Embed Size (px)
Citation preview

Br. J. Cancer (1981) 43, 417
NEW APPROACHES TO THE MANAGEMENT OF PATIENTS WITHNON-HODGKIN'S LYMPHOMA OF HIGH-GRADE PATHOLOGYFIRST GAORI)ON HAMILTON-FAIRLEY MEMORIAL LECTURE*
PROFESSOR DEREK CROWTHERCRC Departnent of Medical Oncology, Christie Hospital and Holt Radium Institute;
Manchester M20 9BX
OF ALL THE LECTURES I have been askedto give, I count this one as my greatesthonour. Gordon Hamilton-Fairley was apersonal friend, colleague and mentor formore than 10 years until he was killed sotragically by a terrorist bomb in 1975. Hewas the father of Medical Oncology inBritain and played an important part inencouraging the development of academicdepartments of Medical Oncology not onlyin St Bartholomew's Hospital where hisown unit was based, but also at the RoyalMarsden Hospital and other centres inLondon. His efforts led to Medical Onco-logy becoming an established subspecialtyin Medicine and the development of severalmajor academic departments in the speci-alty outside London (e.g. Manchester,Glasgow, Edinburgh and Southampton).There is now a sound base for training anddoctors of high calibre with a strong back-ing in clinical oncology and research arenow available to fill new posts in MedicalOncology. Such posts are undoubtedlyneeded in view of the increasingly import-ant role of systemic treatment in im-proving the survival of patients withcancer. The number of posts must betailored to the relative work load andresearch requirements in chemotherapy,radiotherapy and surgery. My own view isthat, initially, such posts should be intro-duced in close association with existingDepartments of Radiotherapy in ourmajor cities and, following this, physicianswith a special interest and training in
Medical Oncology could be appointed tolocal district general hospitals to improvechemotherapy services in the region. Thisis the pattern of development which isbeing encouraged in the north-west ofEngland.My talk concerns new approaches being
made in the management of patients withnon-Hodgkin's lymphoma (NHL) of high-grade pathology (i.e. those composed oflarge cells arranged in a diffuse pattern)and I will colour my presentation withdata from studies being undertaken inManchester, in both the clinic and thelaboratory.A recent publication of the Office of
Population Censuses and Surveys (1980)is rather disturbing. The 5-year survivalof patients with NHL in England andWales has not improved significantly overa period of almost 10 years, in spite ofnotable improvements in chemotherapy(Table I). The overall 5-year survival ofabout 300/o must be considered in thecontext of an expected 50%o in thesubgroup with low-grade histology treatedin a palliative manner with low-dosesingle-agent chemotherapy and radio-therapy. This means that patients withhigh-grade histology are faring badly, andthe object of the first part of my talk is tosuggest that the new approaches nowbeing adopted for this unfavourable groupof patients in special centres should leadto an improvement in survival in thecountry as a whole.
* Delivered at the joint meeting of the British Association for Cancer Researcht and(i Section of Oncology,Royal Society of Medicine, December 11th 1980.
30
D. CROWTHER
TABLE I.-Cancer statistics survival, Eng-land and Wales (OPCS, 1980)
Non-Hodgkin's Lymphoma (NHL)
Year Diagnosis1964-66 RSa/LSa*
Other
1971-73 RSa/LSa
Other
SexM
FM
FM
FM
F
No. regis-tered29282319556553
27852435926777
5-yr sur-vivals (0%corrected)
24-326-341-939.930-131-742-842-7
* Reticulo-sarcomas and lymphosarcomas.
In NHL patients careful documentationof the extent of disease is important indetermining the part to be played by localtreatment such as surgery or radiotherapy,and is necessary in defining the role ofchemotherapy. Although some patientscan be cured by radiotherapy or surgeryalone, not more than 10% of all patientsachieve long-term relapse-free survivalfollowing local treatment alone. Chemo-therapy, therefore, has a major role inthese diseases.
CHEMOTHERAPY FOR GENERALIZEDDISEASE
Combination chemotherapy used inter-mittently has proved to be of greatervalue than single-agent chemotherapy inpatients with high-grade lymphomas andcomplete remissions are now obtained in40-70% of treated patients. Several retro-spective studies have been reported re-
cently showing an advantage in usingAdriamycin-containing regimens in termsof rate of complete remission and relapse-free survival (Cabanillas et al., 1978;Jones et al., 1979; Johnson et al., 1979;MacKintosh et al., 1980). The role ofcyclophosphamide in the induction pro-gramme is less clear, with at least one
report showing an advantage to an
Adriamycin-containing combination with-out cyclophosphamide (Bodey & Rod-riguez, 1978).The duration of relapse-free survival
after induction of complete remission is
dependent upon the histological subtype,with those classified as diffuse "histio-cytic" lymphomas using the Rappaportclassification having long-term relapse-free survival compared with a continuingrelapse pattern for those classified asdiffuse poorly differentiated lymphocytic(Schein et al., 1975).The group at the National Cancer
Institute, Bethesda, reported a completeremission rate in 56 patients with diffusehistiocytic lymphoma of 47%. Althoughthe overall median survival was poor (14months), one third of the patients sur-vived in complete remission at 5 years.Very few patients relapsed if they werestill in remission one year after inductionof remission using combination chemo-therapy, and the suggestion was madethat these patients could well be cured(Fisher et al., 1977).Most reports have involved combination
chemotherapy given intermittently, butthe poor median survival illustrates thepropensity for early relapse and death inmore than half the patients. The recog-nition that treatment failure frequentlyoccurs early in the first few months ofinduction chemotherapy, with failure toachieve complete remission and a tendencyto relapse between courses, led to theintroduction of a more continuous form ofchemotherapy using combined chemo-therapy involving a weekly schedule atSt Bartholomew's Hospital in 1972. Thecombination was similar to that successfulin treating acute lymphoblastic leukaemia,and involved vincristine, prednisolone,Adriamycin and L-asparaginase (OPAL).We recently reported the results of treat-ing a small number of patients with diffusehistiocytic lymphoma using this approach(Lister et al., 1978). All 10 patients withStage III disease and 6/11 patients withStage IV disease achieved a completeremission, and preliminary results showedpromising long-term relapse-free survival.The Manchester Lymphoma Group has
addressed the problem of early failureusing a similar approach (Blackledge et al.,1980b). More than 18 months of further
418
MANAGEMENT OF NON-HODGKIN'S LYMPHOMA
follow-up is now available for patients inthis study, and updated results are in-cluded here. Induction chemotherapy con-sisted of prednisolone (40 mg orally dailyfor 6 weeks), vincristine (2 mg weekly i.v.for 6 weeks) and 3 i.v. injections ofAdriamycin (50 mg/M2) at 2-weeklyintervals (VAP). In addition, local radio-therapy was given to areas of residual orpreviously bulky disease in an attempt toreduce the relapse rate in these areas.Subsequent chemotherapy involved a 2-year programme of continuing therapyusing cyclophosphamide (200 mg/M2),methotrexate (10 mg/Mi2 orally weekly)and 6-mercaptopurine (50 mg/M2 orallydaily). The doses were tailored to maintainthe white blood count 3000-3500/pl.One hundred and seven patients entered
the study between 1975 and 1980. Therewere 19 patients with Stage II abdominalinvolvement and massive nodal disease;11 of these had gastrointestinal involve-ment. Eighteen patients had Stage IIIdisease and 70 Stage IV disease. The agerange was 19-70 years and the overallcomplete remission rate was 62%. Twentyfive patients achieved a good partial re-mission, with only minimal residualdisease remaining. Six further patientshad a remission with a tumour regressionof > 50%, and only 10 patients wereclassified as failures (< 50% regression).A multivariate analysis of factors affecting
TABLE IT.-Multivariate analysis of vari-ables influencing the probability of com-plete remission in 107 patients withlymphomas of diffuse pathology (NHD4/1Study, Manchester Lymphoma Group,October 1980)
VariableNoneAlkaline
phosphatase+ Age groups+ B symptoms+ Marrow+ Sex
Scaled De-deviance crease134-6
120-7115-0109-1101-897-7
13-95-75-97-34-1
Favour-able
P feature
0-00020-0170-0150-0070043
NormalYoungAbsentNormalFemale
A step-up procedure was used for the analysis.
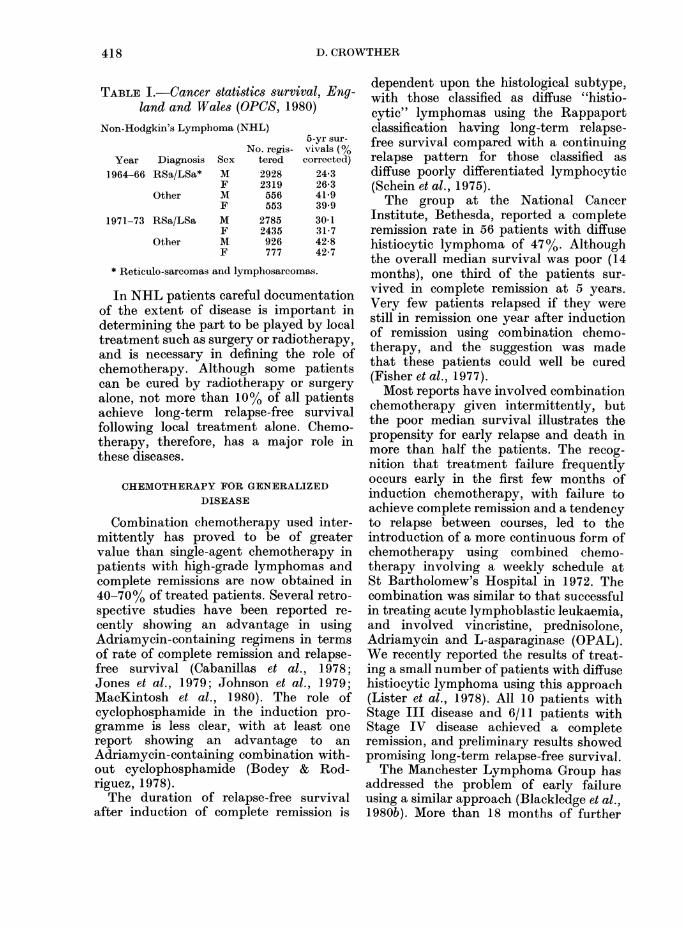
probability of achieving a complete re-mission revealed 5 factors of independentsignificance (Table II). Increased serumalkaline phosphatase, increasing age, pres-ence of B symptoms, marrow involve-meiit and male sex were all associatedwith a significant reduction in the prob-ability of a complete remission. There wasno difference in complete-remission ratebetween patients with diffuse histiocyticand diffuse poorly-differentiated lympho-cytic lymphoma. The median duration offollow-up was 4 years, and the overallsurvival in the 107 patients is shown inFig. 1. Survival was related to a numberof pretreatment variables: the influenceof stage B symptoms, gastrointestinaltract involvement, overall assessment ofliver function, alkaline phosphatase,serum albumin, histology, peripheral-blood lymphocyte count and haemoglobinwere all assessed individually in relationto survival, and following this a Cox re-gression analysis was performed. Four
100-
80
60-0
.C ',
0 1 2 3 4 5Years
FiG. 1. Overall survival of 107 patientswith diffuse histiocvtic, diffuse poorlvdifferentiated lymphocytic, diffuse mixedand diffuse undifferentiated lymphomas,trcated with the VAP protocol.
