Embed Size (px)
Citation preview

24 (2006) 181–204
Hospice: Comprehensive Care at the End
of Life
Perry G. Fine, MDa,b,T, Malene Davis, RN, MBAb,c
aPain Research Center, School of Medicine, University of Utah, Suite 200, 615 Arapeen Drive,
Salt Lake City, UT 84108, USAbNational Hospice and Palliative Care Organization, Alexandria, VA 22314, USA
cHospice Care, PO Box 760, Arthurdale, WV 26520, USA
The roots of hospice can be traced to early Christendom as places of respite for
weary travelers. These refuges spread through the Byzantine and Greek cultures
and later the Roman Empire, where the Latin term hospitium was adopted, and
its derivation continues today. Throughout the Middle Ages and during the
Crusades, hospices proliferated and expanded their role to provide care for the
sick and dying but then virtually disappeared during the Reformation. Then, in
nineteenth-century century Ireland and France, hospices were established spe-
cifically to provide terminal care. In the mid-twentieth century, Dame Cicely
Saunders recognized the need to provide a haven for patients dying of cancer,
where there would be the focus of around-the-clock symptom control in an
ambiance of caring. Through her work at St. Christopher’s Hospice on the
outskirts of London, the modern era of hospice was born [1].
Modern era of hospice in the United States
The concept of hospice migrated to the United States in the 1970s, beginning
with small grassroots programs and demonstration projects, followed by a rapid
proliferation in the 1980s, largely as a result of legislation that created a defined
Anesthesiology Clin N Am
0889-8537/06/$ – see front matter D 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.atc.2005.12.004 anesthesiology.theclinics.com
T Corresponding author. Pain Research Center, School of Medicine, University of Utah, Suite 200,
615 Arapeen Drive, Salt Lake City, UT 84108.
E-mail address: [email protected] (P.G. Fine).

fine & davis182
Medicare Hospice Benefit (MHB). The past decade has seen a continued mod-
ernization and rapid expansion of hospice services, mostly in the home en-
vironment, concurrent with the growing acceptance of palliative medicine as a
credible and much-needed specialty and domain of the health care continuum to
improve end-of-life care. During this time, hospice has broadened its scope, from
a service dedicated almost entirely to cancer patients to the care of all patients
who have life-limiting illnesses, such as end-stage cardiac or pulmonary disease
and advanced dementia (eg, Alzheimer disease), to name a few.
The essential philosophy of hospice care focuses on comfort, dignity, and
personal growth at life’s end. This focus encompasses biomedical, psychosocial,
and spiritual aspects of the dying experience, emphasizing quality of life and
healing or strengthening interpersonal relationships, rather than prolongation of
the dying process at any and all costs. To reach these goals requires expertise in
pain and symptom management, as well as intra- and interpersonal dynamics, at
this unique time in the human life cycle. Additionally, hospice care supports the
well being of those (usually family members) who are in primary care-giving
roles and provides bereavement care for survivors.
Modern hospice care is a team effort, in which the typical hospice inter-
disciplinary team consists of medical providers (physician, nurse, and nursing
assistant), psychosocial care providers (social worker), spiritual care providers
(chaplain), and other supportive care professionals, as needed (nutritionist,
physical therapist, pharmacist, speech therapist, and other specialists). Hospice
programs are managed by individuals with a diversity of backgrounds, includ-
ing business, nursing, social work, and theology. Notwithstanding their primary
credentials, increasingly sophisticated management and information technology
skills are required to meet the demands of the current clinical, regulatory, and
fiscal environment. A hallmark of hospice care, and a requirement under the
provisions of the Medicare Hospice Benefit, is the involvement of volunteers
who provide visitation, companionship, housekeeping help, errands, and many
other types of needed assistance.
In the United States, most hospice care is provided in the home, but it can be
rendered in any environment, including inpatient settings, long-term care fa-
cilities (nursing homes and assisted living centers) or anywhere else the patient
resides. There are currently over 3000 hospice programs operating within the
United States. Most are small programs with a census of less than 30 patients,
with budgets bolstered by charitable giving to provide needed services. Currently,
there is a trend toward growth and a consolidation to form larger multisite pro-
grams, creating operating efficiencies through economies of scale and integra-
tive information systems. This increased efficiency allows more effective use of
limited resources to reach far more patients from all social spheres, with the
ability to provide more advanced palliative services for symptom control and
optimization of quality of life. As a result, we are beginning to witness a blending
of the humanistic family and patient-centered philosophy that has characterized
traditional hospice with the myriad innovations that have been derived through
scientific advances of modern medicine. Significant improvements in quality of

hospice: comprehensive care at the end of life 183
life at the end of life, often with reductions in health care expenditures, can now
be realized by patients who elect modern-day hospice care [2–4].
Hospice as a system of care and community resource
Hospice is the comprehensive and coordinated palliative care for patients
who have predictably limited life expectancy, provided both at home and across all
institutional settings. As a community asset, hospice programs serve as their
communities’ leaders in issues related to end-of-life care. High-functioning pro-
grams operate broadly and holistically as social and community service agencies
and educational resources, in addition to providing patient-care and bereave-
ment services.
Hospice care is based on a ‘‘biopsychosocial’’ model rather than a disease
model of care, emphasizing quality of life at the end of life and supportive care
rather than a cure or life prolongation. With the understanding that death is an
inevitable consequence of living and that loss is difficult, hospice has taken a
leadership role in providing grief support for communities. Examples include
the organization and direction of bereavement groups and counseling and pro-
grams for children, such as bereavement camps. Another important aspect of
hospice care is the provision of support and respite for family members and
friends involved in the patient’s care. Because the death of a child is particularly
difficult for all involved, partnerships among community-based hospice programs
and pediatric providers have been of great value in fostering continuity of care
from the time of diagnosis through death, for the sake of the patient, siblings,
parents, and health care professionals.
Hospice and palliative care continuum
In the United States, the developing specialty of palliative care has evolved out
of the collective hospice experience. Palliative care is a broader application of
hospice concepts, applicable to patients who have a significant burden of illness
but earlier in the disease trajectory, when death is not imminently foreseeable or
when prognosis is too unsure to consider hospice referral. To optimize outcomes
for patients who have chronic, progressive illness, palliative care should be in-
tegrated fully into disease-modifying and life-prolonging treatments. When life
expectancy is limited to months, rather than years, hospice becomes the optimal
system of care in the chronic care continuum (Fig. 1).
The intent of palliative care at all stages and settings is to prevent and relieve
unnecessary suffering. Goal-setting, along with early identification and careful
assessment and treatment of pain and other physical, psychosocial, and spiritual
problems, prevents crises and leads to a more effective use of health care re-
sources. Anticipatory planning is an important component of palliative care. In
certain settings, such as hospitals, palliative care services use a team approach to

