Embed Size (px)
Citation preview

©ORUEN LTDCNS 2019: 5:(1). JULY 2019 34
Introduction: Keeping pace with advances in anticoagulationMore than 30 million people globally are estimated to have
atrial fibrillation.1 The presentation of data with dabigatran
in 2009 in the Evaluation of Long Term Anticoagulant
Therapy (RE-LY) study introduced the modern era of stroke
prevention in patients with AF using direct oral anticoagulant
agents. Approval of dabigatran was achieved in 2010 in
the US and in 2011 in Europe, and since then other novel
oral anticoagulant agents (NOACs) have been approved,
including rivaroxaban, apixaban, and edoxaban.2-5 The 2015
approval of idarucizumab for dabigatran specific reversal
is another landmark development in the NOAC field, as is
the recent approval for andexanet–alpha as a reversal agent
for factor Xa-inhibitors. NOACs address many of the limita-
tions associated with using vitamin K antagonists, including
the narrow therapeutic window and the need for frequent
monitoring with warfarin; warfarin’s slow onset and offset
of action, its variability in dose response; and the increased
risk of intracranial hemorrhage (ICH) with warfarin.4-9
However, clinical practice challenges persist. Registries and
observational data consistently show that NOAC therapy is
underused in eligible patients and in some countries aspirin
is still used in patients who are eligible for OAC therapy.
In addition, reduced NOAC doses are sometimes used in
clinical practice in patient populations that were not tested
in clinical trials.10-13 In addition, in emergency situations
when anticoagulation needs to be removed quickly, it
Received – 16 July 2019; Accepted – 19 July 2019
Abstract The global burden of atrial fibrillation remains high. The approval of several novel oral anticoagulant agents (NOACs) as well as of idarucizumab for dabigatran reversal and andexanet-alpha for factor Xa-inhibitors represent landmark developments in the NOAC field. Although NOACs have also shown a positive net clinical benefit, even in patients with one additional stroke risk factor, clinical practice challenges persist. NOAC therapy is often underused in eligible patients despite clear recommendations in international guidelines. Moreover, it remains challenging to implement appropriate strategies for reversing NOACs in emergency settings. A symposium, How NOAC Selection and Reversal Can Help Protect Our Patients: Your Questions Answered, was held during the 5th European Stroke Organization Conference in May 2019 in Milan, Italy. This symposium reviewed advances in anticoagulation, including: NOAC selection; dosing strategies; evidence concerning anticoagulation reversal strategies; and strategies for using reversal agents before surgery, in patients with intracerebral hemorrhage, and in patients presenting with ischemic stroke prior to thrombolysis.
KEYWORDS: ATRIAL FIBRILLATION; ICH; NOACS; DABIGATRAN; REVERSAL AGENTS; IDARUCIZUMAB
How NOAC Selection and Reversal Can Help Protect Our Patients: Your Questions Answered
Corresponding author: James Coe – [email protected]
Acknowledgements: Manuscript preparation provided by Thistle Editorial, LLC
Disclaimer: The views and opinions expressed in this article are not necessarily endorsed by Oruen Ltd or Thistle Editorial LLC.
NOAC_ESOC.indd 34 26/07/2019 12:33

CNS 2019: 5:(1). JULY 2019 35 ©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
patient populations. This dosing distinction is important.
The 150 mg—and most effective dabigatran dose—the
only NOAC associated with significant reduction in both
all stroke and ischemic stroke. This dose is also associated
with reduction in cardiovascular mortality, comparable major
bleeding, and a dramatic reduction in ICH. As the worst
complication of anticoagulation, this dramatic reduction
in ICH makes NOACs especially appealing to neurolo-
gists. The 110 mg BID dabigatran dose is associated
with ischaemic outcomes that are similar to warfarin, but
significant reductions in both major bleeding and also in
ICH. A post-hoc outcomes analysis of RE-LY according to
the European Union (EU) label, which allows for age-based
dose reduction to 110mg bid, showed reduced major
bleeding, life threatening bleeding, ICH, and mortality but
still significant stroke prevention vs warfarin.17
Both dabigatran doses also have efficacy in the secondary
prevention setting with patients who have had a transient
ischemic attack (TIA) or stroke.18 Bleeding rates in patients
with prior TIA or ischemic stroke also remains a concern.
This patient population is typically older, frail, at risk for
falls, and polypharmacy is a problem; therefore, the safety
of a drug regimen in stroke patients is important. Compared
with warfarin, dabigatran at either dose of 150mg or 110mg,
apixaban, and edoxaban all show significantly improved
safety profiles and a non-significant trend was seen with
rivaroxaban. In general, NOACs have demonstrated greater
safety than warfarin in patients with a previous stroke and
TIA.
remains challenging to implement appropriate strategies for
reversing NOACs.14
A symposium, How NOAC Selection and Reversal Can Help
Protect Our Patients: Your Questions Answered, was held
during the 5th European Stroke Organization Conference in
May 2019 in Milan, Italy. This symposium reviewed advances
in anticoagulation, including: NOAC selection; dosing
strategies; evidence concerning anticoagulation reversal
strategies; in patients with intracerebral hemorrhage, and in
patients presenting with ischemic stroke who may require
thrombolysis.
