socialsupport
• In many areas of need, including rural areas, insurance policies do not coverthe therapy
MacArthur GJ, et al. BMJ. 2012;345;e5945; Tsui JI, et al. JAMA Intern Med. 2014;174:1974-81; Dick AW, et al. Health Aff (Millwood). 2015;34:1028-34; Knudsen HK, et al. J Stud Alcohol Drugs. 2014;73:476-85.
Before Exposure: Identifying PWID at Risk of HCV / HIV
• Medical settings– Primary care– Ante-natal care– ED– Drug-treatment programs– Pharmacies
• Nonmedical settings– SEPs (mobile and non-mobile)– Jail– Home
• Traveling providers, peer educators– Community outreach centers
Slide courtesy of Dr. Patrick Milligan.

10
Point of Transmission:Safer Injection Practices and SSPs
• Research shows that SSPs are a highly effective strategy toprevent HIV and possibly HCV among PWID– HIV diagnoses among PWID dropped by 48% from 2008 to
2014, and HIV-prevention programs, including SSPs, wereinstrumental in this decline
• Basic services of SSPs allow PWID to exchange used needlesand syringes for new, sterile needles and syringes– 200 sterile syringes per injector per year for a high level of
coverage (UNAIDS)– Services can be expanded to included HCV/HIV testing, linkage
to care, and treatment for substance use disorders
amfAR. Preventing HIV and Hepatitis C Among People Who Inject Drugs: Public Funding for Syringe Services Programs Makes the Difference. www.amfAR.org; CDC. HIV and Injection Drug Use. www.cdc.gov; Des Jarlais DC, et al. MMWR Morb Mort Wkly Rep. 2015;64:1337-41; UNAIDS. People Who Inject Drugs. www.unaids.org.
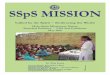
HIV Incidence and Public Funding, 1985-2012
• Laws allowing SSPs,permitting OTC sales ofsyringes, and providingpublic funding for SSPsare associated withreducing new HIVincidence and maintainingalready low levels ofincidence among PWID
Bramson H, et al. J Public Health Policy. 2015;36:212-30;amfAR. Preventing HIV and Hepatitis C Among People Who Inject Drugs: Public
Funding for Syringe Services Programs Makes the Difference. www.amfar.org.
HIV Incidence and Public Funding, 1985-2012
States With HighInfection Rates That
REMAINED HIGH, 1985-2012
States With HighInfection Rates That DECLINED TO LOW,
1985-2012
States With Low Infection Rates That
REMAINED LOW, 1985-2012
High new HIV infections yearly (> 2%)• Florida• Louisiana• South Carolina• Texas
• Connecticut• District of Columbia• Maryland• Massachusetts• Michigan• North Carolina• New Jersey• New York• Oklahoma• Pennsylvania• Tennessee• Virginia• Wisconsin
• Arizona• California• Colorado• Missouri• New Mexico• Ohio• Oregon• Utah• Washington
Low new HIV infections yearly (< 2%)
Note: Bolded states are those that receive public funding for SSPs.

11
OST, NSPs, and HCV Incidence
Slide courtesy of Dr. Kimberly Page.
0
0.5
1
1.5
2
2.5
Opioid substitutiontherapy
High NSP vs no/low NSP coverage
Low NSP vs noNSP
Combined: OST &NSP vs NSP (no
OST)
Combined: OST &NSP vs low NSP
HC
V In
cid
ence
, 95%
CI
Laboratory Screening for PrEP Candidates
• HIV– Must be HIV negative
• Renal function– CrCl ≥ 60 mL/min
• HBV– TDF/FTC may be recommended– Referral to infectious disease specialist
• Pregnancy– Positive pregnancy test does not preclude women from PrEP,
but potential risks and benefits of PrEP should be discussed
CDC. PrEP for the Prevention of HIV Infection in the US. www.cdc.gov.

