Embed Size (px)
Citation preview

6/23/2015
1
Hot Topics in Sports Medicine 2015
Carlin Senter M.D.UCSF Internal Medicine and Orthopaedics
UCSF Advances in Internal Medicine
Hot Topics in Sports Medicine 2015• Sports concussion
– Diagnosis– Treatment
• Knee pain due to osteoarthritis + meniscus tear– Exam– Treatment evidence
• Rotator cuff tears– Physical examination evidence
Concussions are common US military and traumatic brain injury
• 320,000 blast-related TBIs from wars in Iraq and Afghanistan (MacDonald CL et al. Detection of Blast-Related Traumatic Brain Injury in US Military Personnel, New England Journal of Medicine 2011.)
• mTBI accounts for 80-90% of TBI in civilian and military populations (Levin HS and Diaz-Arrastia RR. Lancet Neurol2015; 14: 506-17.)

6/23/2015
2
Concussion numbers increasing
Marin JR et al. Trends in visits for traumatic brain injury to emergency departments in the United States. JAMA. 2014 May 14;311(18):1917-9.
Concussion legislation• California: Education Code 49475 (effective
1/2012)1. Student athletes and guardians sign a concussion
information form yearly2. Athlete suspected of having concussion removed at
time of injury for the rest of the day3. Athlete can return only after cleared by healthcare
professional trained in evaluation and management of concussion
http://fuerzadesign.com/wp-content/uploads/2014/10/thumbnail-United-States.jpg
Case #1• 40 y/o woman presents to your office for ER follow-up
two days after bike accident.• Slid out while crossing streetcar tracks on wet city
streets. • No loss of consciousness.• Taken by ambulance to ER.• Had trauma work-up including head CT (-).• Has headache, fatigue, dizziness, light sensitivity.
Trouble staying focused at work, sleeping more than usual.
• Normal neck and neurologic exam.
Concussion definition• Type of mild traumatic brain injury• Blow to head, neck, body � force to head• Rapid onset of neurologic impairment• Symptoms usually resolve in weeks, spontaneously,
but in some cases can be prolonged.• May or may not include loss of consciousness.• CT and MRI studies are normal
Adapted from 4th International Conference on Concussion in Sport (2012). Br J Sport Med.
6/23/2015
3
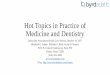
Physical
Cognitive
Emotional
Sleep
Concussion symptoms
http://www.cdc.gov/ncipc/tbi/Facts_for_Physicians_booklet.pdf. Accessed Nov. 9, 2008.
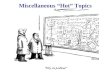
Clinic concussion evaluation• History of injury• PMHx ADHD, anxiety,
depression, head injury• Clinical status: improving or
worsening since time of injury?
• Neck and neurological exam
• Age > 60• GCS < 14 initially or < 15
two hours post injury• Vomiting more than once• Seizure• LOC• Focal neuro deficit• Suspected skull fx• Severe headache
• Decreased alertness after initially lucid
• High velocity injury (hit by car, fall from height)
• Comorbid illness (cirrhosis, diabetes, immunosuppression)
• Pregnancy• Anticoagulants
Adapted from Levin HS and Diaz-Arrastia RR. Lancet Neurol 2015; 14: 506-17, using NICE 2014 and 2008 American College of Emergency Physicians/US CDC policy statement.
How severe is my concussion?• Concussion grading is retrospective
– Historically concussions were graded on the sideline based on amnesia and LOC at time of injury.
– American Academy of Neurology, 1997– Cantu, 2001
– Studies have shown these factors not to be predictive of recovery.
• Only when the athlete recovers can you tell how severe the concussion was
http://thehoopla.wpengine.netdna-cdn.com/wp-content/uploads/2012/10/rage-meter-1.jpg

6/23/2015
4
Symptom resolution• Athletes become asymptomatic in 1-2 weeks
(Williams RM et al. Sports Med. 2015 Mar 28.)• Recovery in athletes may be faster than in others
(Levin HS and Diaz-Arrastia RR. Lancet Neurol 2015; 14: 506-17.)• Pre-existing neuropsychiatric disorder associated
with symptoms > 3 months (Levin HS and Diaz-Arrastia RR. Lancet Neurol 2015; 14: 506-17.)
Case #1• 40 y/o woman presents to your office for ER follow-up
two days after bike accident.• Slid out while crossing streetcar tracks on wet city
streets. • No loss of consciousness.• Taken by ambulance to ER.• Had trauma work-up including head CT (-).• Has headache, fatigue, dizziness, light sensitivity.
Trouble staying focused at work, sleeping more than usual.
• Normal neck and neurologic exam.
How would you treat this patient?A. Order urgent head CT to rule out subtle
post traumatic bleed, return to clinic after CT.
