Embed Size (px)
Citation preview
How do you approach a patient you think may have a
PE?
04/18/23 2
Case 1
• 42 yo female presents to ED with complaint of 3 weeks of congestion and several days of difficulty catching her breath
• No significant PMH, meds, non-smoker, no recent immobility or surgeries
• T 37.9, P 82, RR 20, room air sats 98%– Sinus tenderness, boggy turbinates, red throat– Lungs clear and no respiratory distress– CXR clear– Spiral CT reveals left lower lobe sub-segmental defect
How good is a CTA (-CTV) to rule in or out a PE?
04/18/23 3
PIOPED II – NEJM, 2006
• Prospective cohort study• Consecutive inpatient and outpatients
with suspected acute pulmonary embolism
• Composite reference standard– Clinical assessment, VQ scanning, CUS, if
necessary DSA
• CTA-CTV – stringent standards
04/18/23 4
PIOPED II – NEJM, 2006
• No PE– Normal DSA– Normal VQ scan– Low or very low prob VQ scan, low prob
Wells, normal CUS– PLUS telephone interviews at 3 and 6 months
• PE– High Prob VQ scan– Abnormal DSA– Abnormal CUS
04/18/23 5
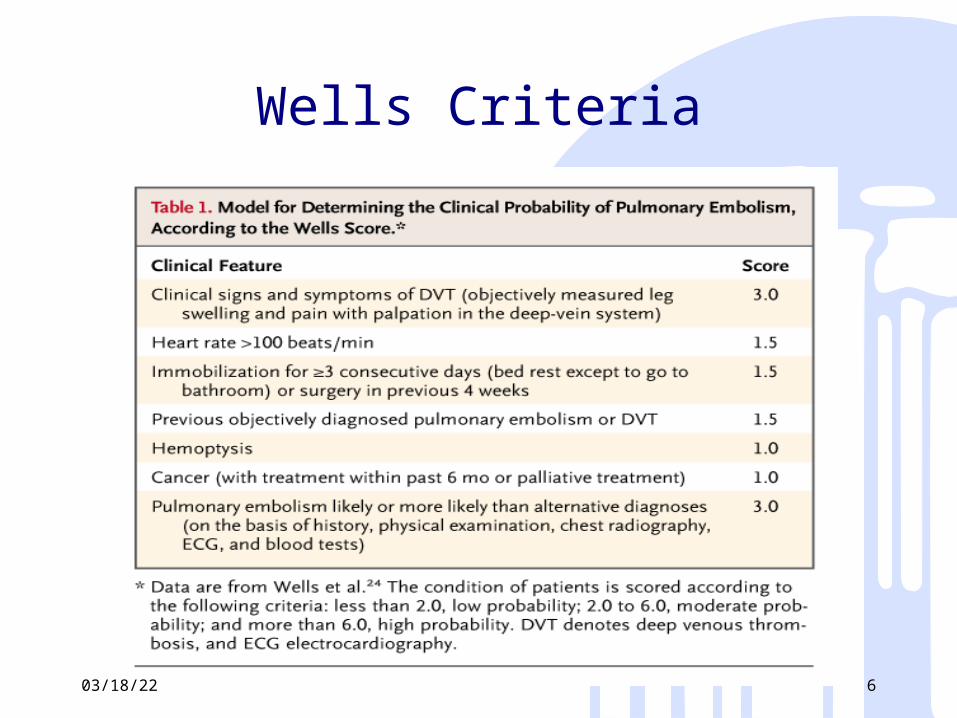
Wells Criteria
04/18/23 6
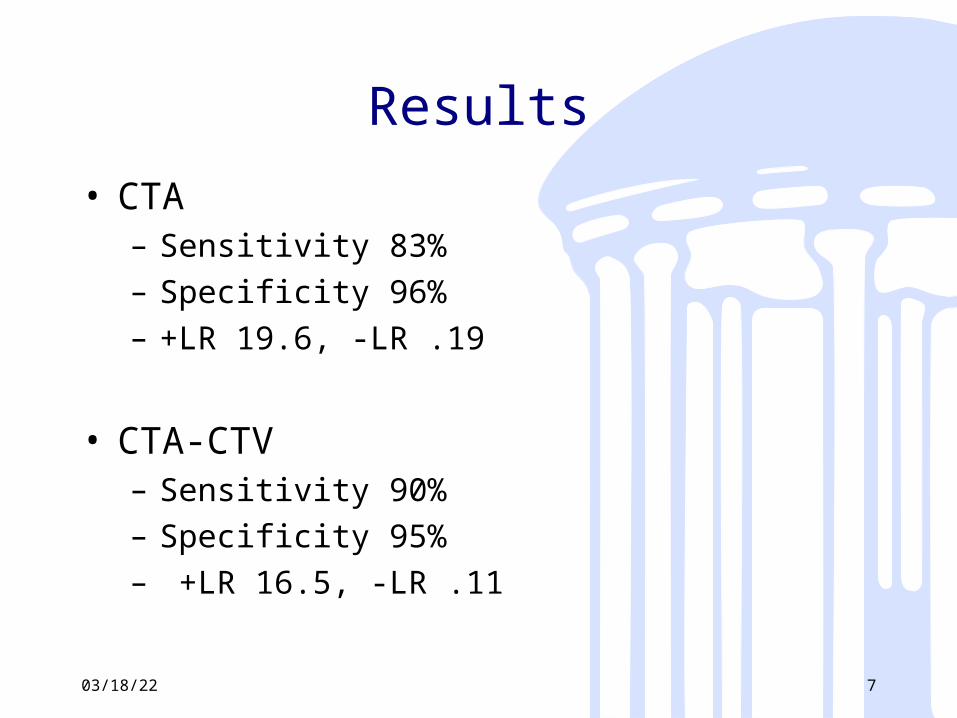
Results
• CTA– Sensitivity 83%– Specificity 96%– +LR 19.6, -LR .19
• CTA-CTV– Sensitivity 90%– Specificity 95%– +LR 16.5, -LR .11
04/18/23 7
Problems
• Exclusions and dropouts– “inconclusive results”
• 6% for CTA• 11% for CTV
– Of 1090 enrolled, 238 did not receive reference diagnosis
• This represents best case scenario
04/18/23 8
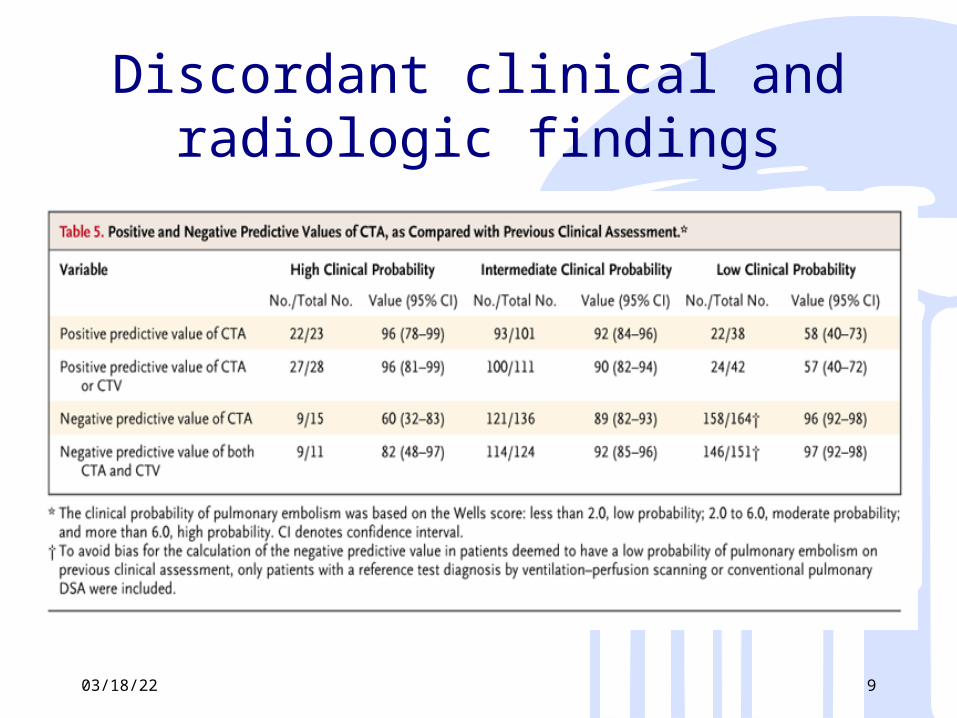
Discordant clinical and radiologic findings
04/18/23 9
04/18/23 10
Christopher study – JAMA 2006
• Prospective cohort study of a sequential application of a clinical decision rule, D-Dimer testing, and CTA
• Consecutive patients – sudden onset dyspnea, sudden deterioration of existing dyspnea, or sudden pleuritic chest pain– ED and wards
