Embed Size (px)
Citation preview
How Clinical Faculty Can Develop Scholarship Out of
Clinical Work
Susan K. Pingleton, MD
Scholarship Out of Clinical Work
Why? What is Scholarship??
Resources – Mentor
Squire Guidelines
QI vs. Clinical ResearchHow to develop a project
Where to get the data
WHY ??
• You are faculty in an academic medical center
• Scholarship is needed for promotion
• It is the right thing to do for your students and trainees
Resources
• Mentor
– Now School of Medicine Requirement for all Departments – clinical and basic science
• Pediatrics• Dept of Medicine Mentoring Toward Promotion
– Understanding Ranks and Tracks– Understanding Criteria for Promotion
Scholarship
• Discovery• Traditional research
– Basic and Clinical
• Quality Improvement• Educational curriculums• Health Policy
• Dissemination• Presentations• Publications• Other Academic Medical Centers, Hospitals
Survey IM Chairs
• 65 responses (55%)• 80% have one or more faculty members
spending 20% effort on QI• 78% think faculty should be promoted
based on QI• 26% think evidence of scholarship or
academic progress should be required; few consider it “service”
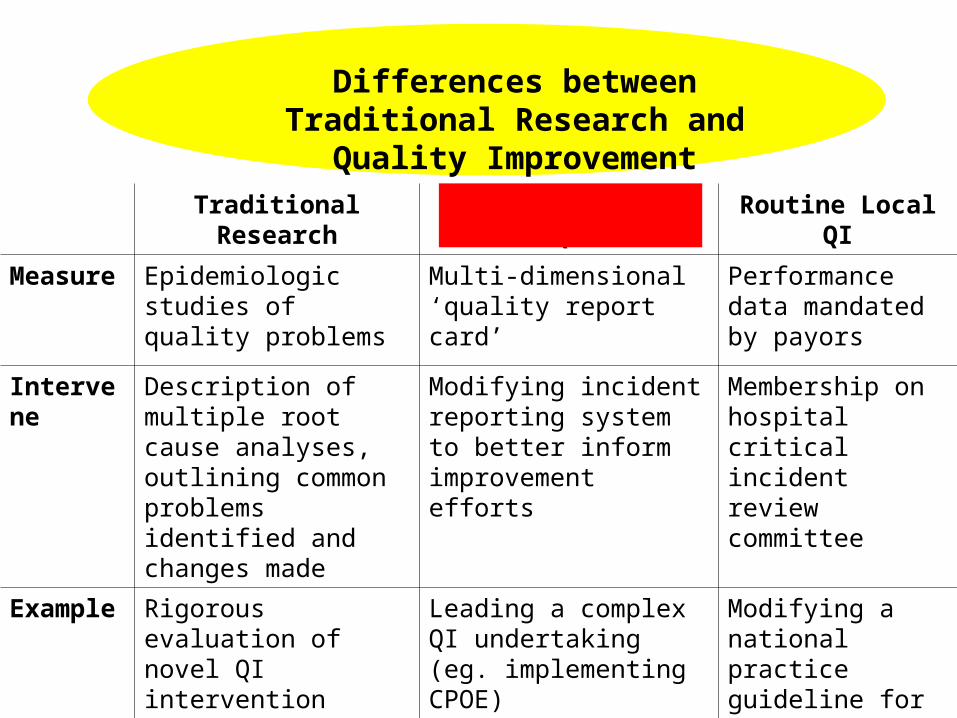
Traditional Research Innovative Local QI Routine Local QI
Measure Epidemiologic studies of quality problems
Multi-dimensional ‘quality report card’
Performance data mandated by payors
Intervene Description of multiple root cause analyses, outlining common problems identified and changes made
Modifying incident reporting system to better inform improvement efforts
Membership on hospital critical incident review committee
Example Rigorous evaluation of novel QI intervention
Leading a complex QI undertaking (eg. implementing CPOE)
Modifying a national practice guideline for local uptake
Differences between Traditional Research and Quality
Improvement
Routine Quality-Related Activities
• General internist who led the local adoption of national guidelines for peri-operative care
• Chairs hospital P&T committee• Also sits on critical incident review
committee
Counts as ‘Hospital Service’, expected of all faculty, but little to intrinsic academic merit
Clinician Engaged in Innovative QI
• Hospitalist who during his non-clinical time led development of an innovative program to improve the discharge process
• Successfully led hospital-wide implementation of medication reconciliation
• Based on above successes, hospital now supports part of his salary to lead new QI projects
Discovery and dissemination characteristics worthy of academic promotion
How to Develop a Project ?