B. Rest from work and biking, return to clinic 1 week.
C. Return to work but rest from biking, return to clinic in a month.
D. Return to work and biking.O r d
e r ur g e
n t he a d
C T t o
. . .
R e st f r o
m wo r k
a n d b i k
i n . .
R e tu r n
t o w o r
k bu t r
e s t . . .
R e tu r n
t o w o r
k a nd b
i k i ng .
14%
0%
18%
69%
Concussion treatment• Cognitive rest• Physical rest• Medication
– Tylenol– Ibuprofen after first 72
hours• No driving• No alcohol• Education
6/23/2015
5
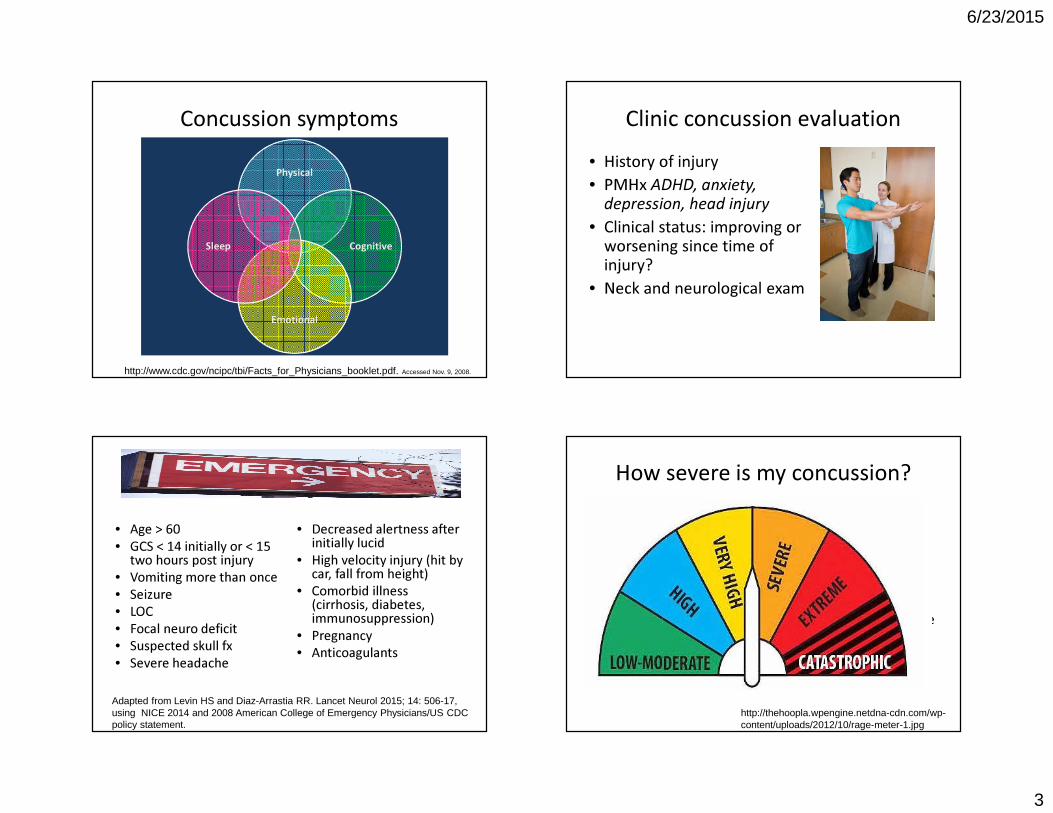
Return to school/work progression
No school. OK to do light reading, little bit TV, drawing, cooking as long as doesn’t worsen symptoms.
15 min cognitive activity at a time.
Return to full day of school.
http://www.chop.edu/service/concussion-care-for-kids/returning-to-school.html
30 min schoolwork at a time until can do 1-2 hours.
Return to ½ day of school.
Physical rest• Evidence sparse on benefit of rest• Management largely guided by expert opinion• No same-day return to play• Once concussion symptoms have resolved
gradually return to play
Return to play progression
Light aerobic activity
Sport specific activity
Game play
Non-contact training
Full contact practice
Clinician clearance
Asymptomatic
2nd International Conference on Concussion in Sport (2004). 2005 Br J Sport Med 39:196.
