Embed Size (px)
Citation preview

Hospital Family Reunification: Debut of a New AAP Tool
Children’s Hospitals and Preparedness WebinarFriday, June 29, 2018, at 2:00pm ET/1:00pm CT

OBJECTIVES
1. Describe the importance of having a hospital reunification plan.
2. Outline the key components that should be included in a hospital’s family reunification plan.
3. Identify where to find the most up-to-date guidance, recommendations, and resources.

TECHNICAL SUPPORT
• Type issue into the chat feature
• Call 800-843-9166
• Email [email protected]
Q & A• Submit questions at any time through the chat box
• Over the phone, call 800-289-0459, ID #512312
• Dial *1 on your phone to ask a live question

PRA CREDITS STATEMENT• The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing
Medical Education (ACCME) to provide continuing medical education for physicians.
• The AAP designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
• This activity is acceptable for a maximum of 1.0 AAP credits. These credits can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Members of the American Academy of Pediatrics.
• The American Academy of Physician Assistants (AAPA) accepts certificates of participation for educational activities certified for AMA PRA Category 1 Credit™ from organizations accredited by the ACCME. Physician assistants may receive a maximum of 1.0 hours of Category 1 credit for completing this program.
• Successful completion of this CME activity, which includes participation in the activity, with individual assessments of the participant and feedback to the participant, enables the participant to earn 1 MOC points in the American Board of Pediatrics’ (ABP) Maintenance of Certification (MOC) program. It is the CME activity provider’s responsibility to submit participant completion information to ACCME for the purpose of granting ABP MOC credit.

FACULTY
Sarita Chung, MD, FAAPDirector, Disaster PreparednessDivision of Emergency MedicineBoston Children’s HospitalBoston, MA
Member, American Academy of PediatricsDisaster Preparedness Advisory Council
Insert Photo Here

FACULTY
Rachel Charney, MD, FAAPPediatric Emergency MedicineSSM Health Cardinal Glennon Children's HospitalSt Louis, MO

DISCLOSURES
• The presenters have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in this activity.
• The presenters do not intend to discuss an unapproved/investigative use of a commercial product/device in this presentation.
• The photographs shown in this presentation were acquired via free domain Web sites.

Hospital Family Reunification: Debut of a New AAP Tool
Sarita Chung, MD, FAAPRachel Charney, MD, FAAP


NEED FOR REUNIFICATION
Hurricane Katrina, 2005 Border Crisis, 2018

HOSPITALS = PART OF THE SOLUTION

HOSPITAL EXPECTATIONS
Assumptions Reality
My hospital will not be affected - we are not a trauma center
Scoop and Run• “Siri”
My community has a family reunification plan
Families will head to hospitals first• Community family assistance
centers take time to set up
My hospital already has a plan That’s great - but make your spaces bigger. Drill to failure.

FAMILY EXPECTATIONS
Assumptions Reality
Families expect all hospitals have a plan to reunite families after a disaster
Peds Ready Data:• Only 47% of EDs report having a
disaster plan that addresses children
Families expect immediate identification and reunification of all victims, living or deceased
Hospitals will not have that information• Identity of deceased victims may
take days, weeks

DEVELOPMENT OF THE AAP FAMILY
REUNIFICATION TOOL
2016 AAP Disaster Reunification Subcommittee

HIGHLIGHT: AAP FAMILY REUNIFICATION TOOL
❑Beginning the Planning Process❑Needs Assessment
❑Assembling an Internal Planning Team
❑External Stakeholder Involvement
❑Essential Elements of Hospital Family Reunification Plan

BEGINNING THE PLANNING PROCESS
• Needs Assessment
– Unique patient population and community characteristics
– Logistical needs
– Hospital Space
▪ Hospital Family Reunification Center
▪ Pediatric Safe Area
▪ Family Reunification Site
Sample Reception/Family Waiting Area

ASSEMBLING AN INTERNAL TEAM
Adjunct Hospital Departments for Family Reunification Planning
• Public Affairs / Media Relations
• Risk Management
• Psychiatry / Behavioral Health
• Telecommunications
• Health Information Management
• Front Desk / Greeter Staff
• Nutrition / Food Services
• Chaplaincy
• Interpreter Services
• Patient Relations / Family
Advisory Group
Key Hospital Departments for Family Reunification Planning
• Pediatrics
• Family Medicine
• Child Life Services
• On-site Child Care
• Security
• Nursing
• Social Work
• Emergency Medicine
• Emergency Management
• Legal Counsel

EXTERNAL STAKEHOLDERS
• Goal is to prevent duplication of effort

ESSENTIAL ELEMENTS OF HOSPITAL FAMILY
REUNIFICATION PLAN
Essential Plan Elements 1. Leadership and Organization2. Registration, Intake & Tracking
of Unaccompanied Children3. Definitive Identification4. Hospital Family Reunification
Center (HFRC)5. Pediatric Safe Area6. Family Reunification Site7. Information Sharing

LEADERSHIP & ORGANIZATION
• Family Reunification typically falls within the Operations Section of the Hospital Incident Command System (HICS)
Family Reunification Branch Director
Patient Tracking and Identification Unit
Leader
Hospital Family Reunification Center (HFRC) Unit Leader
Pediatric Safe Area Unit Leader
Family Communications
Unit Leader

