Embed Size (px)
Citation preview
![Page 1: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/1.jpg)
September 2017⎪Vol. 27⎪No. 9
J. Microbiol. Biotechnol. (2017), 27(9), 1549–1558https://doi.org/10.4014/jmb.1705.05032 Research Article jmbReview
Host-Directed Therapeutics as a Novel Approach for TuberculosisTreatmentYe-Ram Kim1,2 and Chul-Su Yang1,2*
1Department of Molecular and Life Science, Hanyang University, Ansan 15588, Republic of Korea2Department of Bionano Technology, Hanyang University, Seoul 04673, Republic of Korea
Introduction
Tuberculosis (TB), which is caused by infection with
Mycobacterium tuberculosis (MTB), is a global health
problem with significant lethality [1]. In 2015, 10.4 million
people were infected with TB, and 1.8 million people died
because of the disease, including 0.4 million people who
were coinfected with human immunodeficiency virus (HIV).
This is significant because in that same year, 35% of HIV-
related deaths were caused by TB. In 2015, approximately
480,000 people had multidrug-resistant TB (MDR-TB), and
9% of TB patients were infected with an MTB strain that
was classified as extensively drug-resistant TB (XDR-TB).
Treatment of these resistant strains requires a considerably
long duration, with toxic side effects and at a great expense
[2]. For the past 40 years, TB therapy has used a combination
of effective anti-TB drugs to manage active infections.
Generally, TB needs to be treated for 6 months and XDR-TB
for 12–18 months. Furthermore, the current therapy for
XDR-TB is effective in only 50% of cases and imposes a
severe financial burden on patients [3]. Current anti-TB
drugs have other limitations such as adverse effects and
interactions with other drugs [4]. In addition, patients
experience abnormal host inflammatory responses caused
by permanent lung tissue damage [5]. Therefore, novel
therapeutic strategies are required to treat these difficult TB
cases. One novel approach, termed host-directed therapeutics
(HDTs), involves directly targeting host factors rather than
pathogen components [6]. HDTs also reduce pathogen
proliferation and the hyperinflammatory response by
modulating the host immune system [7]. HDTs have
improved clinical outcomes with reduced morbidity,
mortality, organ damage, and TB therapy duration.
Current Anti-TB Drugs
Treatment with first-line anti-TB drugs (Table 1) is a two-
step process that was developed from 1950 to 1960;
treatment lasts for at least 6 months [8]. The first step is an
intensive treatment over 2 months with four first-line
drugs: isoniazid (4-pyridinecarboxylic acid hydrazide, INH),
rifampicin, pyrazinamide, and ethambutol. The second step
is 4 months long and involves continuous isoniazid and
rifampicin administration (short-course chemotherapy) [9].
Received: May 11, 2017
Revised: June 20, 2017
Accepted: June 26, 2017
First published online
July 7, 2017
*Corresponding author
Phone: +82-31-400-5519;
Fax: +82-31-436-8153;
E-mail: [email protected]
pISSN 1017-7825, eISSN 1738-8872
Copyright© 2017 by
The Korean Society for Microbiology
and Biotechnology
Despite significant efforts to improve the treatment of tuberculosis (TB), it remains a prevalent
infectious disease worldwide owing to the limitations of current TB therapeutic regimens.
Recent work on novel TB treatment strategies has suggested that directly targeting host factors
may be beneficial for TB treatment. Such strategies, termed host-directed therapeutics (HDTs),
focus on host-pathogen interactions. HDTs may be more effective than the currently approved
TB drugs, which are limited by the long durations of treatment needed and the emergence of
drug-resistant strains. Targets of HDTs include host factors such as cytokines, immune
checkpoints, immune cell functions, and essential enzyme activities. This review article
discusses examples of potentially promising HDTs and introduces novel approaches for their
development.
Keywords: Tuberculosis, Mycobacterium tuberculosis, multidrug resistance, host-directed
therapeutics, immunomodulatory regulator
![Page 2: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/2.jpg)
1550 Kim and Yang
J. Microbiol. Biotechnol.
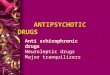
Table 1. Current drugs for treatment of tuberculosis (TB).
Classification Drug name Year of discovery Group Structure
First-line
anti-TB drugs
Isoniazid 1952 Group1 : Oral
Rifampicin 1963
Pyrazinamide 1954
Ethambutol 1961
Second-line
anti-TB drugs
Streptomycin 1944 Group 2 :
Injectable aminoglycosides
Kanamycin 1957
Amikacin 1972
Capreomycin 1963 Group 2 :
Injectable polypeptides
Viomycin 1951
Ciprofloxacin 1961 Group 3 :
Oral and injectable fluoroquinolones
![Page 3: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/3.jpg)
Novel Alternative TB Treatments 1551
September 2017⎪Vol. 27⎪No. 9
INH targets an enoyl-(acyl-carrier-protein) reductase and
inhibits mycolic acid synthesis; it is a prodrug that requires
activation by the catalase-peroxidase enzyme KatG [10].
