Embed Size (px)
Citation preview
How Do Clinicians Practicing in the U.S. ManageHelicobacter pylori-Related Gastrointestinal Diseases?
A Comparison of Primary Care and Specialist Physicians
Thomas Breuer, M.D., M.S., Karen J. Goodman, Ph.D., Hoda M. Malaty, M.D., Ph.D.,Thomas Sudhop, M.D., and David Y. Graham, M.D.
Department of Medicine, V.A. Medical Center and Baylor College of Medicine, Houston; School of Public Health, University of Texas,Houston, Texas; and Department of Clinical Pharmacology, University of Bonn, Germany
Objectives:We sought to examine the extent to whichphysicians recognizeH. pylori as a causal agent in pepticulcer disease or as a potential cofactor in other gastro-intestinal diseases, and to observe how this knowledgehas influenced diagnostic and therapeutic practices.Methods: We used a national mail survey in the U.S.between February and May of 1996, querying 5994 U.S.physicians (family/general practitioners [FPs], internists[IMs], and gastroenterologists) selected at random fromthree different membership databases of professionalassociations.Results:The response rate was 52%. Morethan 95% of physicians who treat symptoms empiricallywould prescribe acid suppressant therapy rather thananti-H. pylori therapy. Between 43% and 66% of physi-cians, varying in frequency by medical specialty, wouldtreat the infection in H. pylori-positive patients withnonulcer dyspepsia. In confirmed peptic ulcer disease,between 88% and 100% of physicians would treat theH.pylori infection, depending on the physician group andwhether or not the presentation of an ulcer was recur-rent. Although 103 distinct anti-H. pylori regimens werereported, 89% of the gastroenterologists and 70% of theprimary care physicians (PCPs) used combinations ofantimicrobials with reported cure rates of at least 80%.Conclusions: General knowledge regarding H. pylori-associated diseases was widespread among primary carephysicians and gastroenterologists. However, anti-H. py-lori therapies judged ineffective were reported as thefirst choice regimen by 5% of gastroenterologists and18% of primary care physicians. Gastroenterologistsappear to implement the latest scientific developments inthe field rapidly whereas PCPs manifest a delayed re-sponse, due to either insufficient knowledge or to otherfactors influencing their approach to treatment. (Am JGastroenterol 1998;93:553–561. © 1998 by Am. Coll. ofGastroenterology)
INTRODUCTION
It is now accepted that infection of the gastric mucosawith Helicobacter pyloricauses chronic gastritis. More than90% of peptic ulcer patients are infected withH. pylori andit has been shown that successful treatment prevents ulcerrelapse (1, 2). These findings have greatly changed diag-nostic and therapeutic options concerning peptic ulcer dis-ease. Further evidence has implicatedH. pylori as an etio-logic component of other gastrointestinal diseases includingmultifocal atrophic gastritis, gastric carcinoma, and primarygastric lymphoma (3–13). In 1994, an International Agencyfor Research on Cancer working group evaluated the scien-tific findings linking this infection to cancer of the stomachand concluded thatH. pylori is carcinogenic to humans (14).The evidence of an association betweenH. pylori and non-ulcer dyspepsia (NUD) is still inconclusive (15–18).
Upper gastrointestinal symptoms are common reasons forpatients to visit both primary care physicians (PCPs: inter-nists [IMs] and family/general practitioners [FPs]) and gas-troenterologists. In recent years, the development of nonin-vasive H. pylori detection methods, including serologicalassays and the urea breath test, has enabled PCPs to diag-nose and treatH. pylori infection without the involvement ofgastroenterologists. The extent to which research findingsregardingH. pylori have modified the practice of physiciansin general has not been well studied. Clinical application ofcurrent knowledge is crucial, given that inadequate treat-ment of peptic ulcer disease results in therapy failures, highrecurrence rates, the emergence of resistant bacterial strains,and increased health care costs.
We conducted the present study to investigate the extentto which the scientific literature regardingH. pylori infec-tion has reached the general community of physicians andwhether this knowledge has influenced their diagnostic andtherapeutic practices. We were particularly interested inobserving whether responses of clinicians to current knowl-edge depend on the area of medical specialty. Such a dis-tinction is important for health policy decision makers givenongoing discussions of the optimal balance of PCPs andReceived July 9, 1997; accepted Jan. 12, 1998.
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 93, No. 4, 1998Copyright © 1998 by Am. Coll. of Gastroenterology ISSN 0002-9270/98/$19.00Published by Elsevier Science Inc. PII S0002-9270(98)00041-0
553

specialists and the trend toward decreasing the number ofpatients referred to specialty physicians.
MATERIALS AND METHODS
From February through May of 1996, we conducted anational mail survey of 5994 U.S. physicians selected atrandom (according to a computer-generated randomizationlist by each association) from membership databases of thefollowing professional associations:American Academy ofFamily Physicians(2,000 selected from the total member-ship of 44,400 FPs);American College of Physicians(1,994[16 incomplete addresses on received data file] selectedfrom the total membership of 87,179 IM specialists); andAmerican College of Gastroenterology(2,000 selected fromthe total membership of 9,000 gastroenterologists).
To maximize the response rate, follow-up mailings weresent according to the following schedule: 8 wk after the firstmailing a second questionnaire was sent to selected partic-ipants who did not respond to the initial mailing within 6wk; a reminder postcard was sent to those who did notrespond to the first mailing 2 wk after the second mailing.Finally, a third questionnaire was sent by registered mail tothose who did not respond to the reminder postcard within8 wk. In the final mailing we asked physicians who wereretired or had no contact with patients to return the blankquestionnaire and identify their area of specialization. Weterminated the study at the end of July 1996, 2 months afterthe final mailing.
To evaluate the response rate, we classified physicians inthe original sample as responders or nonresponders. Re-sponders were further classified as eligible or ineligiblebased on self-reported medical specialty. Responders wereineligible if the self-reported area of specialty differed fromthat of the database from which they were selected, if theydid not state a field of specialization, or if they were notactive in clinical medicine. We defined the response rate asthe fraction of eligible responders out of all selected subjectswho met the eligibility criteria (19). Because the denomi-nator for this proportion is unknown, we assumed that theeligibility of nonresponders was equal to the eligibility ofthose who responded to the last mailing, given that thisgroup should have characteristics that most closely resemblethe nonresponders (receipt of this mailing was verified andineligible recipients were specifically encouraged to re-spond).