Concussion statement 2012

6/23/2015
6
Case #2• 55 y/o man with medial-sided pain and swelling
of the R knee for 6 weeks.• No locking, no instability• Exam: effusion, tender medial joint line and
above/below medial joint line, (+) medial knee irritation with medial McMurray, (+) medial pain with squat and Thessaly, no ligamentous laxity
• He brings with him x-rays and MRI for your review
EFFUSION
Area of tenderness
http://www.ski-injury.com/kneeanat.gif, Accessed 10/04/05. Accessed 10/4/05
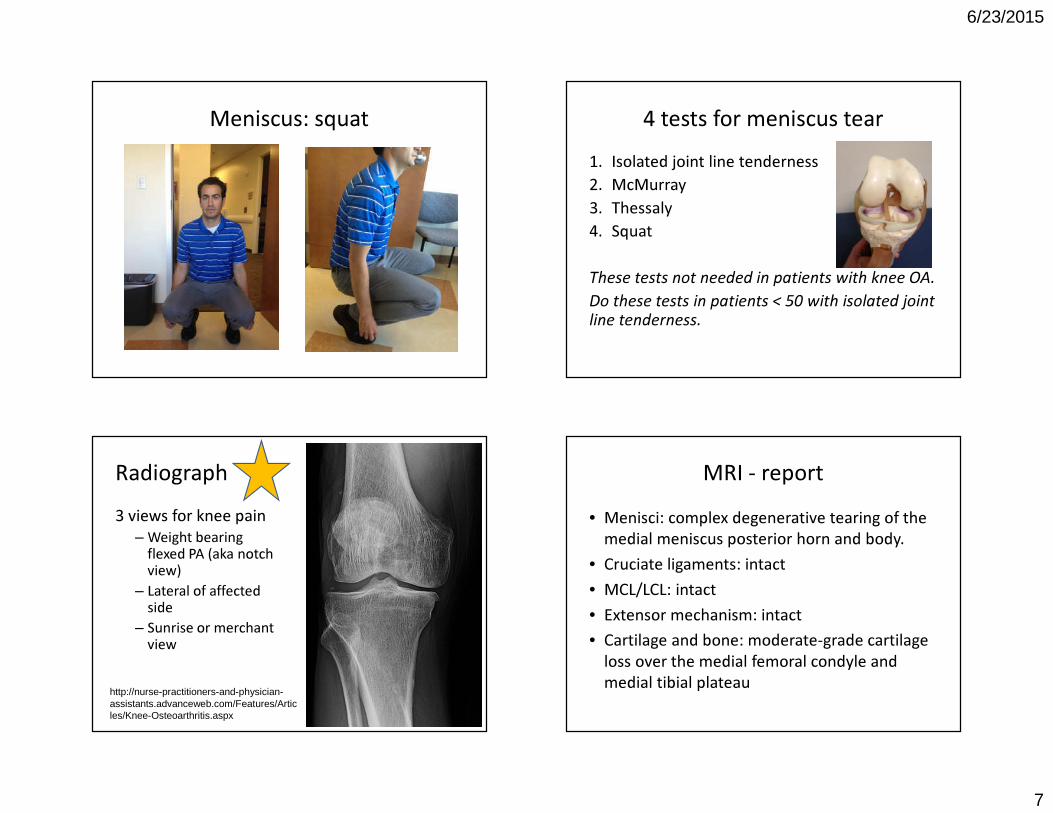
Meniscus: McMurray
Sensitivity medial 65%, Specificity medial 93%Magee, DJ. Orthopaedic Physical Assessment, 5th ed. 2008.
Meniscus: Thessaly
Video used with permission from Anthony Luke, MD.
6/23/2015
7
Meniscus: squat 4 tests for meniscus tear1. Isolated joint line tenderness2. McMurray3. Thessaly4. Squat
These tests not needed in patients with knee OA.Do these tests in patients < 50 with isolated joint line tenderness.