Pyrazinamide inhibits translation by inhibiting the 30S
ribosomal S1 component [11]. First-line drugs such as INH
and pyrazinamide contribute to host defenses against MTB
by triggering the formation of cellular and mitochondrial
reactive oxygen species (ROS) and activating autophagy,
which reduces the MTB-induced proinflammatory response
in macrophages [12, 13]. Ethambutol targets arabinosyl
transferase, which blocks arabinogalactan biosynthesis
[14]. Although these first-line drugs initially show anti-TB
Table 1. Continued.
Classification Drug name Year of discovery Group Structure
Second-line
anti-TB drugs
Levofloxacin 1987 Group 3 :
Oral and injectable fluoroquinolones
Moxifloxacin 1988
Ofloxacin 1980
Gatifloxacin 1992
Para-aminosalicylic acid 1948 Group 4 : Oral
Cycloserine 1954
Terizidone 1965
Ethionamide 1961
Prothionamide 1956
Thioacetazone 1951
Linezolid 1996
Anti-TB drugs are categorized by evidence of efficacy, potency, and case of use.
![Page 4: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/4.jpg)
1552 Kim and Yang
J. Microbiol. Biotechnol.
effects, they have several limitations. These TB treatment
regimens are lengthy, involve drug intolerance and toxicity,
and require the consideration of pharmacokinetic drug-drug
interactions, particularly with anti-HIV drugs for patients
with HIV coinfection [4]. The development of an improved
TB therapeutic approach that is shorter, more effective
against resistant strains, and has fewer drug interactions is
needed [15]. Drug resistance to MTB is typically caused by
inappropriate treatment of active TB infections [16].
MDR-TB is characterized by resistance to isoniazid and
rifampicin. XDR-TB is defined as TB that is resistant to both
isoniazid and rifampicin, as well as to any fluoroquinolone
and at least one of the second-line injectable drugs
(capreomycin, kanamycin, and amikacin) [17]. A World Health
Organization TB treatment report has recommended treating
MDR/XDR-TB using a combination of four or more anti-
TB drugs that are effective against MTB [18].
Second-line anti-TB drugs are used to treat MTB infections
that are resistant to first-line drugs (Table 1: Groups 2, 3, and
4). Group 2 contains injectable anti-TB drugs. Streptomycin
is an aminoglycoside antibiotic, derived from the soil
microorganism Streptomyces griseus, which is used to treat
many bacterial infectious diseases, including TB [2]. This
drug was the first antibiotic used against TB. Streptomycin
interacts directly with the 12S and 16S rRNA components
of the 30S ribosomal subunit, thus inhibiting protein
synthesis [19]. Unfortunately, the use of this antibiotic led
to the rapid emergence of a resistant strain [20]. Because
many MDR-TB patients have resistance to streptomycin, it
is not commonly used for treating MDR-TB [21]. Second-line
anti-TB drugs such as kanamycin, amikacin, capreomycin,
and viomycin target protein synthesis. Kanamycin and
amikacin are aminoglycosides and target the 30S ribosomal
subunit [22]. Capreomycin and viomycin are cyclic peptide
antibiotics with similar structures that bind at the same site
on the ribosome. They target the interface between the 30S
and 50S ribosomal subunits. However, Group 2 drugs
also cause several adverse effects such as ototoxicity,
neurotoxicity, nephrotoxicity, and hypersensitivity. In
particular, aminoglycosides may act as neuromuscular
blocking agents, leading to respiratory failure [23]. Group 3,
composed of fluoroquinolones, inhibits topoisomerase II
(DNA gyrase), topoisomerase IV, and MTB topoisomerase II
[24]. The side effects of fluoroquinolones occur mainly in
the gastrointestinal tract, and 3–17% of patients treated with
fluoroquinolones experience these side effects [23]. Group 4,
oral bacteriostatic second-line anti-TB drugs, includes para-
amino salicylic acid (PAS), cycloserine, ethionamide, and
linezolid. PAS targets dihydropteroate synthase, causing it
to inhibit folate biosynthesis and iron uptake [25]. Common
adverse effects of PAS include nausea, pain, and diarrhea.
PAS can also cause liver inflammation and other allergic
reactions [26]. Cycloserine, a D-alanine analog, inhibits
peptidoglycan synthesis [27] and can have neurological
and psychiatric side effects. [23] Ethionamide is a potent
drug used to treat MDR-TB, and its structure is similar to
that of isoniazid. It is also a prodrug that requires activation
by a monooxygenase encoded by the ethA gene [28]. Similar
to isoniazid, ethionamide targets an enoyl-(acyl-carrier-
protein) reductase and inhibits mycolic acid biosynthesis
[29]. It can also lead to adverse effects in the gastrointestinal
tract, along with hepatotoxicity, neurotoxicity, cardiovascular
effects, and endocrine effects [23]. Linezolid (Zyon) is a
representative drug for eradicating resistant strains. Linezolid
was approved for use against drug-resistant, gram-positive
bacteria in the 2000s [30]. It is a member of the oxazolidinone
antibiotic class, and inhibits protein synthesis by interfering
with the functioning of the 23S rRNA. In addition, linezolid
has in vitro antibacterial activity against MTB, including
against MDR and XDR strains [31]. Moreover, linezolid
had an effect on XDR strains in a study on pulmonary-TB
patients [32] (Table 1). Linezolid therapy can last for less
than 28 days and has mild side effects. This drug affects the
nervous, gastrointestinal, hematologic, hepatic, and metabolic
systems [33]. Second-line anti-TB drugs, which are used to
treat infections resulting from a first-line drug-resistant
strain, have also led to the development of resistant MTB
strains. A spontaneous mutation in a MTB gene targeted by
a current TB drug can result in drug resistance.