I 1,
419
1). CROWTHER
TABLE III.-Cox regression analysis of variables influencing survival in 107 patients withlymphoma of diffuse pathology
LogVariable likelilhood Increase T) Unfavoourable feature
Albumin 8-45 8-45 0 00004 Low albumin+Stage 12 60 4-15 0 004 Stage IV+Alkaline phosphatase 15-21 2-61 0-023 Raised+ Pathology 17-14 1-93 0.05 Histology otlier tlha
diffuse histiocvticEachi of the 4 variables hias a significant effect on survival after a(djustment for the other 3.
(I 'I OId B I~ O a:alllo
en~~~~~~~~~~~wg uLn-t0
Cl)
40-
Stag IV n=70
20-
0 1 2 3 4 5Years
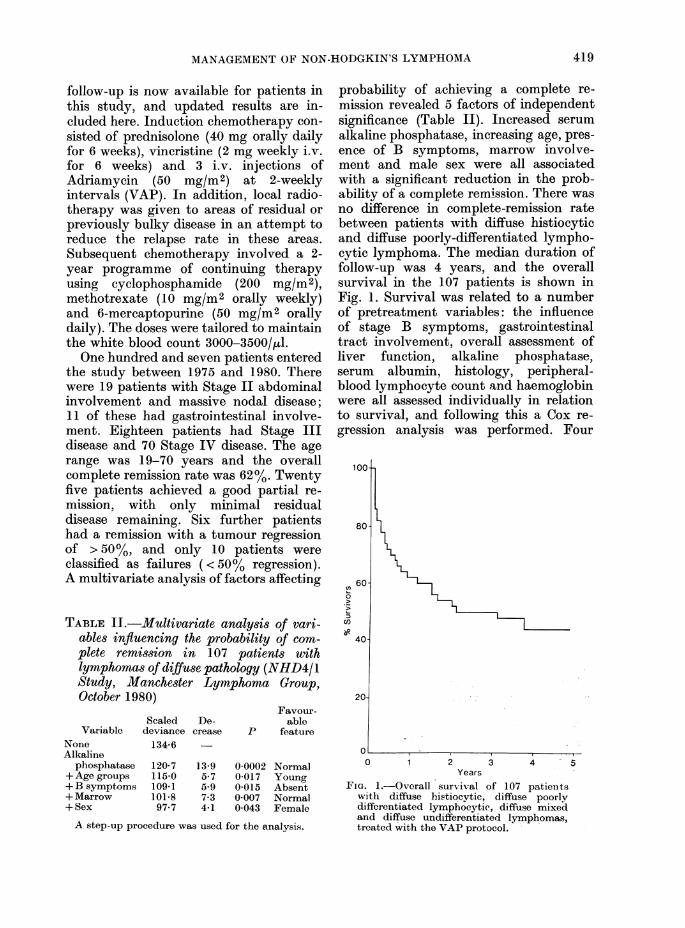
FIG. 2. Survival related to stage (P = 0 003).Stage II patients were a group withabdominal or gastrointestinal involvement,but no evidence of spread outside theabdomen.
variables, including a low serum albumin,Stage IV disease, high serum alkalinephosphatase and diffuse histiocytic path-ology, had a significant effect on survivalafter adjustment for the other 3. None ofthe other pretreatment variables had astatistically significant effect on survivalafter adjusting for the effects of these 4variables (Table III). Patients with ab-dominal Stage II disease did particularlywell under this treatment policy, withmore than 70% surviving, relapse-free,beyond 4 years (Fig. 2). Survival was alsoclosely related to remission status whichwas of individual prognostic significance,
Cl,0
Cl)0
CR n=66
PR n=6
I] F n=10
0 1 2 3 4 5Years
FIG. 3.-Survival related to remission status(P < 0-00001). Complete remission (CR) wasdefined as resolution of all evidence oflymphoma. Good partial remission (GPR)included patients with > 90% reduction intumour masses. Partial remission (PR) wasdefined as > 50% but < 90% reductioni inthe mass of disease and failure (F) was< 50% reduction in the mass of disease.
with 60% of those achieving a completeremission surviving for more than 4 years.Failure to achieve a complete remissionwas associated with a poor survival(Fig. 3).There was a statistically significant
difference in survival (P=0 001) andrelapse-free survival (P = 0.01) in patientswho received bulk radiotherapy afterinduction chemotherapy. The improved
420
AMANAGEMENT OF NON-HODGKIN'S LYMPHOMIA
surxvival seen in patients receiving radio-therapy was still significant after adjust-ment for the effects of the 4 pretreatmentvariables in Table III, but this treatmentwas not randomized, and the data mustbe interpreted with caution. The resultssuggest that a prospective randomizedstudy of radiotherapy following inductionchemotherapy could be well worthwhile.
Skarin and his colleagues from Boston(Skarin et al., 1980) have recently reporteddata on another frequent chemotherapyschedule which lends support to the sug-gestion that this approach may lead toimproved complete remission rates andlong-term relapse-free survival. A groupfrom Seattle (Sullivan et al., 1979) havealso suggested that radiotherapy couldhave a useful role following initial chemo-therapy and one third of the patientscompleted their remission using radio-therapy in their series. The radiotherapygiven included whole-body irradiation ifthe marrow was involved, and thisapproach, which was more aggressive thanour own, may have contributed to thehigher complete-remission rate. The con-tribution of these different forms of radio-therapy to the improved survival inpatients with diffuse lymphomas deservesfurther study under controlled conditions.The appreciation that patients with
some forms of diffuse pathology have acontinuous relapsing pattern and poorsurvival in spite of a high apparent initialremission rate is disappointing. A moreintensive approach using combinedchemotherapy and radiotherapy may leadto further improvement in survival, butthis remains to be tested. In my view, aradical approach following the inductionof remission is now required. In contrastwith diffuse histiocytic lymphoma, wherehigh-dose irradiation frequently fails tocontrol local disease, recurrences in theirradiated area after moderate-dose radio-therapy for diffuse lymphocvtic or lympho-blastic disease are less common (Fuks &Kaplan, 1]975). Low-dose whole-bodyirradiation (1-3 Gy) has proved of somevaluie in the control of lymphocytic
lymphomas, though it is no better thanchemotherapy, and myelodepression con-tributes to difficulties in later treatment(Johnson et al., 1978). For these reasons,an approach using combined intensivecombination chemotherapy with higher-dose whole-body irradiation (1I Gy) forselected patients with diffuse poorlydifferentiated lymphocytic or lympho-blastic forms of lymphoma is now worthstudying. The marrow is frequently in-volved in such patients, and homologousmarrow transplantation would be re-quired. The promising results in patientswith acute leukaemia using this approachprovide a good argument for studying thisnew method of treatment in patients withdiffuse lymphoma in whom a, completeremission has been achieved.
Central nervous system (CONS) involvementInvolvement of the CNS is a well known
complication in patients with lymphoma.The reported incidence varies from < 5oto > 25%, with the highest incidence inpatients with diffuse histology. However,few patients are likely to benefit fromprophylactic treatment of the CNS, sincemost patients in whom CNS involvementdevelops present at a time of advancing oruncontrolled disease in other areas (Younget al., 1979). In addition, the routineprophylaxis may compromise the abilityto deliver adequate chemotherapy for cure.For these reasons, the careful selection ofpatients at high risk is mandatory ifprophylaxis is to be tested. Further studyof this topic is also warranted because thechoice of effective therapy for CNS diseaseis in doubt. Our policy in the ManchesterLymphoma Group is to avoid prophylactictreatment of the CNS until further dataaccrue on the incidence of CNS relapse inpatients who are otherwise in completeremission.