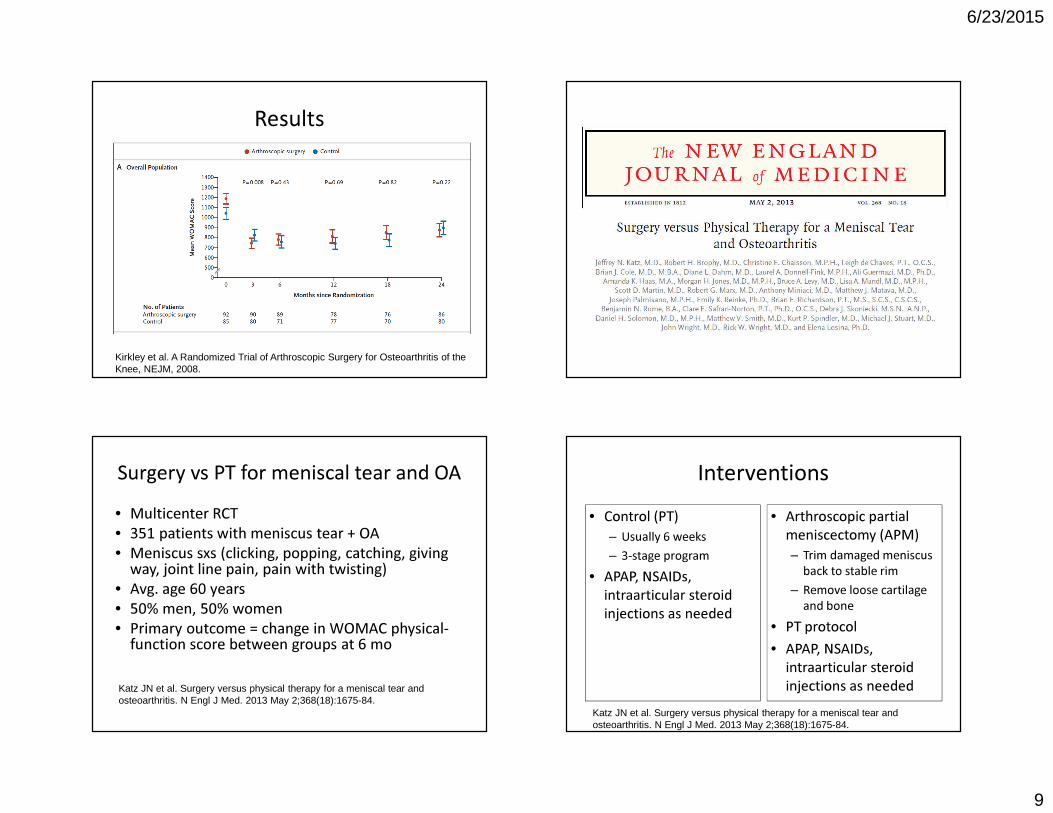
Radiograph3 views for knee pain
– Weight bearing flexed PA (aka notch view)
– Lateral of affected side
– Sunrise or merchant view
http://nurse-practitioners-and-physician-assistants.advanceweb.com/Features/Articles/Knee-Osteoarthritis.aspx
MRI - report • Menisci: complex degenerative tearing of the
medial meniscus posterior horn and body.• Cruciate ligaments: intact• MCL/LCL: intact• Extensor mechanism: intact• Cartilage and bone: moderate-grade cartilage
loss over the medial femoral condyle and medial tibial plateau

6/23/2015
8
Diagnosis?A. Medial meniscus tearB. ACL tearC. Moderate medial compartment
osteoarthritisD. Patellar dislocationE. Septic arthritisF. Medial meniscus tear and moderate
medial compartment osteoarthritisM ed i a
l me n i
s c us t e
a rA C L
t e ar
M od e r
a t e m e
d i al c o
m pa . . .
P a te l l a
r d is l o c
a t i on
S e pt i c
a r t hr i t i s
M ed i a
l me n i
s c us t e
a r a. .
0% 0%
88%
2%0%10%
Initial treatment?A. Refer for arthroscopic debridement of
meniscus tear and lavageB. Nonoperative knee OA programC. Refer for total knee arthroplasty
R e fe r f
o r ar t h r
o s co p i
c d e. . .
N o no p e
r a t iv e k
n e e O A
p . ..
R e fe r f
o r to t a
l k ne e a
r t h .. .
21%
2%
77%
• 188 patients followed x 2 years• Primary endpoint WOMAC score (knee pain + fxn)• Avg age 60, 2/3 female, BMI 31• Excluded bucket handle meniscus and severe
varus or valgus alignment
Interventions• Control
– PT: 1 hour/week x 12 weeks
– Home ex program 2x/day
– Instruction on ADLS– Self management
arthritis education reading + videotape
– Medications (APAP, NSAIDs, hyaluronic acid injections)
• Arthroscopic surgery– Irrigation with saline– 1 or more of the
following:• Debridement or excision
of degenerative meniscus tears
• Removal loose bodies, chondral flaps, bone spurs
– Medical and physical therapy like controls
Kirkley et al. A Randomized Trial of Arthroscopic Surgery for Osteoarthritis of the Knee, NEJM, 2008.
