Embed Size (px)
Citation preview

Hospitals’ Provision of Community Benefit: Is there a Trade-off between Charity Care and other Community Benefit Activities?
Simone Rauscher, PhD
Daniel Rubin, JD(c), PhD(pc)
Mark Vyzas, BS, MHSA(c)

Presenter DisclosuresSimone Rauscher, Daniel Rubin, Mark Vyzas
• The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
No relationships to disclose for any of the three presenters listed above.

Motivation
• In exchange for tax exemptions, not-for-profit hospitals are required to provide a public benefit to the community
• Traditionally, hospitals have focused on charity care to justify tax exemptions
• Affordable Care Act (ACA) is expected to decrease need for charity care, so community benefit activities other than charity care will gain in importance
• Little is known currently about hospitals’ provision of community benefits besides charity care

Legal Background
• The Internal Revenue Services’ community benefit standard is the touchstone for the exemption of not-for-profit hospitals from federal taxation
• Charity care has been the central feature of this standard
• Historically, most states and localities have adopted this same standard for the purposes of state and municipal tax exemption

Legal Developments
• With the passage and implementation of the ACA, the number of uninsured individuals will be reduced, and the need for charity care will diminish– This calls into question the current focus on charity care
• State innovation: Increasingly, states have implemented their own standards– Reporting requirements– Minimum standards– Increased accountability
• Federal innovation: IRS redesigned Form 990 Schedule H– Reporting requirements– Increased accountability

Research Questions
• How much community benefit besides charity care do not-for-profit hospitals provide?
• What are the relationships among different elements of hospitals’ community benefit activities?
Do hospitals that provide more free and reduced cost care spend more or less on other community benefits?

Data and Sample
• Since IRS data is just becoming available, we used state-level data from California hospitals’ community benefit reports
• Community benefit information was for the year 2009
• Sample was limited to 91 of 218 hospitals (42%)– State provided reports for 141 hospitals– 50 hospitals were excluded because of insufficient
financial information or because reports were not at individual hospital level

Sample Representativeness
Final sample (n=91)
All hospitals (n=232)
Number of beds 198 171
System affiliation**
59% 71%
Av. length of stay 4.7 days 4.7 days
Occupancy rate 65.1% 63.3%
Operating margin 2.5% 2.5%
Total margin 2.7% 2.7%Table shows medians; ** denotes statistically significant difference in means at 5% level.

Measures of Community Benefits
• Charity care – Unreimbursed cost of free care provided to patients who are unable to pay
• Government payer payment shortfalls – Unreimbursed cost of care provided to patients in means-based government programs
• Other community benefits – Unreimbursed cost of all other community health services
To facilitate comparisons, all measures are expressed in terms of dollars per adjusted discharge

Median Expenditures per Adjusted Discharge
Statistical Analysis
• Nonparametric Spearman’s rho correlation coefficients to test relationships among key community benefit indicators
Is there any—not necessarily linear—relationship between any two of the three community benefit indicators?

Charity Care and Government Payer Payment Shortfalls
corr = 0.28
(p=0.009)
05
001
000
150
0C
CP
erA
DjD
is
0 1000 2000 3000 4000GovProgPerAdjDis
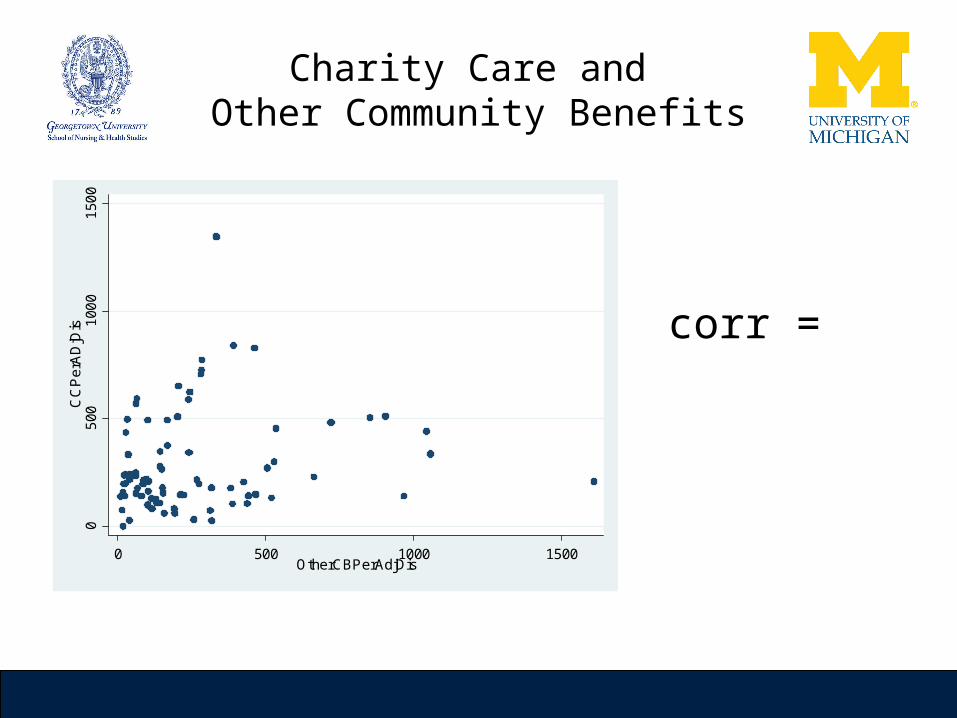
Charity Care and Other Community Benefits
corr = 0.22
(p=0.048)
05
001
000
150
0C
CP
erA
DjD
is
0 500 1000 1500OtherCBPerAdjDis

Government Payer Payment Shortfalls and Other Community Benefits
corr = 0.27
(p=0.014)
01
000
200
03
000
400
0G
ovP
rogP
erA
djD
is
0 1000 2000 3000 4000OtherCBPerAdjDis

Summary and Discussion
• California hospitals provide substantial community benefits besides charity care and government payer payment shortfalls– Other community benefits ≈ 20% of spending
• Reduced need for charity care as a result of ACA will likely be more than offset by
Increased government payer shortfalls due to greater numbers of
Medicaid-eligible patients
Increased spending on other community benefits due to new requirements (e.g.,
community needs assessments)
Summary and Discussion
• For California hospitals, there is no trade-off between charity care and other community benefits
• Hospitals that currently provide substantial charity care to justify tax exemptions also provide substantial other community benefits
Even as need for charity care declines, these hospitals are in good shape
• Hospitals that currently provide little charity care do not compensate for their below-average spending
Revised Form 990 will increase transparency and require these hospitals to rethink their approach to community benefit

Thank You
Any Questions or Comments?
Contact information:
Simone Rauscher, PhDPhone: (202) 687 - 6628
Email: [email protected]





























