Embed Size (px)
Citation preview

20
HOMOZYGOUS HÆMOGLOBIN-E DISEASE
IN INDONESIA
LIE-INJO LUAN ENGM.D., D.T.M.&H.SENIOR ASSISTANT
OEY HOEY GIOK
MEDICAL STUDENT
DEPARTMENT OF PARASITOLOGY AND GENERAL PATHOLOGY,UNIVERSITY OF INDONESIA, DJAKARTA
SINCE the discovery- of haemoglobin E in 1954 byItano et al. (1954) in a family of partly Indian origin andsimultaneously by Chernoff et al. (1954) in the Siamese,this abnormal pigment has been observed in Veddas fromCeylon (Graff et al., 1954), in Indonesians (Lie-Injo LuanEng 1955a), and in Burmese (Lehmann et al. 1956).Three conditions associated with this abnormal pigment
have been recognised : the haemoglobin-E trait, which isthe heterozygous form for the gene of this abnormalhaemoglobin ; pure haemoglobin-E disease, representingthe homozygous state ; and hsemoglobin-E/thalasssemiadisease, representing the double heterozygous state forthe haemoglobin-E and the thalassaemia genes.
Six cases of pure haemoglobin-E disease have been
reported from Thailand (Chernoff et al. 1956) and twoin Burmese (Lehmann et al. 1956) ; but in no case was itpossible to study both parents to prove the homozygosityof the condition.We report here three cases of pure haemoglobin-E
disease in Indonesians. In two of the three cases both
parents were carriers of haemoglobin E.
Methods
All pipettes and counting-chambers used for hsemato-logical determinations carried the certificate of the U.S.National Bureau of Standards. Observations were madein - duplicate. Foetal haemoglobin in the blood wasestimated by the method of alkali denaturation describedby Singer et al. (1951). For normal adults 2% alkali-resistant hsemogJobin of the total amount of haemoglobinwas taken as the upper limit of normal (Singer et a].1951, Lie-Injo Luan Eng 1955b).Haemoglobin was analysed by paper electrophoresis
according to the method described by Smith and Conley(1953) with veronal buffer pH 8-6 and ionic strength0-05 and phosphate buffer pH 6-5 ionic strength 0-1.Serum-bilirubin and urobilin and urobilinogen - in theurine were examined in the laboratory of the CentralGeneral Hospital, Djakarta.
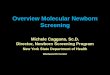
Fig. 1-Case 1 : peripheral blood showing slight anisocytosis andpoikilocytosis. Here no target cells are seen, but in other areas a fewtarget cells were found. (x 837.) -
Case-reportsCase 1.-A girl, aged 9 years, was examined only because,
during a survey on pathological haemoglobins in the wards ofthe Central General Hospital in Djakarta, her mother, whowas being treated for chronic bronchitis, was found to be acarrier of haemoglobin-E trait. The whole family was there-fore examined, and it was found that case 1, the eldest child;had pure hsemoglobin E in her blood, and her father was acarrier of hsemoglobin-E trait. The family came from Padang,in Sumatra. So far as they knew they were pure Indonesians.The girl did not feel ill but, according to her mother, she wasriot strong, was easily fatigued, and had always lookedsomewhat pale. She had never had icterus. -
Physical examination on Jan. 31, 1956, showed that shewas in good nutritional state and did not look ill but seemedslightly ansemic. Her lymph-nodes were not enlarged, heartand lungs were normal, and spleen and liver both slightlyenlarged, firm, and not tender. No other physicalabnormalities were noticed.Radiography of her skull, long bones, metacarpals and
metatarsals, thorax, vertebrae, and pelvis did not show any
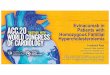
Fig. 2-Paper electrophoresis at pH 8.6 of haemoglobin of case I, herparents, and her grandmother compared with controls.
abnormality. Her lungs and heart were also normal on
radiography.Laboratory /MtcKM.<j’.s.—Haematological data are summarised.