6/23/2015
9
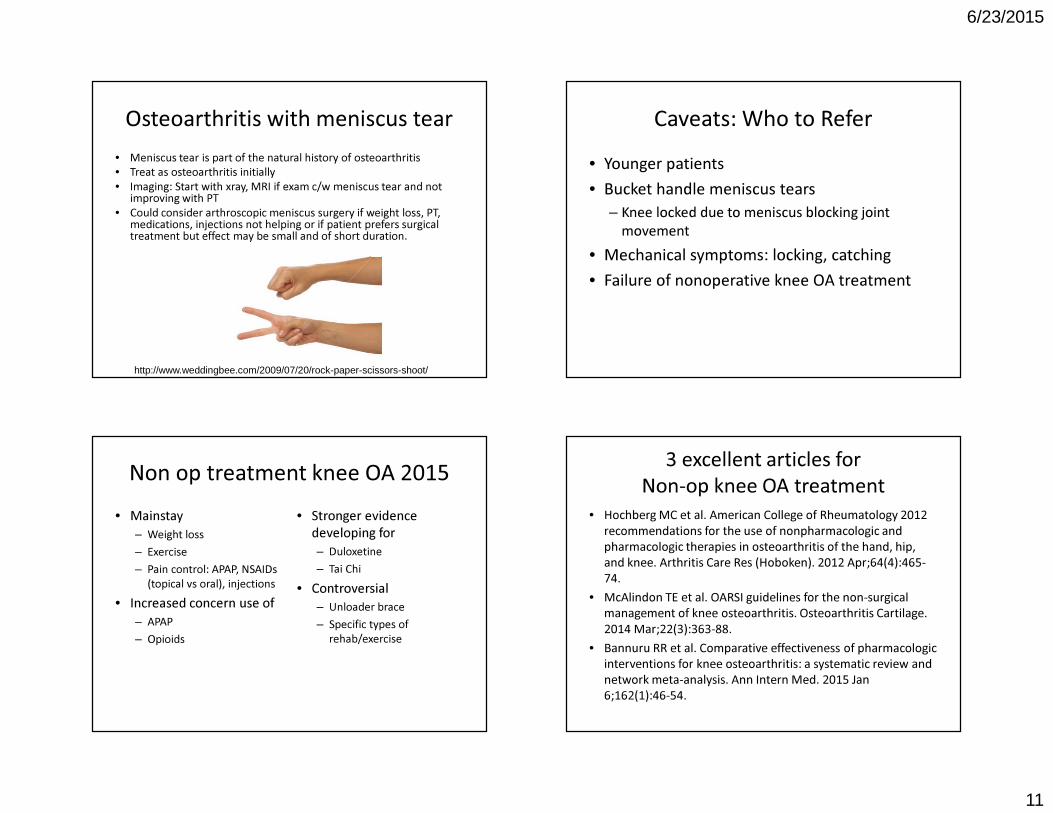
Results
Kirkley et al. A Randomized Trial of Arthroscopic Surgery for Osteoarthritis of the Knee, NEJM, 2008.
Katz JN et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013 May 2;368(18):1675-84.
Surgery vs PT for meniscal tear and OA• Multicenter RCT• 351 patients with meniscus tear + OA• Meniscus sxs (clicking, popping, catching, giving
way, joint line pain, pain with twisting)• Avg. age 60 years• 50% men, 50% women• Primary outcome = change in WOMAC physical-
function score between groups at 6 mo
Interventions• Control (PT)
– Usually 6 weeks– 3-stage program
• APAP, NSAIDs, intraarticular steroid injections as needed
• Arthroscopic partial meniscectomy (APM)– Trim damaged meniscus
back to stable rim– Remove loose cartilage
and bone• PT protocol• APAP, NSAIDs,
intraarticular steroid injections as needed
Katz JN et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013 May 2;368(18):1675-84.

6/23/2015
10
Results
Katz JN et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013 May 2;368(18):1675-84.
Results
Katz JN et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013 May 2;368(18):1675-84.
Conclusions• 30% crossed over from PT to APM at 6mo
– These people had WOMACs that didn’t improve until crossover
• No sig difference in adverse events• PT and APM are reasonable options with similar
outcomes for these patients (with allowed cross over if not achieving relief with PT)
• Starting with conservative approach is reasonableKatz JN et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013 May 2;368(18):1675-84.
Thorlund et al. Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms. BMJ. 2015 Jun 16;350:h2747.
• Benefits and harms of knee arthroscopy for degenerative knees• Meta-analysis of RCTs to determine benefit and including cohort
studies to determine harms• Arthroscopy effect size 2.4 mm on a 0-100 mm visual analog scale.
No effect after 6 months.• Harms: DVT, PE, infection, death• Conclusion: “These findings do not support the practise of
arthroscopic surgery for middle aged or older patients with knee pain with or without signs of osteoarthritis.”
6/23/2015
11
Osteoarthritis with meniscus tear• Meniscus tear is part of the natural history of osteoarthritis• Treat as osteoarthritis initially• Imaging: Start with xray, MRI if exam c/w meniscus tear and not
improving with PT• Could consider arthroscopic meniscus surgery if weight loss, PT,
medications, injections not helping or if patient prefers surgical treatment but effect may be small and of short duration.
http://www.weddingbee.com/2009/07/20/rock-paper-scissors-shoot/
Caveats: Who to Refer• Younger patients• Bucket handle meniscus tears
– Knee locked due to meniscus blocking joint movement
• Mechanical symptoms: locking, catching• Failure of nonoperative knee OA treatment
Non op treatment knee OA 2015• Mainstay
– Weight loss– Exercise– Pain control: APAP, NSAIDs
(topical vs oral), injections• Increased concern use of
– APAP– Opioids
• Stronger evidence developing for– Duloxetine– Tai Chi
• Controversial – Unloader brace– Specific types of
rehab/exercise
3 excellent articles forNon-op knee OA treatment
• Hochberg MC et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012 Apr;64(4):465-74.