CHEMOTHERAPY FOR LOCALIZED DISEASE
Localized or regional radiotherapy mayproduce prolonged relapse-free survival inabout half the patients with lymphomas
421-
D. CROWTHER
of diffuse pathology presenting withclinically localized disease (CS I/II).Patients with diffuse histology constituteabout 80% of the total presenting withlocal disease. A recent analysis of datafrom St Bartholomew's Hospital showed a
50% relapse-free survival for 29 patientswith diffuse poorly-differentiated lympho-cytic, compared with 34% of 32 patientswith diffuse histiocytic histology (Timothyet al., 1979). Their results are similar toother recently published series fromCanada (Bush et al., 1979) and the UnitedStates (Chen et al., 1979), and are con-
sistent with the earlier literature (seereview, Bonadonna et al., 1976). The re-
lapse rates for patients with CS II diseaseare higher than for CS I disease. Analysisof local failures shows that nearly all in-volved diffuse tumours and, in contrastwith nodular tumours, these can provedifficult to control, even with high-doseirradiation (Fuks & Kaplan, 1975). Nearlyall relapses, however, occur by wide dis-semination, and chemotherapy thereforehas an important role in this context inpreventing the growth of tumour in thesedisseminated sites and the recurrence oftumour in areas treated previously withradiotherapy.The Milan group have reported their
5-year follow-up data of a controlled ran-domized trial of combination chemo-therapy used as an adjuvant after radio-therapy for pathological stage (PS) I/IINHL (Monfardini et al., 1979). After treat-ment with regional radiotherapy, patientsin complete remission were randomized toreceive either no further therapy or 6cycles of CVP (cyclophosphamide, vin-cristine and prednisolone). A total of 96patients were evaluable. At 5 years fromcompletion of irradiation, the relapse-freesurvival was 46% after radiotherapy and72% after radiotherapy with CVP (P=0.005). The corresponding findings for theoverall survival calculated from the begin-ning of irradiation were 55% and 83%respectively (P= 0.03). The favourableeffect of adjuvant chemotherapy on re-
lapse-free survival was statistically signifi-
cant, irrespective of stage and clinicalpresentation in the subgroup with diffusehistology which represented more than70% of the entire series. In contradistinc-tion, patients with nodular histologyshowed no improved relapse-free survivalafter 6 cycles of CVP. In patients relapsingafter radiotherapy alone, salvage therapyfailed to induce a high incidence of seconddurable remissions. This study is importantin that 98% of the patients had patho-logical staging (26% by laparoscopy and74% by laparotomy). Glatstein and hiscolleagues from Stanford (Glatstein et al.,1977) reported a study in which they failedto observe an improvement in overall sur-vival or relapse-free survival in PS 1/11patients with high-grade histology usingtotal nodal irradiation with CAT (cytosinearabinoside, Adriamycin and thioguanine)for diffuse histiocytic lymphoma, andCVP for all other histologies. This was alsotrue for the study reported by Panahonet al. (1977). The reason for these differentresults may well be related to the differ-ences in the radiotherapy rather than thechemotherapy used in the studies.A study from Stockholm supports the
findings of the Milan group (Landberg etal., 1979). Fifty five patients with nodularor diffuse lymphoma of CS I/II wererandomized for 9 cycles of CVP afterradiotherapy; the relapse-free survival at30 months was 41% for patients withoutand 86% for patients with adjuvantchemotherapy (P=0 02). Survival wasthe same for both treatment arms, being90% at 30 months. Analysis of the sub-groups showed that adjuvant chemo-therapy significantly prolonged the re-lapse-free survival in diffuse histiocyticlymphoma, but there were only 20evaluable patients in this group. Thisstudy suffers from the defect of smallnumbers of patients and short follow-up.The Manchester Lymphoma Group is
conducting a study comparing the effectsof two forms of combination chemo-therapy as an adjuvant after radiotherapyfor nodal stages I/II disease. Patients withStage IE disease were not included since
422
MANAGEMENT OF NON-HODGKIN'S LYMPHOMA
these have a relatively good relapse-freesurvival after radiotherapy alone. Thechemotherapy was either 6 courses of acombination without Adriamycin (CMOPP-cyclophosphamide, vincristine, procarb-azine and prednisolone) or the regimenused by the group for advanced stages ofhigh-grade lymphoma (vincristine, Adria-mycin and prednisolone for 6 weeks fol-lowed by 2 years oral 6-mercaptopurine,cyclophosphamide and Methotrexate).Only 5/34 patients have relapsed (medianfollow-up 21 years) with a 3-year relapse-free survival of 88%. As yet, there is nosignificant difference between the treat-ment arms, since the number of events istoo low.The recognition that chemotherapy
alone can produce long-term relapse-freesurvival in patients with Stage III/IVdiffuse histiocytic lymphoma, and thatadjuvant chemotherapy prolongs survivaland relapse-free survival in carefullystaged localized diffuse histiocytic lymph-oma has prompted the use of chemo-therapy alone in patients with Stage I/IIlymphoma of this type. Miller & Jones(1979) retrospectively analysed a series of22 patients with diffuse lymphoma, StagesI/II, treated with chemotherapy alone (14patients) or chemotherapy with localirradiation. All 22 patients achieved acomplete remission and remained alive(median survival 27 + months). Twentyone patients remained continuously freeof disease, with a median relapse-freesurvival from completion of chemotherapyof 23 + months. Most patients receivedCHOP chemotherapy (cyclophosphamide,Adriamycin, vincristine and prednisolone).
It seems that chemotherapy now has anestablished role in the treatment of Stage1/11 lymphomas of high-grade histology.
STAGING
The studies I have already mentionedemphasize the importance of staging. Afurther example of the important role ofcareful staging can be obtained from astudy of patients presenting with gastro-
intestinal lymphoma. A recent retro-spective series of patients with gastro-intestinal lymphoma presenting at theChristie Hospital, Manchester, has beenanalysed by our group (Blackledge et al.,1979). There were 104 patients with fulldetails of the surgery obtained. Althoughthe median survival was only 15 months,35% were alive and well at 10 years. Thetumour type (histology, site and whethersingle or multiple) extent of lymph-nodeinvolvement and the presence of localextension to adjacent organs, perforationwith peritonitis or distant metastases wereof considerable prognostic importance.The Ann Arbor staging classification wasinadequate for this group of patients, anda new staging system for gastrointestinallymphoma has been proposed, which hasprognostic significance and can be used toselect appropriate poor prognostic groupsfor chemotherapy. It was clear from thedata that patients fared much better iftumour excision was complete. Each ofthe patients had initial surgery involvinglaparotomy, and all apparent tumour wasremoved in 41 patients. This includedremoval of locally involved nodal massesand tumour which had spread to adjacenttissues. The group had a much better sur-vival than the remainder with either in-complete tumour removal or merelytumour biopsies (P=0.0005). Of the 49patients who had complete removal of thetumour, only 11 had a single tumour con-fined to the gut; all the others had eitherlocal nodes involved or spread to adjacenttissues. Considering only Stage II patientswith disease extending outside the gastro-intestinal tract, there was still a highlysignificant difference between the patientswith complete and incomplete removal ofthe tumour (P = 0.004). Cure is a distinctpossibility after surgery alone for patientswith gastrointestinal lymphoma, buttumour removal must be complete. Othergroups with incomplete removal have apoor survival, in spite of the addition ofradiotherapy, and early chemotherapy isthen of recognizable value.
Unlike most forms of nodal lymphoma,
423
D. CROIITHER
gastrointestinal lymphoma has a propen-sity for remaining apparently localized tothe gut wall and draining lymph nodes(gastric or mesenteric) allowing a moder-ate proportion of cures by surgery alone.Peripheral nodes become palpable late inthe history of the disease, if at all, and inthis series, only two patients had a palp-able spleen at presentation. Only 20% hadwidespread nodal disease; involvement ofadjacent organs after spread through thebowels was more common than indirectmetastatic spread to distant organs, andthe bulk of disease remains confined to theabdomen for most of its course. For thesereasons, the Ann Arbor classification,which is so useful for nodal Hodgkin'sdisease, is less appropriate for gastro-intestinal NHL. A study of the pattern oflymphoid-cell migration can offer anexplanation of the difference betweengastro-intestinal lymphoma and otherforms of lymphoma, and will be discussedlater.
Wt'hole-body scanning with computedtomography (CT)
Surgical staging is not recommended formost patients presenting with NHL,since laparotomy is potentially dan-gerous and generalized disease can usuallybe documented by conventional clinicalstaging. Treatment decisions are usuallybased on staging procedures which avoidlaparotomy in this group of patients. CThas enabled a more accurate documenta-tion of the pattern of disease at presenta-tion than could be achieved by conven-tional clinical staging alone, and thereforeplays an important part in initial staging.Its advantages over abdominal lympho-graphy have previously been documented(Crowther et al., 1979). In Manchester,whole-body CT has replaced abdominallymphography in lymphoma patients.At presentation and clinical relapse, CT
scanning detects unsuspected disease in ahigh proportion of patients with lymph-oma, and has an important influence ontreatment policy. The evaluation of re-sponse to chemotherapy and the detection
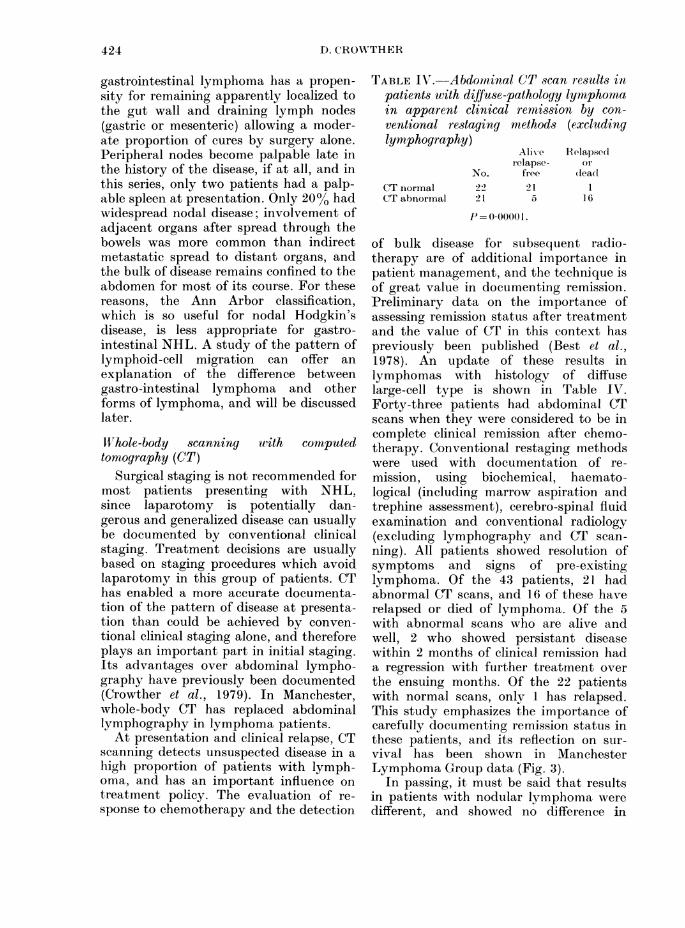
TABLE IN'.-Abdominal C(T scan results inpatients with diffuse-pathology lymphomain apparent clinical remission by con-ventional restaging methods (excludinglymiphography)
No.CT normal 22CT abnormal 21
AlivNerelapse-
free215
Eelapsedorlead
16
P= 0 0000 1.
of bulk disease for subsequent radio-therapy are of additional importance inpatient management, and the technique isof great value in documenting remission.Preliminary data on the importance ofassessing remission status after treatmentand the value of CT in this context haspreviously been published (Best et al.,1978). An update of these results inlymphomas with histology of diffuselarge-cell type is shown in Table IV.Forty-three patients had abdominal CTscans when they were considered to be incomplete clinical remission after chemo-therapy. Conventional restaging methodswere used with documentation of re-mission, using biochemical, haemato-logical (including marrow aspiration andtrephine assessment), cerebro-spinal fluidexamination and conventional radiology(excluding lymphography and CT scan-ning). All patients showed resolution ofsymptoms and signs of pre-existinglymphoma. Of the 43 patients, 21 hadabnormal CT scans, and 16 of these haverelapsed or died of lymphoma. Of the 5with abnormal scans who are alive andwell, 2 who showed persistant diseasewithin 2 months of clinical remission hada regression with further treatment overthe ensuing months. Of the 22 patientswith normal scans, only I has relapsed.This study emphasizes the importance ofcarefully documenting remission status inthese patients, and its reflection on sur-vival has been shown in ManchesterLymphoma Group data (Fig. 3).