Disease Management/Palliative Care Hospice
Interventions with Curative Intent
Disease Modifying Interventions
Palliative Interventions
Bereavement
Diagnosis of a chronic condition or illness
Prognosis of foreseeable limited life expectancy or end-stage disease
Death
Fig. 1. Conceptual model of the chronic care continuum.
fine & davis184
address the needs of patients and their families. The most successful hospital-
based palliative care programs form partnerships with local hospice programs to
provide continuity through hospital discharge, to prevent crises, to provide an
alternative to emergency department or hospital-based acute care, and to prevent
unwanted or unnecessary rehospitalization. In this model, a hospice representa-
tive (usually a social worker or nurse) also may be a member of the hospital
palliative care team. Increasingly, this approach to care improvement is being
adapted to long-term care settings because approximately 20% of the United
States population dies in nursing homes, and this number is projected to double
in the next few decades.
Access to hospice care
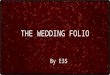
Despite significant increases in the numbers of patients recently using hospice
services (over 1 million patients in 2004) (Fig. 2), barriers remain to access and
timely referral, notable mostly in rural and inner city areas and among minority
populations. The need for hospice care comes at a time of life when emotions run
high, so discussions of various options and care paths require a delicate touch.
Optimally, these discussions would have occurred in advance of a life-threatening
illness to allow time for sufficient contemplation, comprehension, emotional
preparation, and documentation of patient preferences and values. Regardless
of timing, it is critically important that clinicians be able to enumerate the in-
dications for and benefits of hospice care clearly, proactively, and succinctly,

0
200000
400000
600000
800000
1000000
1985 1989 1992 1996 2000 2002
Served 1985 - 2003
Fig. 2. Number of hospice patients served between 1985 and 2003. (From National Hospice and
Palliative Care Organization (NHPCO) Web site. Available at: www.nhpco.org/files/public/Patients_
Served_1985_2002.pdf; with permission.)
hospice: comprehensive care at the end of life 185
just as they would for any significant clinical option, such as the decision to
pursue coronary revascularization or renal transplantation.
Clinicians can learn to emphasize that when there is no longer a ‘‘curative’’
pathway, their patients and their families who elect modern-day hospice care
are more likely to enjoy significant improvements in the quality of their lives
during the final stages of illness than those who do not. There is growing
evidence, too, to suggest that these benefits might come with appreciable cost
savings to families. This is important in view of the findings by the Study to
Understand Prognoses and Preferences for Outcomes and Risks of Treatment
(ie, SUPPORT) that families who did not obtain hospice care suffered major
financial hardship through the course of their loved ones’ last months of life [5].
This is corroborated by Medicare claims data, which find that 30% of Medicare
dollars are spent during the last 12 months of life, but only 3% of the annual
Medicare budget is spent on the MHB [6].
Characteristics of a quality hospice program
A quality hospice program provides an interdisciplinary team of experts who
deal with all aspects of the dying process: physical, emotional, social, practical,
and spiritual. Tracking key quality measures (eg, pain relief) is part of a good
hospice’s compliance and continuous quality improvement program. Recently,
this imperative has been added to the MHB conditions of participation, which
delineate the standards that must be followed to maintain Medicare certification
and payment for services [7].
Small programs may be financially challenged to admit patients who are
undergoing costly but helpful concurrent therapies (eg, palliative chemotherapy

fine & davis186
or radiation therapy, transfusions, hematologic- and immunologic-enhancing thera-
pies, interventional pain management, and similar therapies). Similarly, many
patients who have end-stage disease are receiving ‘‘aggressive’’ therapies
(eg, tube feedings, parenteral nutrition, and antiretroviral therapies) that are no
longer medically beneficial but have taken on significant symbolic value (ie, the
patient or family has become psychologically dependent on them). These patients
and their families need skilled help in making a transition to other more useful
forms of palliative and supportive therapy. Therefore, quality hospice programs
will have plans and capable staff in place to help with the transition from a ‘‘do
everything’’ mindset to ‘‘context appropriate’’ care, without preselecting patients
based on the level of complexity involved in their care. Because of financial
exigencies and current clinical expectations, it is becoming an economic reality
that consolidation of small programs is likely to be the only realistic way to
provide comprehensive, high-quality services to all hospice-eligible patients.
The National Hospice and Palliative Care Organization (NHPCO) (see Ap-
pendix), as part of its National Quality Initiative to improve end-of-life care,
benchmarks hospice programs nationally through a standardized Family Satis-
faction Survey tool. This survey tool is distributed to families after the death of
the patient and assays a diverse range of experiences, including pain control, the
efficiency of the after-hours staff, and timeliness from referral to admission to
the hospice program. Physicians and families can request the results and are
encouraged to do so when deciding on a program in their community.
Care settings and levels of care
Notwithstanding the historical roots of hospice in Great Britain as a com-
modious home specifically designed for care of the dying, hospice no longer
defines itself as a place per se but rather an applied approach to care. Hospice care
is provided in the patient’s own home, a nursing home, or, when appropriate to a
given set of circumstances, other facilities. By statute, Medicare-certified hos-
pices must provide inpatient care if it is needed. Similarly, there must be provi-
sions for extended hours of continuous nursing care if clinical circumstances
warrant it and respite care for families as dictated by each patient’s or family’s
clinical and social circumstances at any given time.
Some hospice programs maintain a separate ‘‘hospice house’’ for inpatient or
residential care, and others contract with long-term care facilities or hospitals to
provide inpatient care when this level of care is indicated. A 2004 compilation
by the National Hospice and Palliative Care Organization found that, of the
approximately 1 million patients cared for under hospice during that calendar
year, approximately 58% died at home, and approximately 22% died in a
nursing facility. The remaining 20% of the patients were in hospitals, hospice-
operated inpatient facilities, free-standing hospice units, or residential care set-
tings (S. Connor, NHPCO, personal communication, 2005).