12
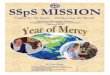
Clinical Study of PrEP in PWID
• Bangkok Tenofovir Study (2013) investigated the effects of a PrEP strategy forHIV prevention in 2,413 Thai PWID
Choopanya K, et al. Lancet. 2013;381:2083-90.
• 48.9% reductionin HIV incidence(95% CI, 9.6-72.2;P = .01)
• 73.5% reduction in HIVincidence in individualswith detectable druglevels (95% CI,16.6-94.0; P = .03)
Number at RiskTDF 1,204 1,007 933 857 736 521 241Placebo 1,207 1,029 948 844 722 500 234
Kaplan-Meier Estimates of Time to HIV Infection in the Modified Intention-to-Treat Population
Months Since Randomization0
0
2
4
6
8
10
Cu
mu
lati
ve P
rob
abili
ty
of
HIV
Infe
ctio
n,
% TDFPlacebo
12 24 36 48 60 72 84
Revised PrEP Algorithm (May 2015)
Janowicz DM. Persistent Challenges of HIV Transmission Control in Injection Drug Use: Lessons From the Indiana Outbreak. IAS 2016. Los Angeles, CA. April 25, 2016.
Intake Visit- Risk assessment- Lab tests:
- HIV viral load- CrCl- HBV sAg- HBV sAb
-Verify insurance
PrEP is contra-indicated
- HIV Ab test- Refer for cART
Prescribe TDF/FTC for 30 days, 2 refills
2-week visit for adherence
(first time only)
30-Day Visit- Counseling- Pill count- Optional HIV Ab
test
60-Day Visit- Counseling- Pill count- Optional HIV Ab
test
90-Day Visit- Counseling- Pill count- Check CrCl- HIV Ab test- Risk assessment
Viral load positive
Viral load negative
Risk assessment negative or CrCl < 60
Initiation Visit(<7 days from Intake)
- Verify labs- Counseling- Additional HBV counseling
if necessary

13
Project ECHO: Effect on HCV Care in Rural Settings
• Almost 94% of providers participating in an ECHO clinic in Utah and Arizonahad no experience managing HCV– After participating in the clinic, 46% of patients seen were started on
treatment
• An ECHO program conducted through the Indian Health Service reported that100% of its participants found benefits of participating, including being well-informed, having access to expertise, collegiality, and decreased professionalisolation– One-half of respondents indicated they would not have treated HCV without
regular participation in the ECHO clinics
• In New Mexico, the ECHO model was used to develop a program focused onthe treatment of substance use disorders and behavioral health (IntegratedAddictions and Psychiatry Clinic)
Mitruka K, et al. MMWR Morb Mort Wkly Rep. 2014;63:393-8; Pindyck T, et al. SAGE Open Med. 2015;3:2050312115612805; Komaromy M, et al. Subst Abus. 2016;37:20-4.
Acknowledgment of Commercial Support
This activity is supported by an educational grant from Gilead Sciences, Inc.
Call (toll-free) 866 858 7434E-mail [email protected]
Please visit us online at www.Med-IQ.com for additional activities provided by Med-IQ®.
Contact Information

14
© 2017
To receive credit, click the “Get Credit” tab at the bottom of the Webcast for access to the evaluation, attestation, and post-test.
Unless otherwise indicated, photographed subjects who appear within the content of this activity or on artwork associated with this activity are models; they are not actual patients or doctors.

Abbreviations
CDC = Centers for Disease Control and Prevention ECHO = Extension for Community Health Outcomes ED = emergency department HCV = hepatitis C virus HIV = human immunodeficiency virus IDU = injection drug use MAT = medication‐assisted therapy NSP = needle and syringe program OST = opioid substitution therapy OTC = over the counter PCP = primary care provider PO = prescription opioids PrEP = pre‐exposure prophylaxis PWID = people who inject drugs SEP = syringe exchange program SSP = syringe services program US = United States