In passing, it must be said that resultsin patients with nodular lymphoma weredifferent, and showed no difference in
424
MTANKAGEMENT OF NON-HOI)GKIN'S LYMIPHOAIA
ilelapse-free survival or overall survivalbetween those with abnormal scans andpatients with no evidence of disease onCT scans (unptublished data).An accurate documentation- of sites of
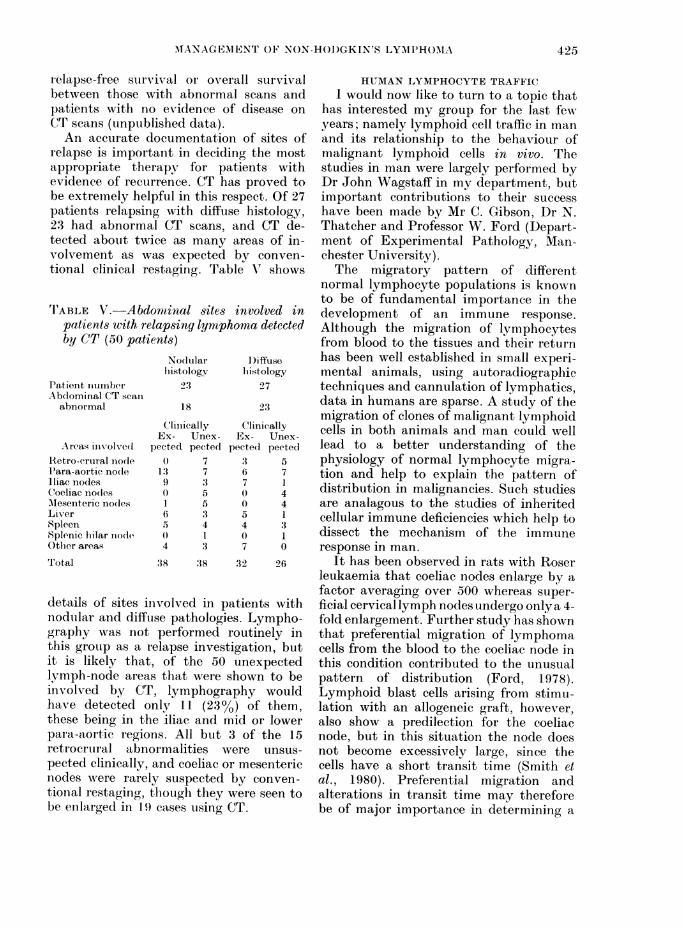
relapse is important in deciding the mostappropriate therapy for patients withevidence of recurrence. CT has proved tobe extremely helpful in this respect. Of 27patients relapsing with diffuse histology,23 had abnormal CT scans, and CT de-tected about twice as many areas of in-volvement as was expected by conven-tional clinical restaging. Table V' shows
rIABLE V. Abdomtinal sites involved inpatients with relapsing lymphoma detectedby CT (50 patients)
I'atient iiumnberAbdominal CT scan
abnormal
.Areas involved
1Retr o-erural nodleP'ara-aortic no(leIliac nodesCoeliac no(lesM\lesenteric no(lesLiverSpleeIn
Splenic lilar niode
Otlher areas
Total
Nodularhiistology
23
18
C'linicallyEx- Unex-
pected pectecl0 7
1'3 79 3() 51 56 :35 4o) I4 :3
38 38
I)iffusehistology
27
ClinicallyEx- Unex-
pected pected3 56 77 1
40 45 14 3() 17 0
32 26
details of sites iiivolved in patients withnodular and difftse pathologies. Lympho-graphy was not performed routinely inthis grouip as a relapse investigation, butit is likely that, of the 50 unexpectedlymph-node areas that were shown to beinvolved by CT, lymphography wouldhave detected only 11 (23o%) of them,these being in the iliac and mid or lowerpara-aortic regions. All but 3 of the 15retrocrural abnormalities were unsus-pected clinically, and coeliac or mesentericnodes were rarely suspected by conven-tional restaging, though they were seen tobe enlarged in 1 9 cases using CT.
HUMAN LYMPHOCYTE TRAFFICI would now like to turn to a topic that
L has interested my group for the last fewyears; namely lymphoid cell traffic in manand its relationship to the behaviour ofmalignant lymphoid cells in vivo. The
I studies in man were largely performed byDr John Wagstaff in my department, butimportant contributions to their successhave been made by Mr C. Gribson, Dr N.Thatcher and Professor W. Ford (Depart-ment of Experimental Pathology, Man-chester University).The migratory pattern of different
normal lymphocyte populations is knownto be of fundamental importance in thedevelopment of an immune response.Although the migration of lymphocytesfrom blood to the tissues and their returnhas been well established in small experi-mental animals, using autoradiographictechniques and cannulation of lymphatics,data in humans are sparse. A study of themigration of clones of malignant lymphoidcells in both animals and man could welllead to a better understanding of thephysiology of normal lymphocyte migra-tion and help to explain the pattern ofdistribution in malignancies. Such studiesare analagous to the studies of inheritedcellular immune deficiencies which help todissect the mechanism of the immuneresponse in man.
It has been observed in rats with Roserleukaemia that coeliac nodes enlarge by afactor averaging over 500 whereas super-ficial cervical lymph nodes undergo only a 4-fold enlargement. Further study has shownthat preferential migration of lymphomacells from the blood to the coeliac node inthis condition contributed to the unusualpattern of distribution (Ford, 1978).Lymphoid blast cells arising from stimu-lation with an allogeneic graft, however,also show a predilection for the coeliacnode, but in this situation the node doesnot become excessively large, since thecells have a short transit time (Smith etal., 1980). Preferential migration andalterations in transit time may thereforebe of major importance in determining a
425
D. CROWTHER
pattern of disease distribution. Ford hassuggested that the high incidence ofcoeliac-node involvement in Hodgkin'sdisease could be explained by migrationof tumour cells via the blood to the liverand thence to the coeliac node, rather thanby retrograde lymphatic spread. In addi-tion, the use of lymphoma lines in experi-mental systems has indicated that theremay be differences in the high endothelialvenules of different tissues and organsthrough which lymphocytes migrate(Butcher & Weissman, 1980).Surface-marker and enzyme studies
have shown that the malignant cell inmost NHL patients is of lymphocytelineage. A study of the migratory be-haviour of these cells is therefore likely tobe of importance, not only in understand-ing more about the nature of the immunedeficiency in these patients, but also mayhelp explain the pattern of spread in thevarious types of malignant lymphoma.For example, an understanding of themigratory behaviour of lymphoid cellsoffers an explanation of the disease dis-tribution pattern seen in the gastro-intestinal lymphomas, where the mainbulk of disease remains confined to the gutand mesenteric node areas for a consider-able period in an appreciable proportionof patients. It is now recognized thatlymphocytes from gut-associated lymph-oid tissue have characteristic recirculationpatterns (see review by Hall, 1980).Immunoblasts and small lymphocytesobtained from efferent lymph draining thesmall intestine, preferentially home toregions adjacent to the lamina propria orto the small intestine (very few to periph-eral nodes or to the large intestine).Immunoblasts and small lymphocytesobtained from efferent lymph drainingperipheral nodes, on the other hand,preferentially home to peripheral nodesand spleen. Both T and B cells have sub-populations with migratory characteris-tics of peripheral nodal or intestinal type.It is to be expected that if the phenotyperesponsible for this migration pattern isconserved in patients with lymphomas
arising from gut-associated lymphoid cells,the bulk of tumour would be confined tothose areas for a prolonged period in spiteof blood involvement.Many of the techniques used for the
study of lymphocyte migration in experi-mental animals are invasive and impos-sible to carry out in man. The few humanstudies have mainly used Na251CrO4labelled lymphocytes; a technique withmany disadvantages. McAfee & Thakur(1976) showed that Indium-ill oxineconjugate was an efficient means oflabelling cells in vitro, and studies usingIndium-ill oxine as a lymphocyte labelhave demonstrated that more reliableinformation on lymphocyte kinetics inanimals systems can be obtained by thismethod (Rannie et al., 1977a,b; Chisholmet at., 1978; Issekutz et at., 1980; Sparshottet al., in preparation). Lavender et al.(1977) showed that external imaging of11lIn-labelled lymphocytes was possiblein man, and following studies in Man-chester, the method has an establishedvalue in following the traffic of normallymphocytes and their malignant counter-parts in man (Wagstaff et at., 1981a,b).
