Embed Size (px)
Citation preview

18 AAOSNow December2010 ClinicalNewsandViews ClinicalNewsandViews December2010 AAOSNow 19
Howdowetreatwristfracturesintheelderly?
Distalradiusfracture(DRF)pre-dominantlyaffectstheelderlypopulation,withsome80,000fracturessustainedperyear,cost-ingtheU.S.healthcaresystemanestimated$632million.Thesefractureshavetraditionallybeentreatedwithcasting,aconservativeandrelativelyinexpensivetreat-ment.Buttheuseofinternalfixa-tioninelderlypatientsisgrowing,accordingtotheresultsofastudypresentedatthe2010annualmeet-ingoftheAmericanSocietyforSurgeryoftheHand.
Thestudy,presentedbyKevinC.Chung,MD,MS,identified85,924patientsaged65yearsor
olderwhohadreceivedtreatmentwithin2weeksofDRFdiagnosis.Although74percentofpatientsweretreatedwithcasting,17per-centunderwentinternalfixation,7.6percentreceivedpercutaneouspinning,and1.3percentreceivedexternalfixation.Internalfixa-tionhadthehighestrateof90-daymajorcomplications—nearly6percentofcases.
Incomparingpatientdemo-graphics,theresearchersfoundthefollowingsignificantdifferences:•Menwerelesslikelythan
womentoreceiveinternalfixa-tionversusclosedtreatment.
•Menweremorelikelythanwomentoreceiveinternalfixa-tionversuspinningorexternalfixation.
•AfricanAmericanpatientswerelesslikelythanCaucasianpa-tientstoreceiveinternalfixationversusclosedtreatment.Theauthorsattributethese
differencestothereducedriskofosteoporosisinmenandAfricanAmericans.
Comparedtoyoungerpatients,olderpatientswerelesslikelytoreceiveinternalfixationversusothertreatments.Patientswithhighersocioeconomicstatus(SES)weremorelikelytoreceiveinternalfixationversuspinningorexternalfixationthanthoseinthelowestSESgroup.Patientswithcomorbidconditionswerelesslikelythanpatientswithoutcomorbiditiestoreceiveinternalfixationversuspin-
ningorexternalfixation.Handsurgeonsperformedinter-
nalfixationonethirdofthetime,comparedtoorthopaedicsurgeons,whogenerallyusedclosedtreat-ment(71.8percent).Thedifferencecouldbeexplainedbyseverityoffractureandlikelihoodofreferraltoaspecialist,aswellasbyahigh-erawarenessamongspecialistsofnewertechniquesandimplants—specifically,thevolarlockingplat-ingsystemforDRF.
Theuseofinternalfixationfor
DRFintheMedicarepopulationhasbeengrowing,from3percentofcasesin1996to16percentin2005,andislikelytocontinue,notetheauthors.Theyconcludedbycallingforarandomizedmulti-centerclinicaltrialtodeterminewhetherornotthemoneyiswellspent. NOW
CoauthorsincludeMelissaJ.Shauver,MPH;HuiyingYin,MA;andJohnD.Birkmeyer,MD.Theauthorsreportnoconflicts.
0%
10%
20%
30%
40%
50%
60%
70%
80%
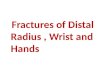
Treatment Received by Patient Age Group
Open Treatment Pinning External Fixation Closed Treatment
65–69 70–74 75–79 80+
Fig 1AbreakdownoftreatmentsprovidedtoMedicarebeneficiariesinvariousagegroupswhohavedistalradiusfracturesshowsthatclosedtreatmentisstillthemostpopulartreatmentmode.
Morecomplicationswithsingle-incisionrepair
Patientstreatedwithdouble-incisionrepairusingtransosseousdrillholesforacutedistalbicepsrupturemayseefewercompli-cationsthanthosetreatedwithsingle-incisionrepairusingsutureanchors,accordingtotheresultsofaprospective,randomizedclinicaltrialpresentedbyRuby Grewal, MD, MSc,FRCSC, atthe2010ASSHannualmeeting.
Theresearchersrandomized90malepatientstoreceiveeithersingle-incisionrepair(n=48)ordouble-incisionrepair(n=42).Thetwogroupshadnosignificant
differencesinpatientage,domi-nanthand,ornumberofworkerscompensationcases.OverallmeanAmericanShoulderandElbowSocietypainscoresweresimilarinbothgroupsatallfollow-uppoints(3,6,12,and24months).
At24months,nosignificantdifferenceswerefoundbetweenthetreatmentgroupsinfinalex-tension,pronation,orsupination.Theresearchteamnotedamar-ginaladvantageinmeanisometricflexionstrengthregainedamongparticipantsinthedouble-incisiongroup(double:104percent;single:94percent;p=0.01).
Overall,19of48patientsinthesingle-incisiongrouphadcompli-cations,comparedto3of42inthedouble-incisiongroup(p<0.01)—primarilyduetoahighnumberofearlytransientneuropraxiasinthe
single-incisiongroup.Threeneuro-praxiasinthesingle-incisiongroupremainedsymptomaticafter6months.Theresearchersnotedfourtendonruptures,allofwhichwereduetononcomplianceorreinjuryintheearlypostoperativeperiod.Noneoftheruptureswasrelatedtofixationtechnique.NOW
Dr.Grewal’scoauthorsincludeGeorge S. Athwal MD, FRCSC;JoyC.McDermid,BScPT,MSc,PhD;Kenneth J. Faber, MD, FRCSC;Darren S. Drosdowech, MD, FRCSC;Graham J.W. King, MD, MSc, FRCSC.
Disclosureinformation—Drs.GrewalandMcDermid—nocon-flicts;Dr.Athwal—WrightMedi-calTechnologies,Arthrosurface,ConMedLinvatec,Tornier,Arthrex;
Dr.Faber—TenetMedical,Zimmer;Dr.Drosdowech—DePuy;Dr.King—WrightMedicalTechnol-ogy,Inc.;Tornier;TenetMedical.
BottomlineNooveralldifferencesinfunctionaloutcomeswerefoundbetweendistalbicepsrupturestreatedwitheitherasingleordoubleincisionrepairtechnique;howeverflexionstrengthwasslightlygreaterwithatwo-incisiontechnique.
•Thesingle-incisiongrouphadagreaterincidenceofcomplications.
ASSH 2010AnnuAl Meeting
ASSH 2010AnnuAl Meeting
Bottomline•Despitetheincreasing
useofinternalfixationtechniques,mostelderlypatientswithdistalradiusfracturesarestilltreatedwithclosedtreatment.
•Demographicfactors,suchaspatientgender,raceandage,haveasignificanteffectonthetypeoftreatmentreceived.
Cou
rtes
yof
Kev
inC
.Chu
ng,M
D,M
S
AAOS Now_December 2010.indd 18 11/23/2010 4:14:34 PM