• A modified Wells assessment, An elisa ddimer test, and Multirow detector CT scan
• 3 month follow up04/18/23 11
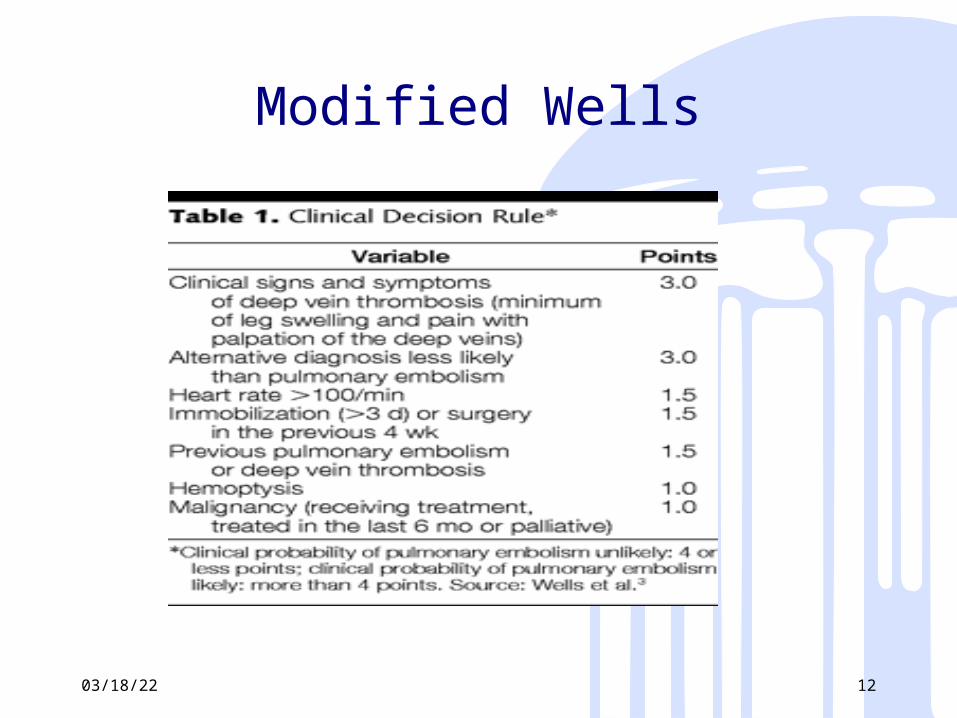
Modified Wells
04/18/23 12
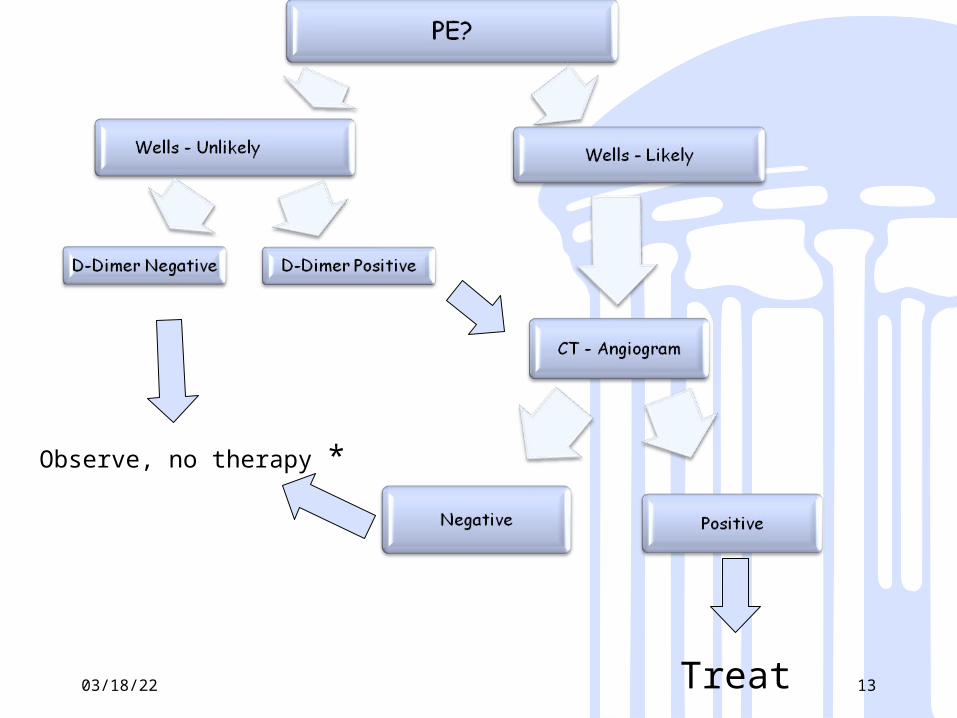
04/18/23 13Treat
Observe, no therapy *
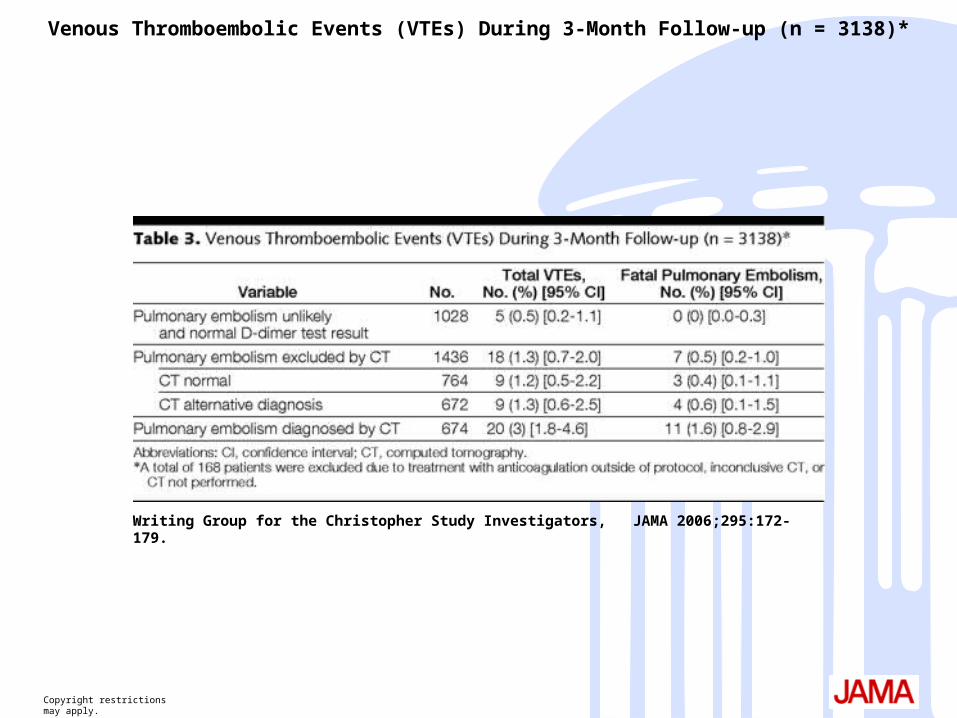
Copyright restrictions may apply.
Writing Group for the Christopher Study Investigators, JAMA 2006;295:172-179.
Venous Thromboembolic Events (VTEs) During 3-Month Follow-up (n = 3138)*
Summary
• Safety with concordant findings– Low PTP/normal D-Dimer/negative CTA
• Consider going further if discordant findings
04/18/23 15
04/18/23 16
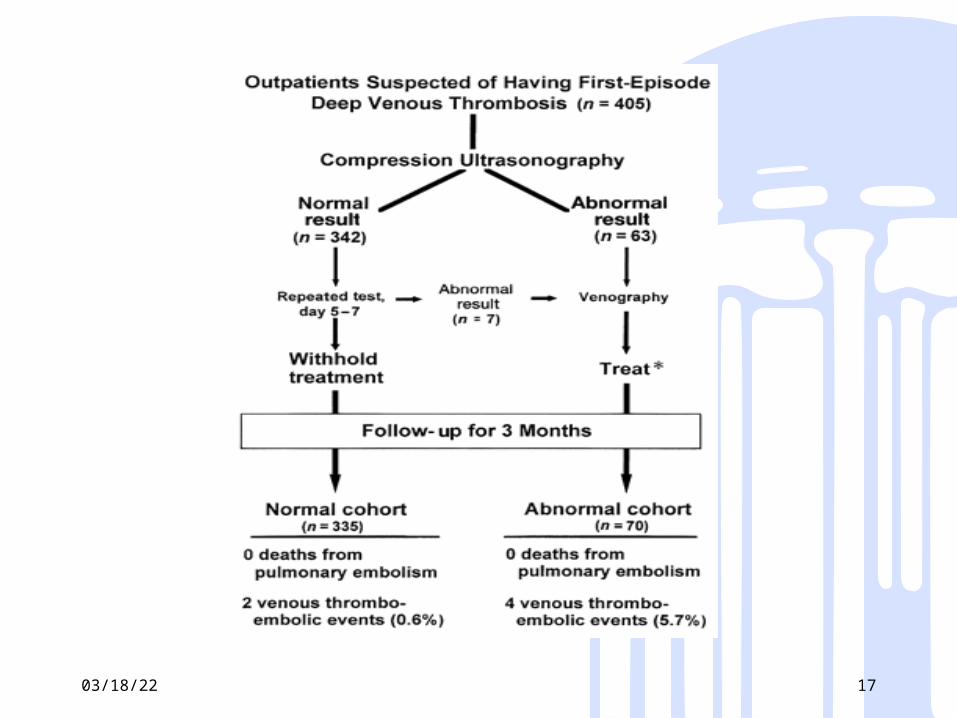
Lower Extremity Ultrasound
• Annals of Internal Medicine 01/98• Cohort study of consecutive patients
presenting to referral center with suspected DVT
• All underwent CUS initially and if normal again in 5-7 days