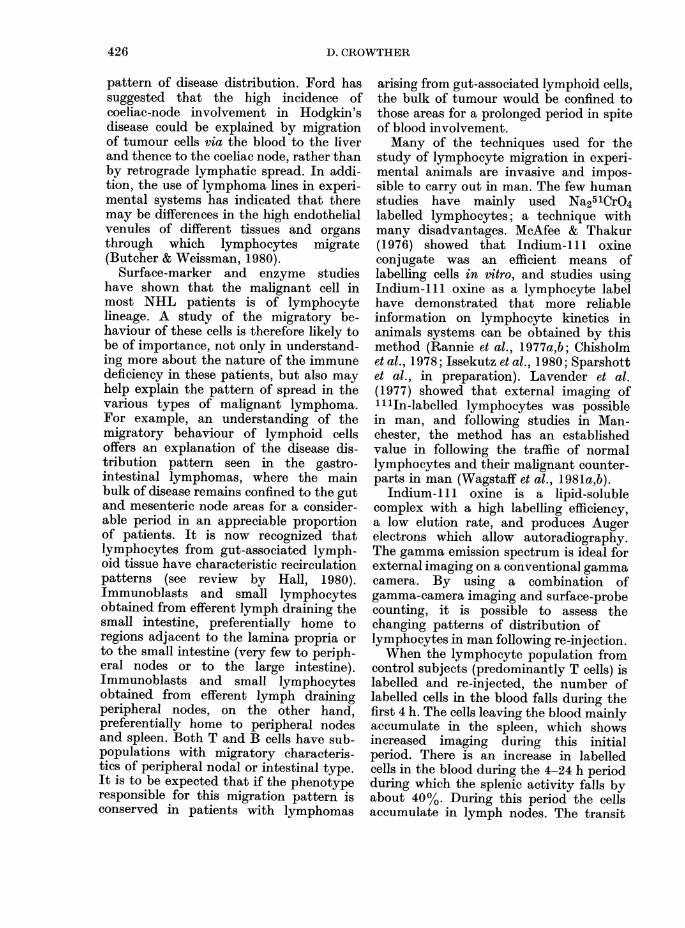
Indium-ill oxine is a lipid-solublecomplex with a high labelling efficiency,a low elution rate, and produces Augerelectrons which allow autoradiography.The gamma emission spectrum is ideal forexternal imaging on a conventional gammacamera. By using a combination ofgamma-camera imaging and surface-probecounting, it is possible to assess thechanging patterns of distribution oflymphocytes in man following re-injection.When the lymphocyte population from
control subjects (predominantly T cells) islabelled and re-injected, the number oflabelled cells in the blood falls during thefirst 4 h. The cells leaving the blood mainlyaccumulate in the spleen, which showsincreased imaging during this initialperiod. There is an increase in labelledcells in the blood during the 4-24 h periodduring which the splenic activity falls byabout 40%. During this period the cellsaccumulate in lymph nodes. The transit
426
MANAGEMENT OF NON-HODGKIN'S LYMPHOMA
00m
-c
Ea)
U,an
0
-CE-J
aR
O Normal Lymphocytes (65% T Cells)
A Heat Damaged but Intact Lymphocytes
800-
a 600o a
a) a;
"O
a) 400oL 0
_ -0O a)
o0, n,%n-
0
0
Spleen
LiverA
1AA-
0 o ,/t I- l0 4 6 8 10 12 24 36 48 0 20 40 60
Hours After Re-injection
FIG. 4. Blood-clearance curves, together with spleen and liver uptake, of indium-111 oxine-lahelledlymphocytes from a normal subject. The secondary rise of labelled lymphocytes in the blood (at 4 h)is seen at a time when the surface probe counts over the spleen are decreasing.
time of small lymphocytes through thehuman spleen seems to be similar to thatin small experimental animals, and pre-liminary data suggest that the traffic intoand out of lymph nodes also approximatesto that found in experimental animalsystems. The data are consistent with theT cells leaving the blood and entering thespleen after re-injection. After 4-6 h, theywould have traversed the splenic whitepulp and reappeared in the blood, causingthe observed secondary rise in the blood-clearance curves (Fig. 4).The transit of different lymphocyte
subpopulations in the blood make animportant contribution to the magnitudeof the immune response in vivo, andquantitative aspects of lymphocyte trafficare important in the interpretation of invitro immunological studies of lymphoidcells taken from the blood. Much less timeis spent in the blood than in the othertissues where immunoclogical reactionstake place, and the relative numbers oflymphocytes measured in the blood withdifferent functional characteristics may
not reflect the magnitude of the immuneresponse.
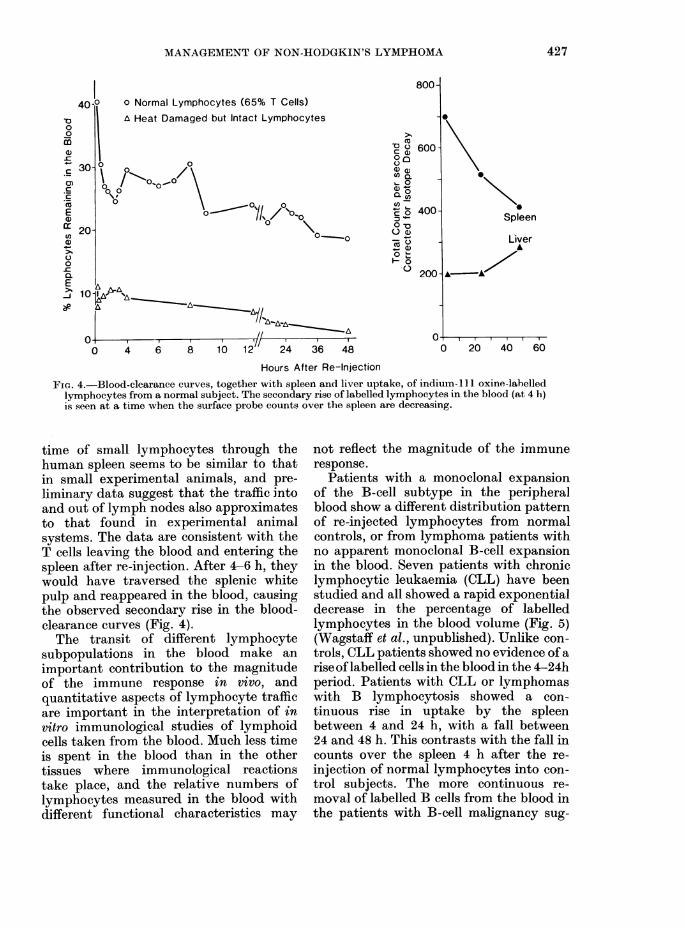
Patients with a monoclonal expansionof the B-cell subtype in the peripheralblood show a different distribution patternof re-injected lymphocytes from normalcontrols, or from lymphoma patients withno apparent monoclonal B-cell expansionin the blood. Seven patients with chroniclymphocytic leukaemia (CLL) have beenstudied and all showed a rapid exponentialdecrease in the percentage of labelledlymphocytes in the blood volume (Fig. 5)(Wagstaff et al., unpublished). Unlike con-trols, CLL patients showed no evidence of arise oflabelled cells in the blood in the 4-24hperiod. Patients with CLL or lymphomaswith B lymphocytosis showed a con-tinuous rise in uptake by the spleenbetween 4 and 24 h, with a fall between24 and 48 h. This contrasts with the fall incounts over the spleen 4 h after the re-injection of normal lymphocytes into con-trol subjects. The more continuous re-moval of labelled B cells from the blood inthe patients with B-cell malignancy sug-
427
2UU
14). (ROWTHER
40j
30- i
20 0
0,
10 \-,\ /
, _ n // n 1 n 4 & A0
800-
cu 600-
0a)
Qoa)en-
o 0
o .o'a
4 6 8 10 12" 24 36 48
Spleen0
200-
0-0 20 40 60
Hours After Re-InjectionFie(1. 5.-Blood-clearance cur.-es, together with spleen and liver uptake of indium- oxine- labelledlymphocytes from a patient with chronic lymphocytic leukaemia. Unlike normal lymplhocytes(Fig. 4) there is no secondary increase of labelled cell sin the blood following their rapid clearance,an1(l thle piobe couints over ths spleen are relatiVely constant over 48 hi.
gests that even at 48 h, few labelled cellshave returned to the blood after primarylocalization. The distribution to heavilyinvolved organs such as the liver andmarrow in these patients has also beenobserved. Marrow imaging is more intensein CLL patients than in control subjects.
It does not follow that the kinetics ofmigration of these cells is related to theirmalignancy, however, since it is knownthat B cells in animals have a more pro-longed migration pattern than T cells(Ford, 1975 review). T lymphocytesgenerally recirculate much more rapidlythan B cells, though they leave the bloodby crossing the post-capillary venules inlymph nodes at the same rate. T cells havea mean transit time of 5-6 h through thespleen, and 16-18 h through lymph nodes,compared with B cells which have not leftthe spleen in significant numbers by 24 hafter re-injection and have a mean transittime of 30-36 h through the lymph nodes.The observed difference in distributionseen in patients with lymphoid-cell malig-lignancy could be explained by the pro-
portion of T and B cells used, since T cellsmigrate more rapidly through the spleen,the major site of primary localization oflymphocytes. The subsequent rise andplateau seen under normal circumstancescould be due to the reappearance oflabelled T cells in the blood that havepassed through the spleen. The questionof whether CLL B lymphocytes havemigratory properties similar to normal Bcells needs to be answered. This shouldbe possible with further work using thellln-oxine labelled lymphocytes.Other subsets of lymphocytes within
the blood are known to have differentpatterns of migration in experimentalsystems, and gut, lung and salivarylymphoid tissue may well have character-istic migratory patterns. Further work on
this important new concept, using experi-mental animals, would be well worth-while.Using l1lln oxine-labelled cells, it can
be shown that some patients with othermalignancies have an extremely large fluxof lymphocytes through tumour tissue.
V00mci,-cC
0)C:CCcoEa)
a)00-C
E-J
428
-
,&,__!.yerA,
MANAGEMENT OF NON-HODGKIN'S LYMIPHTOAIA
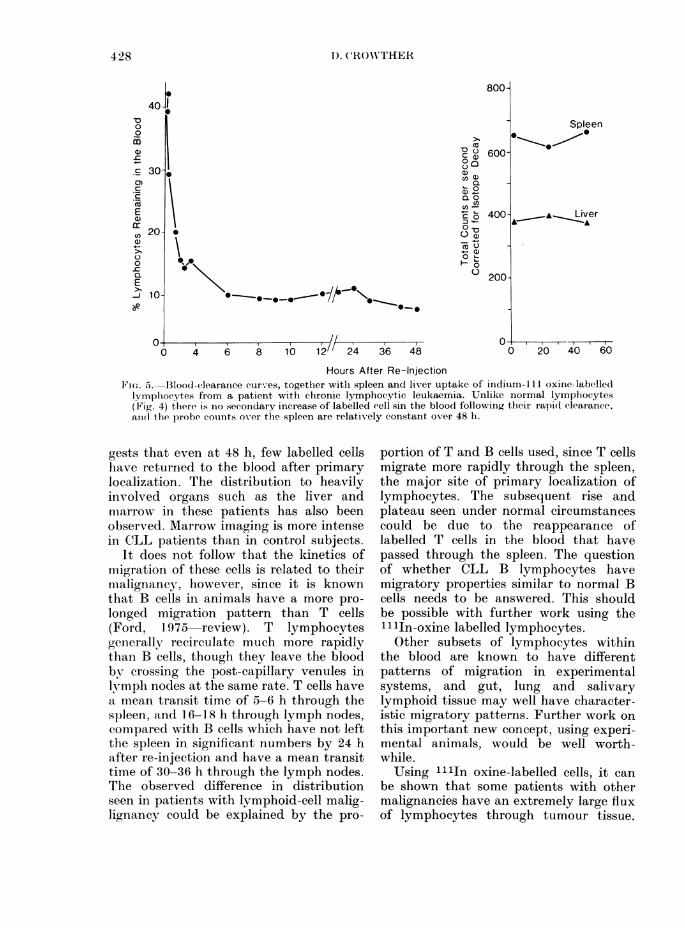
Fig. 6, for example, shows a scan of thechest in a patient with nodular sclerosingHodgkin's disease involving the medias-tinum a few hours after injecting his ownlabelled lymphocytes. A very large num-ber of labelled lvmphoid cells has been
(a)
3 n an. .. ,
4.