The five-page questionnaire covered topics concerningmanagement of suspected peptic ulcer disease, treatment ofconfirmed ulcer disease, and treatment of confirmedH.pylori infection in patients with diverse disease presenta-tions (dyspepsia, ulcer, atrophic gastritis of the antrum,localized low-grade malignant mucosa-associated lymphoidtissue [MALT] lymphoma of the gastric mucosa, and familyhistory of gastric cancer). Physicians were further askedabout sources of information regardingH. pylori infection.Participants could rate the different sources of information
on an ordinal 5-point rating scale (0–4: no, minimal, mod-erate, substantial, or extensive information). To observewhether there is a differential time lag in the disseminationof scientific findings to PCPs and specialists, we asked thedifferent physician groups about their knowledge of therelationship betweenH. pylori gastritis and peptic ulcerdisease, which has been widely discussed in the medicalliterature for over 5 yr and of the more recent 1994 NIHrecommendations to treatH. pylori-infected peptic ulcerpatients with antimicrobial agents, whether on first presen-tation or recurrence (20).
To evaluate the influence of scientific evidence on treat-ment choices forH. pylori infection, we classified the re-ported regimens according to their cure rates, as summa-rized by van der Hulstet al. (21). State-of-the-art regimens(class A) were combinations of antimicrobials that have ledto cure rates of at least 80% in clinical trials conducted inseveral geographical locations, as reported in the literature.These regimens included proton pump inhibitor (PPI)-basedtriple therapies using PPI with two antibiotics selected fromamoxicillin, clarithromycin, or metronidazole (22–24); stan-dard triple therapy using bismuth, tetracycline, and metro-nidazole (25); quadruple therapy (standard triple therapyplus PPI or H2-receptor antagonist [26, 27]); and dual ther-apy using PPI plus clarithromycin. Regimens with knownpoor cure rates (class B) were therapies that have resulted inpoor cure rates in clinical trials reported in the literature.These regimens included mono therapies and dual therapiesother than PPI plus clarithromycin. Regimens with unknownperformance (class C) were therapies that have not beenevaluated in clinical trials reported in the literature.
Data were entered by computer using Microsoft Excel forWindows 95, Version 7.0 (Microsoft, Seattle, WA). Thebasic analytic approach was the comparison of responsesacross physician groups. Whenever the responses of IMsand FPs did not show a meaningful difference, the twogroups were combined because the comparison of specialistversusnonspecialist was the primary interest.p values forresponse differences across groups were based on thex2-testfor contingency tables with categorical variables. Student’st test was used for comparing the mean proportion of pa-tients for whom the two physicians groups (gastroenterolo-gists, PCPs) would prescribe treatment without orderingdiagnostic tests (possible response, 0% to 100%). Thesetechniques were implemented using SAS 6.11 statisticalsoftware package (SAS Institute, Cary, NC). Binomial 95%confidence intervals (CI) for single proportions were calcu-lated using Epi-Info 6, version 6.04a (Centers for DiseaseControl and Prevention, Atlanta, GA). Data are presented asmean6 SD unless stated otherwise.
RESULTS
Response
Of the 5994 selected physicians, 2831 (47%) respondedto the questionnaire, while 194 (3%) were deceased or not
554 BREUERet al. AJG – Vol. 93, No. 4, 1998
located by the post office. Of the 2831 responders, 35%responded to the first mailing, 27% to the second, and 38%to the third; 2122 (75%) of those who responded met thecriteria for eligibility. Assuming that the eligibility rateamong nonresponders equals the eligibility of those re-sponding to the third mailing (65%), the overall responserate was 52%. The response rates by physician group were62% of gastroenterologists, 51% of IMs, and 43% of FPs.
