Embed Size (px)
Citation preview
How I do it/short communication: the middle temporal artery fl ap for coverage of an exposed cochlear implant cable in the mastoid cavity
MARK CRAIG, JEREMY LAVY, Royal National Throat, Nose and Ear Hospital, Gray’s Inn Road, London WC1X 8DA, UK
ABSTRACT A patient who had previously undergone a modifi ed radical mastoidectomy subsequently underwent cochlear implantation with good results. At surgery the mastoid cavity was partially obliterated to provide soft tissue cover for the implant cables. Follow-ing local infection the cable became exposed and we used a middle temporal artery local fl ap to provide cover for the cable. The anatomy of the fl ap and methods used are described here. The patient continues to have good hearing from the implant with a good coverage over the cable. Copyright © 2006 John Wiley & Sons, Ltd.
Keywords: cochlear implant; middle temporal artery; fl ap
Introduction
The middle temporal artery fl ap has previously been described for use in primary and revision mastoid surgery (Black and Kelly, 1994; Fagan and Rodrigues, 2004; O’Sullivan and Atlas, 2004). Here we describe its use for the fi rst time in associa-tion with a cochlear implant.
History
A 58-year-old lady who had previously undergone a left modifi ed radical mastoid-ectomy subsequently underwent cochlear implantation on the same side. At surgery the mastoid cavity was partially obliterated with abdominal fat to provide suffi cient soft tissue cover for the implant cables. For fi ve years the ear was trouble free and she achieved good use of her implant, with CUNY sentences scores improving from 9% pre-operatively to 99% at three months post-surgery. However, she sub-sequently developed a persisting infection of the cavity. This was successfully treated with topical and systemic antibiotics but, at resolution of the infection, it
Cochlear Implants InternationalCochlear Implants Int. 7(4), 214–218, 2006Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/cii.322
214
Cochlear Implants Int. 7(4), 214–218, 2006Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/cii
How I do it/short communication 215
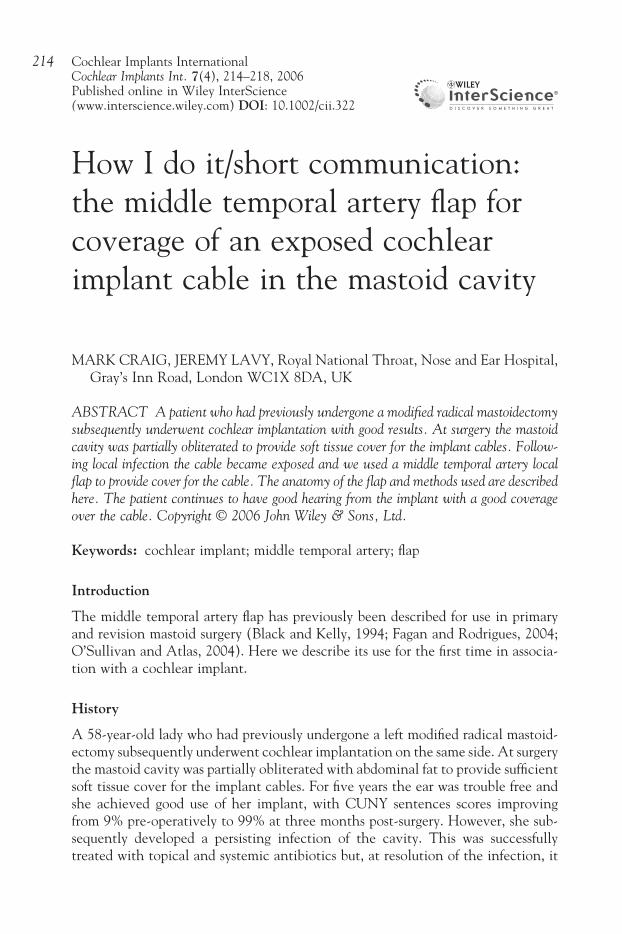
was found that part of the cable from the implant package to the electrode array was exposed in the base of the cavity (Figure 1).