XJ.4w*t.
a *; ; *sS;WK :t
* #jliaiL* * 3**4|*'+ *.*: * ,_
^ * t .:_* * ,' t-E, %1
..w*..L.._I_
4
gp
STEEL a
(b)
FIe. 6. (a) A plain clhest X-ray slhoNmedliastinal enlargement with nod:sclerosing Hodgkin's (lisease. (b) Garr
camera picture 24 h aft!er the patient'speripheral-blood lymplhoctyes labelledinidiim- 111 oxine were re-injecterl.
taken up by the mediastinal tumour, andvisualization of the enlarged nodes mayoccur as early as 30 min after re-injection.Such a flux of lymphocytes may be animportant mechanism enabling contactto be made between tumour tissue and thereactive lymphoid cells which are knownto be in the blood of patients withHodgkin's disease (Crowther et al.,1969a,b). These cells are similar to thoseseen in the blood after antigenic stimu-lation.Although an antigenic stimulus pro-
motes lymphocyte migration, antigenspecificity does not appear to contributeto the initial homing. Lymphocyte migra-tion is, however, facilitated by an increasein local blood flow, and this appears to bean important mechanism for bringingantigen-specific lymphoid cells into appro-priate contact with foreign material atsites of inflammation (Hay et al., 1980).We are also hoping that the technique
will shed light on the cause of the lympho-paenia in patients with malignant diseaseand its relationship with prognosis.
CLASSIFICATION
s5 Classification of NHL by conventionalhistopathological techniques is notoriouslytinreliable, and the large number of histo-pathological classifications available re-flects this problem. The cell types can bedescribed, but the cell lineage and differ-entiation cannot be determined withoutmore sophisticated techniques.Normal lymphoid cells and their malig-
nant counterparts have been reported tovary in their biochemical properties, andvariation in surface glycoproteins, mem-brane-transport molecules, content ofmetabolites such as glycogen, ability to
n. go synthesize certain amino acids and specificenzyme content has been observed. Bio-chemical characterization is proving of
wing objective value in classifying lympho-lular proliferative tumours in addition toima- routine histological techniques. Hetero-own geneity of lymphoid malignancies has been
demonstrated within the T-cell, B-cell and
lhk0- 26a
429
4
D. CROWTHER
non-T, non-B groupings with respect tosurface properties of the individual cells,and enzymatic content and correlationswith clinical features have been noted.The classification of lymphoproliferative
disorders has dramatically changed in thelast few years, as our understanding ofimmunology has increased. Studies ofmembrane properties and functionalattributes of the lymphocytes has led to abetter understanding of the biology of thelymphomas. Subpopulations of both T andB cells have been identified, and character-istic lymphoma patterns can be related toa homogeneous expansion of a particularsubpopulation. In addition, immunologicalstudies are providing information on thesequence of cell-surface-related differ-entiation in cells of the lymphocytic,granulocytic and erythrocytic series.The method of monoclonal antibody
production using mouse hybridomas(Kohler & Milstein, 1975) is already prov-ing of value, in addition to the moregenerally available techniques for charac-terizing cell-surface phenotypes within thelymphoid malignancies. The biochemicalfeatures of the antigenic determinantsreacting with monoclonal antibodies cannow be investigated, and this most im-portant area of research is now open.Monoclonal antibodies may be directedagainst specific oligosaccharide sequences,and can be used to dissect the chemistryof the cell-surface glycoproteins. Pre-liminary results suggest that the tech-nique is of importance in determining theimmunological phenotype of patients withdiffuse large-cell lymphoma, and this maybe helpful in defining groups with differentsurvival prospects (Warnke et al., 1980).Clearly, prospective studies involvingthese new techniques in untreated patientsare likely to lead to a better understandingof the biology of these tumours, but theprognostic weight of each parameter mustbe measured against other known prog-nostic features, using multi-variateanalysis. An approach has already beenmade to evaluate enzyme and membranemarker properties of leukaemia cells using
multi-parameter analysis (Janossy et al.,1980).The detection of cells of B lineage
belonging to a single clone in the periph-eral blood of patients with lymphoma canhelp confirm the diagnosis and define thetumour type. Such studies also have rele-vance in terms of staging (Garrett et at.,1979; Ault et al., 1979). Abnormalities canbe detected in the presence of a normalwhite cell count and differential usinganti-light-chain sera, but interpretation isdependent on the ratio of Kappa: Lambdabearing cells. Other techniques, such asthe detection of colchicine-sensitivelymphoid cells in the peripheral bloodmay also be helpful in this regard (Thom-son et al., 1972; Scarffe et al., 1980).
These methods, however, are not theonly ones available for studying the com-position of the plasma membrane in singlecells. A method of current interest to ourgroup in Manchester involves a study ofthe biochemistry of the lymphoid cell sur-face using plant-lectin binding assessedby flow cytometry. A large number ofworkers are contributing to the success ofthese studies, but particular mention mustbe made of Dr G. Blackledge who con-ducted the flow-cytometric studies andDr J. Gallagher who provided the neces-sary expertise in glycoprotein and lectinchemistry. The immunological studieswere in collaboration with Dr B. Vose(Department of Immunology, PatersonLaboratories).
Lectins can be bound to fluoresceinisothiocyanate, and the amount attachingto the plasma membrane of single cells canbe determined by measuring the emissionof fluorescence from each cell in flowcytometry. Differences in lectin bindingbetween cells within a separated popula-tion may be investigated using thismethod. Flow cytometry involves themeasurement of different properties ofcells passing singly at high speed througha beam of light (Kamentsky et al., 1965).Light scattering of the beam (related tocell size) and emission of light from aspecific fluorescent probe can be assessed
430
MANAGEMENT OF NON-HODGKJN'S LYMPI1HOMA
quantitatively for each cell. An interfacebetween the flow cytometer and a DeskTop computer (HP9845S) allows a 3-dimensional presentation of data for cellsize, number and fluorescence measure-ments (Blackledge et al., 1980a). Cellpopulations with different properties caneasily be recognizedI and selected forfurther study, using this system. Themethod is rapid and means that the lectin-binding properties of several thousandindividual cells within a population canbe characterized.The carbohydrate residues of glyco-
proteins and glycolipids are located on theexternal face of the plasma membrane,where they play an important part in cellbehaviour. The migratory properties ofnormal lymphoid cells and their malignantcounterparts may well be determined to alarge extent by differences in cell-surfacechemistry. For these reasons, the study ofcertain plant lectins with highly specificsaceharide-binding properties is beingundertaken. The technique with flowNcytometry provides a tool for examiningthe carbohydrate structure of the intactplasma membrane of single cells.Some lectins react only with certain
terminal sugar residues, others react withsugars within the carbohydrate chaini, andoccasionally they may react specificallywith a particuilar sugar sequence. The useof enzyvmes to remove terminal sugarresidtues, followed by further bindingstudies with appropriate lectins, will allowthe concentration and/or affinity of specificsubterminal sugars to be determined.When a lymphoid cell population is
obtained from peripheral blood by re-moving the erythrocytes and phagocyticcells, the lymphocytes show a character-istic pattern of binding with 60% of thecells having low binding to Lens calinatrisaggltitinin (LCA) and the remaining 40%0showing considerably higher binding, in-dependent of cell size. This plant lectinbinds to a-mannoside residues within thecarbohydrate chain, and binding can beinhibited by the analogue a-methyl man-noside. Separ-ation of the T lvmphocytes
31
on the basis of the capacity to form rosetteswith sheep red blood cells (E+) indicatedthat most (80-870o) had low LCA binding,whereas lymphocytes not binding to sheepred blood cells (E-) had high bindingactivity. The production of an enrichedT-cell population by removinig B cells in abead column coated with human Igreacted with human anti-Ig, produced asimilar binding pattern to the T-cell popu-lation separated with sheep red cells.Subsequent experiments uising a BecktonDickinson Fluorescence-activated CellSorter 4, showed that E+ cells could beseparated on the basis of LCA binding(Blackledge et al., in preparation). Studyof the patterns of inhibition with appro-priate sugars indicate that the distinctionbetween T (E+) and non-T (E-) cells isquantitative rather than qualitative, withnon-T cells having the greater number ofboth high- and low-affinity sites for LCA.This means that the concentration of N-glycosidically-linked mannose containingoligosaccharides is highest in the E- popul-lation. Wheat germ agglutinin (WVGA)binds to terminal sialic acid and N-acetylglucosamine residuies and can be used toindicate the number of complete cell-surface oligosaccharides. Experimentswith this lectin show increased binding inthe E- subset, indicating a higher sacehar-ide chaiii density in these cells.
Fuirther experiments, in which stubsetsof lymphocytes wAithli different functionalcharacteristics were separated by a den-sity-gradient technique, have allowed acorrelation to be made between functionalactivity and lectin-binding properties(Vose et al., in preparation). Studies in-volving monoclonal antibodies and lectinbinding are providing the tools for separ-ating subsets of lymplhocytes with differentfunctional capacity, <and provide a newapproach in removing unwanted immutnecells from a marrow graft.