hospice: comprehensive care at the end of life 187
Medicare hospice benefit
Most hospice care in the United States is reimbursed under the MHB, which
was first legislated in 1982. Currently, more than 90% of hospice programs in the
United States are certified by Medicare. Medicare beneficiaries who elect hospice
care may choose to receive a full range of palliative medical and support services
for their terminal illness. The MHB is covered under Medicare Part A in lieu of
standard Part A (hospital) benefits (Table 1) [6]. Because approximately 80% of
those dying in the United States are Medicare beneficiaries, this entitlement has
had an enormous impact on end-of-life care in this country. In fact, the only
operational definition of ‘‘terminal illness,’’ defined as a ‘‘prognosis of 6 months
or less if the disease runs its normal course,’’ comes from the legislative language
of the MHB. Although this is a rather arbitrary determination, with significant
inherent difficulties because of prognostic uncertainty [8], it has created some
structure around which to educate providers, patients, and their families, and to
construct guidelines for hospice eligibility under Medicare.
The Medicare Hospice Benefit has become the model for the coverage
provisions of most private insurers and state Medicaid programs. Medicare pays
Table 1
Provisions of the Medicare Hospice Benefit
Category Description of benefits
Criteria Eligible for Part A of Medicare
Terminally ill with a life expectancy of 6 months or less if disease runs its
normal course
Coverage Physician (hospice medical director) oversight
Nursing care
Case management
Medical appliances and supplies
Medications related to the terminal illness and palliation of symptoms
Speech therapy
Short-term inpatient and respite care
Physical and occupational therapy
Dietary counseling
Homemaker and home health aide services
Continuous care
Counseling and social work service
Spiritual care
Volunteer participation
Bereavement services
Timing Two 90-day certification periods
An unlimited number of subsequent 60-day periods
For the first 90-day certification period, hospice certification must be obtained from
both the beneficiary’s attending physician and the hospice medical director or the
physician member of the hospice interdisciplinary group. After that, other 60-day
periods require certification by only one physician.

fine & davis188
the hospice program a daily rate that is intended to cover all clinically indicated
expenses related to the patient’s terminal illness. Because patients may require
different intensities of care during the course of their disease, there are four
levels of care available, reimbursed at different rates: routine home care, con-
tinuous home care, inpatient respite care, and general inpatient care. More than
95% of hospice care is provided at the routine home care level.
Historically, most hospice patients were end-stage cancer patients, with rela-
tively short length of stays in hospice, and still today, 50% of cancer patients
admitted to hospice die in less than 1 week. Recent statistics show a median
length of stay of approximately 2 weeks for all patients. Over the last several
years, terminally ill patients who have noncancer diagnoses have been encour-
aged to take advantage of the myriad benefits of hospice care, and this trend
is increasing both the hospice use and the average lengths of stay. The MHB
requires that 80% of the total number of patient care days provided by a hospice
provider must be under the routine home care level of care and no more than
20% be under the Inpatient level of care.
The MHB is reimbursed through one of five Regional Home Health and
Hospice Intermediaries (RHHI), designated by the Centers for Medicare and
Medicaid Services (CMS): Palmetto Government Benefit Administrators, As-
sociated Hospital Service, United Government Services (two divisions), and
Cahaba Government Benefit Administrators. Each RHHI serves several states
(Table 2). The RHHIs have the authority and responsibility to assure that pay-
ment for services is justified, based on beneficiary or patient eligibility. For
hospice, a set of criteria for various diagnostic groups (initially called local medi-
Table 2
Medicare regional home care and hospice intermediaries
Provider States served
Palmetto GBA Alabama, Arkansas, Florida, Georgia, Illinois,
Indiana, Kentucky, Louisiana, Mississippi,
New Mexico, North Carolina, Ohio, Oklahoma,
South Carolina, Tennessee, Texas
Associated Hospital Service Connecticut, Maine, Massachusetts, New
Hampshire, Rhode Island, Vermont
United Government Services (Wisconsin) Michigan, Minnesota, New Jersey, New York,
Puerto Rico, the Virgin Islands, Wisconsin
United Government Services (California) Alaska, Arizona, California, Hawaii, Idaho,
Oregon, Nevada, Washington, Northern Mariana
Islands, Guam, American Samoa
Cahaba Government Benefit Administrators Colorado, Iowa, Kansas, Missouri, Montana,
Nebraska, North Dakota, South Dakota, Utah,
Wyoming, Delaware, District of Columbia,
Maryland, Pennsylvania, Virginia, West Virginia
Data from Centers for Medicare and Medicaid Services. Provider Enrollment. Available at: http://
www.cms.hhs.gov/providers/enrollment/providers/hospice.asp. Accessed June 6, 2005.

hospice: comprehensive care at the end of life 189
cal review policies but more recently renamed local coverage determinations
[LCDs]) were established several years ago. The criteria may differ among
intermediaries, and they are modified periodically at the discretion of the inter-
mediary. The LCDs outline specific clinical determinants of limited life expec-
tancy to support the assertion of a prognosis of 6 months or less (Table 3).
Hospice eligibility and use under Medicare
Notwithstanding the value of the MHB, notably the past 20-year history of
high marks for patient and family satisfaction, a minority of Medicare bene-
ficiaries take advantage of this entitlement. Election of the MHB seems to have
more to do with systems issues than with diagnosis or prognosis. For instance,
recent data indicate that Medicare beneficiaries enrolled in managed care plans
are more likely to use hospice (33%) than those with fee-for-service coverage
(25%) [9].
Under-usage of hospice has led the CMS, a branch of the federal Depart-
ment of Health and Human Services, to encourage physicians to consider
whether their patients are eligible for hospice care. Because life expectancy is not
commonly considered during routine office visits, a helpful aid for physicians
is to ask themselves, ‘‘Would I be surprised if this patient were to die from
progression or complications of their underlying chronic condition?’’ If the
answer is, ‘‘No, I would not be surprised,’’ then the physician should enter into
serious discussions about goals of care, a review of advance directives, and the
benefits versus burdens of hospitalization (including intensive care) and shift
the emphasis of clinical management to a palliative care focus, including hos-
pice referral.
The statutory language of the MHB simply states that a Medicare Part A
beneficiary is eligible for hospice if she or he has a life expectancy of 6 months or
less if the disease runs its normal (ie, typical, usual, or expected) course. Because
this is a statistical probability, based on a population of patients at the same stage
of an illness (eg, stage IV heart failure), any given patient may die far more
quickly or, conversely, live much longer than 6 months. The 6-month life expec-
tancy certification is based on the physician’s best clinical judgment. Neither
the physician nor the patient will be penalized if the patient lives longer than
6 months because the benefit may continue indefinitely, as long as there con-
tinues to be reasoned clinical judgment sustaining a prognosis of 6 months or
less. Being intimately familiar with the determinants of limited life expectancy,
many hospice programs can be of assistance by providing consultation services to
establish hospice eligibility (see below).
Contrary to popular belief, the MHB does not require that the patient have a
do-not-resuscitate order, nor is it mandated that any specific intervention (eg, tube
feedings, transfusions, or palliative chemo- or radiation therapy) be discontinued
to qualify for hospice.