Sources of information
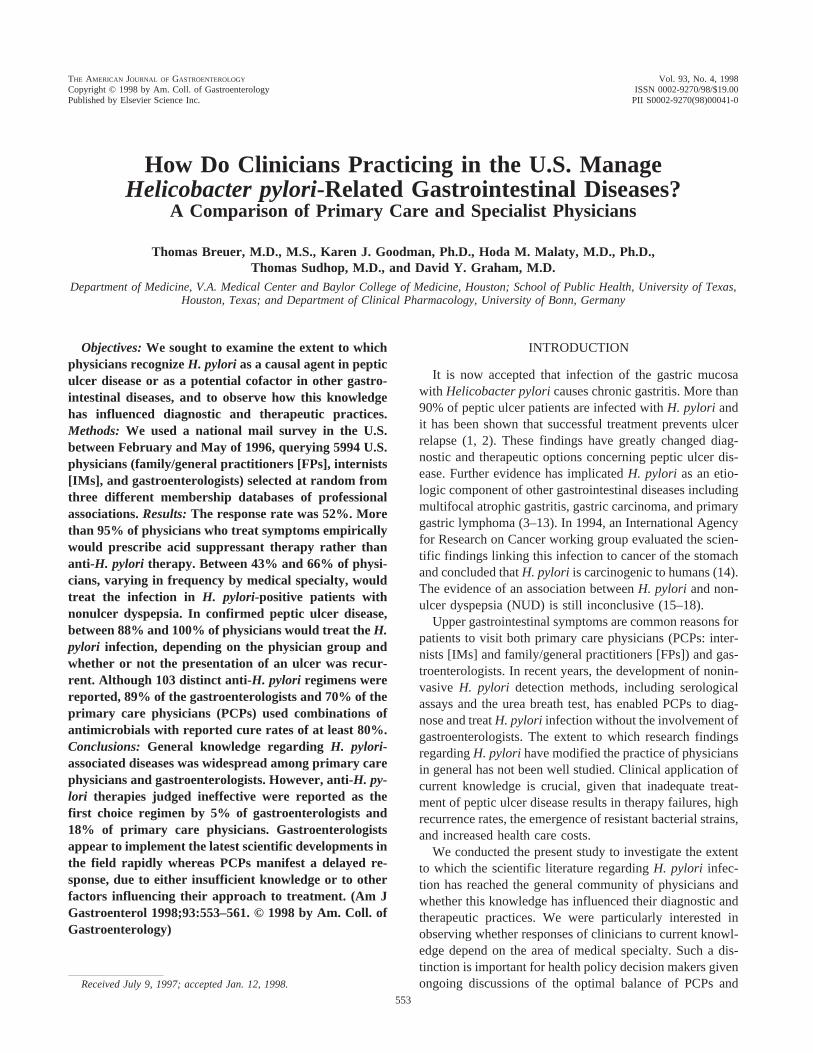
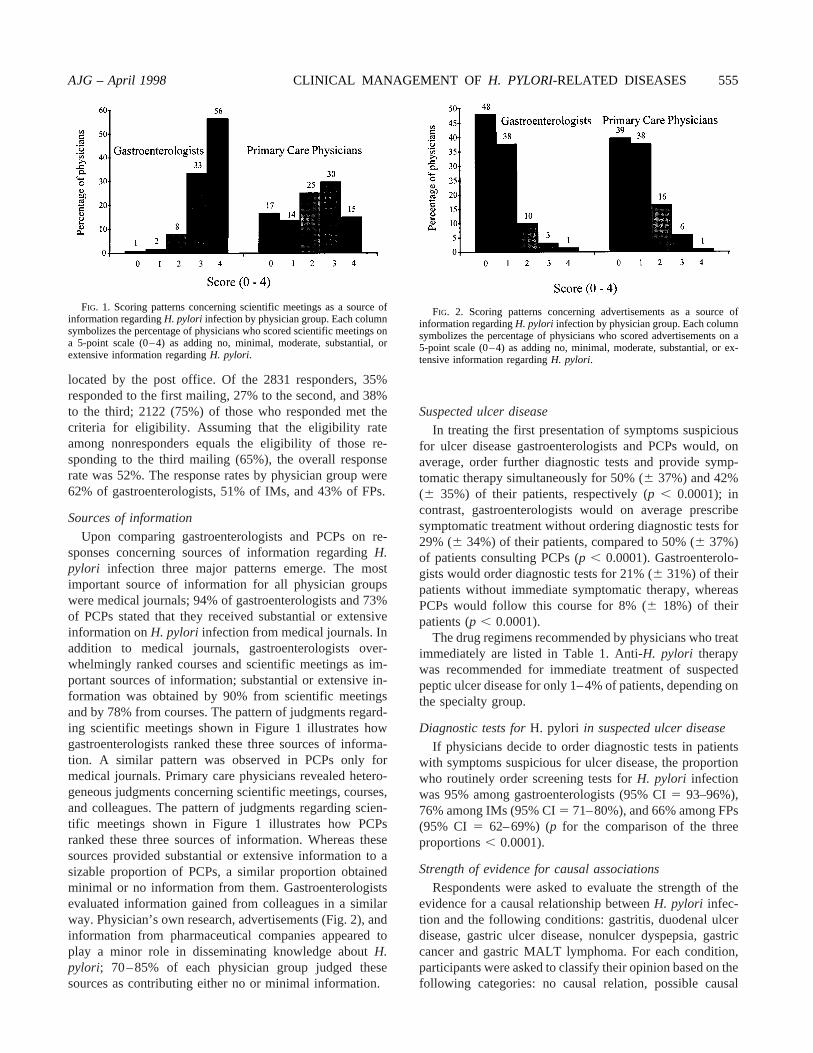
Upon comparing gastroenterologists and PCPs on re-sponses concerning sources of information regardingH.pylori infection three major patterns emerge. The mostimportant source of information for all physician groupswere medical journals; 94% of gastroenterologists and 73%of PCPs stated that they received substantial or extensiveinformation onH. pylori infection from medical journals. Inaddition to medical journals, gastroenterologists over-whelmingly ranked courses and scientific meetings as im-portant sources of information; substantial or extensive in-formation was obtained by 90% from scientific meetingsand by 78% from courses. The pattern of judgments regard-ing scientific meetings shown in Figure 1 illustrates howgastroenterologists ranked these three sources of informa-tion. A similar pattern was observed in PCPs only formedical journals. Primary care physicians revealed hetero-geneous judgments concerning scientific meetings, courses,and colleagues. The pattern of judgments regarding scien-tific meetings shown in Figure 1 illustrates how PCPsranked these three sources of information. Whereas thesesources provided substantial or extensive information to asizable proportion of PCPs, a similar proportion obtainedminimal or no information from them. Gastroenterologistsevaluated information gained from colleagues in a similarway. Physician’s own research, advertisements (Fig. 2), andinformation from pharmaceutical companies appeared toplay a minor role in disseminating knowledge aboutH.pylori; 70–85% of each physician group judged thesesources as contributing either no or minimal information.
Suspected ulcer disease
In treating the first presentation of symptoms suspiciousfor ulcer disease gastroenterologists and PCPs would, onaverage, order further diagnostic tests and provide symp-tomatic therapy simultaneously for 50% (6 37%) and 42%(6 35%) of their patients, respectively (p , 0.0001); incontrast, gastroenterologists would on average prescribesymptomatic treatment without ordering diagnostic tests for29% (6 34%) of their patients, compared to 50% (6 37%)of patients consulting PCPs (p , 0.0001). Gastroenterolo-gists would order diagnostic tests for 21% (6 31%) of theirpatients without immediate symptomatic therapy, whereasPCPs would follow this course for 8% (6 18%) of theirpatients (p , 0.0001).
The drug regimens recommended by physicians who treatimmediately are listed in Table 1. Anti-H. pylori therapywas recommended for immediate treatment of suspectedpeptic ulcer disease for only 1–4% of patients, depending onthe specialty group.
Diagnostic tests forH. pylori in suspected ulcer disease
If physicians decide to order diagnostic tests in patientswith symptoms suspicious for ulcer disease, the proportionwho routinely order screening tests forH. pylori infectionwas 95% among gastroenterologists (95% CI5 93–96%),76% among IMs (95% CI5 71–80%), and 66% among FPs(95% CI 5 62–69%) (p for the comparison of the threeproportions, 0.0001).
Strength of evidence for causal associations
Respondents were asked to evaluate the strength of theevidence for a causal relationship betweenH. pylori infec-tion and the following conditions: gastritis, duodenal ulcerdisease, gastric ulcer disease, nonulcer dyspepsia, gastriccancer and gastric MALT lymphoma. For each condition,participants were asked to classify their opinion based on thefollowing categories: no causal relation, possible causal
FIG. 1. Scoring patterns concerning scientific meetings as a source ofinformation regardingH. pylori infection by physician group. Each columnsymbolizes the percentage of physicians who scored scientific meetings ona 5-point scale (0–4) as adding no, minimal, moderate, substantial, orextensive information regardingH. pylori.