The middle temporal artery fl ap
This was fi rst described by Black and Kelly (1994) for a method of revascularization of the reconstructed external auditory canal wall in patients with troublesome mastoid cavities. Fagan and Rodrigues (2004) described its use for relining the superior aspect of the mastoid cavity in modifi ed radical mastoidectomy to facilitate epithelialization, especially in large cavities. It was further used by O’Sullivan and Atlas (2004) for mastoid cavity obliteration in conjunction with the musculoperi-osteal fl ap from post-auricular muscle.
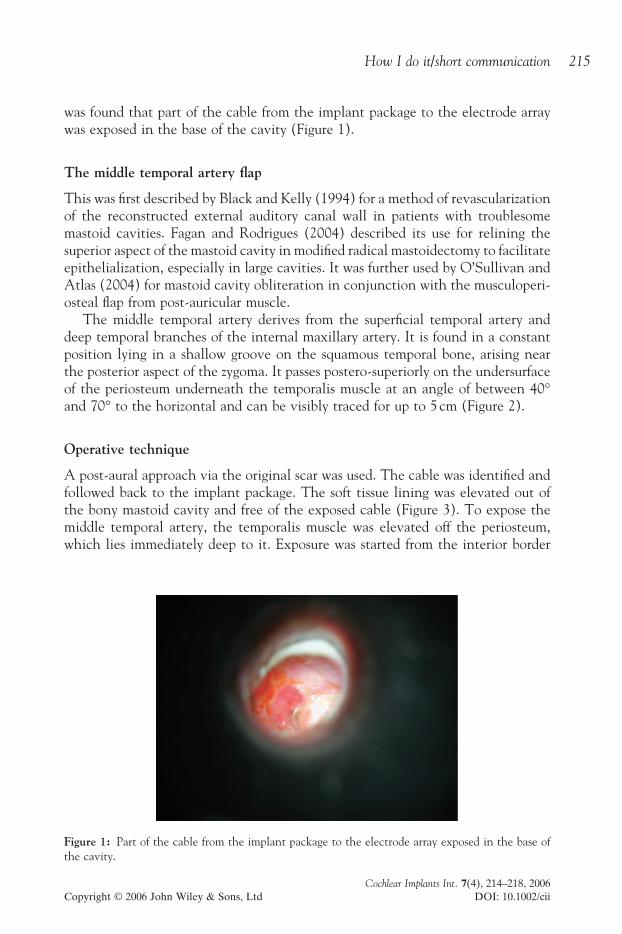
The middle temporal artery derives from the superfi cial temporal artery and deep temporal branches of the internal maxillary artery. It is found in a constant position lying in a shallow groove on the squamous temporal bone, arising near the posterior aspect of the zygoma. It passes postero-superiorly on the undersurface of the periosteum underneath the temporalis muscle at an angle of between 40° and 70° to the horizontal and can be visibly traced for up to 5 cm (Figure 2).