Table
3
Localcoveragedeterminationcriteria
forhospiceeligibilityunder
medicare
Condition
Primarycriteria
Secondarycriteria/notes
Heartdisease
Patienthas
oris
Other
factors
supportingdiagnosisofend-stage
heartdisease:
1.A
poorresponse
to(orchoosesnotto
pursue)
optimal
treatm
entwithdiuretics,vasodilators,and/orACEinhibitors
1.Treatment-resistantsymptomatic
supraventricular
orventriculararrhythmias
2.Anginapectorisat
restthat
isresistantto
standard
nitrate
therapy
2.A
history
ofcardiacarrestorresuscitationand
unexplained
syncope
3.Notacandidateforordeclines
invasiveprocedures;and
3.A
brain
embolism
ofcardiacorigin
4.SignificantsymptomsofrecurrentCHFat
restand/or
refractory
angina
4.Anejectionfractionof20%
orless,and
5.Classifiedas
NYHA
IV5.ConcomitantHIV
disease
HIV
/AID
SPatientsareconsidered
tobein
theterm
inal
stageoftheir
disease
ifthey
have
Documentationofthefollowingfactors
willsupport
eligibilityforhospicecare:
1.CD4+count�25cells/mL
orpersistentviral
load
�100,000copies/mL,
plusoneofthefollowing:
1.Chronic
persistentdiarrhea
for1y
a.CNSlymphoma
2.Persistentserum
albumin
�2.5
g/dL
b.Loss
of33%
lean
bodymass
3.Concomitant,activesubstance
abuse
c.Mycobacterium
avium
complexbacteremia,untreated,
unresponsiveto
treatm
ent,ortreatm
entrefused
4.Age�50y
d.Progressivemultifocalleukoencephalopathy
5.Absence
ofantiretroviral,chem
otherapeutic,
and
prophylactic
drugtherapyrelatedspecifically
to
HIV
disease
e.System
iclymphoma,
withadvancedHIV
disease
and
partial
response
tochem
otherapy
6.AdvancedAID
Sdem
entiacomplex
f.VisceralKaposi’ssarcomaunresponsiveto
therapy
7.Toxoplasm
osis,and
g.Renal
failure
intheabsence
ofdialysis
8.Congestiveheartfailure,symptomatic
atrest
h.Cryptosporidium
infection;or
i.Toxoplasm
osis,unresponsiveto
therapy
2.Decreased
perform
ance
status,as
measuredbythe
KarnofskyPerform
ance
Statusscale,
of50%
fine & davis190

Pulm
onarydisease
Forpatientswithvariousform
sofadvancedpulm
onarydisease
who
eventually
follow
afinal
commonpathway
toend-stagepulm
onarydisease:
Tolendsupportingdocumentation:
1.Severechronic
lungdisease
asdocumentedbyboth
aandb:
1.Corpulm
onaleandrightheartfailure
secondary
topulm
onarydisease
(eg,notsecondaryto
left
heartdisease
orvalvulopathy)
a.Disablingdyspnea
atrest,unresponsiveto
bronchodilators,
withdecreased
functional
capacity;and
2.Unintentional
progressiveweightloss
ofgreater
than
10%
ofbodyweightover
thepreceding
6months,and
b.Progressionofend-stagepulm
onarydisease,evidence
includingpriorincreasingvisitsto
theem
ergency
departm
entorpriorhospitalizationsforpulm
onary
infectionsand/orrespiratory
failure
3.Restingtachycardia
�100/m
in
2.Hypoxem
iaat
restonroom
air;evidence:pO2�55mm
Hg
oroxygen
saturation�88%
orhypercapnia;evidence
pCO2�50mm
Hg
Renal
disease
Patientsareconsidered
tobein
theterm
inal
stageofrenal
disease
if
Supportingdocumentation
Forchronic
renal
failure:
Signsandsymptomsofrenal
failure:
1.Thepatientisnotseekingdialysisorrenal
transplant;or
consideringdiscontinuation
1.Uremia;
2.Creatinineclearance
�10cc
3/m
inute
(�15cc
3/m
infor
diabetes),and
2.Oliguria(�
400cc
3/d)
3.Serum
creatinine�8.0
mg/dL(�
6.0
mg/dLfordiabetes)a
3.Intractable
hyperkalem
ia(�
7.0)notresponsive
totreatm
ent
4.Uremic
pericarditis
5.Hepatorenal
syndrome,
and
6.Intractable
fluid
overload,notresponsive
totreatm
ent
ALS
Patientsareconsidered
tobein
theterm
inal
stageofALSif
oneofthefollowingthreesituationsoccurs
within
the12mo
precedinginitialhospicecertification:
Somegeneral
considerations
1.Criticallyim
pairedbreathingcapacityas
dem
onstratedby
allofthefollowingcharacteristics12mobefore
initial
hospicecertification:
1.ALStendsto
progress
inalinearfashionover
time,
sotheoverallrate
ofdeclinein
each
patientisfairly
constantandpredictable
Vital
capacityless
than
30%
ofnorm
al
Significantdyspnea
atrest
2.Multiple
clinical
param
etersarerequired
tojudge
theprogressionofALS
3.AlthoughALSusually
presentsin
alocalized
anatomic
area,thelocationofinitialpresentation
does
notcorrelatewithsurvival
time
(continued
onnextpage)
hospice: comprehensive care at the end of life 191

Table
3(continued)
Condition
Primarycriteria
Secondarycriteria/notes
ALS
Requiringsupplementaloxygen
atrest,and
Patientdeclines
artificial
ventilation
4.Progressionofdisease
differs
markedly
from
patientto
patient
5.In
end-stageALS,twofactors
arecritical
in
determiningprognosis:abilityto
breatheand,to
a
lesser
extent,abilityto
swallow
2.Rapid
progressionofALSandcritical
nutritional
impairm
ent
dem
onstratedbyallofthefollowingcharacteristics:
a.Rapid
progressionfrom
Independentam
bulationto
wheelchairorbedboundstatus
Norm
alto
barelyintelligible
orunintelligible
speech
Norm
alto
pureed
diet,and
Independence
inmostorallADLsto
majorassistance
by
caretaker
inallADLs
b.Criticalnutritional
impairm
ent:
Oralintakeofnutrientsandfluidsinsufficientto
sustainlife
Continuingweightloss
Dehydrationorhypovolemia,and
Absence
ofartificial
feedingmethods
3.Both
rapid
progressionofALSandlife-threatening
complications,includes
rapid
progressionofALS(see
2a
above)
and
a.Life-threateningcomplications:
Recurrentaspirationpneumonia
(withorwithout
tubefeedings)
Upper
urinarytractinfection(eg,pyelonephritis)
Sepsis,and
Recurrentfever
afterantibiotictherapy
fine & davis192