Cell-surface lectin-binding properties ofmalignant lymphoid cells can be studiedby similar techniques. The lectin-bindingproperties of acute leukaemia cells takenfrom the peripheral blood differ markedly
431
1). CROWN"THER
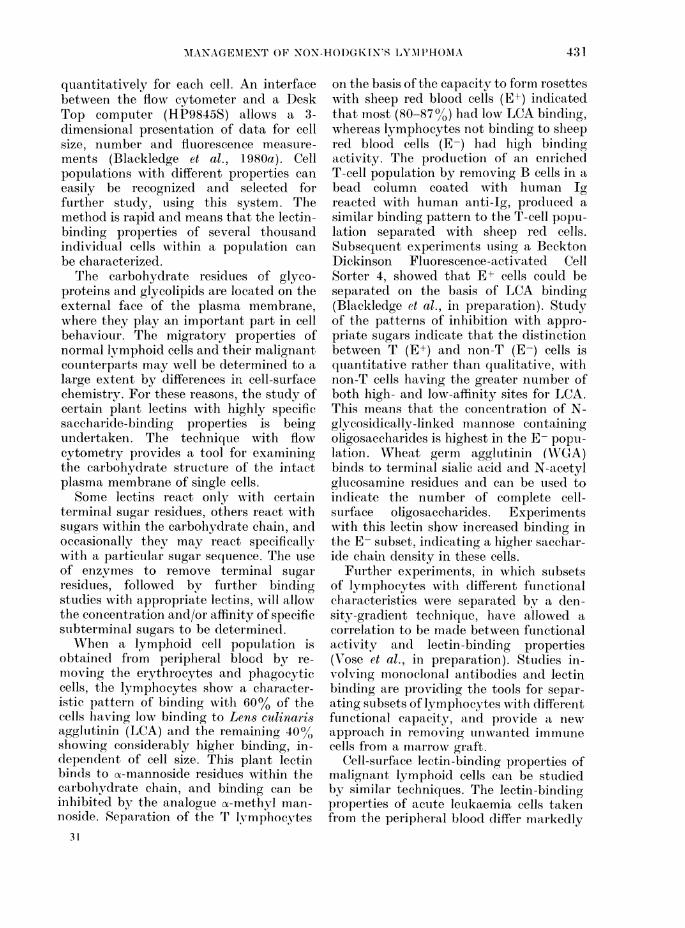
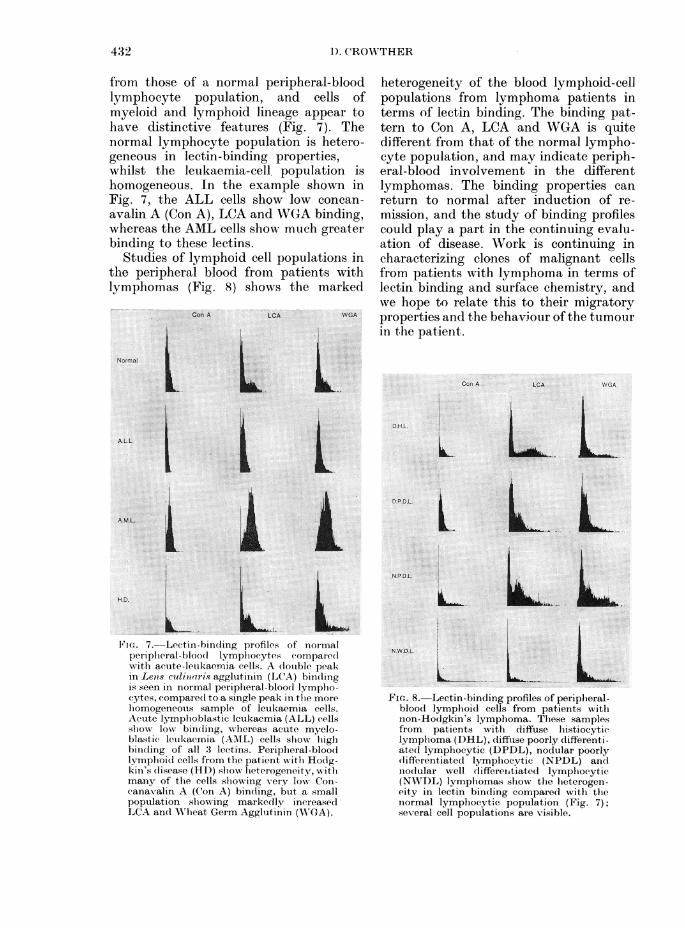
from those of a normal peripheral-bloodlymphocyte population, and cells ofmyeloid and lymphoid lineage appear tohave distinctive features (Fig. 7). Thenormal lymphocyte population is hetero-geneous in lectin-binding properties,whilst the leukaemia-cell population ishomogeneous. In the example shown inFig. 7, the ALL cells show low concan-avalin A (Con A), LCA and WGA binding,whereas the AML cells show much greaterbinding to these lectins.
Studies of lymphoid cell populations inthe peripheral blood from patients withlymphomas (Fig. 8) shows the marked
Fi-. 7. Lectin-bincding profiles of noimalperiplieral-bloo(l lymphocytes compare(dwrvith acute-leukaemia cells. A (lolible peakin Lenis culio(tris agglutiriin (LCA) bindingis seen in normal periplheral-bloodl lympho-cytes, compare(l to a single peak in the morehomogeneouis sample of leukaemia cells.Acute lymphoblastic leukaemia (ALL) cellsslhow low binding, wlhereas acute myelo-blastic leukaemia (AM1L) cells showv highbinding of all 3 lectins. Peripheral-bloodlymploiod cells from the patient with Hodg-kin's (disease (HD) show lheterogeneity, w ithmany of the cells showring very low Con-canavalin A (Con A) binding, btit a smallpopulation showing markedly increasedLCA andl Wheat Germ Agglutinin (W'GA).
heterogeneity of the blood lymphoid-cellpopulations from lymphoma patients interms of lectin binding. The binding pat-tern to Con A, LCA and WGA is quitedifferent from that of the normal lympho-cyte population, and may indicate periph-eral-blood involvement in the differentlymphomas. The binding properties canreturn to normal after induction of re-mission, and the study of binding profilescould play a part in the continuing evalu-ation of disease. Work is continuing incharacterizing clones of malignant cellsfrom patients with lymphoma in terms oflectin binding and surface chemistry, andwe hope to relate this to their migratoryproperties and the behaviour of the tumourin the patient.
FIG. 8. Lectin-binding profiles of peripheral-blood lymphoid cells from patients withnon-Hodgkin's lymphoma. These samplesfrom patients with diffuse histiocyticlymplioma (DHL), diffiuse pooi-ly differenti-ated lympliocytic (DPDL), nodular poorly(lifferentiated lymphocytic (NPDL) ancdnodular well differentiated lymphocytic(NWDL) lympliomas slhow the lieterogen-eity in lectin binding compared with thenormal lymphocytic population (Fig. 7);several cell populations are visible.
4.32
MANAGEMENT OF NON-HODGKIN'S LYMPHOMA 433
The abnormal lectin binding of lymph-oid cells from the peripheral blood ofpatients with Hodgkin's disease is ofinterest (Fig. 7). Reactive lymphoid cellsare known to be increased in the periph-eral blood of such patients, and it istempting to surmise that the markedlyincreased LCA and WGA binding seen ina proportion of the cells may be related tothis. The large number of cells with verylow Con A binding is also an interestingfeature, and requires further study.A further technique involving the
assessment of lectin binding by fluores-cence microscopy of lymph-node sectionshas been devised, and this is providinguseful information on lectin binding to theplasma and nuclear membrane of normallymphoid cells and malignant lymphomacells. In these studies the lymph-nodearchitecture remains intact and the workis providing useful additional informationabout differences between lymphomas(Bramwell et al., unpublished observa-tions).
I started my talk by illustrating the lackof improvement in overall survival inpatients with NHL in England and Walesduring the 1960s and early 1970s. How-ever, I hope I have demonstrated thatthere is no need for pessimism. The im-proved combined-modality treatmentalready available for the least favourablegroup of patients should now lead to someimprovement in these national figures.The intensity of research into distinguish-ing groups of patients with characteristicmalignant cells and biological behaviouris leading to innovative approaches totherapy likely to improve the welfare ofpatients in the poor-risk groups. The pathsof basic research and clinical research arecloser in this subject than they have everbeen before, and it is clear that the 1980swill be coloured by further exciting jointventures of value to the patient.
I -would like to thanbk my colleagues in the Alan-chester Lymphoma Group for allowving me to publishthe data concerrning chemotherapy in the non-Hodgkin's lymphoma of dliffuise pathology. Dr M1.
Palmer, Dr G. Blackledge, AMr R. Swindell and Dr V.Blair were responisible for the development of thecomputerized analysis presented here. I am mostgrateful to my secretary, Airs B. Wthittle, for typingthe manuscript.
REFERENCES
AULT, K. A. (1979) Detection of small numbers ofmonoclonal B lymphocytes in the blood of patientswith lymphoma. N. Engl. J. Med., 300, 1401.
BEST, J. J. K.. BLACKLEJiGE, G., FORBES, W. ST C.& 4 others (1978) Computed tomography ofabdomen in staging and clinical management oflymphoma. Br. Med. J., ii, 1675.
BLACKLEDGE, G., BUSH, H., DODGE, 0. G. &CROWTHER, D. (1979) A study of gastro-irAtestinallymphoma. Clin. Oncol., 5, 209.
BLACKLEDGE, G., SWINDELL, R., HODGSON, B. &CROWTHER, D. (1980a) Computerised acquisitionand analysis of flow cytomelIric data. Int. J. Bio-Med. Comput., 11, 41.
BLACKLEDGE, G., BUSH, H., CHANG, J. & 9 otlhers(1980b) IntensiVe combination chemothierapywith Vincristine, AdIriamycirn and Prednisolone(VAP) in the treatment of diffuse histology non-Hodgkin's lymphoma. Eur. J. Cancer, 16, 1459.
BODEY, G. P. & RODRIGUEZ, V. (1978) MIalignantlymphoma. Sem. Haematol., 15, 221.
BONADONNA, G., LATTUADA, A. & BANFI, E. (1976)Recent trends in the medical treatment of nor.-Hodgkin's lymphoma. Eur. J. Cancer, 12, 661.
BUSH, R. S., GOSPODAROWICZ, M., BERGSAGEL, D. E.& BROWN, T. C. (1979) Radiation therapy forpatients with localised non-Hodgkini's lymphoma.In Advances in Medical Oncology, Research andEducation. Leukaemi(a & Lyn?phoma. Ed.Crowtlher. Oxford: Pergamon Press. p. 209.
BUTCHER, E. & WEISSMAN, I. (1980) I. Cellular,genetic and evolutionary aspects of lymphocyteinteractions with high endothelial venule. InBlood Cells and Vessel Walls: Functionzal Inter-actions. Ed. O'Connor. London: Churchill. p. 265.
CABANILLAS, F., RODRIGIUEZ, V. & FREIREICH, E. J.(1978) Improvement in complete response rate,duration of response and survival with Adria-mycin combination chemothlerapy for non-Hodgkin lymphomas: A prognostic factor com-parison of two regimes. Med. Paediat. Oncol., 4,321.