• Assignment of a project by a mentor
• Interesting clinical/educational/health policy question that you have and cannot find an answer
• “Does routine phone call after discharge improved discharge planning”?
• “Does a serum lactate predict mortality in acute bowel obstruction?”
• “What interventions in the EMR can improve core measure compliance?”
• “What are the benefits of a Hospitalist Administrator on Duty?”
• Requires literature search
DATA
Role of data in quality improvement
Characteristics of “good” data
Sources/categories of data
Administrative databases – pros &cons
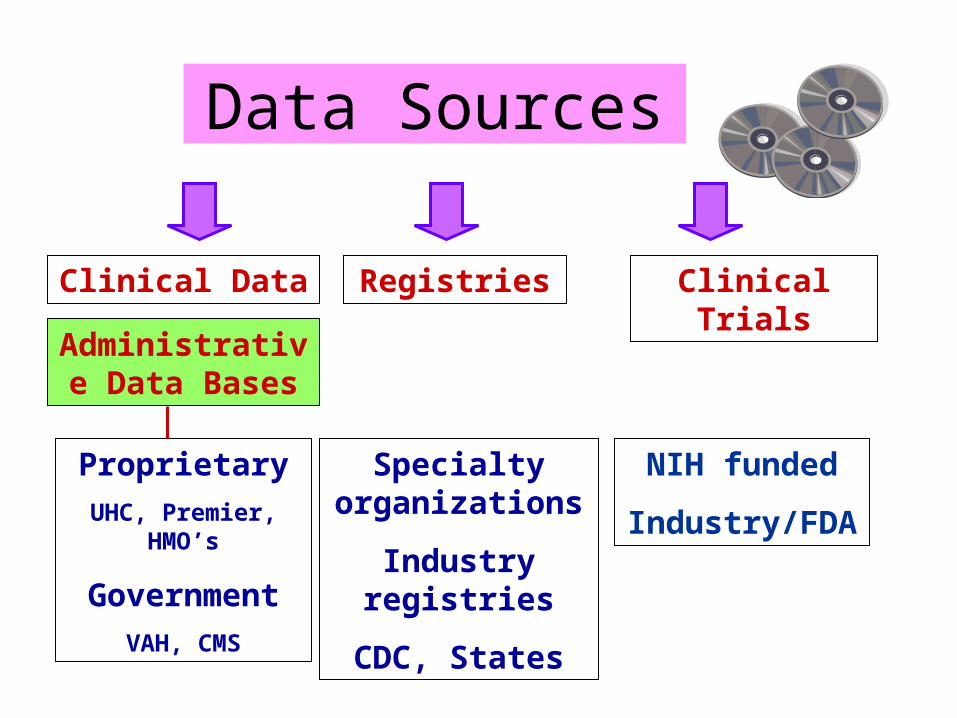
Data Sources
Clinical Data
Administrative Data Bases
Registries Clinical Trials
Proprietary
UHC, Premier, HMO’s
Government
VAH, CMS
Specialty organizations
Industry registries
CDC, States
NIH funded
Industry/FDA
Multiple types of Clinical registries:
All afford data for clinical research
• Specialty registries, e.g.• CTS• Anesthesia Quality Institute (AQI) Data Registry • American College of Chest Physicians Bronchoscopy
Registry
• Disease registries, e.g.• Cancer • Pulmonary Hypertension
• Government/Organization registries, e.g.• CDC• Veterans Administration CDB• State of Kansas Diabetes Registry