The Need for Novel TB Drugs
New drugs for treating MDR-/XDR-TB would ideally
have a novel mechanism of action to circumvent the
current drug resistance. Lower toxicity drugs could reduce
side effects during TB treatment. The period of treatment,
which imposes a considerable economic burden and is
associated with the risk of the development of antibiotic-
resistant strains, also needs to be shortened. To shorten the
treatment period, novel drugs should have potent bactericidal
activity against most types of MTB. Novel drugs should be
effective and safe, and a low dosage frequency would also
be promising. Therefore, the development of dose formulations
and delivery technologies is another requirement for more
advanced TB treatment. Effective drug combination regimens
can also reduce the number of pills required [17].
![Page 5: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/5.jpg)
Novel Alternative TB Treatments 1553
September 2017⎪Vol. 27⎪No. 9
Host-Directed Therapies
HDTs for managing TB are composed of two main
strategies: enhancing the antimicrobial activity to clear
pathogens, and controlling excess inflammation to prevent
permanent lung tissue damage. Current HDTs can potentially
inhibit TB development via diverse host pathways, such as
signal transduction-mediating cytokines, antimicrobial
processes, immune cell regulation, and epigenetic modulation
[34]. The use of HDTs can be expected to reduce the bacterial
burden and fine-tune the host inflammatory response.
HDTs may also require minimal doses and short treatment
durations and may be used in combination with existing
drugs to enhance their overall effect.
Next, this review introduces several representative HDTs
for the treatment of TB (listed in Table 2) [34].
(1) Metformin (Glucophage), which acts as an autophagy
inducer, is currently approved for the treatment of type 2
diabetes. Many studies have shown that the activation of
autophagy leads to the clearance of MTB [35]. Metformin
activates adenosine monophosphate-activated protein kinases,
which are sensors of cellular energy levels [36]. Targeting
adenosine monophosphate-activated protein kinases is
predicted to be a potential anti-TB treatment [37]. Metformin
inhibits MTB growth by inducing mitochondrial ROS
production in vitro. The effect of current anti-TB drugs can
be enhanced by metformin, which was confirmed in both
acute and chronic TB mouse models. Furthermore,
metformin reduced the TB-mediated tissue pathology and
enhanced interferon (IFN)-γ-secreting CD8+ and CD4+
Table 2. Development of host-directed therapeutics for tuberculosis.
Category NameCurrently approved
indication(s)Host target
Developmental
stageRef.
Repurposed
drug
Imatinib Leukemia and gastrointestinal
stromal tumors
Tyrosine kinase Preclinical/clinical
(early phase)
[39]
Verapamil High blood pressure,
chest pain and supraventricular
tachycardia
Voltage-dependent
calcium channels
[34]
Metformin Diabetes AMP-activated protein
kinase activator
[38]
Ibuprofen Pain and fever relief Cyclooxygenase inhibitor [41]
Cytokine
therapy
IL-2 Renal cancer and melanoma Cytokine modulation Clinical
(late phase)
[53]
GM-CSF Acute myelogenous leukemia,
after bone marrow
transplantation
Cytokine modulation [64]
IFN-γ Chronic granulomatous disease Cytokine modulation [65]
Monoclonal
antibody
Adalimumab (Anti-TNFα) Rheumatoid arthritis Cytokine neutralization Preclinical/
clinical
(early phase)
[54]
Tocilizumab (Anti-IL6R) Juvenile arthritis,
Castleman’s disease
Cytokine neutralization [56]
Bevacizumav (Anti-VEGF) Various cancer types Angiogenesis inhibitor [57]
Monoclonal
antibody
Nivolumab
/pembrolizumab (Anti-PD-1)
Melanoma,
various other cancers
Immune checkpoint
inhibitor
Preclinical [45]
Anti-LAG3 Various cancers Immune checkpoint
inhibitor
[66]
Ipilimumab (Anti-CTLA-4) Melanoma,
various other cancers
Immune checkpoint
inhibitor
[67]
Vitamin Vitamin D3 Dietary supplement Innate immune response
activator
Clinical
(late phase)
[44]
Cellular
therapy
Bone marrow-derived
mesenchymal stromal cells
Various inflammatory
indications
Reduction of inflammation
and enhancement of tissue
regeneration
Clinical
(late phase)
[68]
Antigen-specific T cells Cancer and viral infections Targeted killing of
MTB-infected host cells
[68]
![Page 6: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/6.jpg)
1554 Kim and Yang
J. Microbiol. Biotechnol.
T-cell populations. It also reduced the activity of chronic
inflammatory genes in TB patients, in addition to reducing
mortality [38].