FIG. 2. Scoring patterns concerning advertisements as a source ofinformation regardingH. pylori infection by physician group. Each columnsymbolizes the percentage of physicians who scored advertisements on a5-point scale (0–4) as adding no, minimal, moderate, substantial, or ex-tensive information regardingH. pylori.
AJG – April 1998 CLINICAL MANAGEMENT OF H. PYLORI-RELATED DISEASES 555
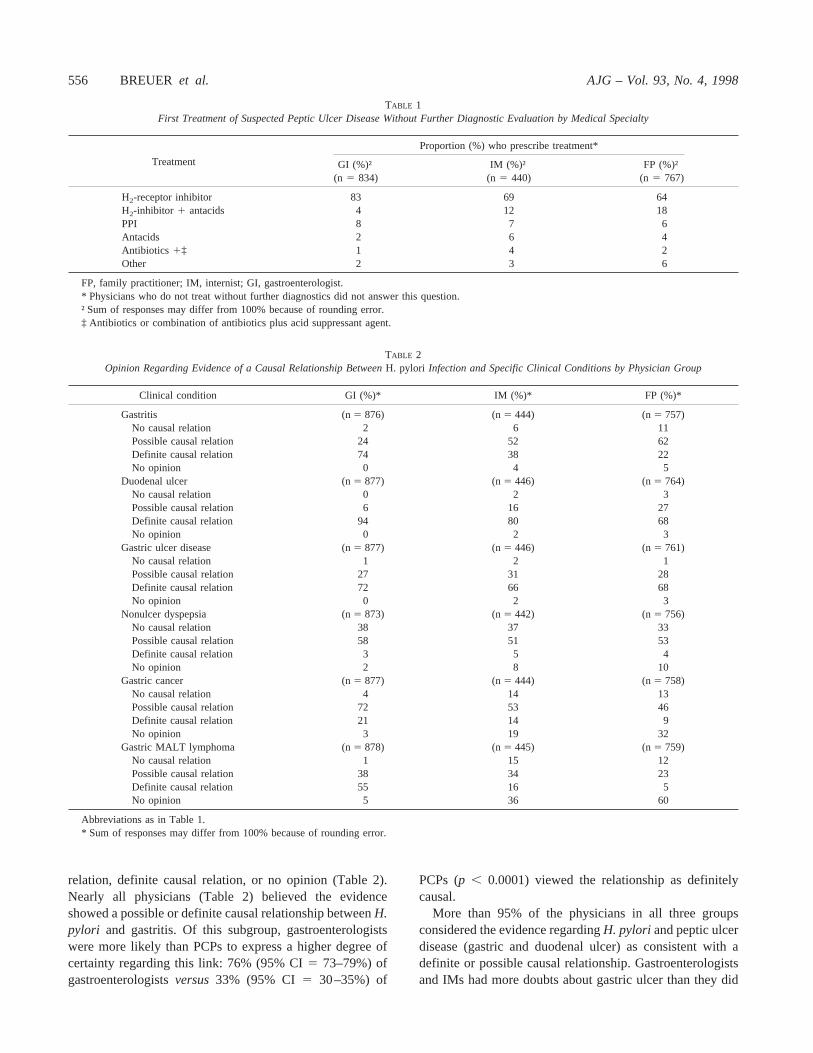
relation, definite causal relation, or no opinion (Table 2).Nearly all physicians (Table 2) believed the evidenceshowed a possible or definite causal relationship betweenH.pylori and gastritis. Of this subgroup, gastroenterologistswere more likely than PCPs to express a higher degree ofcertainty regarding this link: 76% (95% CI5 73–79%) ofgastroenterologistsversus33% (95% CI 5 30–35%) of
PCPs (p , 0.0001) viewed the relationship as definitelycausal.
More than 95% of the physicians in all three groupsconsidered the evidence regardingH. pylori and peptic ulcerdisease (gastric and duodenal ulcer) as consistent with adefinite or possible causal relationship. Gastroenterologistsand IMs had more doubts about gastric ulcer than they did
TABLE 1First Treatment of Suspected Peptic Ulcer Disease Without Further Diagnostic Evaluation by Medical Specialty
Treatment
Proportion (%) who prescribe treatment*
GI (%)†(n 5 834)
IM (%)†(n 5 440)
FP (%)†(n 5 767)
H2-receptor inhibitor 83 69 64H2-inhibitor 1 antacids 4 12 18PPI 8 7 6Antacids 2 6 4Antibiotics 1‡ 1 4 2Other 2 3 6
FP, family practitioner; IM, internist; GI, gastroenterologist.* Physicians who do not treat without further diagnostics did not answer this question.† Sum of responses may differ from 100% because of rounding error.‡ Antibiotics or combination of antibiotics plus acid suppressant agent.
TABLE 2Opinion Regarding Evidence of a Causal Relationship BetweenH. pylori Infection and Specific Clinical Conditions by Physician Group
Clinical condition GI (%)* IM (%)* FP (%)*
Gastritis (n5 876) (n5 444) (n5 757)No causal relation 2 6 11Possible causal relation 24 52 62Definite causal relation 74 38 22No opinion 0 4 5
Duodenal ulcer (n5 877) (n5 446) (n5 764)No causal relation 0 2 3Possible causal relation 6 16 27Definite causal relation 94 80 68No opinion 0 2 3
Gastric ulcer disease (n5 877) (n5 446) (n5 761)No causal relation 1 2 1Possible causal relation 27 31 28Definite causal relation 72 66 68No opinion 0 2 3
Nonulcer dyspepsia (n5 873) (n5 442) (n5 756)No causal relation 38 37 33Possible causal relation 58 51 53Definite causal relation 3 5 4No opinion 2 8 10
Gastric cancer (n5 877) (n5 444) (n5 758)No causal relation 4 14 13Possible causal relation 72 53 46Definite causal relation 21 14 9No opinion 3 19 32
Gastric MALT lymphoma (n5 878) (n5 445) (n5 759)No causal relation 1 15 12Possible causal relation 38 34 23Definite causal relation 55 16 5No opinion 5 36 60
Abbreviations as in Table 1.* Sum of responses may differ from 100% because of rounding error.