The evidence for dabigatranNOAC Safety and Efficacy Profiles in Patients with AF
A wealth of results from both randomized controlled trials
(RCTs) and real-world analyses consistently demonstrate
the safety and efficacy profiles of dabigatran in patients
with AF and show improved outcomes for patients with AF
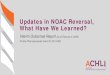
compared with INR-adjusted warfarin. In the pivotal clinical
trials of NOACs, all showed favorable profiles as compared
to warfarin. Notably, all of the NOACs are associated with a
dramatic reduction in ICH (Figure 1).
The RE-LY trial is the only trial to evaluate two independent
fully randomized doses that were subsequently both
approved.2 The ARISTOTLE and ROCKET AF trials for
apixaban and rivaroxaban,15,16 respectively, included a dose
reduction as an addition to the standard dose in pre-defined
Figure 1. Outcomes associated with NOACs
NOAC_ESOC.indd 35 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 36
NOACs in Embolic Stroke of Undetermined Source
In addition to the pivotal clinical trials in AF, other clinical
studies have tested NOACs in the neurology setting.
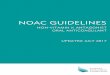
The recently published RE-SPECT ESUS trial compared
dabigatran to aspirin in patients with recent embolic stroke
of undetermined source.19 RE-SPECT ESUS provides the only
comparison for dabigatran with aspirin in stroke patients
that do not have AF. When dosed in keeping with the EU
label, dabigatran had a similar safety profile as aspirin in this
population of stroke patients (Figure 2).
No significant difference was evident in the risk of major
bleeding with dabigatran versus aspirin. Aspirin is generally
considered a benign drug. Although the RE-SPECT ESUS
trial was not comprised of an AF population, the similarity
in major bleeding risk between dabigatran and aspirin
provides reassurance for neurologists as they discuss AF with
their patients.
In contrast to RE-SPECT ESUS, the RE-SPECT CVT trial
involved a very different patient population.20 RE-SPECT
CVT included younger people with sinus thrombosis (a form
of venous thromboembolism) treated with anticoagulation
approximately for six months. Though this trial only enrolled
120 patients, 60 in each group, this is the largest randomized
trial performed so far in this indication. The risk of major
bleeding between dabigatran and warfarin was similar,
though the number of outcome events was small. The risk
of clinically relevant but non-major bleeding was negligible
and the risk for any bleeding was the same in both groups.
The risk of worsening ICH was very low in both groups.
Real world studies provide additional data about how NOACs
are being used in everyday clinical practice. These studies
take their information from sources such as health insurance
databases and are not as robust as clinical trials; however,
such studies have the advantage of being able to include
large number of patients and also potentially those not
included in clinical trial populations. Such studies, provide
considerable evidence for the safety profile of dabigatran
in a wide range of practice settings and consistently
demonstrate that dabigatran has a similar or better safety
profile compared with VKAs in terms of major bleeding; less
major bleeding and ICH compared with rivaroxaban; and
Figure 2. RE-SPECT ESUS Safety Profile19
NOAC_ESOC.indd 36 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 37
Vitamin K
l Specific for VKAs
l Slow acting (4 to 6 hrs even if administered IV)
l Clinically significant variability between patients
l Not a true reversal agent as it does not counter the effects of warfarin, but merely allows production of depleted coagulation factors
(a)PCC, rFVIIa (or FFP)
l Act by repletion of coagulation factors in the blood
l Not approved for NOAC reversal
l Limited clinical data
l Prothrombotic risk
l FFP: can be used for fluid repletion but concerns about large volumes required for coagulation factor supplementation
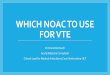
Figure 3. Previous options for OAC reversal8,30
Although vitamin K is available for vitamin K antagonists, it
is slow acting. This agent requires at least 4 to 6 hours, even
if administered intravenously (IV), with total effects occurring
in approximately 24 hours. Vitamin K is associated with
clinically significant variability between patients. Vitamin K
is not considered a true reversal agent as it does not directly
interact with warfarin but counters its effects by allowing
the resumption of the production of vitamin K-dependent
coagulation factors. Activated prothrombin complex
concentrate (aPCC), prothrombin complex concentrate
(PCC), recombinant Factor VII (rFVIIa), and to some extent
frozen fresh plasma (FFP), act by repletion of coagulation
factors in the blood, thereby replacing the depleted vitamin
K-dependent coagulation factors.30 However, these products
are not approved for NOAC reversal, are associated with
prothrombotic risk, and are supported by limited clinical
data. FFP can be used for fluid repletion but concerns have
emerged about the large volumes required for coagulation
factor supplementation.