in table i. There was slight erythrocytosis and microcytosis.The mean corpuscular haemoglobin concentration (M.C.H.C.),however, was normal. The changes in the peripheral bloodwere not obvious (see fig. 1). There were only slight poikilo-cytosis and anisocytosis. No normoblasts were seen. Therewere no Howell-Jolly bodies and no rings of Cabot, but therewere a fair number of cells with basophil stippling, Only afew target cells were seen. There was also a slight reticulo-cytosis. A sickling test with 2% sodium metabisulphite wasnegative. No malarial parasites were observed. The resistanceof the erythrocytes to hypotonic saline solution was increased.The amount of alkali-resistant haemoglobin was found not tobe increased. Paper electrophoresis of the haemoglobin at
pH 8-6 showed only one type of haemoglobin, having a mobilitywhich seemed to be similar to that of haemoglobin C. How-ever, since both parents were found to carry haemoglobin Ewith a mobility higher than that of haemoglobin C, it was,
expected that the child had haemoglobin E and not haemoglobinC. Indeed, at pH 6-5 the mobility was found to be definitelyless than that of haemoglobin C. When the child’s haemoglobinwas mixed with normal haemoglobin so that the relativeconcentrations of the abnormal and the normal componentwere about the same as in a trait-carrier, the abnormalcomponent had the same mobility at pH 8-6 as that of

21
* Control determinations of the osmotic saline fragility in normal persons showed initial haemolysis at 0-44-0-40 % (mostly at 0. 44%);complete hsemolysis at 0-32-0’28 % (mostly at 0-32%).
haemoglobin E and was slightly faster than haemoglobin C.It was therefore evident that the child had pure haemoglobin E(see fig. 2). The serum-bilirubin level was not raised. Theurine contained urobilin and urobilinogen but no bilirubin oralbumin. In the fseces a few eggs of Ascaris lumbrieoides werefound but no other parasites or other abnormalities. Bone-marrow puncture was’unfortunately not allowed.Progres8.-After three weeks’ iron therapy there was no
hsematological improvement. The amount of alkali-resistanthaemoglobin was again found not to be increased.
FamilyThe mother, aged 45, had chronic bronchitis, was very
thin, and looked ill. Her heart was normal; her spleen andliver were not enlarged. The laboratory findings are sum-marised in table i.The father, aged 50, was healthy, no abnormalities being
found on physical examination. His spleen and liver werenot enlarged. The laboratory findings are summarised intable T. t1A was a. farrier of hæmoglobin-E trait.
The second child, a girl aged 3
years, was not ill. On physicalexamination no abnormality wasfound except slight rhinitis. Her
spleen and liver were not enlarged.The laboratory data are summarisedin table i. The haematologicalfindings were within the normal
range for her age except for eosino-philia. Her haemoglobin was of thenormal type.The youngest child, a boy of 13
months, was dystrophic and hadinfluenza, diarrhœa, and bronchitis.His spleen and liver were not
enlarged. The laboratory findings arelisted in table i. He was found tobe a carrier of hsemoglobin-E trait.The grandmother of case 1 was
aged 70 and haa.lt,hv On physical
examination no abnormalities were found. Her spleen andliver were not enlarged. She was a carrier of haemoglobin-Etrait (fig. 2 and table i). Other laboratory findings are alsolisted in table i.
The pedigree of this family is shown in fig. 3.
Case 2.-An Indonesian soldier, aged 36, from the islandof Timor, was registered as a regular donor at the BloodTransfusion Service of the Red Cross in Djakarta. When hegave 500 ml. of blood on May 9, 1956, a small amount wastaken for routine survey of pathological hæmoglobins ; andhis erythrocytes were found to contain pure haemoglobin E.We studied him further on July 7, 1956. He said that he wasquite healthy, was very seldom ill, and did his heavy jobwithout any complaint. He had never had anaemia or icterus.He was married and had two healthy children.On physical examination he was in a good nutritional state
and not anæmic. There was not the slightest icterus. His
lymph-nodes were not enlarged, his lungs and heart werenormal, and his liver was not enlarged, but his spleen was justpalpable one finger-breadth below the costal margin, firm, andnot tender. ’
Radiography of his skull, long bones, metacarpals andmetatarsals, thorax, vertebrae, and pelvis did not reveal anyabnormality.