556 BREUERet al. AJG – Vol. 93, No. 4, 1998

about duodenal ulcer. Family/general practitioners did notappear to differentiate between the two ulcer types. Gastro-enterologists were more likely than PCPs to view the rela-tionship betweenH. pylori and duodenal ulcer disease asdefinitely causal: 94% (95% CI5 92–96%) of the gastro-enterologistsversus76% (95% CI5 73–78%) of PCPs (p ,0.0001). For gastric ulcer disease, the proportion evaluatingthe link with H. pylori as definitely causal differed little byphysician group: 72% (95% CI5 69–75%) of gastroenter-ologistsversus70% (95% CI5 67–73%) of PCPs (p 50.2214). All gastroenterologists and 95–98% of the otherphysician groups indicated an opinion regarding the strengthof the evidence for gastritis, duodenal ulcer, and gastriculcer. Slightly over half of the respondents in each physiciangroup believed there is a possible causal relationship be-tweenH. pylori infection and nonulcer dyspepsia, whereasroughly a third of each group believed there is no causalrelationship. The proportion having no opinion regardingthe strength of the evidence for nonulcer dyspepsia was 2%among gastroenterologists and 8–10% among PCPs. Nearlyall gastroenterologists believed that there is a possible ordefinite causal relationship betweenH. pylori and gastricmalignancies and were more certain of causality for MALTlymphoma than for carcinoma. A small proportion of PCPsbelieved there was a definite causal relationship betweenH.pylori infection and either carcinoma or lymphoma, whereasa large proportion had no opinion regarding the strength ofthe evidence for cancer (Table 2).
Treatment ofH. pylori infection in patients withconfirmedH. pylori-positive ulcer disease
Nearly 100% of the gastroenterologists reported theywould use anti-H. pylori treatment in theirH. pylori-positivepatients with peptic ulcer disease, without differentiatingbetween first and recurrent presentation (Table 3). Morethan 95% of PCPs would treat the infection in patients with
H. pylori-positive recurrent peptic ulcer disease, whereas6–10% fewer would treat the infection in cases presentingfor the first time (Table 3).
When asked to specify therapeutic regimens used to treatdiagnosedH. pylori infection in patients with confirmedpeptic ulcer disease, a total of 103 distinct regimens werereported, although the majority of respondents used a smallnumber of regimens. Approximately 40% of each groupused bismuth-based triple therapies (Table 4). Another 40%of gastroenterologists used PPI-based triple therapies, thecombination containing PPI, clarithromycin, and metroni-dazole being mentioned most frequently (by 28% of gas-troenterologists, 10% of IMs, and 6% of FPs). The use ofdual therapies was far less common in the three physiciangroups. PPI combined with amoxicillin, a regimen with aknown poor cure rate, was mentioned infrequently (4% ofgastroenterologists, 5% of PCPs). The total proportion ofphysicians using Class B or C regimens (known pure curerate or unknown performance) was 31% among PCPs and11% among gastroenterologists.
Other gastrointestinal diseases associated withH. pyloriinfection
A substantial proportion of physicians reported that theywould use antibiotics to treat infection inH. pylori-positivepatients with nonulcer dyspepsia: 66% (95% CI5 63–70%)of FPs, 49% (95% CI5 44–54%) of IMs, and 43% (95%CI 5 39–46%) of gastroenterologists. The proportion ofphysicians who would use antibiotics to treat confirmedH.pylori infection in patients with a family history of gastriccancer was 53% (95% CI5 49–56%) among gastroenter-ologists, 35% (95% CI5 30–40%) among IMs, and 41%(95% CI 5 38–45%) among FPs, whereas anti-H. pyloritherapy was recommended for infected patients with atro-phic gastritis by 39% of gastroenterologists and 46% ofPCPs.
TABLE 3Percent of Physicians Who Recommend Use of Antibiotics to Treat DiagnosedH. pylori Infection by Disease Presentation and Medical Specialty
Disease Presentation
Percent Treating DiagnosedH. pylori Infection
Specialist PCP
GI % (n)* IM % (n)* FP % (n)*
Ulcer diseaseUncomplicated duodenal ulcer(first presentation)
99 (863/876) 89 (393/440) 88 (656/749)
Uncomplicated duodenal ulcer(recurrent)
100 (875/877) 96 (422/441) 95 (709/748)
Uncomplicated gastric ulcer(first presentation)
97 (849/877) 88 (388/440) 91 (686/751)
Uncomplicated gastric ulcer(recurrent)
99 (866/877) 98 (433/441) 97 (728/751)
Other clinical profilesNonulcer dyspepsia 43 (370/866) 49 (211/433) 66 (492/742)Family history of gastric cancer 53 (457/869) 35 (152/437) 41 (306/744)Atrophic gastritis of the antrum 39 (339/868) 46 (199/435) 46 (337/739)
Abbreviations as in Table 1.* Sum of responses may differ from 100% because of rounding error.
AJG – April 1998 CLINICAL MANAGEMENT OF H. PYLORI-RELATED DISEASES 557

DISCUSSION
We conducted the present study to investigate the extentto which scientific knowledge regardingH. pylori infectionhas influenced the practice of physicians in the U.S. andwhether PCPs and gastroenterologists have been influencedto different degrees. Primary care physicians reported thatthey do not pursue diagnostic evaluation for 50% of thepatients in whom they suspected ulcer disease for the firsttime, treating these patients symptomatically. Anti-H. pyloritherapy was almost never recommended for suspected ulcerdisease without the prior use of diagnostic tests by any of thephysician groups investigated. Therapeutic regimens recom-mended by physicians who did not order diagnostic tests forthe first presentation of suspected ulcer disease rely mostlyon antisecretory therapy. It is possible that a high percentageof PCPs treat the initial onset of a suspected ulcer empiri-cally without consideringH. pylori infection and then referrecurrent onsets to a specialist. It should be noted that aboutone-third of patients presenting for the first time to gastro-enterologists with symptoms suspicious for ulcer disease aretreated empirically as well. Although we do not know theproportion of patients with symptoms suspicious for pepticulcer disease who actually have an ulcer, we suspect that thenumber of patients with ulcers in this group will be sub-stantial. Therefore, the opportunity to diagnose and treat theunderlying disease is currently being missed in these pa-tients when they first seek help.