Stroke
Thefollowingareim
portantindicators
offunctional
andnutritional
status,respectively,
andsupportaterm
inal
prognosisifmet:
Ifthepatientdoes
notmeetboth
oftheprimary
criteria,thereshould
bedocumentationthat
describes
arelevantcomorbidityand/orrapid
decline
1.A
PalliativePerform
ance
scalescore
of�40%
a.Degreeofam
bulation;mainly
inbed
b.Activity/extentofdisease:unable
todowork;
extensivedisease
c.Abilityto
doself-care;
mainly
assistance
d.Food/fluid
intakenorm
alto
reduced
e.State
ofconsciousnesseither
fullyconsciousor
drowsy/confused
2.Inabilityto
maintain
hydrationandcaloricintake
withoneofthefollowing:
a.Weightloss
�10%
duringprevious6mo
b.Weightloss
�7.5%
inprevious3mo
c.Serum
albumin
�2.5
g/dL
d.Currenthistory
ofpulm
onaryaspirationwithout
effectiveresponse
tospeech
languagepathology
interventions,or
e.Caloriecountsdocumentinginadequate
caloric/fluid
intake
Alzheimer
disease
and
relateddisorders
ForAlzheimer
disease
andrelateddisorders,theidentificationof
specific
structural/functional
impairm
ents,together
withanyrelevant
activitylimitations,should
serveas
thebasisforpalliativeinterventions
andcare
planning.Thestructuralandfunctional
impairm
entsassociated
withaprimarydiagnosisofAlzheimer’sdisease
areoften
complicated
bycomorbid
and/orsecondaryconditions.
TheFASTscalehas
beenusedformanyyears
to
describeMedicarebeneficiaries
withAlzheimer
disease
andaprognosisof6moorless
TheFASTscaleisa16-item
scaledesigned
to
paralleltheprogressiveactivitylimitations
associated
withAlzheimer
disease
(continued
onnextpage)
hospice: comprehensive care at the end of life 193

Table
3(continued)
Condition
Primarycriteria
Secondarycriteria/notes
Alzheimer
disease
and
relateddisorders
Comorbid
conditionsaffectingbeneficiaries
withAlzheimer
disease
arebydefinitiondistinct
from
theAlzheimer
disease
itself.Exam
plesincludecoronaryheartdisease
andCOPD.
Secondaryconditionsaredirectlyrelatedto
aprimarycondition.
Inthecase
ofAlzheimer
disease,exam
plesincludedelirium
andpressure
ulcers.
FASTstage7identifies
thethreshold
ofactivity
limitationthat
would
supporta6-m
oprognosis
Ultim
ately,
thecombined
effectsofAlzheimer
disease
(FAST
stage7)andanycomorbid
orsecondaryconditionshould
be
such
that
thepatientwhohas
Alzheimer
disease
andsimilar
impairm
entswould
haveaprognosisof6moorless.
TheFASTscaledoes
notaddress
theim
pactof
comorbid
andsecondaryconditions
Abbreviations:
ACE,angiotensin-convertingenzyme;
ALS,am
yotrophic
lateralsclerosis;CHF,congestiveheartfailure;CNS,central
nervoussystem
;COPD,chronic
obstructivepulm
onarydisease;FAST,functional
assessmentstaging.
aSee
Ref.12foracute
renal
failure
criteria.
Data
from
SchonwetterRS,Chirag
RJ.Survivalestimationam
ongnoncancerpatientswithadvanceddisease.In:PortenoyRK,BrueraE,editors.Topicsin
palliativecare,
volume4.New
York:Oxford
University
Press;2000.p.55–74;NYHA,New
York
HeartAssociation.
fine & davis194

hospice: comprehensive care at the end of life 195
Hospice in the nursing home
The value of hospice care in the nursing home, to patients, their families, and
to the facility staff, seems to be increasingly appreciated. The proportion of
hospice patients residing in nursing homes is growing faster than the growth of
hospice enrollees as a whole, from 11% of all hospice patients in 1992 to 36% in
2000. Medicare requires a contract agreement between each hospice and the long-
term care facility, and there must be a documented, coordinated care planning
process in place for each hospice patient residing in the nursing home. This re-
quires good ongoing communication among hospice and nursing home person-
nel, especially the respective provider groups’ medical directors.
Recent developments in hospice care
The US Congress and CMS recently have made changes through the Medicare
Prescription Drug Improvement and Modernization Act of 2003 [10] to en-
courage use of the MHB benefit.
Consulting services
If a Medicare beneficiary is believed to be terminally ill and has not yet elected
the hospice benefit, Medicare will pay for a consultation visit with the hospice
medical director or physicians who are employees of a hospice program. During
this visit, the physician may evaluate the individual’s need for pain and symptom
management, counsel the individual on end-of-life issues and care options, and
give advice on planning end-of-life care. Hospices receive payment for this ser-
vice that is equal to the allowable Medicare fee for an outpatient visit of mod-
erate severity. In turn, the physician will be paid by the hospice.
Nurse practitioner services
It is recognized that nurse practitioners (NPs) are playing an increasing role
in primary care. With respect to hospice services, this provision changes the
definition of ‘‘attending physician’’ to include NPs, to help maintain continuity of
care between patient and primary care provider. It removes the disincentive for
nurse practitioners from actively promoting hospice care as an appropriate health
care choice for their patients who have advanced illnesses. However, this pro-
vision specifically excludes NPs from officially certifying a patient as termi-
nally ill, a determination that must be made by the hospice medical director
under these circumstances. As a result of this statutory change, NPs who are
not employed by a hospice are able to continue to bill Medicare for services
for their patients who elect hospice, as attending physicians do currently, and
to review and participate in the plan of care.

fine & davis196
Prognostication
Prognostication can be a difficult and delicate task, involving both sociologic
and physiologic judgments. Although death per se is a clear biological phenome-
non, perceptions about the meaning, eventuality, timing, and circumstances sur-
rounding death and dying are socially constructed. Consequently, prognosis can
be difficult to gauge with precision. Standard medical texts generally give the
subject short shrift, and there are few tools available to aid in the judgment.
Physicians may be aided through consultation with an experienced hospice medi-
cal director or palliative medicine practitioner who has experience in this area.
A study in 2000 by Christakis and Lamont [8] has found that prognostic
accuracy generally errs on the side of excessive optimism. Only 20% of surveyed
physicians’ prognoses were accurate within 33% of the actual survival time, 63%
of physicians were overoptimistic about life expectancy, and 17% of physicians
underestimated survival time. As the duration of the doctor-patient relationship
increased, prognostic accuracy actually decreased. There was an average 8-fold
overestimation of life expectancy for patients who died within 30 days of the
prognostic determination. These data strongly reinforce the need for research in
this area and for evaluating life expectancy with as many objective measures as
possible. Otherwise, patients will die without the benefits of hospice care.
Clinical judgment and atypical cases
Some frail, elderly patients manifest a pattern of diminishing vitality and seem
to be on a predictable trajectory toward imminent death but without a specific
pathophysiologic (ie, organ system-specific) diagnosis. Similarly, there are older
individuals with progressive functional impairment and continuous weight loss
who may have several chronic conditions (eg, hypertension, coronary artery dis-
ease, and diabetes) but no single imminently fatal disease process. They may have
a recent acceleration in functional or cognitive decline and may have decided not
to pursue aggressive medical evaluation or treatment because of advanced age,
poor general health, cognitive impairment, or excessive opportunity costs (high
burden-to-benefit determination). They, too, should be evaluated actively and
referred for hospice care as indicated. For these patients, hospice care is important
for their (and their family members’) overall well being at this critical life juncture,
so clinical judgment must come into play even more to assure timely referral to
hospice. The recognition of this within the medical community is evidenced by
the growing proportion of noncancer patients referred to hospice in recent years,
from 24% in 1992 to 43% in 1998 and to 49% of hospice caseloads in 2000.
In elderly patients, one of the most sensitive but nonspecific indicators of lim-
ited life expectancy is unintended weight loss (�10%) over a period of 6 months
or a body mass index (BMI) of less than 22 kg/m2 [11]. Patients of any age with
a BMI less than 20 kg/m2 who are ill enough to be hospitalized, regardless of
diagnosis have the highest overall mortality in the 6 months after discharge.