• All followed for 3 months
04/18/23 17
Prevention
04/18/23 18
04/18/23 19
Limitations of the literature
• DVT screening methods– Venography – 20-40% nondiagnostic, clinical
relevance of small thrombi– DUS – poor accuracy for calf veins, operator
dependent
• End points– Mortality > fatal PE > PE > Symptomatic
DVT > Asymptomatic DVT
• Industry sponsorship
04/18/23 20
Risk Factors• Increasing age (>50)• Malignancy – history, active, under therapy• Medications
– OCPs, HRT, SERM, Erythropoiesis stimulating compounds
• Medical condition– IBD, Nephrotic syndrome, history of MI, atrial
fibrillation, ischemic stroke, diabetes mellitus, obesity, CHF, paralysis, previous VTE, varicosities
• Thrombophilia– FVL, Prothrombin gene mutation, Protein C, S,
ATIII deficiencies
04/18/23 21
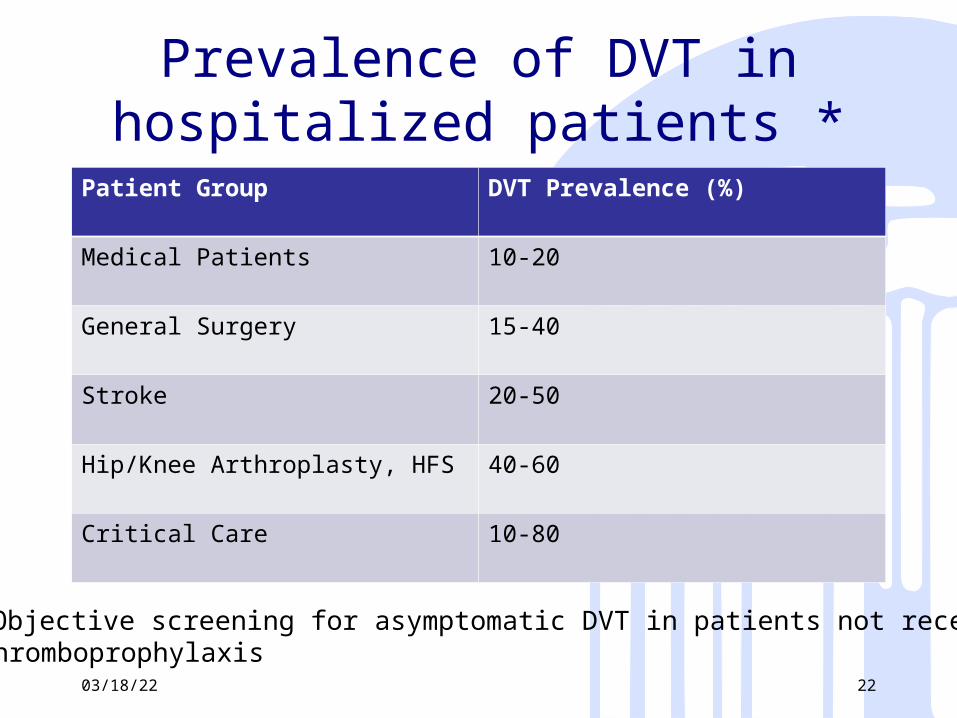
Prevalence of DVT in hospitalized patients *
Patient Group DVT Prevalence (%)
Medical Patients 10-20
General Surgery 15-40
Stroke 20-50
Hip/Knee Arthroplasty, HFS 40-60
Critical Care 10-80
04/18/23 22
*Objective screening for asymptomatic DVT in patients not receiving thromboprophylaxis
Medical Patients• Pharmacologic Thromboprophylaxis
(LMWH, LDUH, fondaparinux) recommended for…
acutely ill hospitalized patients with CHF, severe respiratory disease or confined to bed
PLUSone or more additional risk factors such as
– Active cancer– Previous VTE– Sepsis– Acute neurologic disease– IBD04/18/23 23
Meta-analysis• Annals of Internal Medicine, February,
2007• Anticoagulant prophylaxis to prevent
symptomatic venous thromboembolism in hospitalized medical patients
• “Individual randomized trials of anticoagulant prophylaxis in medical patients have been underpowered to show a reduction in PE and have assessed treatment effects on asymptomatic, venography-detected DVT, which is a less compelling outcome.”