• Clinical data (National Surgical Quality Improvement Program)
– Prospective data collection, chart abstraction– Expensive, labor-intensive, but face validity among
physicians
• Administrative data base (UHC’s CDB, Premier, Thomson-Reuters)
– Always retrospective, Claims data (medical record coding)– Very efficient way to collect data
• Hybrid (CDB/Resource Manager)– Administrative clinical data supplemented with resource
utilization
Differences between Abstracted Clinical Data and Administrative Data Bases for Clinical
Performance
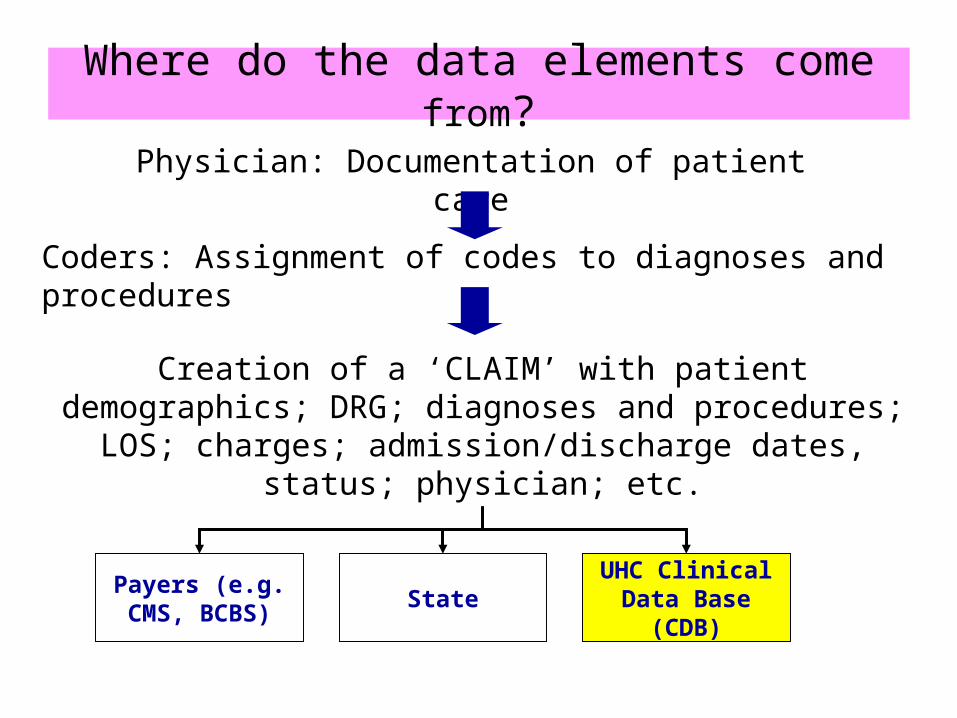
Where do the data elements come from?
Physician: Documentation of patient care
Coders: Assignment of codes to diagnoses and procedures
Creation of a ‘CLAIM’ with patient demographics; DRG; diagnoses and procedures; LOS; charges;
admission/discharge dates, status; physician; etc.
Payers (e.g. CMS, BCBS)
StateUHC Clinical
Data Base (CDB)
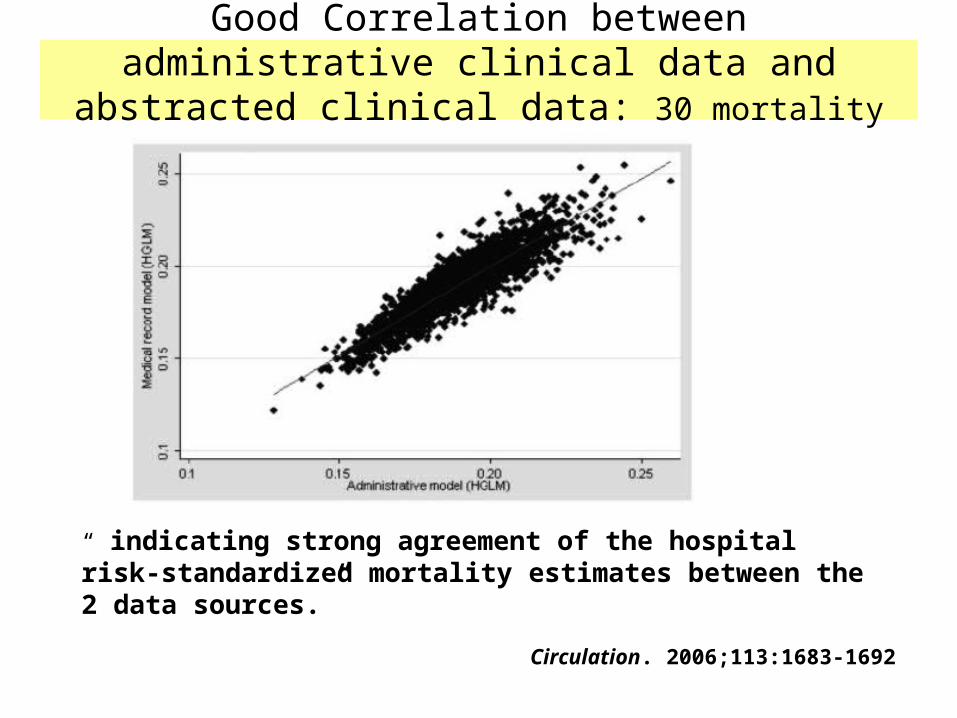
Good Correlation between administrative clinical data and abstracted clinical data: 30 mortality AMI
“ indicating strong agreement of the hospital risk-standardized mortality estimates between the 2 data sources.”