hospice: comprehensive care at the end of life 197
Coupled with weight loss, progressive difficulties with the activities of daily
living (ADLs) and limited functional capacity (inability to ambulate) are sensitive
predictors of 6-month mortality, independent of other disease-related variables [12].
These factors are important to recognize, document, and consider when caring for
these patients so that realistic and truly helpful conversations and care planning can
take place before crises occur or nonbeneficial therapies are begun.
Measuring clinical decline
The Karnofsky Performance Status scale was developed several decades ago
for cancer patients as an objective means of documenting a patient’s clinical
decline by assessing his or her ability to perform certain basic activities. Most
patients with a Karnofsky scale lower than 70% are eligible for hospice care
because this threshold signals progression to end-stage disease, unless there is a
predictably reversible cause of morbidity or a beneficial and sustaining anti-
neoplastic therapy that is both available and tolerable.
A more useful tool that can be applied to all patients to measure clinical
decline and aid in prognosis, irrespective of chronic progressive disease, is the
Palliative Performance Scale (PPS) [13,14]. The initial applications of the PPS
included its use as a communication tool, analysis of home nursing care work-
load, profiling admissions and discharges to the hospice unit, and prognostica-
tion. The investigators assessed 119 patients in their homes, 73% of whom had a
PPS rating between 40% and 70%. Of 213 patients admitted to the hospice unit,
175 (83%) had PPS ratings of 20% to 50% on admission. The average period
until death for 129 patients with PPS ratings of 10% on admission who died in
the unit was 1.88 days, 2.62 days at 20%, 6.70 days at 30%, 10.30 days at 40%,
and 13.87 days at 50%. Only two patients with a PPS score of 60% or higher died
in the unit.
On the PPS scale, a score of 50% indicates that the patient tolerates only
sitting or recumbency and requires considerable assistance with ADLs. A 40%
score identifies a patient who spends a majority of time in bed and requires
assistance with all ADLs, whereas a 30% score indicates that the patient is con-
fined to a bed and requires total care. Absent other comorbid conditions, a patient
is generally seen as eligible for hospice if the PPS score is 40% or less, without
the likelihood of improvement. Older patients with higher PPS scores accom-
panied by other morbid findings (eg, unintended weight loss and rapid decline in
physical or mental capacities) also should be evaluated for hospice care because
they too have predictably short life expectancies.
Needs of the patient and family
End-of-life care means different things to different people. Singer and col-
leagues [15] identified five factors that terminally ill patients felt were most

fine & davis198
important in their care: relief from unpleasant symptoms, the avoidance of pro-
longed dying, control over care decisions, the desire not to be a burden, and
strengthening relationships with loved ones.
For the patient (who has the greatest stake in obtaining high quality care but
often has the least decision-making capacity), the clinical imperative is for a
dignified transition from living to dying to death that occurs peacefully and
without discomfort. For the family, this is usually a time of reflection, family
restructuring, and sadness. It may also be a time of relief at the end of suffering
and exhausting care giving; however, often there also are feelings of regret and
guilt over missed opportunities and damaged relationships. For most clinicians,
end-of-life situations occur regularly, and although these may be considered to
be an unavoidable part of the profession, there is usually little formal training
to prepare for the myriad issues that attend the imminent and actual death of a
patient. As a result, it is common for denial, emotional distancing, or a personal
or professional sense of defeat to prevail. Establishing a relationship with a
quality hospice program can help clinicians meet their professional responsibili-
ties to their patients and to obtain a greater sense of competency, even mastery
and profound personal and professional growth, in dealing with dying, death,
recurrent grief, and bereavement.
Barriers to hospice access
Difficulties with facing and discussing death and dying by patients, families,
and clinicians continue to be the major reason that hospice is underused and so
many patients are referred late in the course of a terminal illness.
Difficult conversations
Larson and Tobin [16] elaborate several reasons why clinicians may shy
away from end-of-life conversations. The efforts of the modern era of medical
care have been focused on curing or, at least, stabilizing serious illness and
rescuing patients from imminent death. Fear of failure, causing pain and dis-
appointment through admitting and sharing news about a negative prognosis,
and the lack of knowledge of how to proceed with practical and interpersonal
details related to death may delay the conversation. Clinicians who see death as
an enemy to be defeated will perceive a recommendation to hospice as a de facto
admission of defeat. Anticipating disagreements or discomfort with the patient
or family and worrying about medical-legal concerns can make discussions
about end-of-life care difficult, as well. Simply, it is far easier and in confor-
mance with our cultural norms for clinicians and patients and families to prac-
tice avoidance.
Physicians and other health care providers also are less likely to initiate end-
of-life discussions when they lack the needed interpersonal and communication