Laboratory findings on July 23, 1956, are listed in table m.There was microcytosis but no anæmia. The M.C.H.C. wasnormal. The peripheral blood showed only slight aniso-
cytosis, but there were numerous target cells (fig. 4). Redcells with basophil stippling were present. The number of
reticulocytes was not increased. The numbers of leucocytesand of thrombocytes were normal. A sickling test with 2%sodium metabisulphite was negative. No malarial parasites.were found. The resistance of the red cells to hypotonic salinesolution was increased. The serum-bilirubin level was notraised. Electrophoresis showed only haemoglobin E (fig. 5).The percentage of alkali-resistant haemoglobin was withinnormal limits. The urine did not show any abnormality.
F arnilyOn Sept. 14, 1956, the parents of case 2 could not be
examined, but we examined his wife and two children.The wife did not feel ill. She was two months pregnant.
On physical examination no abnormalities were found. The
laboratory findings are shown in table 11. She was a carrier ofhæmoglobin-E trait.The elder child, a girl aged 3 years, had pure hæmoglobin-E
disease (see case 3). ’
The second child, a boy aged 1 year, had rhinitis and wasvery often ill with pyrexia. He had had dysentery of undeter-mined aetiology two months before examination. On physicalexamination he was found to be somewhat dystrophic. The
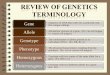
Fig. 4-Case 2 : : peripheral blood showing numerous target cells
( x 837).

22
TABLE II—LABORATORY FINDINGS IN CASES 2 AND 3 AND FAMILY
laboratory findings are shown in table 11. In his faeces noabnormalities were found. He was a carrier of haemoglobin-Etrait.
Case 3.-A girl, aged 3 years, daughter of case 2, washealthy. She was in a good nutritional state and very seldomill. On physical examination no abnormalities were found.Her spleen and liver were not enlarged. Her heart and lungswere also normal. The laboratory findings are shown in table11. Her haemoglobin was within normal limits for her age.There was a clear microcytosis of the erythrocytes. The mean
corpuscular haemoglobin was normal. The peripheral bloodshowed slight anisocytosis. Target cells were present but notso numerous as in her father’s blood. Basophil stippled cellswere not found. The number of reticulocytes was not increased.A sickling test with 2% sodium metabisulphite was negative.No malarial parasites were found. The resistance of the
erythrocytes to hypotonic saline solution was increased.
- Electrophoresis of the haemoglobin revealed haemoglobin Eand a trace of foetal haemoglobin. The amount of alkali-resistant haemoglobin was 6% of the total amount. Noabnormalities were found in the urine. The faeces containeda few eggs of Trichocephalus dispar, no other parasites.
Discussion
It is not strictly permissible to describe a person ashomozygous for a gene responsible for an abnormal
haemoglobin unless the diagnosis by electrophoresis hasbeen confirmed by a study of his family (Lehmann et al.
Fig. S-Paper electrophoresis at pH 8-6 of haemoglobin of case 2, case 3,and family.
1956, Chernoff et al. 1956). It is known that the labora-tory findings in sickle-cell/thalasssæmia disease may beindistinguishable from those found in homozygous sickle-cell disease. Analogous to this, certain cases of hæmo-
globin-E/thalass2emia disease indistinguishable fromhomozygous haemoglobin-E disease might also be found.In such cases only study of the family would be conclusive.In none of the few cases of pure haemoglobin-E disease
published up to now were both parents studied. There-fore the homozygosity of the cases was not entirelyproved.