Operative technique
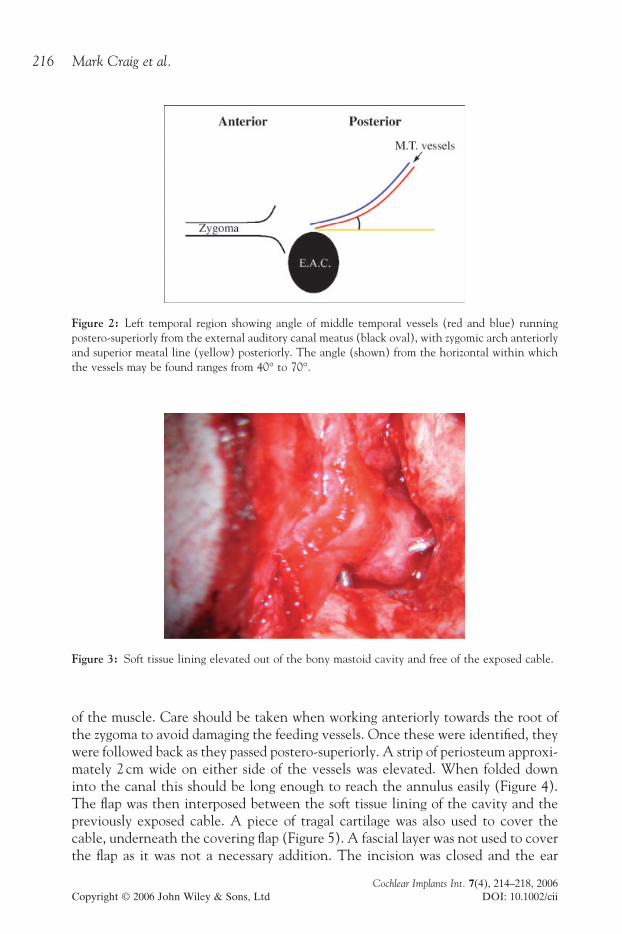
A post-aural approach via the original scar was used. The cable was identifi ed and followed back to the implant package. The soft tissue lining was elevated out of the bony mastoid cavity and free of the exposed cable (Figure 3). To expose the middle temporal artery, the temporalis muscle was elevated off the periosteum, which lies immediately deep to it. Exposure was started from the interior border
Figure 1: Part of the cable from the implant package to the electrode array exposed in the base of the cavity.
Cochlear Implants Int. 7(4), 214–218, 2006Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/cii
Mark Craig et al.216
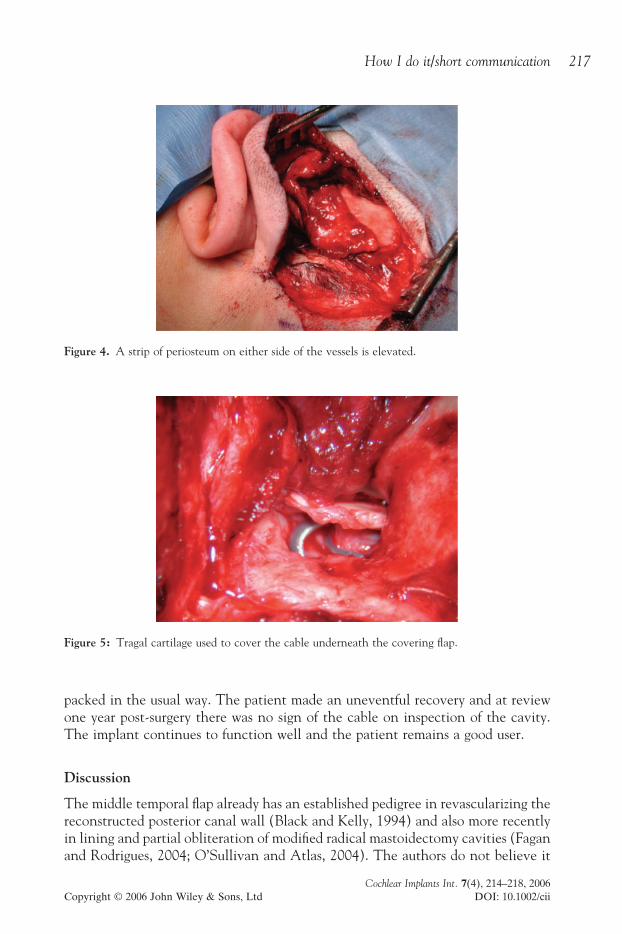
of the muscle. Care should be taken when working anteriorly towards the root of the zygoma to avoid damaging the feeding vessels. Once these were identifi ed, they were followed back as they passed postero-superiorly. A strip of periosteum approxi-mately 2 cm wide on either side of the vessels was elevated. When folded down into the canal this should be long enough to reach the annulus easily (Figure 4). The fl ap was then interposed between the soft tissue lining of the cavity and the previously exposed cable. A piece of tragal cartilage was also used to cover the cable, underneath the covering fl ap (Figure 5). A fascial layer was not used to cover the fl ap as it was not a necessary addition. The incision was closed and the ear
Figure 2: Left temporal region showing angle of middle temporal vessels (red and blue) running postero-superiorly from the external auditory canal meatus (black oval), with zygomic arch anteriorly and superior meatal line (yellow) posteriorly. The angle (shown) from the horizontal within which the vessels may be found ranges from 40° to 70°.