• McAlindon TE et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2014 Mar;22(3):363-88.
• Bannuru RR et al. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: a systematic review and network meta-analysis. Ann Intern Med. 2015 Jan 6;162(1):46-54.

6/23/2015
12
Case #357 y/o RHD man presents with R shoulder pain that started after he slipped and fell 3 months ago. Pain at R deltoid. He tried physical therapy without benefit. Waking at night from sleep due to pain.
Differential diagnosis?
Rotator cuff disease in primary care• The 3rd most frequent musculoskeletal reason
patients present to the office• The most common cause of shoulder pain in
patients in the US primary care settings
Whittle S, Buchbinder R. In the clinic. Rotator cuff disease. Ann Intern Med. 2015 Jan 6;162(1):ITC1-15.
What is rotator cuff disease?• Impingement• Tendinitis/tendinopathy• Partial thickness tear• Full thickness tear
6/23/2015
13
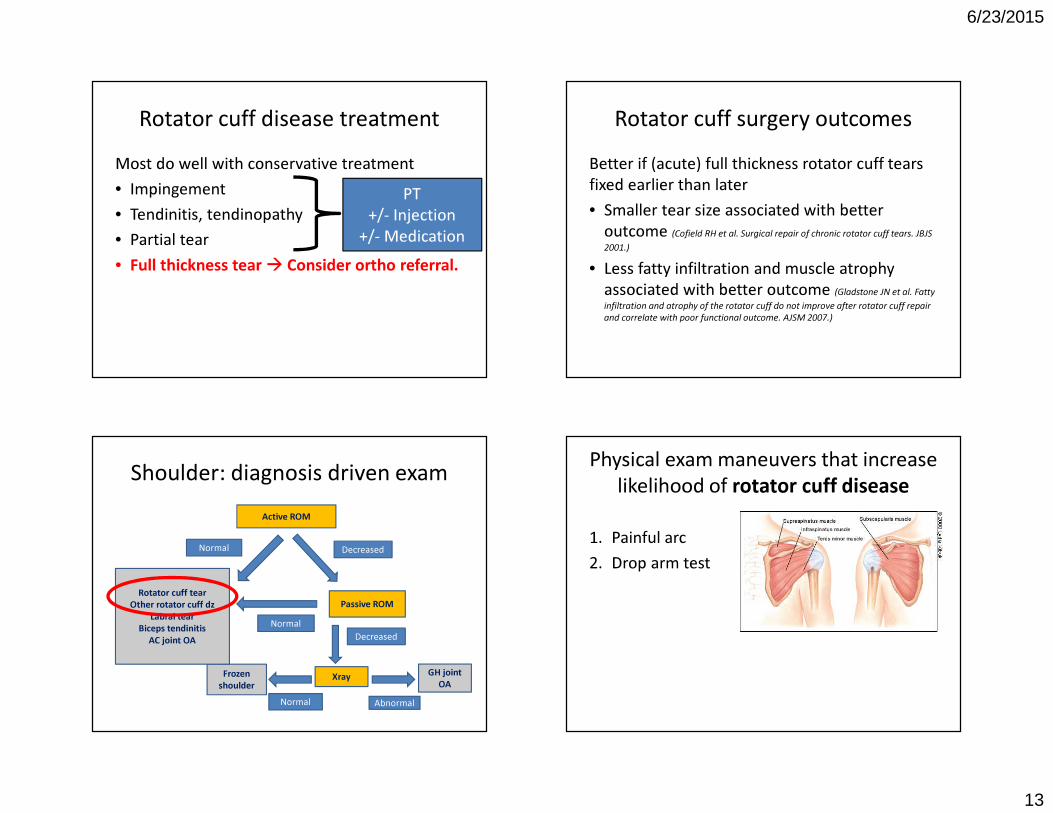
Rotator cuff disease treatmentMost do well with conservative treatment• Impingement• Tendinitis, tendinopathy• Partial tear • Full thickness tear � Consider ortho referral.
PT+/- Injection
+/- Medication
Rotator cuff surgery outcomesBetter if (acute) full thickness rotator cuff tears fixed earlier than later • Smaller tear size associated with better
outcome (Cofield RH et al. Surgical repair of chronic rotator cuff tears. JBJS 2001.)
• Less fatty infiltration and muscle atrophy associated with better outcome (Gladstone JN et al. Fatty infiltration and atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with poor functional outcome. AJSM 2007.)