In all three of our cases the diagnosis by electro-nhoresis was Dure hæmoglobin-E disease. In case 1 the
diagnosis was confirmed by a
family study, both parents beingcarriers of haemoglobin-E trait,and no thalassaemia factor beingfound in this family.The parents of case 2 were
not examined ; in case 3 both
parents were carriers of hæmo-globin-E, but a thalassæmiafactor in the father could not be
entirely ruled out.As one of us (Lie-Injo Luan
Eng 1956) has pointed out, in
comparing haemoglobin types oneshould compare them in similarconditions. The pure form of a haemoglobin typeshould not be compared with the trait form, becausethis can lead to a wrong conclusion (fig. 2). This is
especially important when one has to differentiate twohaemoglobin types showing only a slight difference in
mobility-e.g., haemoglobin E and haemoglobin C at
pH 8.6. If one compares the mobility of the haemoglobinof case 1 with haemoglobin C found in the control traithaemoglobin C (fig. 2), the wrong conclusion could bereached that the haemoglobin found in case 1 was hemo-globin C. However, both parents and the grandmotherof case 1, who were trait carriers of the abnormal haemo-globin, had a pathologic component in their haemoglobinwith exactly the same mobility as that of haemoglobin E,being slightly greater than that of haemoglobin C. How-ever, the relative mobilities seen on paper electrophoresisare not entirely constant, owing to factors which we donot yet understand. Small differences are thereforedifficult to assess, and one must repeat the procedureseveral times before one can be sure of the constancy ofthe differences in relative mobility on paper electro-phoresis. Electrophoresis at an acid pH will help inmaking an accurate diagnosis. This has been pointed outby H. A. Itano (personal communication). Also at pH

23
6.5 one should compare haemoglobin solutions undersimilar conditions. We found that, at this pH, the pureform of haemoglobin E seems to have a mobility slightlygreater than that of haemoglobin E found in the traitcondition. Study by open-boundary electrophoresis ismore accurate, but this method is available only in a fewlaboratories and is impracticable for the mass survey.The clinical picture in case 1 resembled that described
in the cases of Chernoff et al. (1956). She complained ofeasy fatigability and tiredness, her spleen and liver wereslightly enlarged, and she had slight anaemia. Case 2resembled the cases described by Lehmann et al. (1956).He was entirely healthy and led a very active life withoutany complaint. His spleen was only just palpable. Therewas not the slightest anemia. Case 3 also was healthyand had no anaemia. In all our cases the blood showed
microcytosis and the M.c.H.c. was normal. The resistanceof the erythrocytes to hypotonic saline solution wasincreased. In all three cases there was no clear evidenceof increased haemolysis. In cases 1 and 2 the amount offretal haemoglobin was not increased. In all the publishedcases the amount of alkali-resistant haemoglobin wasslightly increased, ranging from 2% to 6-4% of the totalamount of haemoglobin (Chernoff et al. 1956, Lehmannet al. 1956). Case 1 had only a few target cells in herperipheral blood. Other workers have always foundnumerous target cells in the peripheral blood of cases ofpure haemoglobin-E disease.The two other conditions associated with haemoglobin E
in the blood are the trait haemoglobin E and haemoglobin-E/thalassaemia disease. In a study of 15 families it wasfound by one of us (Lie-Injo Luan Eng 1956) that theheredity of hemoglobin E fits the theory that this geneis transmitted as a mendelian dominant factor, andthat this gene is an allele of the gene for normal hoemo-
globin. Carriers of the trait are heterozygous for thegene for haemoglobin E. They are clinically asymptomatic.But hsematological study of 36 carriers of haemoglobin-Etrait by Chernoff et al. (1956) and of 44 by Lie-InjoLuan Eng (1956) revealed that many of the trait carriersshowed slight microcytosis of the erythrocytes, and thatthe resistance of the red blood-cells to hypotonic salinesolution was sometimes increased.The gene for haemoglobin E has been found in many
countries in South East Asia and plays an importantrole in this part of the world. The distribution of
haemoglobin E in Asia has been discussed by Lehmannet al. (1956). In a survey of about 4000 samples of bloodfrom different islands in Indonesia haemoglobin E wasfound on all the islands examined (Lie-Injo Luan Eng1956). On the island of Java the approximate incidenceis 3%. On the island of Madura, however, the incidenceis much higher-about 17% (Lie-Injo Luan Engunpublished).Haemoglobin-E/thalassaemia disease has been described
especially by Chernoff et al. (1956) and by Lie-InjoLuan Eng (1956). Both clinical and laboratory findingswere very variable. Different haemoglobin patterns-namely, E + F, E + A, and E + A + F-were foundby Lie-Injo Luan Eng (1956). The syndrome was verylike that found in Cooley’s anaemia.
REFERENCES
Chernoff, A. I., Minnich, V., Chongchareonsuk, S. (1954) Science,120, 605.