Circulation. 2006;113:1683-1692
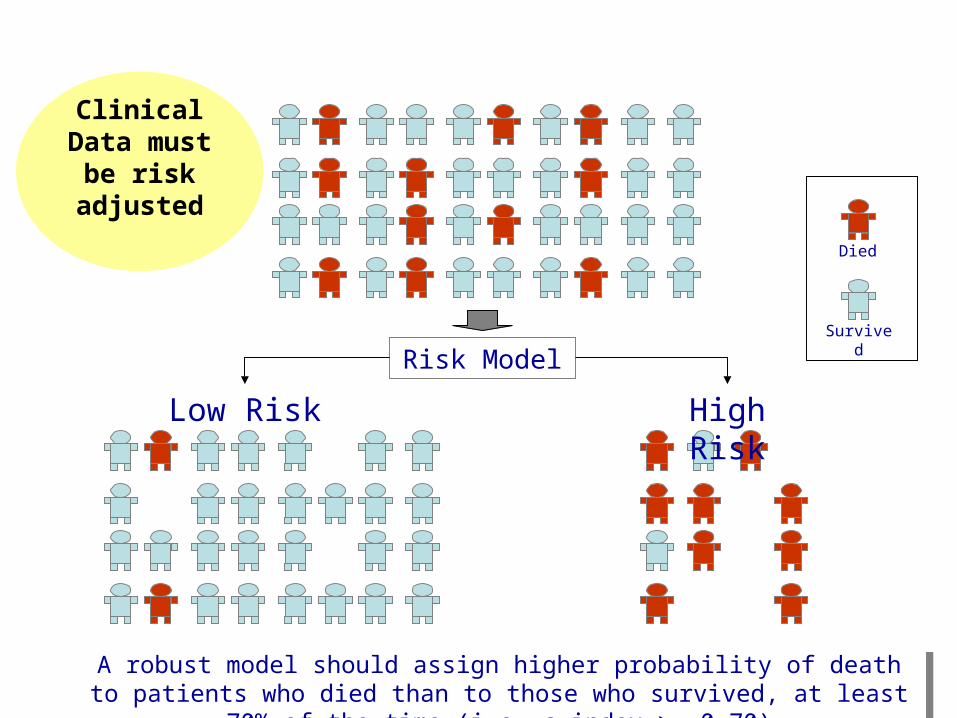
Risk Model
High RiskLow Risk
A robust model should assign higher probability of death to patients who died than to those who survived, at least 70% of the time (i.e. c-index >= 0.70)
A robust model should assign higher probability of death to patients who died than to those who survived, at least 70% of the time (i.e. c-index >= 0.70)
Survived
Died
Clinical Data must
be risk adjusted
SQUIRE:Standards for Quality
Improvement Reporting Excellence
http://www.squire-statement.org/
Scholarship Out of Clinical Work
Scholarship is discovery and dissemination
All departments will have mentoring program and web site
Squire Guidelines
QI vs. Clinical ResearchHow to develop a project? What are you interested in?
Where to get the data – Registries, Clinical Data Base, O2













![CLINICAL SCHOLARSHIP AND SCHOLARSHIP BY … Kruse...\\jciprod01\productn\N\NYC\26-1\NYC115.txt unknown Seq: 3 22-AUG-19 7:07 Fall 2019] Scholarship by Clinicians 309 scholarship about](https://img.pdfslide.net/doc/110x75/5f4485b49abc8a004a360957/clinical-scholarship-and-scholarship-by-kruse-jciprod01productnnnyc26-1.jpg)