(2) Imatinib mesylate (Gleevec) is used to treat leukemia
and gastrointestinal stromal tumors. Imatinib is a small-
molecule kinase inhibitor that blocks tyrosine kinase
enzymes. The therapeutic administration of imatinib
promotes the acidification and maturation of MTB-infected
macrophage phagosomes, reducing the number of colony-
forming units (CFUs) in MTB-infected mice. Furthermore,
imatinib works synergistically with first-line anti-TB drugs to
inhibit drug-resistant mycobacterial strains. At subtherapeutic
concentrations, imatinib strengthens host defenses by
increasing neutrophil and monocyte numbers through
myeloproliferation [39, 40].
(3) Ibuprofen (Advil, Motrin, Nurofen) is a non-steroidal
anti-inflammatory drug normally used as a painkiller and
an antipyretic. This inhibitor of cyclooxygenase inhibits
prostaglandin E2 production and enhances tumor necrosis
factor (TNF) production in macrophages. Although the
direct antimycobacterial activity of ibuprofen is not potent,
it reduces lung tuberculous lesions and bacterial burden
and enhances the survival rate in a mouse model that
mimics active TB [41].
(4) Zileuton (ZYFLO) is a 5-lipooxygenase inhibitor that
inhibits the formation of leukotrienes (LTB4, LTC4, LTD4,
and LTE4) and has been approved to treat asthma. Mice
and humans infected with MTB show decreased IL-1
responses and increased production of type I IFN, resulting
in an eicosanoid imbalance that causes severe TB. Zileuton
reduces weight loss and the number of CFUs and protects
against acute mortality by increasing prostaglandin E2 levels
[42].
(5) Vitamin D3 is a dietary supplement that activates the
innate immune response. Low vitamin D3 levels are involved
in the development of active TB. Vitamin D3 has an
important role in converting 2,5(OH)D into 1,25-(OH)2D3,
which is its active form. This active form induces the
production of cathelicidin, which is an antimicrobial peptide.
After MTB infection, macrophages produce cathelicidin
through Toll-like receptor signaling; thus, vitamin D can
indirectly inhibit MTB [43]. Treatment with both vitamin D3
and 4-phenyl butyrate synergistically enhances cathelicidin
production [44].
(6) Another potent target of HDTs is immune checkpoints.
These immunomodulatory therapeutic strategies have been
studied extensively in cancer research. Programmed cell
death 1 (PD-1) is a protein on the surface of active T cells.
When programmed death-ligand 1 (PD-L1) and PD-L2
associate with PD-1 on the T-cell surface, T cells cannot
attack other cells. Nivolumab and pembrolizumab are PD-1
inhibitors currently used to treat melanomas and other
cancers. Antigen-specific IFN-γ was rescued using a PD-1
inhibitor in TB patients, confirming that nivolumab/
pembrolizumab has potential in treating TB [45]. Cytotoxic
T-lymphocyte-associated protein 4 affects immune checkpoints,
and it is expressed in active TB patients. Antigen-specific
lymphocyte expansion and cytokine expression can be
increased by blocking cytotoxic T-lymphocyte-associated
protein 4 [46].
(7) Cytokine therapy could be an alternative method to
limit the currently used TB chemotherapy. This method
uses immunomodulators to boost the immune system [47].
Cytokines contribute to various cellular responses, including
immune signaling in TB. Cytokine therapy induces a
proinflammatory immune response and antimicrobial
activity, which can be beneficial in treating TB. IFN-γ plays
a major role in the host defenses against MTB. IFN-γ, as a
prototypical product of Th1 cells, promotes the secretion of
Th1 cytokines (such as IL-12) and inhibits Th2 cytokines
(such as IL-4). In addition, IFN-γ upregulates class I and II
antigen-presenting cells and increases the antimicrobial
activity of macrophages. Mutations in the IFN-γ receptor gene
result in high susceptibility to mycobacterial infections
[48]. Granulocyte macrophage colony-stimulating factor
(GM-CSF) increases the number of macrophages, leading to
an enhanced inflammatory response. GM-CSF also shows
antimycobacterial activity in human macrophages [49].
Studies on GM-CSF-deficient mice showed that GM-CSF
plays critical immunomodulatory roles in the host defenses
against pulmonary TB [50]. Moreover, IL-2 induces the
expansion of T cells. However, recent studies have shown
that IL-2 promotes CD4+CD25+ regulatory T-cell expansion,
which suppresses the T-cell response [51]. Some clinical
trials testing the effectiveness of IL-2 against TB have been
reported [52, 53].
Excessive proinflammatory cytokine production causes
permanent host tissue damage. Therefore, regulating
cytokine production could be an alternative approach to
treat TB by reducing destructive inflammation. The current
monoclonal antibody used for cytokine neutralization
modulates inflammatory responses. The anti-TNF therapeutic
agent adalimumab has been previously used to treat TB
[54]. IL-6, which accelerates the severity of disease in TB
patients, is a promising candidate. Blockage of the IL-6/IL-6
receptor pathway is considered therapeutic in treating
various diseases [55]. The use of a monoclonal antibody,
along with the IL-6 receptor blockage, enhances anti-TB
![Page 7: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/7.jpg)
Novel Alternative TB Treatments 1555
September 2017⎪Vol. 27⎪No. 9
T-cell responses, decreases severe pathology, and reduces
the MTB burden in mice [56]. The anti-vascular endothelial
growth factor (anti-VEGF, bevacizumab) monoclonal antibody
inhibits TB by normalizing vasculature, increasing the
delivery of small molecules, and decreasing hypoxia in
tuberculous granulomas [57]. Therefore, the anti-VEGF
monoclonal antibody may increase the efficacy of current
treatment regimens.