04/18/23 24
Meta-analysis• Well designed and described search
strategy• Two independent reviewers• Treatment efficacy outcomes
– All-cause mortality, fatal and non-fatal symptomatic PE, symptomatic DVT
• On-treatment period• Anticoagulant Regimens
– LDUH 5000IU bid/tid, Enoxaparin 40-60mg daily or 30mg bid, Nadroparin 4000/6000 IU daily, Dalteparin 5000IU daily or Fondaparinux 2.5mg daily
04/18/23 25
Dentali, F. et. al. Ann Intern Med 2007;146:278-288
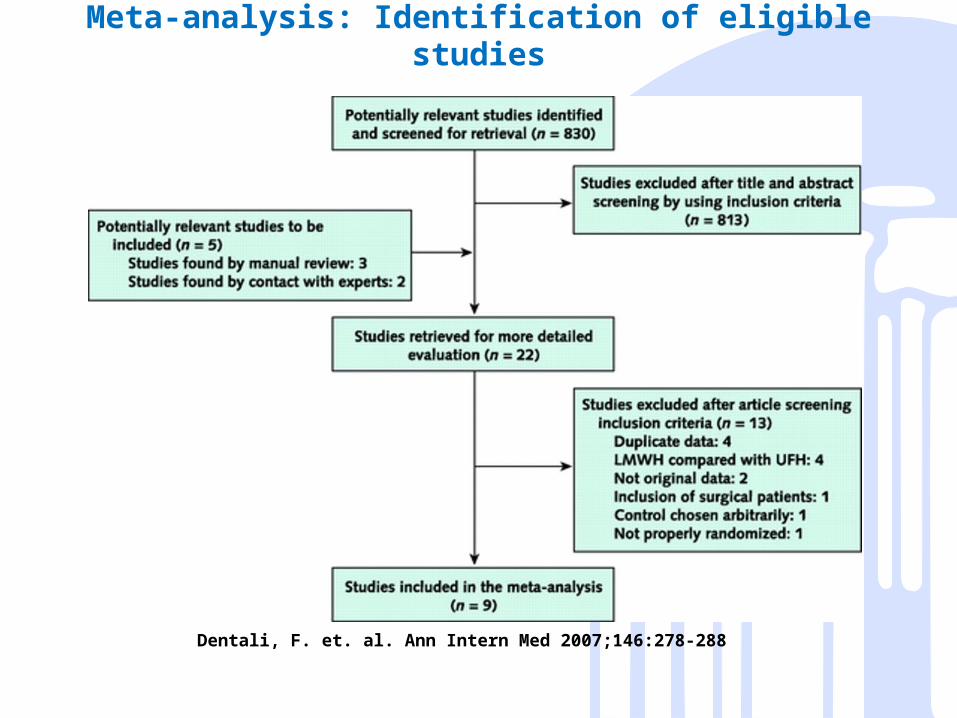
Meta-analysis: Identification of eligible studies
Dentali, F. et. al. Ann Intern Med 2007;146:278-288