More than 65% of the physicians in all three groupsbelieved that the evidence regardingH. pylori and bothgastric and duodenal ulcers demonstrated a definite causalrelationship, whereas the remainder accepted the possibility
of causality. Although PCPs were more tentative in theiropinions than gastroenterologists, this high proportion sug-gests that U.S. physicians in general have accepted thescientific evidence regarding the infectious etiology of pep-tic ulcer disease and viewH. pylori as a cause of thisdisease. This acceptance is further confirmed upon notingthat nearly 100% of all three groups of physicians recom-mended antibiotic therapy for recurrent peptic ulcer disease.A small percentage of PCPs distinguish the approach takenfor first and recurrent presentation of disease. The recom-mendation to use antibiotics only for recurrent peptic ulcerdisease appeared frequently in the literature before the NIHconsensus statement of 1994 (28). We interpret these data asa sign of a more rapid dissemination of new knowledge inthe field to specialists than to general practitioners (Table 3).It is interesting to note that fewer physicians in all threegroups were convinced of causality in the case of gastritisthan in that of peptic ulcer disease, given thatH. pylori-induced gastritis precedes the development ofH. pylori-associated peptic ulcer disease. This suggests a lack ofunderstanding of the role of gastritis in ulcer disease, prob-ably due to a lack of attention paid to aspects of the diseasethat are not connected to clinical features.
Approximately 40–70% of the responding physicians,varying in frequency by medical specialty, reported thatthey would use antibiotic therapy forH. pylori-positivepatients with nonulcer dyspepsia, in spite of the small pro-portion who believed thatH. pylori causes nonulcer dys-pepsia. We therefore looked at the opinions regarding cau-sality for H. pylori and nonulcer dyspepsia among the 1073physicians who indicated that they would treat the infection
TABLE 4Therapeutic Regimens to Cure DiagnosedH. pylori Infection in Confirmed Peptic Ulcer Disease by Medical Specialty
Treatment choiceGI %
(n 5 881)IM %
(n 5 445)FP %
(n 5 764)
By regimenBismuth-based (total)* 38 37 41
Bismuth-based triple 15 20 23Bismuth-based triple1 PPI 15 11 10Bismuth-based triple1 H2 8 5 9
PPI-based triple (total)* 40 19 16PPI 1 CLA 1 MET 30 10 7PPI 1 CLA 1 AMO 5 2 1PPI 1 AMO 1 MET 4 6 7
PPI/CLA* 11 13 13Other 11 31 31
By classClass A (state-of-the-art) 89 69 70Class B (known poor cure rate) 5 15 19Class C (unknown performance) 6 16 12
PPI, proton pump inhibitor; AMO, amoxicillin; H2, H2 inhibitors; CLA, clarithromycin; bismuth-based triple, bismuth plus metronidazole plus tetracyclineor amoxicillin; PPI-based triple, PPI plus combination of two of the following antibiotics: amoxicillin, clarithromycin, tetracycline. Other abbreviations asin Table 1.
* State-of-the-art regimens (for details refer to text).Sum of responses may be different than 100% because of rounding error.
558 BREUERet al. AJG – Vol. 93, No. 4, 1998

in nonulcer dyspepsia patients. In this subset, the responsesvaried little by physician group: 6% believed there was adefinite causal relationship, 68% believed there was a pos-sible causal relationship, whereas 20% believed the rela-tionship was not causal, and 6% had no opinion.
Given that the 1994 NIH consensus statement concludedthat there was no convincing evidence of a causal relation-ship betweenH. pylori infection and nonulcer dyspepsia andtherefore no indication for antibiotic treatment ofH. pylori-positive patients with nonulcer dyspepsia (20), it appearsthat a large proportion of physicians ignore both the NIHconsensus statement and their own beliefs regarding theH.pylori-nonulcer dyspepsia association when they treatH.pylori-infected nonulcer dyspepsia patients. A possible ex-planation could be a tendency to treat allH. pylori-positivepatients once the infection has been diagnosed, regardless ofthe underlying disease. In light of the potential demand bypatients to have this infection treated, along with the linkbetweenH. pylori infection and gastric malignancies, webelieve such an approach is reasonable.
Few physicians believed thatH. pylori definitely causesgastric cancer. Primary care physicians were more likely tohave no opinion regarding cancer than regarding gastritis,ulcer, and nonulcer dyspepsia. Gastroenterologists weremost likely to believe in the possibility of a causal relation-ship and to recommend anti-H. pylori treatment in patientswith a family history of gastric cancer. The majority ofgastroenterologists indicated the opinion thatH. pylori in-fection definitely causes low-grade gastric MALT lym-phoma, possibly reflecting knowledge of clinical studies inwhich lymphomas regressed in manyH. pylori-infectedcases after cure of the infection (29–32).
The most effectiveH. pylori regimens (Class A) are usedby nearly all gastroenterologists and the majority of PCPs.PPI-based triple therapies were used to a much greaterextent by gastroenterologists than by PCPs, suggesting amore rapid adoption by gastroenterologists. Several expla-nations may account for the delayed adoption of the latesttreatment developments by PCPs: a slower dissemination ofnew treatment patterns to PCPs, a wait-and-see attitude innewly emerging treatments, greater caution in applyingmore costly regimens without being certain of potentialbenefits, or greater restrictions on treatment options bymanaged care providers. Five percent of gastroenterologistsand over 15% of PCPs used regimens with known poor curerates, suggesting that an important percentage of physiciansare inadequately informed regarding the drug combinationsused to cure patients of theH. pylori infection.
A major concern regarding this survey is how represen-tative the responders are of the target populations. Ourresponse rate of 52%, which we optimized by applying anextended schedule of repeated mailings as recommended byexperts who have perfected mail survey techniques (33–35),is consistent with the maximum response to be expected ina national mail survey of physicians. Nevertheless, validinterpretation of the study results requires assumptions re-
garding differences between responders and nonrespondersin terms of knowledge about the role ofH. pylori infectionin gastrointestinal disease. We presume that physicians whohave a greater interest in peptic ulcer disease and/orH.pylori infection would be more motivated to respond to thissurvey. It is, therefore, probable that responders include agreater proportion of physicians who are knowledgeableabout the subject matter of the questionnaire than nonre-sponders. This assumption is consistent with the observationthat gastroenterologists had a higher response rate than theother physician groups. Furthermore, there is no reason tosuppose that respondents reflect lower levels of knowledgeregarding current recommendations concerning the manage-ment of peptic ulcer disease than exists among nonrespon-dents. Therefore, any existing selection bias is likely tooverestimate the proportion of physicians who manageH.pylori-related diseases in accordance with current recom-mendations and to underestimate differences between gas-troenterologists and PCPs. Statistically significant differ-ences between gastroenterologists and PCPs are thereforenot likely to be due to bias; to the contrary, the true differ-ences may be even greater. Misclassification of the medicalspecialty is unlikely because we included only those physi-cians who reported the same specialty indicated by theprofessional association. Furthermore, 99% of gastroenter-ologists stated that they perform esophagogastroduodenos-copy, whereas very few PCPs reported that they performthis procedure.