Cell-based therapies are considered effective alternative
therapies in treating cancer and infectious diseases. In
addition, such therapies might decrease tissue-destructive
inflammation, enhance organ repair, and intensify antigen-
specific immune responses [58].
Several studies have focused on immunomodulatory
functions that show antimycobacterial activity [59-61].
Previously, we developed a novel treatment strategy for
treating an intracellular parasite infection, which might be
used as an HDT strategy against TB. We investigated
interactions between the intracellular parasite Toxoplasma
gondii and host macrophages and clarified the cellular
signaling involved in this interaction. T. gondii dense
granule antigen (GRA) 7 is essential for the innate immune
response and acts through an association with TNF receptor-
associated factor 6 (TRAF6) via myeloid differentiation
primary response gene 88. The interaction between GRA7
and TRAF6 confers a protective effect against T. gondii
infection in vivo [62]. We performed further experiments to
determine whether GRA7 modulation of the innate
immune response could work for other infectious diseases
such as TB. We found that GRA7 interacted with many host
proteins, including important host immune response
regulators. We showed that the protein kinase C alpha-
mediated phosphorylation of GRA7 is essential for the
interaction between apoptosis-associated speck-like protein
Fig. 1. Comparison between current anti-tuberculosis (TB) drugs and potential host-directed therapeutic (HDT) strategies for
treating TB.
Current anti-TB drugs have been developed by targeting pathogenic factors such as bacterial proliferation. A spontaneous mutation in one of the
genes that is targeted by these antibiotics can lead to the emergence of drug-resistant TB strains. To overcome the limitations of current anti-TB
drugs, the development of new drugs is necessary. HDTs directly affect host factors. Strategies for developing anti-TB HDTs have been verified in
several TB studies. IL-2, Interleukin-2; GM-CSF, Granulocyte macrophage colony-stimulating factor; IFN-γ, Interferon gamma; PD-1, Programmed
cell death protein 1, LAG3, Lymphocyte activation gene 3; CTLA-4, Cytotoxic T-lymphocyte-associated antigen 4; GRA7, Toxoplasma gondii dense
granule antigen 7.
![Page 8: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/8.jpg)
1556 Kim and Yang
J. Microbiol. Biotechnol.
containing a carboxyl-terminal CARD and phospholipase
D1. These interactions induced antibacterial activity against
TB. GRA7 controlled the innate immune response by
interacting with host cell proteins. Our current studies
have established proof of concept for developing novel
HDT strategies that could serve as alternatives to treat TB
[63] (Fig. 1).
In conclusion, by directly targeting host factors, HDTs
enhance immune responses and fine-tune inflammation,
and can thus be used to treat bacterial, viral, and parasitic
infectious diseases. Current treatment for MTB-mediated
TB has several limitations, including the long period of
treatment, emergence of resistant strains, and toxicity of
the drugs. These limitations increase the need for developing
novel TB treatment strategies. The present review focused
on potential novel HDTs that may be used to treat TB.
HDTs play a role in the clearance of MTB and regulation of
excess inflammatory responses to protect the host from
permanent organ damage. Furthermore, the combination
of HDTs with current TB drugs reduces drug dosages and
improves clinical outcomes. HDTs can be used to target
many pathways, and as such can be used to verify the
antimycobacterial activity of an approved drug (re-purposed
drugs), inhibit immune checkpoints, and modulate cytokine
production. We have shown that antigens derived from
the intracellular parasite T. gondii modulate the immune
response and might be promising for treating MBT infection.
However, the potential uses of HDTs need to be explored
further. Because HDTs directly interact with host factors,
various factors need to be considered prior to their
application. Furthermore, it is difficult to establish HDTs
that manipulate a human factor using animal models.
Because HDTs target complex pathways, there should be
detailed investigations into the potential side effects of HDTs.
Understanding the host immune response in TB-mediated
immune pathology is very important in HDT research.
Acknowledgments
This work was supported by a research fund of Hanyang
University (HY-2014-N).
Conflict of Interest
The authors have no financial conflicts of interest to declare.
References
1. Zaman K. 2010. Tuberculosis: a global health problem. J.
Health Popul. Nutr. 28: 111-113.
2. World Health Organization. 2016. Global Tuberculosis Report
2016. WHO, Geneva, Switzerland.
3. Schnippel K, Rosen S, Shearer K, Martinson N, Long L,
Sanne I, et al. 2013. Costs of inpatient treatment for multi-
drug-resistant tuberculosis in South Africa. Trop. Med. Int.
Health 18: 109-116.
4. Arbex MA, Varella Mde C, Siqueira HR, Mello FA. 2010.
Antituberculosis drugs: drug interactions, adverse effects,
and use in special situations. Part 1: first-line drugs. J. Bras.
Pneumol. 36: 626-640.