— — Nanakorn, S., Tuchinda, S., Kashemsant, C., Chernoff,R. R. (1956) J. Lab. clin. Med. 47, 455.
Graff, J. A. E., Ikin, E. W., Lehmann, H., Mourant, A. E., Parkin,D. M., Wickremasinghe, R. L. (1954) J. physiol. 127, 41P.
Itano, H. A., Bergren, W. R., Sturgeon, P. (1954) J. Amer. chem.Soc. 76, 2278.
Lehnann, H., Story, P., Thein, H. (1956) Brit. med. J. i, 544.Lie-Injo Luan Eng (1955a) Nature, Lond. 176, 469.
— (1955b) Docum. Med. geogr. trop. 7, 273.— (1956) Thesis, University of Indonesia.
Singer, K., Chernoff, A. I., Singer, L. (1951) Blood, 6, 413.Smith, E. W., Conley, C. L. (1953) Bull. Johns Hopk. Hosp. 93, 94.
CUSHING’S SYNDROME WITH CARCINOMAOF BRONCHUS
AND WITH FEATURES SUGGESTING CARCINOIDTUMOUR
M. T. HARRISONM.B. Belf.
HOUSE-SURGEON, ROYAL VICTORIA HOSPITAL, BELFAST
D. A. D. MONTGOMERYM.B.E., M.D. Belf.,
M.R.C.P.PHYSICIAN TO OUTPATIENTS,ROYAL VICTORIA HOSPITAL
A. S. RAMSEYM.B.E., M.D. Belf.,
M.R.C.P.
PHYSICIAN, LAGAN VALLEY
HOSPITAL, LISBURN
J. H. ROBERTSONM.B. Belf.
ASSISTANT LECTURER IN
PATHOLOGY, QUEEN’SUNIVERSITY, BELFAST
R. B. WELBOURNM.A., M.D. Camb.,
F.R.C.S.
READER IN SURGERY,
QUEEN’S UNIVERSITY
Cushing’s syndrome is usually associated with hyper-plasia, hyperfunction, or tumours of the adrenal cortex,whose secretions are responsible for the clinical andmetabolic features of the disease. A few cases, however,have been described in association with carcinoma of thebronchus, pancreas, or thymus (Thorne 1952), cerebrallesions (Zondek 1923), diseases of the liver (Bongiovanniand Eisenmenger 1951), and tumours of the ovaries.The relation between the syndrome and these lesions isnot understood. The patient whose case we report heresuffered from Cushing’s syndrome and a carcinoma of thebronchus, and showed other unusual features whichsuggested the presence of a functioning carcinoid tumour.
Case-reportA woman, aged 55, wa3 first seen by one of us (A. S. R.)
at the Lagan Valley Hospital, inSeptember, 1955, complaining ofpustular spots on the legs andarms, and growth of hair on theface. Her menstrual periods hadceased 2 years previously andthere were no past illnesses. Hermother had had diabetes mellitus,but there was no indication thatthis might have been due to
Cushing’s syndrome. She had astout body and thin limbs, andthere were pads of fat in the supra-clavicular triangles, axillae, groins,and cervico-dorsal region. Therewere no red striae on the skin, but3 weeks later one appeared onthe abdomen and after another 10weeks there were several. The
blood-pressure at this time variedbetween 155/80 and 175/90 mm.Hg.She was regarded as an early case
of Cushing’s syndrome and admit-ted to the Royal Victoria Hospital,Belfast, on Jan. 6, 1956. In addi-tion to the previous complaints,she mentioned diarrhoea and
swelling of the ankles and saidthat her hair had become darkerand had been falling out for 6months. On questioning she saidthat her face had become fatterin the past few months and thatshe was a little short of breathon exertion.
i On examination (see figure) the
face was rounded, the cheek had a cyanosed flush, and therewas moderate hair-growth on the upper lip, sides of face, andchin. An acneiform rash was present over the limbs andabdomen and there were several purple striae on the abdomen.There was marked thoraco-lumbar kyphosis and the blood-pressure was 170/100 mm. Hg. Dullness and decreased air-
entry were found at the base of the right lung. The liver