Worldwide, studies of physicians’ knowledge regardingH. pylori in gastroduodenal disease are sparse and have beendone primarily in Europe (36–38). In comparing resultsacross studies, differences in year, location, and the natureof the questions posed must be considered. The only previ-ously reported survey of U.S. physicians was conducted byFendrick and colleagues (39) about 2 yr before the presentstudy, using the same membership databases to select theirparticipants. The earlier study (39) also elicited opinionsregarding the strength of the evidence thatH. pylori causesvarious gastroduodenal diseases. For each category of dis-ease, the proportion expressing no opinion was roughlytwice as large as what we observed in the current study,suggesting an overall increase in awareness.
A study similar in design to the current study was con-ducted in Germany in 1995, 5 months before we initiated thecurrent study (38), using nearly identical questions. Re-sponses of U.S. and German physicians concerning knowl-edge and the inclination to treatH. pylori infection invarious clinical contexts were similar in both countries,whereas large differences were observed in the specifictherapeutic regimens prescribed. Whereas bismuth-basedtriple therapies were used by approximately 40% of the U.S.physicians,, 1% of German doctors used this regimen. Themost favored regimen among the German physicians wasdual therapy using PPI plus amoxicillin, which was recom-mended by not more than 5% of the U.S. physicians. Mostof the initial clinical research on PPI plus amoxicillin ther-
AJG – April 1998 CLINICAL MANAGEMENT OF H. PYLORI-RELATED DISEASES 559

apy was done by German researchers (40–42), who re-ported good cure rates with this simplified treatment. Later,studies in other locales (21, 43–45) were unable to replicateequally good results. This contrast suggests that local com-munities of physicians are likely to apply research findingsthat are published and promoted by local opinion leaders.
Other studies (36, 39) have confirmed our finding thatmedical journals are the most important source of informa-tion on H. pylori infection among general practitioners,whereas gastroenterologists find educational events to be anequally important source of information.
In conclusion, gastroenterologists appear to implementnew scientific developments in the field more rapidly,whereas PCPs manifest a delayed response, due to eitherinsufficient knowledge or to other factors influencing theirapproach to treatment.
ACKNOWLEDGMENTS
This work was supported by the Department of VeteransAffairs and by the generous support of Hilda Schwartz.Astra Merck assisted in paying for printing the question-naires and the postage. Dr. Breuer was supported in part bya grant from the epidemiology program of the GermanAcademic Exchange Program (DAAD). Dr. Sudhop wassupported in part by grant 01EC9402 from the GermanMinistry for Research and Technology (BMFT). Wethank A. Singh for helping in the preparation of themanuscript.
Reprint requests and correspondence: David Y. Graham, M.D., V.A.Medical Center (111 D), 2002 Holcombe Blvd., Rm. 3A352, Houston, TX77030.
REFERENCES
1. Marshall BJ, Goodwin CS, Warren JR, et al. Prospective double-blindtrial of duodenal ulcer relapse after eradication ofCampylobacterpylori. Lancet 1988;2:1437–42.
2. Graham DY, Lew GM, Klein PD, et al. Effect of treatment ofHeli-cobacter pylori infection on the long-term recurrence of gastric orduodenal ulcer. A randomized, controlled study. Ann Intern Med1992;116:705–8.
3. Correa P, Ruiz B, Hunter F. Clinical trials as etiologic research toolsin Helicobacter-associated gastritis. Scand J Gastroenterol 1991;181(suppl):15–9.
4. Parsonnet J, Friedman GD, Vandersteen DP, et al.Helicobacter pyloriinfec-tion and the risk of gastric carcinoma. N Engl J Med 1991;325:1127–31.
5. Parsonnet J, Hansen S, Rodriguez L, et al.Helicobacter pyloriinfec-tion and gastric lymphoma. N Engl J Med 1994;330:1267–71.
6. Nomura A, Stemmermann GN, Chyou PH, et al.Helicobacter pyloriinfection and gastric carcinoma among Japanese Americans in Hawaii.N Engl J Med 1991;325:1132–6.
7. Fukao A, Komatsu S, Tsubono Y, et al.Helicobacter pyloriinfectionand chronic atrophic gastritis among Japanese blood donors: A cross-sectional study. Cancer Causes Control 1993;4:307–12.
8. Forman D, Newell DG, Fullerton F, et al. Association between infec-tion with Helicobacter pyloriand risk of gastric cancer: Evidence froma prospective investigation. BMJ 1991;302:1302–5.
9. Craanen ME, Dekker W, Blok P, et al. Intestinal metaplasia andHelicobacter pylori: An endoscopic bioptic study of the gastric antrum.Gut 1992;33:16–20.
10. Graham DY, Lew GM, Klein PD, et al. Effect of treatment ofHeli-cobacter pylori infection on the long-term recurrence of gastric or
duodenal ulcer. A randomized, controlled study. Ann Intern Med1992;116:705–8.
11. Graham DY, Hepps KS, Ramirez FC, et al. Treatment ofHelicobacterpylori reduces the rate of rebleeding in peptic ulcer disease. Scand JGastroenterol 1993;28:939–42.
12. Bayerdorffer E, Neubauer A, Rudolph B, et al. Regression of primarygastric lymphoma of mucosa-associated lymphoid tissue type aftercure ofHelicobacter pyloriinfection. MALT Lymphoma Study Group.Lancet 1995;345:1591–4.
13. Stolte M.Helicobacter pylorigastritis and gastric MALT-lymphoma.Lancet 1992;339:745–6.
14. IARC Working Group on the Evaluation of Carcinogenic Risks toHumans. IARC Working Group: Schistosomes, liver flukes andHel-icobacter pylori. Lyon, 7–14 June 1994. IARC Monogr Eval CarcinogRisks Hum 1994;61:1–241.