hospice: comprehensive care at the end of life 199
skills. These skills are no more innate than is pharmacologic expertise, but
training in these skills and in how to have conversations with dying patients is
rarely included in medical school curricula, nor is it commonly modeled during
postgraduate bedside training [17]. It should be noted that, according to the
NHPCO Family Satisfaction Survey, when asked if there is anything they would
change, the most common response by family members receiving hospice care is
that they wish they would have been referred sooner to hospice or, specifically,
‘‘why didn’t my doctor tell me about hospice sooner?’’ (S. Connor, NHPCO,
personal communication, 2005).
Cultural issues
Racial and cultural barriers to accessing hospice services exist, and geographic
location (eg, rural communities and inner cities) clearly affect access to hospice
care [18]. In 2002, 82% of hospice patients identified themselves as white, a rate
that has held steadily since 2000. Although each ethnic and racial group holds a
wide variety of attitudes, there is some evidence for shared views within similar
populations. For example, African Americans express suspicion of their health
care providers’ motives more so than other populations. When there is concern
about the fair distribution of resources and equal access to life-saving health care,
concern about premature referral to hospice is understandable.
Other cultural barriers include religious beliefs that balk at the idea of an
‘‘ending’’ to life, an acceptance of suffering as part of the nature of being human,
and other beliefs about death that prohibit approaching the subject openly and
frankly. Although it is important for clinicians to understand the general cultural
and ethnic beliefs of their patients, each case must be approached individually
because any assumptions may lead to even wider misunderstandings.
Support for caregivers
Counseling services for patients and families are an important part of hospice
care, but there are few outcomes studies that go beyond anecdotal reports. A
review of families’ needs in critical care settings by Hickey [19] has found that
families rated information needs are the most important, followed by needs for
reassurance and convenience.
After the patient’s death, Medicare rules require that bereavement support
be available to families for at least 1 year. These services can take a variety of
forms, including telephone calls, visits, written materials about grieving, and
support groups. Individual counseling may be offered by the hospice, or the
hospice may make a referral to a community resource. For long-term care staff,
hospice-provided bereavement follow-up may take the form of a monthly
memorial service, support groups, or debriefings facilitated by counselors of the
hospice program.

fine & davis200
Physicians and hospice: billing for hospice services
Once a patient is determined to be eligible for hospice care and is enrolled,
several physicians may have involvement in the patient’s care. The patient can
request that her or his attending physician retain that role or the hospice medical
director can take over that designation, at the discretion of the patient’s physician
and the patient. Often, this latter decision is made to simplify decision making
and as an acknowledgment of the hospice physician’s expertise in end-of-life
care. Under the provisions of the Medicare Hospice Benefit, the attending
physician is the clinician whom the patient designates as having the primary role
in the determination and delivery of the individual’s medical care. As described
earlier, as of October 1, 2004, NPs may function in the attending role for hos-
pice patients, at the patient’s discretion. Under this new provision, NPs may
bill Medicare Part B for physician services related to their hospice patients’
terminal illnesses.
Hospice medical directors may bill for physician services to hospice patients,
but those services are paid by Medicare Part A. The patient’s choice of the at-
tending is not absolute, and the patient is free to change the attending physician
or NP. The attending clinician provides orders and, if not the hospice medical
director, often defers to the hospice medical director for medical components of
the hospice plan of care because the medical director tends to be the medical
provider most closely involved in daily clinical care of the patient.
A consulting physician is any nonattending, nonmedical director physician
who provides a service as a part of the hospice plan of care. There must be a
contract between the consultant and the hospice for these services, and the hos-
pice is the manager of the care. The hospice directly reimburses the consultant
physicians for services.
Any attending clinician who is not employed by the hospice (this generally
includes all clinicians except the hospice medical director) can bill Medicare
Part B for Physician Care Plan Oversight (CPT 99,378) if he or she has seen
the patient within 6 months of billing for oversight for the first time, the pa-
tient is not a nursing facility resident, and there were 30 minutes or more of
oversight activity not related to any other separately billable activity in a calen-
dar month. Professional services should be billed by the attending to Medicare
Part B, and the physician or NP will receive 80% of the Medicare-allowable fee.
The patient is still responsible for any remaining deductible and co-insurance.
The attending clinician must indicate that he is not employed by the hospice
on the claim. It is important to verify exact procedures with individual states’
Medicare Part B carrier.
Criteria for Medicare coverage and payment for services are federally regu-
lated and generally do not vary over geographic regions. Private insurers usually
follow the same criteria as Medicare in determining reimbursement rates for
hospice services. For example, both the Oxford Health Plan and Aetna Insurance
Company cover hospice care at no additional charge for 210 days under many
of their plans.

hospice: comprehensive care at the end of life 201
Hospice services for children
According to the most recent figures from NHPCO, hospice serves ap-
proximately 5000 young adults, adolescents, and children under the age of 24
(S. Connor, NHPCO, personal communication, 2005). This number reflects ap-
proximately 20% of those who die each year within this age group in the United
States. Children’s services usually are covered through a variety of private and
public payers because children do not meet Medicare eligibility requirements.
Charitable funding by most hospice programs covers uncompensated care to
children who are not covered under Medicaid and whose families have limited
insurance coverage.
There also are programs such as the Children’s Hospice International (CHI)
Program for All-Inclusive Care for Children and their Families (PACC), which
provides a continuum of care for children and their families from the time that a
child is diagnosed with a life-threatening condition, with hope for a cure, through
the bereavement process, if cure is not found. The CHI PACC model programs
are funded by government grants through the US Department of Health and
Human Services. Model programs are being implemented currently in Colorado,
Florida, Kentucky, New York, Utah, and Virginia. Demonstration programs will
soon be expanded to additional states (see Appendix).
Summary
When life expectancy is short, time is precious. Technologic advances have
given us great power to prolong life but also to prolong dying, a critically im-
portant distinction that patients may not be able to avoid without sagacious
guidance. Understanding patients’ values and goals and assisting them and their
loved ones to come to terms with mortality is a difficult but necessary task, to
help patients avoid unnecessary suffering and to obtain the best care at this final
stage of life. Aiding patients and their families in finding renewed hope through
optimizing quality of life and completing (as much as is possible) the ‘‘unfinished
business’’ of their lives is both an acknowledgment and fulfillment of the im-
peratives of medicine: to value life, restore health when possible, and relieve
suffering always. Hospice is a tangible means to those ends.
Appendix
Online resources for clinicians
The National Hospice and Palliative Care Organization (NHPCO) (www.
nhpco.org) is the largest nonprofit membership organization representing
hospice and palliative care programs and professionals in the United States.