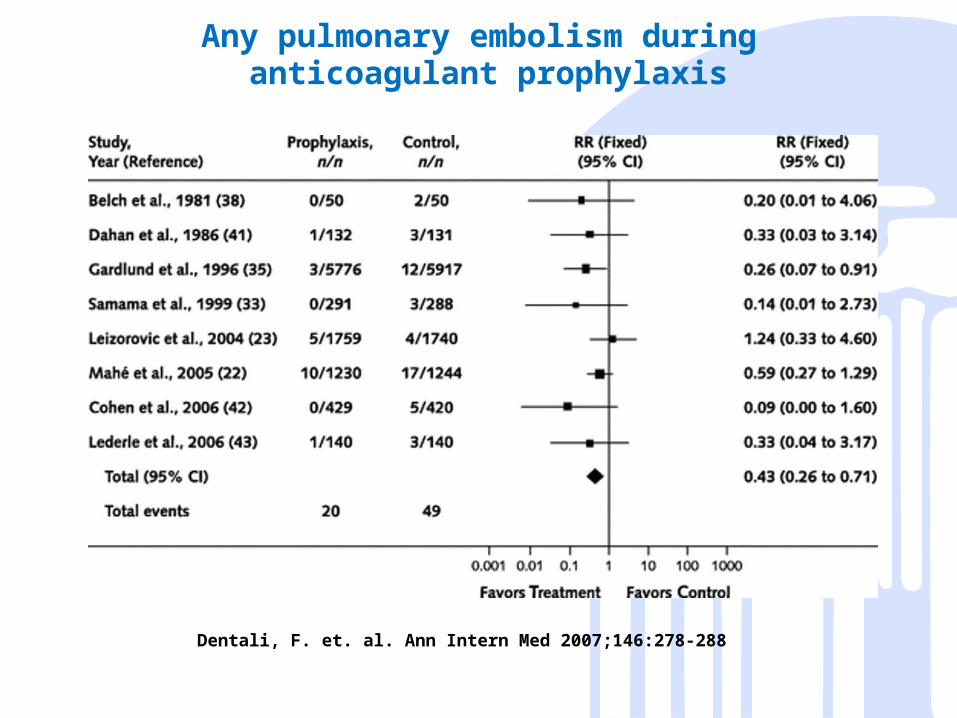
Any pulmonary embolism during anticoagulant prophylaxis
Dentali, F. et. al. Ann Intern Med 2007;146:278-288
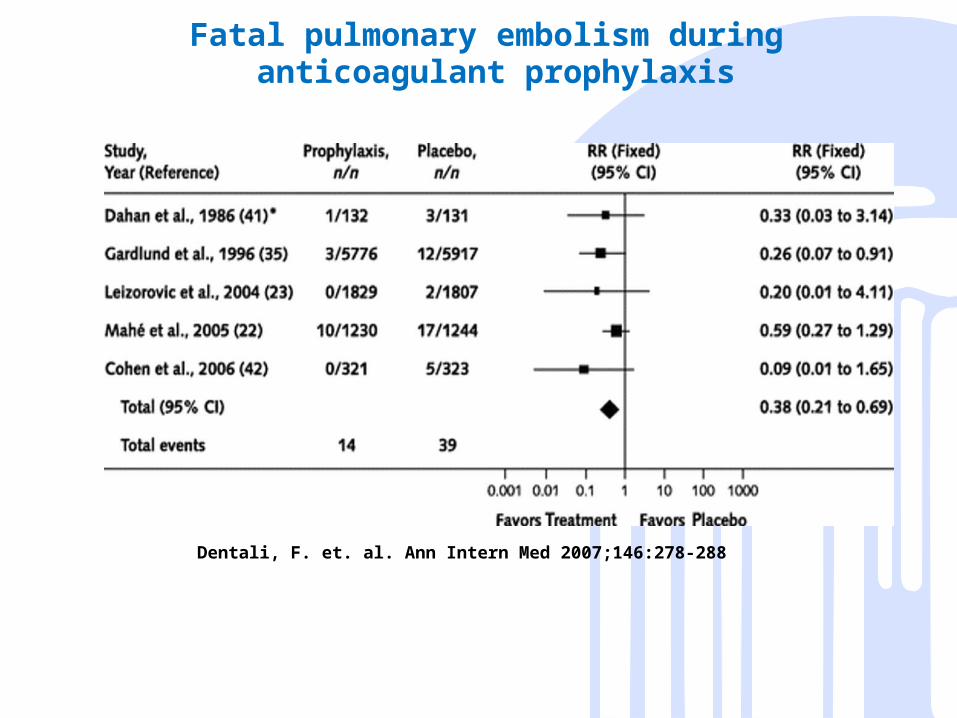
Fatal pulmonary embolism during anticoagulant prophylaxis
Dentali, F. et. al. Ann Intern Med 2007;146:278-288
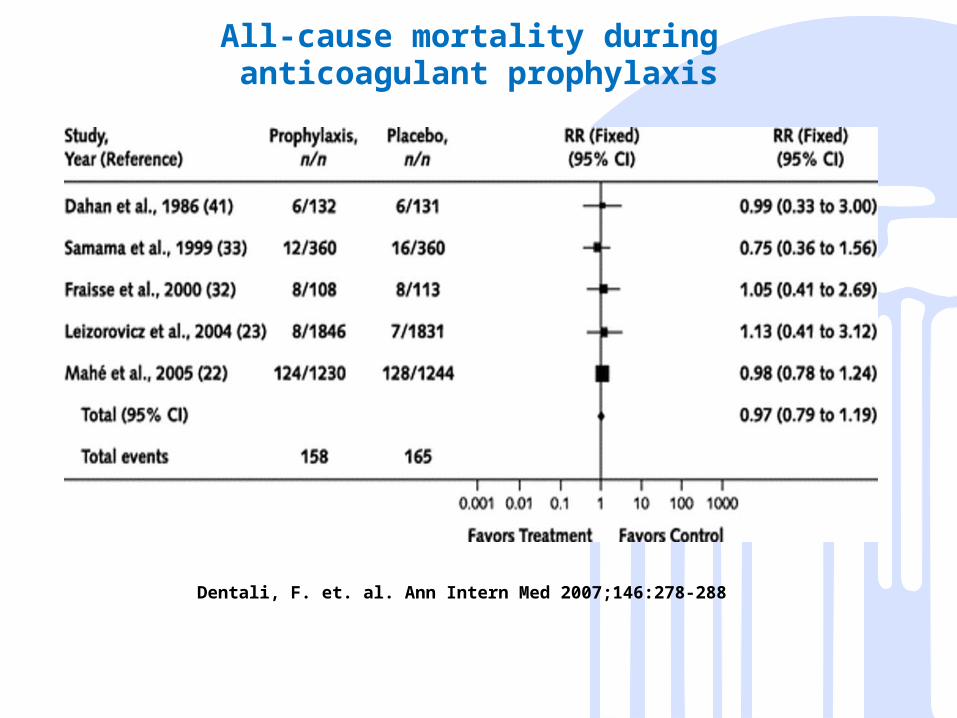
All-cause mortality during anticoagulant prophylaxis
Dentali, F. et. al. Ann Intern Med 2007;146:278-288
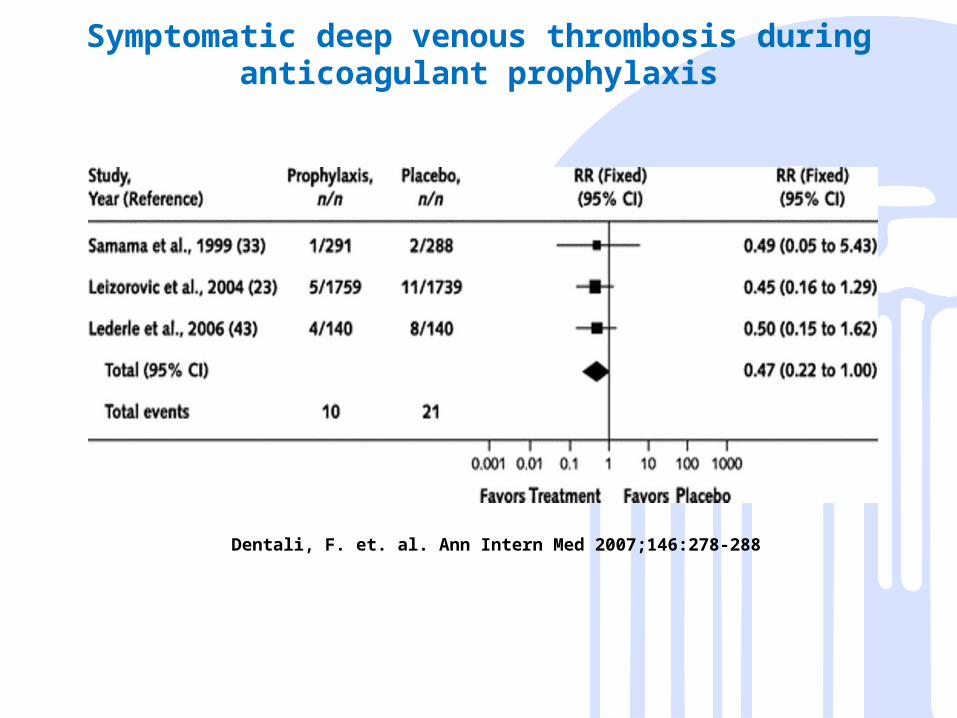
Symptomatic deep venous thrombosis during anticoagulant prophylaxis
Dentali, F. et. al. Ann Intern Med 2007;146:278-288
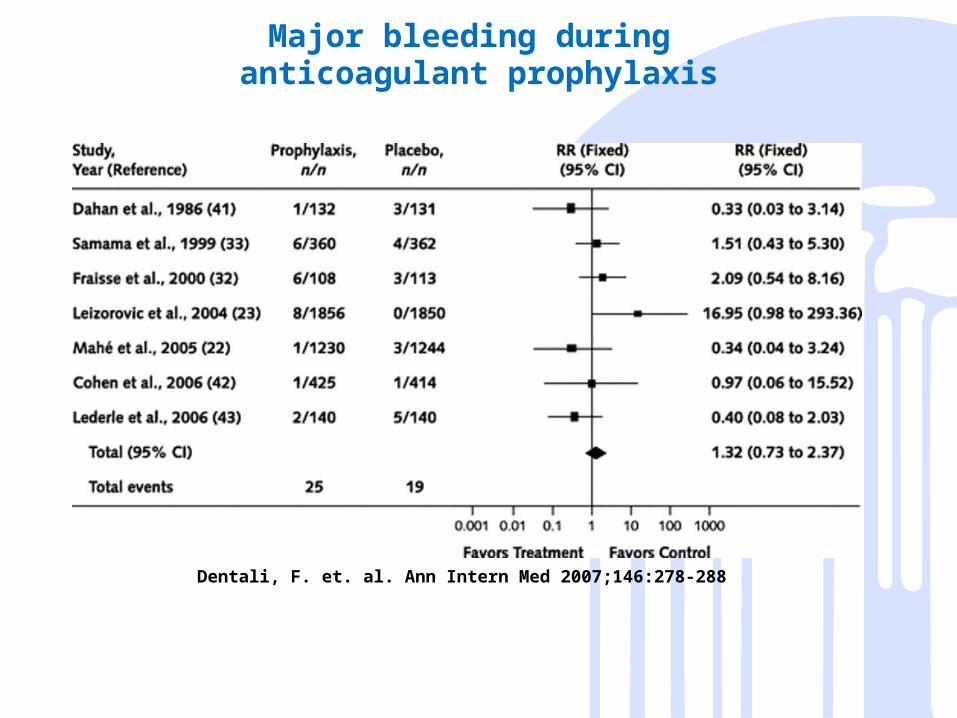
Major bleeding during anticoagulant prophylaxis
Limitations
• Not all studies were double blind– Diagnostic suspicion bias
• Best agent?– No head to head comparisons in this study
• Lack of standardized definition for major bleeding
• Pharmaceutical support
04/18/23 32
04/18/23 33
Summary
• Those at highest risk receive greatest benefit from an intervention– Risk stratify surgical and medical
patients (Joint Commission Requirement)
– Provide anticoagulant prophylaxis to moderate and high risk surgical patients
– Provide anticoagulant prophylaxis to most** hospitalized medical patients
04/18/23 34