Shoulder: diagnosis driven examActive ROM
DecreasedNormal
Passive ROMNormal
Decreased
XrayFrozen shoulder
Normal
GH joint OA
Abnormal
Rotator cuff tearOther rotator cuff dz
Labral tearBiceps tendinitis
AC joint OA
Physical exam maneuvers that increase likelihood of rotator cuff disease
1. Painful arc2. Drop arm test
6/23/2015
14
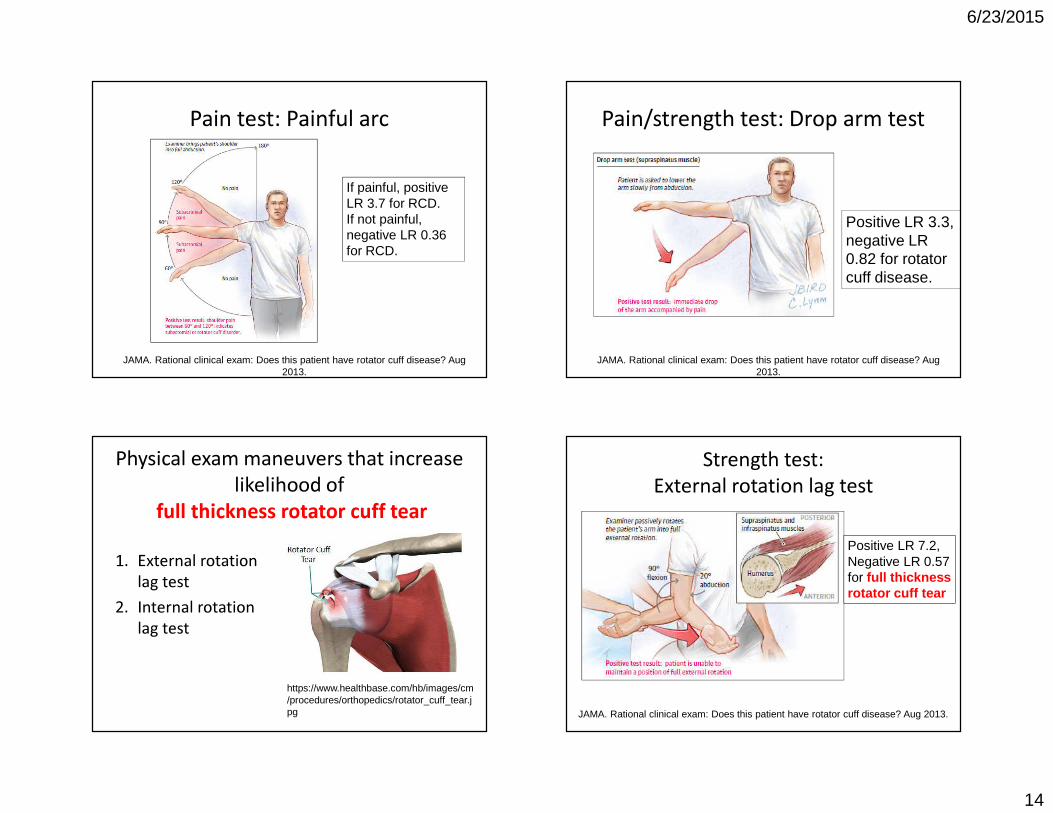
Pain test: Painful arc
JAMA. Rational clinical exam: Does this patient have rotator cuff disease? Aug 2013.
If painful, positive LR 3.7 for RCD.If not painful, negative LR 0.36 for RCD.
Pain/strength test: Drop arm test
JAMA. Rational clinical exam: Does this patient have rotator cuff disease? Aug 2013.
Positive LR 3.3, negative LR 0.82 for rotator cuff disease.
Physical exam maneuvers that increase likelihood of
full thickness rotator cuff tear
1. External rotation lag test
2. Internal rotation lag test
https://www.healthbase.com/hb/images/cm/procedures/orthopedics/rotator_cuff_tear.jpg
Strength test:External rotation lag test
Positive LR 7.2,Negative LR 0.57 for full thickness rotator cuff tear
JAMA. Rational clinical exam: Does this patient have rotator cuff disease? Aug 2013.