fine & davis202
NHPCO offers information for health providers and patients, including
conferences, courses, updates, and more [20].
The American Academy of Hospice and Palliative Medicine (AAHPM)
(www.aahpm.org) is an organization of physicians and other medical pro-
fessionals that helps to educate health professionals on palliative medicine
and hospice care, as well as training physicians, preparing physicians to
become medical directors of hospice, and other services [21].
The End-of-Life Nursing Education Consortium (ELNEC) project (www.
aacn.nche.edu/elnec/about.htm) is a comprehensive, national education
program to improve end-of-life care by nurses. Primary project goals are to
develop a core of expert nursing educators and to coordinate national
nursing education efforts in end-of-life care. This group offers courses and
educational materials for nurses [22].
The EPEC Project–Education for Physicians on End-of-life Care (http://www.
epec.net/EPEC/webpages/index.cem) was developed by the American
Medical Association to aid in educating physicians in the United States
on the clinical competencies required to provide quality end-of-life care.
The project provides courses, manuals, and modules with practical advice
on end-of-life care [23].
The Hospice Foundation of America (HFA) (www.hospicefoundation.org)
provides resources and teleconferences on end-of-life topics for both health
professional and patients [24].
Medical College of Wisconsin Palliative Care Program (www.eperc.mcw.
edu/display/router) is committed to improving care for dying Americans
by developing and implementing ideas and solutions by professional care-
givers and institutions [25].
National Association for Home Care (NAHC) (www.nahc.org) serves the
home care and hospice industry [26].
Online resources for patients, families, and caregivers
Children’s Hospice International (CHI) (www.chionline.org) is a nonprofit or-
ganization that provides education, training, and technical assistance to
those who care for children with life-threatening conditions and their
families [27].
Americans for Better Care of the Dying (ABCD) (www.abcd-caring.org) is a
group that helps organizations and individuals institute improvements in
community care systems. They offer concrete advice and advocacy [28].
Promoting Excellence in End-of-Life Care (www.promotingexcellence.org)
works to provide long-term changes in health care for dying people and
their families. They are involved with demonstration projects and peer
workgroups that address the challenges to existing models of hospice and
palliative care [29].
Caregiver Survival Resources (www.caregiver911.com) is a resource designed
to help people cope with the demands of caregiving [30].

hospice: comprehensive care at the end of life 203
Dying Well (www.dyingwell.com) offers resources for patients and their fami-
lies when facing life-limiting illnesses [31].
Medicare Rights Center (www.medicarerights.org) provides free counseling
services to Medicare beneficiaries [32].
National Family Caregivers Association (http://nfcacares.org) helps caregivers
adjust to their lives and encourages the living of a whole life [33].
References
[1] Fine PG. Hospice care. In: Christensen AJ, Martin R, Smyth JM, editors. Encyclopedia of
health psychology. New York7 Kluwer Academic/Plenum Publishers; 2004.
[2] Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place
of care. JAMA 2004;291(1):88–93.
[3] Connor SR, Tecca M, Lund-Person J, et al. Measuring hospice care: the National Hospice and
Palliative Care Organization national hospice data set. J Pain Symptom Manage 2004;28(4):
316–28.
[4] Hong G, Fine PG, Mendoza TR, et al. A validation study of the Brief Hospice Inventory. J Pain
Symptom Manage 2001;22:637–48.
[5] SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized
patients: the Study to Understand Prognoses and Preferences for Outcomes and Risks of
Treatment (SUPPORT). JAMA 1995;274:1591–8.
[6] Title 42, Public Health Chapter IV, Health Care Financing Administration, Department Of
Health And Human Services, Part 418, Hospice care. Code of Federal Regulations, Title 42,
volume 2, parts 400–429 (revised October 1, 2000). US Government Printing Office. p. 781–99
[Available at: http://www.access.gpo.gov/nara/cfr/waisidx_00/42cfr418_00.html. Accessed
December 8, 2005].
[7] Department of Health and Human Services, Centers for Medicare and Medicaid Services.
Medicare and Medicaid programs: hospice conditions of participation: proposed rule. Fed Reg
2005;70(102):30840–93.
[8] Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally
ill patients: prospective cohort study. BMJ 2000;320:469–72.
[9] McCarthy EP, Burns RB, Ngo-Metzger O, et al. Hospice use among Medicare managed care and
fee for service patients dying with cancer. JAMA 2003;289:2238–45.
[10] Medicare Prescription Drug Improvement and Modernization Act, Public Law 108-173 (2003).
[11] Schonwetter RS, Chirag RJ. Survival estimation among noncancer patients with advanced
disease. In: Portenoy RK, Bruera E, editors. Topics in palliative care, volume 4. New York7
Oxford University Press; 2000. p. 55–74.
[12] Reisberg B. Functional assessment staging (FAST). Psychopharmacol Bull 1998;24:653–9.
[13] Victoria Hospice Society. Palliative performance scale, 2001. version 2. Available at: http://www.
victoriahospice.org/pdfs/PPSv2.pdf. Accessed December 27, 2005.
[14] Anderson F, Downing GM, Hill J, et al. Palliative performance scale (PPS): a new tool. J Palliat
Care 1996;12:5–11.
[15] Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ perspectives. JAMA 1999;
281:163–8.
[16] Larson DG, Tobin DR. End-of-life conversations: evolving practice and theory. JAMA 2000;
284:1573–8.
[17] Truog RD, Cist AF, Brackett SE, et al for the Ethics Committee of the Society of Critical Care
Medicine. Recommendations for end-of-life care in the intensive care unit. Crit Care Med
2001;29:2332–48.
[18] Jennings B, Ryndes T, D’Onofrio C, et al. Access to hospice care: expanding boundaries,
overcoming barriers. Hastings Cent Rep 2003;March–April(Suppl):S30–9.

fine & davis204
[19] Hickey M. What are the needs of families of critically ill patients? a review of the literature since
1976. Heart Lung 1990;19:401–15.
[20] National Hospice and Palliative Care Organization (NHPCO) Web site. Available at: http://
www.nhpco.org. Accessed December 27, 2005.
[21] American Academy of Hospice and Palliative Medicine (AAHPM) Web site. Available at:
http://www.aahpm.org. Accessed December 27, 2005.
[22] End-of-Life Nursing Education Consortium (ELNEC) Web site. Available at: http://www.
aacn.nche.edu/elnec/about.htm. Accessed December 27, 2005.
[23] EPEC Project–Education for Physicians on End-of-life Care Web site. Available at: http://
www.epec.net/EPEC/webpages/index.cem. Accessed December 27, 2005.
[24] Hospice Foundation of America (HFA) Web site. Available at: http://www.hospicefoundation.
org. Accessed December 27, 2005.
[25] Medical College of Wisconsin Palliative Care Program Web site. Available at: http://www.
eperc.mcw.edu. Accessed December 27, 2005.
[26] National Association for Home Care (NAHC) Web site. Available at: http://www.nahc.org.
Accessed December 27, 2005.
[27] Children’s Hospice International Web site. Available at: http://www.chionline.org. Accessed
December 27, 2005.
[28] Americans for Better Care of the Dying (ABCD) Web site. Available at: http://www.abcd-caring.
org. Accessed December 27, 2005.
[29] Promoting Excellence in End-of-Life Care Web site. Available at: http://www.promotingexcellence.
org. Accessed December 27, 2005.
[30] Caregiver Survival Resources Web site. Available at: http://www.caregiver911.com. Accessed
December 27, 2005.
[31] Dying Well Web site. Available at: http://www.dyingwell.com. Accessed December 27, 2005.
[32] Medicare Rights Center Web site. Available at: http://www.medicarerights.org. Accessed
December 27, 2005.
[33] National Family Caregivers Association Web site. Available at: http://nfcacares.org. Accessed
December 27, 2005.