REGISTRATION, INTAKE AND TRACKING OF
UNACCOMPANIED CHILDREN• Modified Registration
– EMS Hospital
• Hospital Tracking system
– Health Information Management
• Tiered Process to get extra data
– Visible identifiers for unaccompanied children
Data Elements to Support Reunification Efforts
1. Patient’s full name
2. Parent/guardian name(s)
3. Nicknames for child and parent/guardian(s)
4. Date of birth (or approximate age if unable to obtain)
5. Weight
6. Height
7. Race/ethnicity
8. Cultural, linguistic (languages spoken), and other special needs (e.g. allergies, medical
conditions, medications, etc.)
9. Hair color and length of hair
10. Eye color
11. Gender
12. Distinguishing marks on the body (may include tattoos, scars, missing teeth, etc.)
13. Clothing worn on initial arrival, along with significant belongings (stuffed animal, etc.)
14. Location and mechanism of arrival/presentation to the system
15. Photo (if system is capable)
16. Association with disaster event (to aid in reporting all patients associated with incident)

GATHERING INFORMATION

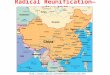
PARENTAL TRUST
0 20 40 60 80 100
Out-of-state gov't
University
United Way
Federal gov't
State gov't
Public health
Local gov't
Red Cross
NCMEC
Hospital
Parental Trust in Agencies and Organizations (%)
You are it!

DEFINITE PATIENT IDENTIFICATION
• Usual hospital procedures
• Majority of children will be able to self identify
• Confirmation– Identifies self or has
identification
– Photographs, biometrics or trusted person can confirm
– Match to answers to questions
• Example QuestionsParent’s Name(s)
Contact Number
Family’s Address
Child’s Name
Child’s Medical Record Number
Child’s Birth Date
Child’s Age
Patient Identifiers
Hair Color
Eye Color
Clothing
Shoes
Jewelry
Other
Name of School/Grade
Teacher’s Name(s)
Pets – Name, Type of Animal(s)

HOSPITAL FAMILY REUNIFICATION CENTER (HFRC)• Where families are placed
when arriving at the hospital seeking missing children
• Staff to assist in– Gathering information
– Providing psychological first aid
– Providing updates
• Away from ED, Pediatric Safe Area, and media staging sites
• Checklist for suppliesSample Family Briefing/Assembly Area

PEDIATRIC SAFE AREA
• Area for unaccompanied pediatric patients who are medically cleared
• Secure location, away from but close to the ED (and near bathrooms)
• Staff
– Reassure children
– Medical presence
• Age appropriate
– Supplies
– Food

FAMILY REUNIFICATION SITE
• Separate location to reunite children and their caregivers
• Away from the Hospital Family Reunification Center
– Avoid trauma to families still waiting for news
– Do not want separate exits for deceased and living
• Away from the Pediatric Safe area
– Avoid other children seeing families reunited

INFORMATION SHARING
• Establish close partnerships with external response organizations
• Consider the following:– Impact of HIPAA and
other laws, regulations, & policies
– Pre-messaging– Message coordination
for consistency– Staff messaging and
preventing inappropriate information leakage
• Role of PIO• Social Media
– Control the message with families and children

STAFFING AND SECURITY
• Staffing for all required areas, including increased supervision needs
• Security Concerns:
– Increased security risks
– Crowd control
– Criminal investigation
– Interaction with outside law enforcement

PLAN ACTIVATION

EXERCISING FAMILY REUNIFICATION PLANS
• Tabletop Exercises– Assessment of overall assumptions and operations of the
family reunification plans
• Drills– Test of physical set up of the Hospital Family Reunification
Center, Pediatric Safe Area, Family Reunification site
• Functional Exercises– Measuring communication between all areas
• Full Scale Exercises– Assessment of overall physical operations coordination of
all components of the hospital family reunification plan

ACKNOWLEDGMENTS
• AAP Disaster Reunification Subcommittee and Staff
• Paul Biddinger MD, FACEP
• Rob Krupa MS, AEM
• Massachusetts stakeholder group
• Missouri stakeholder group
• Reviewers

RESOURCES• AAP Children & Disasters Web Site (www.aap.org/disasters)
• AACAP Disaster Resource Center (www.aacap.org/aacap/Families_and_Youth/Resource_Centers/Disaster_Resource_Center/Home.aspx)
• ASPR TRACIE Family Reunification and Support (https://asprtracie.hhs.gov/technical-resources/64/family-reunification-and-support/60)
• FEMA How Do I Find My Family? (https://www.fema.gov/how-do-i-find-my-family)
If you have resources that you think should be shared with the AAP Family Reunification Tool, please email details to [email protected].

CME/MOC CREDIT
• Complete the post activity survey.
• Only physicians can claim MOC Part 2 credit. A quiz for MOC Part 2 credit will be included in the post activity survey.
• Physicians must identify their ABP ID number.
AAP staff will email each person claiming CME/MOC 2 credit with their certificate of completion. Email [email protected] with any questions.

QUESTIONS?• Dial *1 on your phone to ask a live question.
• Phone: 800-289-0459
• Conference ID: 512312
• Can ask questions through chat box in lower left corner. AAP staff or presenters will address unanswered questions via e-mail after the call.
Please e-mail [email protected] to
receive info on future events, or
follow-up as needed.

This webinar is supported by cooperative agreement number, 5 NU380T000167-05-00 funded by the Centers for Disease Control and
Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the US Department of Health and Human
Services.