6/23/2015
15
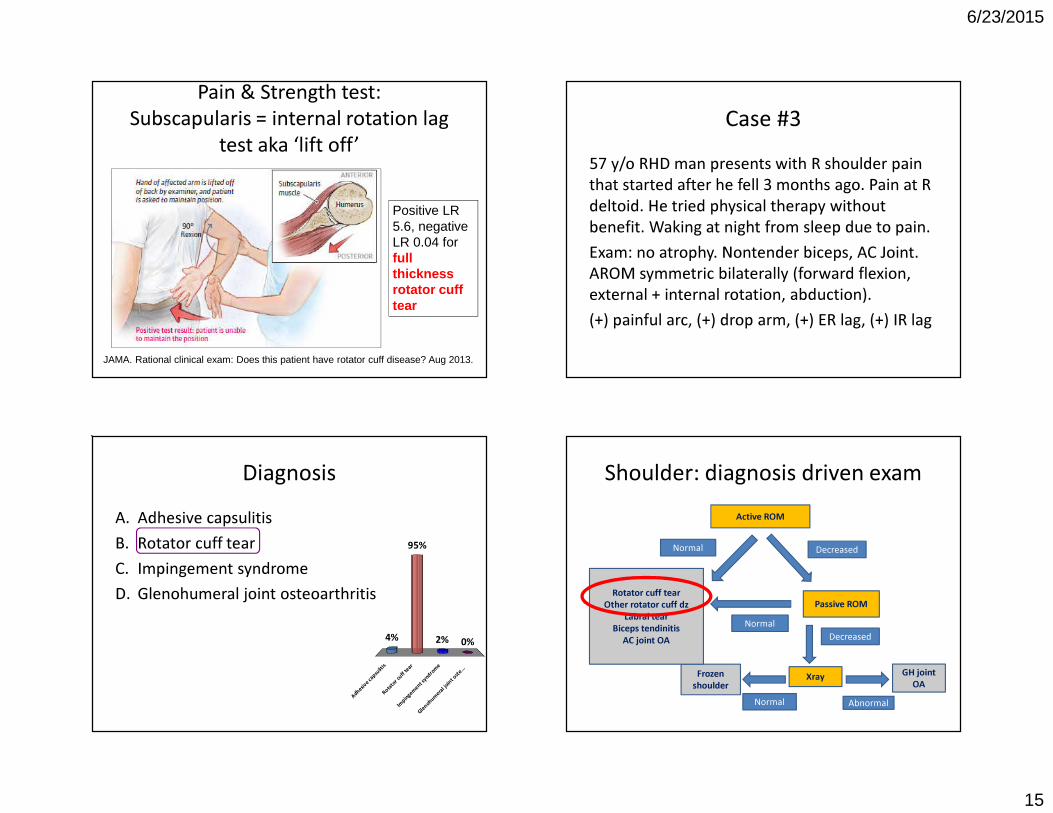
Pain & Strength test:Subscapularis = internal rotation lag
test aka ‘lift off’
JAMA. Rational clinical exam: Does this patient have rotator cuff disease? Aug 2013.
Positive LR 5.6, negative LR 0.04 for full thickness rotator cuff tear
Case #357 y/o RHD man presents with R shoulder pain that started after he fell 3 months ago. Pain at R deltoid. He tried physical therapy without benefit. Waking at night from sleep due to pain.Exam: no atrophy. Nontender biceps, AC Joint. AROM symmetric bilaterally (forward flexion, external + internal rotation, abduction).(+) painful arc, (+) drop arm, (+) ER lag, (+) IR lag
DiagnosisA. Adhesive capsulitisB. Rotator cuff tearC. Impingement syndromeD. Glenohumeral joint osteoarthritis
A d he s i v
e c ap s u
l i t i sR o t
a t or c u
f f t ea r
I m pi n g
e me n t
s y nd r o
m e
G l en o h
u me r a
l j oi n t
o s te . . .
4% 0%2%
95%
Shoulder: diagnosis driven examActive ROM
DecreasedNormal
Passive ROMNormal
Decreased
XrayFrozen shoulder
Normal
GH joint OA
Abnormal
Rotator cuff tearOther rotator cuff dz
Labral tearBiceps tendinitis
AC joint OA

6/23/2015
16
TreatmentA. Refer for surgical consultB. Repeat trial of physical therapy,
f/u 3 months.C. Give NSAIDs and activity
modification, f/u 3 monthsD. Give subacromial injection, f/u 3
months
R e fe r f
o r su r g
i c a l c o n
s u l t
R e pe a t
t r i al o f
p hy s i c
a l t. . .
G i ve N
S A ID s
a n d a c t
i v i t. . .
G i ve s u
b a cr o m
i a l in j e
c t i on . . .
81%
5%7%7%
3 excellent shoulder articles1. O'Kane JW, Toresdahl BG. The evidenced-based
shoulder evaluation. Curr Sports Med Rep. 2014 Sep-Oct;13(5):307-13.
2. Hermans J et al. Does this patient with shoulder pain have rotator cuff disease?: The Rational Clinical Examination systematic review. JAMA. 2013 Aug 28;310(8):837-47.
3. Whittle S, Buchbinder R. In the clinic. Rotator cuff disease. Ann Intern Med. 2015 Jan 6;162(1):ITC1-15.
Thank you!
Carlin Senter, M.D.Primary Care Sports Medicine
UCSF Internal Medicine and Orthopaedics