5. Zumla A, Rao M, Parida SK, Keshavjee S, Cassell G, Wallis R,
et al. 2015. Inflammation and tuberculosis: host-directed
therapies. J. Intern. Med. 277: 373-387.
6. Hawn TR, Matheson AI, Maley SN, Vandal O. 2013. Host-
directed therapeutics for tuberculosis: can we harness the
host? Microbiol. Mol. Biol. Rev. 77: 608-627.
7. Zumla A, Maeurer M, Host-Directed Therapies Network,
Chakaya J, Hoelscher M, Ntoumi F, et al. 2015. Towards
host-directed therapies for tuberculosis. Nat. Rev. Drug Discov.
14: 511-512.
8. World health Organization, Initiative ST. 2010. Treatment of
Tuberculosis: Guidelines. WHO, Geneva, Switzerland.
9. D’Ambrosio L, Centis R, Sotgiu G, Pontali E, Spanevello A,
Migliori GB. 2015. New anti-tuberculosis drugs and regimens:
2015 update. ERJ Open Res. 1: 00010-2015.
10. Timmins GS, Deretic V. 2006. Mechanisms of action of
isoniazid. Mol. Microbiol. 62: 1220-1227.
11. Shi W, Zhang X, Jiang X, Yuan H, Lee JS, Barry CE 3rd, et al.
2011. Pyrazinamide inhibits trans-translation in Mycobacterium
tuberculosis. Science 333: 1630-1632.
12. Kim JJ, Lee HM, Shin DM, Kim W, Yuk JM, Jin HS, et al.
2012. Host cell autophagy activated by antibiotics is
required for their effective antimycobacterial drug action.
Cell Host Microbe 11: 457-468.
13. Zullo AJ, Lee S. 2012. Old antibiotics target TB with a new
trick. Cell Host Microbe 11: 419-420.
14. Kolyva AS, Karakousis PC. 2012. Old and New TB Drugs:
Mechanisms of Action and Resistance. INTECH Open Access
Publisher, Croatia.
15. Zumla A, Nahid P, Cole ST. 2013. Advances in the
development of new tuberculosis drugs and treatment
regimens. Nat. Rev. Drug Discov. 12: 388-404.
16. Rattan A, Kalia A, Ahmad N. 1998. Multidrug-resistant
Mycobacterium tuberculosis: molecular perspectives. Emerg.
Infect. Dis. 4: 195.
17. Lange C, Abubakar I, Alffenaar JW, Bothamley G, Caminero JA,
Carvalho AC, et al. 2014. Management of patients with
multidrug-resistant/extensively drug-resistant tuberculosis in
Europe: a TBNET consensus statement. Eur. Respir. J. 44: 23-63.
18. World health Organization. 2011. Guidelines for the Programmatic
Management of Drug-resistant Tuberculosis - 2011 Update. WHO,
Geneva, Switzerland.
![Page 9: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/9.jpg)
Novel Alternative TB Treatments 1557
September 2017⎪Vol. 27⎪No. 9
19. Sharma D, Cukras AR, Rogers EJ, Southworth DR, Green R.
2007. Mutational analysis of S12 protein and implications
for the accuracy of decoding by the ribosome. J. Mol. Biol.
374: 1065-1076.
20. Crofton J, Mitchison D. 1948. Streptomycin resistance in
pulmonary tuberculosis. Br. Med. J. 2: 1009.
21. Rich M. 2003. The PIH Guide to the Medical Management of
Multidrug-resistant Tuberculosis. International Ed., Partners in
Health, Boston, MA.
22. Salian S, Matt T, Akbergenov R, Harish S, Meyer M, Duscha S,
et al. 2012. Structure-activity relationships among the kanamycin
aminoglycosides: role of ring I hydroxyl and amino groups.
Antimicrob. Agents Chemother. 56: 6104-6108.
23. Arbex MA, Varella Mde C, Siqueira HR, Mello FA. 2010.
Antituberculosis drugs: drug interactions, adverse effects,
and use in special situations. Part 2: second line drugs. J.
Bras. Pneumol. 36: 641-656.
24. Aubry A, Pan XS, Fisher LM, Jarlier V, Cambau E. 2004.
Mycobacterium tuberculosis DNA gyrase: interaction with
quinolones and correlation with antimycobacterial drug
activity. Antimicrob. Agents Chemother. 48: 1281-1288.
25. Wade MM, Zhang Y. 2004. Mechanisms of drug resistance
in Mycobacterium tuberculosis. Front. Biosci. 9: 975-994.
26. Das KM, Eastwood MA, McManus JP, Sircus W. 1973.
Adverse reactions during salicylazosulfapyridine therapy and
the relation with drug metabolism and acetylator phenotype.
N. Engl. J. Med. 289: 491-495.
27. Caceres NE, Harris NB, Wellehan JF, Feng Z, Kapur V,
Barletta RG. 1997. Overexpression of the D-alanine racemase
gene confers resistance to D-cycloserine in Mycobacterium
smegmatis. J. Bacteriol. 179: 5046-5055.
28. Baulard AR, Betts JC, Engohang-Ndong J, Quan S, McAdam RA,
Brennan PJ, et al. 2000. Activation of the pro-drug ethionamide
is regulated in mycobacteria. J. Biol. Chem. 275: 28326-28331.