15. Greenberg RE, Bank S. The prevalence ofHelicobacter pylori innonulcer dyspepsia. Importance of stratification according to age. ArchIntern Med 1990;150:2053–5.
16. Talley NJ. The role ofHelicobacter pyloriin nonulcer dyspepsia. Adebate against. Gastroenterol Clin North Am 1993;22:153–67.
17. Holtmann G, Goebell H, Holtmann M, et al. Dyspepsia in healthyblood donors. Pattern of symptoms and association withHelicobacterpylori. Dig Dis Sci 1994;39:1090–8.
18. Colin-Jones DG. Dyspepsia update. Scand J Gastroenterol 1995;210(suppl):32–5.
19. Siebert C, Lipsett LF, Greenblatt J, et al. Survey of physician practicebehaviors related to diabetes mellitus in the U.S. I. Design and meth-ods. Diabetes Care 1993;42:759–64.
20. Helicobacter pyloriin peptic ulcer disease. NIH Consensus Statement1994;12:1–23.
21. van der Hulst RWM, Keller JJ, Rauws EA, et al. Treatment ofHeli-cobacter pyloriinfection in humans: A review of the world literature.Helicobacter 1996;1:6–19.
22. Bazzoli F, Zagari RM, Fossi S, et al. Short term, low dose tripletherapy for the eradication ofHelicobacter pylori. Eur J GastroenterolHepatol 1994;6:773–7.
23. Labenz J, Ru¨hl GH, Stolte M, et al. Efficacy of low-dose one-weektriple therapy to cureH. pylori infection. Am J Gastroenterol 1994;89:A364.
24. Labenz J, Stolte M, Ru¨hl G, et al. One-week low-dose triple therapy forthe eradication ofHelicobacter pyloriinfection. Eur J GastroenterolHepatol 1995;7:9–11.
25. Chiba N, Rao BV, Rademaker JW, et al. Meta-analysis of the efficacyof antibiotic therapy in eradicatingHelicobacter pylori. Am J Gastro-enterol 1992;87:1716–27.
26. de Boer W, Driessen W, Jansz A, et al. Effect of acid suppression onefficacy of treatment forHelicobacter pyloriinfection. Lancet 1995;345:817–20.
27. de Boer WA, Driessen WM, Potters VP, et al. Randomized studycomparing 1 with 2 weeks of quadruple therapy for eradicatingHeli-cobacter pylori. Am J Gastroenterol 1994;89:1993–7.
28. Heatley RV. Review article. The treatment ofHelicobacter pyloriinfection. Aliment Pharmacol Ther 1992;6:291–303.
29. Bayerdo¨rffer E, Neubauer A, Rudolph B, et al. Regression of primarygastric lymphoma of mucosa-associated lymphoid tissue type aftercure ofHelicobacter pyloriinfection. Lancet 1995;345:1591–4.
30. Cammarota G, Tursi A, Montalto M, et al. Prevention and treatment oflow-grade B-cell primary gastric lymphoma by anti-H. pylori therapy.J Clin Gastroenterol 1995;21:118–22.
31. Binek J, Morant R, Weber A, et al. MALT-type low-grade B-celllymphomas of the stomach andHelicobacter pylori. SchweizerischeMedizinische Wochenschrift 1996;841–4.
32. Alkan S, Karcher DS, Newman MA, et al. Regression of salivary glandMALT lymphoma after treatment forHelicobacter pylori. Lancet1996;348:268–9.
33. Shahar E, Bisgard KM, Folsum AR. Response to mail surveys: Effect ofa request to explain refusal to participate. Epidemiology 1993;4:480–2.
34. Asch AA, Christakis NA. Different response rates in a trial of twoenvelope styles in mail survey research. Epidemiology 1994;5:364–5.
35. Dillman D. Mail and Telephone Surveys: The Total Design Method.John Wiley & Sons, New York, 1978.
36. Christensen AH, Logan RP, Noach LA, et al. Do clinicians accept the
560 BREUERet al. AJG – Vol. 93, No. 4, 1998

role of Helicobacter pylori in duodenal ulcer disease: A survey ofEuropean gastroenterologists and general practitioners. J Intern Med1994;236:501–5.
37. Babbs C.H. pylori-associated gastroduodenal disease: Survey of Brit-ish physicians’ views. Gut 1995;37(suppl 1):347.
38. Breuer T, Sudhop T, Goodman KJ, et al. How do practicing cliniciansmanageHelicobacter pylori-related gastrointestinal diseases in Ger-many? A survey of gastroenterologists and family practitioners. Hel-icobacter 1998;1:1–8.
39. Fendrick AM, Hirth RA, Chernew ME. Differences between generalistand specialist physicians regardingHelicobacter pylori and pepticulcer disease. Am J Gastroenterol 1996;91:1544–8.
40. Labenz J, Gyenes E, Ruhl GH, et al. Amoxicillin plus omeprazoleversus triple therapy for eradication ofHelicobacter pyloriin duodenalulcer disease: A prospective, randomized, and controlled study. Gut1993;34:1167–70.
41. Labenz J, Gyenes E, Ru¨hl GH, et al. Omeprazole plus amoxicillin:Efficacy of various treatment regimens to eradicateHelicobacter py-lori . Am J Gastroenterol 1993;88:491–5.
42. Bayerdo¨rffer E, Mannes GA, Sommer A, et al. High dose omeprazoletreatment combined with amoxicillin eradicatesHelicobacter pylori.Eur J Gastroenterol Hepatol 1992;4:697–702.
43. Graham KS, Malaty H, el-Zimaity HM, et al. Variability with ome-prazole-amoxicillin combinations for treatment ofHelicobacter pyloriinfection. Am J Gastroenterol 1995;90:1415–8.
44. van der Hulst RW, Weel JF, Verheul SB, et al. Treatment ofHelico-bacter pylori infection with low or high dose omeprazole combinedwith amoxycillin and the effect of early retreatment. Aliment Pharma-col Ther 1996;10:165–71.
45. Gisbert JP, Mur M, Sainz S, et al. Is the omeprazole and amoxicillincombination useful in the treatment eradicatingHelicobacter pyloriinSpain? Rev Esp Enferm Dig 1996;88:99–106.
AJG – April 1998 CLINICAL MANAGEMENT OF H. PYLORI-RELATED DISEASES 561