Figure 3: Soft tissue lining elevated out of the bony mastoid cavity and free of the exposed cable.
Cochlear Implants Int. 7(4), 214–218, 2006Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/cii
How I do it/short communication 217
packed in the usual way. The patient made an uneventful recovery and at review one year post-surgery there was no sign of the cable on inspection of the cavity. The implant continues to function well and the patient remains a good user.
Discussion
The middle temporal fl ap already has an established pedigree in revascularizing the reconstructed posterior canal wall (Black and Kelly, 1994) and also more recently in lining and partial obliteration of modifi ed radical mastoidectomy cavities (Fagan and Rodrigues, 2004; O’Sullivan and Atlas, 2004). The authors do not believe it
Figure 4. A strip of periosteum on either side of the vessels is elevated.
Figure 5: Tragal cartilage used to cover the cable underneath the covering fl ap.

Cochlear Implants Int. 7(4), 214–218, 2006Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/cii
Mark Craig et al.218
has ever been described in association with cochlear implant surgery. Cochlear implantation in pre-existing modifi ed radical mastoidectomy cavities presents the surgeon with additional diffi culties relating to soft tissue cover from the implant cable. We believe that the middle temporal fl ap is ideally suited to this purpose and although used here in response to a late complication developing in a previ-ously implanted ear, it could also be used in a primary case to provide additional cover.
The features of the middle temporal fl ap that make it particularly useful are: its thickness; the length of fl ap available, so that it can be made long enough to cover a deep cavity and reach the annulus; its robustness, with less chance of atrophy or necrosis because of the local axial supply, which is also less liable to kinking or stretching; the relative ease of raising the fl ap, with vessels which are visible to the naked eye and constant in position; also, the fl ap is rarely damaged by previous surgery using a post-aural incision.
Other techniques for dealing with this problem include the obliteration of the cavity with abdominal fat and closure of the ear canal by the eversion of canal skin (Gray and Irving, 1995). In comparison, our method takes less time and requires no abdominal incision, and provides an alternative surgical option.
Summary
• The middle temporal artery fl ap (MTA) has been not been previously described in association with cochlear implantation.
• It may provide soft-tissue cover of the implant cable in patients with a pre-existing modifi ed radical mastoidectomy cavity at the initial time of surgery, or in those patients where the cable becomes exposed subsequently.
• The fl ap is robust, thick, easily raised and long enough to reach the annulus.
References
Black B, Kelly S (1994) Mastoidectomy reconstruction: revascularising the canal wall repair. American Journal of Otology 15: 91–5.
Fagan PA, Rodrigues SJ (2004) Technical note: Middle temporal artery fl ap in mastoid surgery. Otology and Neurotology 25: 242–4.
Gray RF, Irving RM (1995) Cochlear implants in chronic suppurative otitis media. American Journal of Otology 16(5): 682–6.
O’Sullivan PG, Atlas MD (2004) How I do it: use of soft tissue vascular fl aps for mastoid cavity obliteration. Laryngoscope 114: 957–9.
Address correspondence to: Mr M Craig, 56 Gerry Raffl es Square, Stratford, London E15 1BG, UK. Tel: (+44) (07968) 213 843. Email: [email protected].