29. Carette X, Blondiaux N, Willery E, Hoos S, Lecat-Guillet N,
Lens Z, et al. 2012. Structural activation of the transcriptional
repressor EthR from Mycobacterium tuberculosis by single
amino acid change mimicking natural and synthetic ligands.
Nucleic Acids Res. 40: 3018-3030.
30. Bouza E, Munoz P. 2001. Linezolid: pharmacokinetic
characteristics and clinical studies. Clin. Microbiol. Infect.
7 Suppl 4: 75-82.
31. Tato M, de la Pedrosa EG, Canton R, Gomez-Garcia I,
Fortun J, Martin-Davila P, et al. 2006. In vitro activity of
linezolid against Mycobacterium tuberculosis complex, including
multidrug-resistant Mycobacterium bovis isolates. Int. J.
Antimicrob. Agents 28: 75-78.
32. Lee M, Lee J, Carroll MW, Choi H, Min S, Song T, et al.
2012. Linezolid for treatment of chronic extensively drug-
resistant tuberculosis. N. Engl. J. Med. 367: 1508-1518.
33. Watkins RR, Lemonovich TL, File TM Jr. 2012. An evidence-
based review of linezolid for the treatment of methicillin-
resistant Staphylococcus aureus (MRSA): place in therapy.
Core Evid. 7: 131-143.
34. Zumla A, Rao M, Dodoo E, Maeurer M. 2016. Potential of
immunomodulatory agents as adjunct host-directed therapies
for multidrug-resistant tuberculosis. BMC Med. 14: 89.
35. Bento CF, Empadinhas N, Mendes V. 2015. Autophagy in
the fight against tuberculosis. DNA Cell Biol. 34: 228-242.
36. Hur KY, Lee MS. 2015. New mechanisms of metformin
action: focusing on mitochondria and the gut. J. Diabetes
Investig. 6: 600-609.
37. Yang CS, Kim JJ, Lee HM, Jin HS, Lee SH, Park JH, et al.
2014. The AMPK-PPARGC1A pathway is required for
antimicrobial host defense through activation of autophagy.
Autophagy 10: 785-802.
38. Singhal A, Jie L, Kumar P, Hong GS, Leow MK, Paleja B, et al.
2014. Metformin as adjunct antituberculosis therapy. Sci.
Transl. Med. 6: 263ra159.
39. Napier RJ, Rafi W, Cheruvu M, Powell KR, Zaunbrecher MA,
Bornmann W, et al. 2011. Imatinib-sensitive tyrosine kinases
regulate mycobacterial pathogenesis and represent therapeutic
targets against tuberculosis. Cell Host Microbe 10: 475-485.
40. Bruns H, Stegelmann F, Fabri M, Dohner K, van
Zandbergen G, Wagner M, et al. 2012. Abelson tyrosine
kinase controls phagosomal acidification required for killing
of Mycobacterium tuberculosis in human macrophages. J.
Immunol. 189: 4069-4078.
41. Vilaplana C, Marzo E, Tapia G, Diaz J, Garcia V, Cardona PJ.
2013. Ibuprofen therapy resulted in significantly decreased
tissue bacillary loads and increased survival in a new
murine experimental model of active tuberculosis. J. Infect.
Dis. 208: 199-202.
42. Mayer-Barber KD, Andrade BB, Oland SD, Amaral EP,
Barber DL, Gonzales J, et al. 2014. Host-directed therapy of
tuberculosis based on interleukin-1 and type I interferon
crosstalk. Nature 511: 99-103.
43. Chun RF, Adams JS, Hewison M. 2011. Immunomodulation
by vitamin D: implications for TB. Expert Rev. Clin. Pharmacol.
4: 583-591.
44. Mily A, Rekha RS, Kamal SM, Arifuzzaman AS, Rahim Z,
Khan L, et al. 2015. Significant effects of oral phenylbutyrate
and vitamin D3 adjunctive therapy in pulmonary tuberculosis:
a randomized controlled trial. PLoS One 10: e0138340.
45. Singh A, Mohan A, Dey AB, Mitra DK. 2013. Inhibiting the
programmed death 1 pathway rescues Mycobacterium
tuberculosis-specific interferon gamma-producing T cells
from apoptosis in patients with pulmonary tuberculosis. J.
Infect. Dis. 208: 603-615.
46. Grosso JF, Jure-Kunkel MN. 2013. CTLA-4 blockade in
tumor models: an overview of preclinical and translational
research. Cancer Immun. 13: 5.
47. Rivero-Lezcano OM. 2008. Cytokines as immunomodulators
in tuberculosis therapy. Recent Pat. Antiinfect. Drug Discov.
3: 168-176.
48. Ottenhoff TH, Verreck FA, Hoeve MA, van de Vosse E.
![Page 10: Host-Directed Therapeutics as a Novel Approach for ......MDR/XDR-TB using a combination of four or more anti-TB drugs that are effective against MTB [18]. Second-line anti-TB drugs](https://reader033.pdfslide.net/reader033/viewer/2022060918/60aad5f8757cd56c21011215/html5/thumbnails/10.jpg)
1558 Kim and Yang
J. Microbiol. Biotechnol.
2005. Control of human host immunity to mycobacteria.
Tuberculosis 85: 53-64.