CHEN, Al. G., PROSNITZ, L. R., GONZALEZ-SERVA, A.& FISCHER, D. B. (1979) Results of radiotherapyin control of Stage I and II non-Hodgkin'slymphoma. Cancer, 43, 1245.
CHISHOLM, P. Al. & FORD, NA. L. (1978) Selection ofantigen-specific cells by adherence to allogeneiccell monolayers: Cytolytic activity, graft-versus-host activity and numbers of adherent and non-adherent cells. Eur. J. Immuniol., 8, 438.
CROWTHER, D., BLACKLEDGE, G. & BEST, J. K.(1979) The role of compute(1 tomography of theabdomen in the diagnosis and staging of patientswi'th lymphoma. Clin. Haernatol., 8, 567.
CROWrTHER, D., HAMILTON-FAIRLEY, G. & SEWELL,R. L. (1969a) Lymphoil cellular responses in thebloodl following immunisation in man. J. Exp.Med., 129, 849.
CROWTHER, D., HAMILTON-FAIRLEY, G. & SEWELL,R. L. (1969b) The significance of the changes in
434 D. CROWrTHER
circulating lymploidl cells in Hodgkin's disease.Br. J. Med., 2, 473.
FISHER, R. I., DE VITA, V. T., JOH-NsoN, B. L.,SIMON, R. & YOUNG, R. C. (1977) Prognosticfactors for advanced diffuse histriocytic lymphomafollowing treatment with combination chlemo-tlherapy. Am. J. Med., 63, 177.
FORD, XV. L. (1975) Lymplhocyte migrationi and theimmune responses. Prog. Allergy, 19, 1.
FORD, NA. L. (1978) AMalignant lymplhoma. UJICCTech. Rep. Series, 37, 206.
FIJKS, Z. & KAPLAN, H. S. (1975) Recurrence ratesfollowing radiation therapy of nodutilar anid (liffuisemalignant, lymplhoma. Radiology, 108, 675.
GARRETT, J. V., SCARFFE, J. H. & NEWTON, R. K.(1979) Abnormal peripheral bloodl lymphocytesan(l bone marrow infiltration in non-Hodgkin'slymplhoma. Br. J. Haemaitol., 42, 41.
GLATSTEIN, E., DON-ALDSON, S. S., ROSENBERG4,S. A. & KAPLAN, H. S. (1977) Combined modalitytlherapy in malignant lymphomas. Cancer Treat.Rep., 61, 1199.
HALL, .1. G. (1980) An essay on lymphocyte (ircula-tion and the gut. Monogr. Allergy, 16, 100.
HAY, J. B., JOHNSTON, Al. G., VAI)AS, P., CHIN, W.,TSSEKIUTZ, T. & MOVAT, H. Z. (1980) Relationshipsbetween changes in blood flow% andl lymphocytemigration induced by antigen. Monogr. Allergy,16, 112.
ISSEKUTZ, T., CIIIN, WV. & H AY, J. B. (1980)Mleasurement of lymphocyte traffic with Inidium-111. Clin. Exp. Immunol., 39, 215.
JANoSSY G., HOFFBRAND, A. V. GREAVES AI. F. &6 otlbers (1980) Terminal transferase enzyme assayand immunological membrane markers in tlhediagnosis of leukaemia: A multiparameter analysisof 300 cases. Br. J. Haeematol., 44, 221.
JOHNSON, R. E., CANELLOS, G. P., YOUNG, R. C.,CHABNER B. A. & DE VITA, V. T. (1978) Chemo-tlherapy (cyclophosphamide, vincristine and pied-nisone) versus radiotherapy (total body irradi-ation) for Stage III-IV poorly differentiatedlymphocytic lymplhoma. Catcer Treat. Rep., 62,321.
JOHNSON, G. J., COSTELLO, WV. G.,OKEN, Al. Al. & 5others (1979) The v-alue of Adriamycin andl ofmid-cycle treatment in multidrug therapy ofunfavourable lhistology non-Hodgkini's lymplhoma.Proc. Am. Soc. Clin . On?col., 20, 196.
JONES, S. E., GROZEA, P. N., AIETz E. N. & 6 others(1979) Superiority of Adriamycin-containing com-bination chemotherapy in the treatment, of dliffiselymphoma. Cancer, 43, 417.
KAMENTSKY, L. A., AIELAMED, M. R. & DORRAN, H.(1965) Spectroplhotometer: New instruLment forultrarapicd cell analysis. Scienice, 150, 630.
KOHLER, G. & -MILSTEIN, C. (1975) Contintuouscultures of fiLsed cells secreting antibody of pre-defined specificity. Nature, 256, 495.
LANDBERG, 1. G., HAKANSSON, L. G., MOLLER, T. R.& 8 others (1979) CVP-remissioni-maintenance inStage I or II non-Hodgkin's lymphoma. Pre-liminarv results of a randomised study. Cancer, 44,831.
LAVENDER, J. P., GOLDMIAN, J. MI., AR-NOT, R. N. &THAKUR, IM. L. (1977) Kinetics of Indium-lu11labelled1 lymphocytes in normal subjects andpatients. Br. Med. J., 2, 797.
LISTER, T. A., CULLEN, Al. H., BREARLEY, R. B. & 7others (1 978) Combinationi chemotherapy for
advanced non-Hodgkin's lymplhoma of unfavour-able histology. Cancer Chemother. Pharmacol., 1,107.
1\IICAFEE, J. G. & THAKUR, M. L. (1976) Survey ofradioactive agents for in vitro labelling of phago-cytic leukocytes. I. Soluble agents. J. Nucl. Med.,17, 480.
M\1ACKINTOSH, F. R., O'NEILL, M. & ROSENBERG, S.(1980) Prognostic factors in advanced histiocyticlyinphoma. Proc. Am. Soc. Clin. Oncol., 21, 465.
AMILLER, T. P. & JONES, S. E. (1979) Chlemoth1erapyof localised histiocytic lymphoma. Lancet, i, 358.
MIONFARDINI, S., BANFI, A., BONADONNA, G. & 4others (1979) Improved five vear survival aftercombined radiotherapy-chemotherapy for StageI-II non-Hodgkin's lymphoma. IJot. J. Radialt.Oncol. Biol. Phys., 6, 125.
OFFICE OF POPULATION CENSuSES ANI) SuTRVEYS(1980) Caincer Statistics Surviva(l. Series M.B.1,No. 3. London: HMlSO.
PANAHON, A., KAUFMAN, J. H., GRASSO, J. A.,FRIEDMAN, M. & STIJTZMAN L. (1977) A ran-domised study of radiation therapy veirsus raclio-therapy and chemotherapy in Stage IA-IJIB non-Hodgkin's lymplhoma. Proc. Am. Soc. Clin. Oncol.,18, 321.
RANNIE, G. H. & FORD, WV. L. (1977a) Phiysiologyof lymphocyte recirculation in anrimal models.Proc. IXth Int. Cong. Lyons.
RANNIE, G. H., THAKITR, M. L. & FORD, W. L.(1 977b) Experimental comparison of radioactivelabels wTith potential application to lymphocytemigration studlies in patients. Clin. Exp. Immunol.,29, 509.
SCARFFE, J. H., PRUDHOE, J., GARRETT, J. V. &CROWN'THER, D. (1980) Colehicine ultrasensitivityof periplheral bloodi lymphocytes from patientswith inon-Hodgkin's lymplhoma. Br. J. Cancer, 41,593.
SCREIN, P. S., CHABNER, B. A., CANELLOS, G. P.,YOUNG, R. C., BERARD, C. & D)E VITA, V. T. (1975)Potential for prolonged disease free sturvivalfollowing combination chemotherapy of norn-Hodgkin's lymphoma. Blood, 43, 181.
SKARIN, A., CANELLOS, G., ROSENTHAL, D., CASE,D., MOLON-EY, WV. & FIaEI, E. III (1980) Therapyof diffuise histiocytic and undifferentiated lymph-oma w'ithi high dose Methotrexate and Citrovorinfactor rescue (MTX/CF), Bleomycins, Adriamycin,Cyclophosphlamidle, Oncovin and Decaclron (AM-BACOD). Proc. Am. Soc. Clin. Onicol., 21, 463.
SMuITH, AT. E., -MARTIN, A. F. & FORD, WV. L. (1980)Mligration of lymphoblasts in the rat. Preferentiallocalisation of DNA-synthesising lymplhocytes inparticular lymph nodes andI other sites. Monogr.Allergy, 16, 203.
SULLIVAN, K., NEIMIAN, P'., FAREWELL, L. V.,HARRISON, D., RUDOLPH, R., EINSTEIN, A. &BAGLEY, C. (1979) Combined modality therapy inadvanced (lifftise non-Hodgkin's lymphoma. Atwo an(l one lhalf year follow uip. Proc. Amn. Soc.Clin. Oncol., 18, 442.
THOMSON, A. E. R., O'CONNOR, T. -W. E., &WETHERLEY-AMEIN, G. (1972) Killing andI chlar-ac-terising action of colchicine in vitro on lympho-cytes of chronic lymphocytic leukaemia. Scand. J.Haematol., 9, 231.
TINIOTHY, A. R., LISTER, T. A., KATZ, D. & JONES,A. E. (1979) Localised non-Hodgkin's lymplhoma.Eur. J. Cancer, 16, 799.

MANAGEMENT OF NON-HODGKIN'S LYMPHOMA 435
WAGSTAFF, J., GIBSON, C., THATCHER, N. & 4 others(1981a) A method for following human lympho-cyte traffic using Indium-111 oxine labelling.Clin. Exp. Immunol., 43, 435.
WAGSTAFF, J., GIBSON, C., THATCHER, N., FORD,W. L., SHARMA, H. & CROWTHER, D. (1981b)Human lymphocyte traffic assessed by Indium- Illoxine labelling-clinical observations. Olin. Exp.Immunol., 43, 443.
WARNKE, R., MILLER, R., GROGAN, T., PEDERSEN,
M., DILLEY, J. & LEVY, R. (1980) Immuniologicphenotype in 30 patients with diffuse large celllymphoma. N. Engl. J. Med., 303, 293.
YOUNG, R. C., HOWSER, D. M., ANDERSON, T.,JAFFE, E. & DE VITA. V. T. (1979) CNS infiltra-tion: A complication of diffuse lymphomas. InCNS Complications of Malignant Disease. EdsWhitehouse & Kay. London: Macmillan Press.p. 121.





