49. Denis M, Ghadirian E. 1990. Granulocyte-macrophage colony-
stimulating factor restricts growth of tubercle bacilli in
human macrophages. Immunol. Lett. 24: 203-206.
50. Chroneos ZC, Jagannath C. 2012. Immunoregulatory Role of
GM-CSF in Pulmonary Tuberculosis. INTECH Open Access
Publisher, Croatia.
51. Nelson BH. 2004. IL-2, regulatory T cells, and tolerance. J.
Immunol. 172: 3983-3988.
52. Johnson BJ, Ress SR, Willcox P, Pati BP, Lorgat F, Stead P,
et al. 1995. Clinical and immune responses of tuberculosis
patients treated with low-dose IL-2 and multidrug therapy.
Cytokines Mol. Ther. 1: 185-196.
53. Johnson BJ, Bekker LG, Rickman R, Brown S, Lesser M, Ress S,
et al. 1997. rhuIL-2 adjunctive therapy in multidrug resistant
tuberculosis: a comparison of two treatment regimens and
placebo. Tuber. Lung Dis. 78: 195-203.
54. Wallis RS, van Vuuren C, Potgieter S. 2009. Adalimumab
treatment of life-threatening tuberculosis. Clin. Infect. Dis.
48: 1429-1432.
55. Rossi JF, Lu ZY, Jourdan M, Klein B. 2015. Interleukin-6 as a
therapeutic target. Clin. Cancer Res. 21: 1248-1257.
56. Okada M, Kita Y, Kanamaru N, Hashimoto S, Uchiyama Y,
Mihara M, et al. 2011. Anti-IL-6 receptor antibody causes
less promotion of tuberculosis infection than anti-TNF-alpha
antibody in mice. Clin. Dev. Immunol. 2011: 404929.
57. Datta M, Via LE, Kamoun WS, Liu C, Chen W, Seano G, et
al. 2015. Anti-vascular endothelial growth factor treatment
normalizes tuberculosis granuloma vasculature and improves
small molecule delivery. Proc. Natl. Acad. Sci. USA 112:
1827-1832.
58. Zumla A, Rao M, Wallis RS, Kaufmann SH, Rustomjee R,
Mwaba P, et al. 2016. Host-directed therapies for infectious
diseases: current status, recent progress, and future prospects.
Lancet Infect. Dis. 16: e47-e63.
59. Podder B, Jang WS, Nam KW, Lee BE, Song HY. 2015.
Ursolic acid activates intracellular killing effect of macrophages
during Mycobacterium tuberculosis infection. J. Microbiol.
Biotechnol. 25: 738-744.
60. Flores-Villalva S, Rogriguez-Hernandez E, Rubio-Venegas Y,
Canto-Alarcon JG, Milian-Suazo F. 2015. What can proteomics
tell us about tuberculosis? J. Microbiol. Biotechnol. 25: 1181-1194.
61. Tiwari B, Soory A, Raghunand TR. 2014. An immunomodulatory
role for the Mycobacterium tuberculosis region of difference 1
locus proteins PE35 (Rv3872) and PPE68 (Rv3873). FEBS J.
281: 1556-1570.
62. Yang CS, Yuk JM, Lee YH, Jo EK. 2015. Toxoplasma gondii
GRA7-induced TRAF6 activation contributes to host protective
immunity. Infect. Immun. 84: 339-350.
63. Koh HJ, Kim YR, Kim JS, Yun JS, Jang K, Yang CS. 2017.
Toxoplasma gondii GRA7-targeted ASC and PLD1 promote
antibacterial host defense via PKCalpha. PLoS Pathog. 13:
e1006126.
64. Pedral-Sampaio DB, Netto EM, Brites C, Bandeira AC,
Guerra C, Barberin MG, et al. 2003. Use of Rhu-GM-CSF in
pulmonary tuberculosis patients: results of a randomized
clinical trial. Braz. J. Infect. Dis. 7: 245-252.
65. Wallis RS. 2005. Reconsidering adjuvant immunotherapy for
tuberculosis. Clin. Infect. Dis. 41: 201-208.
66. Phillips BL, Mehra S, Ahsan MH, Selman M, Khader SA,
Kaushal D. 2015. LAG3 expression in active Mycobacterium
tuberculosis infections. Am. J. Pathol. 185: 820-833.
67. Postow MA, Callahan MK, Wolchok JD. 2015. Immune
checkpoint blockade in cancer therapy. J. Clin. Oncol. 33:
1974-1982.
68. Parida SK, Madansein R, Singh N, Padayatchi N, Master I,
Naidu K, et al. 2015. Cellular therapy in tuberculosis. Int. J.
Infect. Dis. 32: 32-38.




















![16007107 ade-of-anti tubercular-drugs-mdr-tb[1]](https://img.pdfslide.net/doc/110x75/545595b3af795989638b904d/16007107-ade-of-anti-tubercular-drugs-mdr-tb1.jpg)