similar ICH to apixaban.21-26 Analysis of data from the large,
global GLORIA registry of AF patients treated with antico-
agulation also supports the long-term safety of dabigatran
in routine clinical practice.27
While NOACs have been shown to reduce the risk of stroke
in patients with AF, use of these agents does not eliminate
the risk. Thus some AF patients treated with NOACs still
experience stroke due to non-thrombotic related causes,
such as carotid disease, intracranial disease, or small vessel
disease or to uncontrolled hypertension or frequently also
to non-compliance. NOAC failure in many patients is often
associated with suboptimal anticoagulation. Retrospective
analysis of data from the Get with the Guidelines Stroke
Program in the United States (US) found that a majority of
AF patients who have a stroke are not being treated with
any medications, are being treated with aspirin, are not
therapeutic on warfarin, or are underdosed on their novel
anticoagulant.28 The gravitation of clinicians towards lower
NOAC doses may reflect an inherent fear of bleeding;
however, underdosing can harm patients by leading to an
increased risk of stroke. For instance, analysis of Danish
registry data found that compared with warfarin, lower doses
of apixaban and rivaroxaban were associated with similar
rates of ischemic stroke/SE, hemorrhagic stroke, and any
bleeding, but higher risk of death. In contrast, compared
with warfarin, lower-dose dabigatran (110 mg BID), which
was tested as a standalone arm in the randomized RE-LY
trial, was associated with similar rates of ischemic stroke/SE
and death and lower rates of hemorrhagic stroke and any
bleeding.29
EVIDENCE FOR NOAC REVERSAL STRATEGIESCharacteristics of Historically Available Reversal Options
Patients being treated with anticoagulants may experiencing
bleeding for a variety of reasons, such as fractures, trauma,
acute renal failure, that requires an emergency intervention.8
In high-risk AF patients, other reasons for bleeding include
thrombolysis for acute ischemic stroke, intracranial hemorr-
haging, urgent cardiac surgery, and complications of percuta-
neous coronary intervention (PCI) or AF ablation. Historically,
few options have been available for reversal of oral anti co-
agulants (Figure 3).
NOAC_ESOC.indd 37 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 38
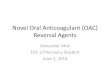
patients, with immediate, complete, and sustained reversal
of effect of anticoagulation reversal (Figure 4).
The median time to bleeding cessation among Group A
patients who could be assessed was 2.5 hours. The median
time from first vial to procedure initiation was 1.6 hours in
Group B and hemostasis was normal in >90% of patients
during their surgery or procedure. At 90 days, 6.3% and
7.4% of Group A and Group B patients, respectively, had a
thrombotic event. Idarucizumab has no contraindications, is
easy to use via infusion or IV injection, and is widely available
in more than 8,500 hospitals worldwide. Anticoagulation with
dabigatran can be restarted within 24 hours and heparin can
be initiated at any time. Post-marketing surveillance data
(RE-VECTO) show that idarucizumab performs well in clinical
practice, is consistent with use in the clinical trial, and no
new safety signals were observed.33
Andexanet Alfa
Andexanet alfa is a recombinant Factor Xa modified to lack
catalytic activity, but still capable of binding to factor Xa
inhibitors. It acts as a reversal agent for all direct specific
factor Xa inhibitors, fondaparinux, low molecular weight
heparin, and unfractionated heparin.34 Andexanet alfa
binds reversibly to factor Xa and thus is most effective when
given as an infusion.35,36 Andexanet alfa requires reconsti-
tution prior to IV administration by bolus and continuous
2-hour infusion. This agent has
a short half-life and transient
procoagulant signals have been
observed. The 2019 ANNEXA-4
trial evaluated reversal of factor
Xa inhibitors, including rivaro-
xaban and apixaban, in patients
with acute major bleeding
within 18 hours after ingesting
their last dose.36 All patients
(n=352) received an andexanet
bolus followed by a 2-hour
infusion and were evaluated
for changes in measures of
anti-factor Xa activity as well
as clinical hemostatic efficacy.
Following bolus admini-
stration, median anti-factor Xa
activity decreased by 92% from
Idarucizumab: A New Era in Reversal
In 2015, idarucizumab was approved for rapid reversal
when the anticoagulant effects of dabigatran is required
for emergency surgery, urgent intervention, or in life-thre-
atening or uncontrolled bleeding.31 Idarucizumab is a
humanized antigen-binding fragment, that binds both free
dabigatran and dabigatran bound to thrombin. There are no
known off-target effects and idarucizumab does not reverse
heparins or any other anticoagulants. Its binding affinity for
dabigatran is approximately 350 times higher than that of
dabigatran for thrombin. Idarucizumab is administered IV
with immediate onset of action. It has a short half-life and is
not associated with intrinsic procoagulant or anticoagulant
activity.
The RE-VERSE AD trial enrolled patients requiring urgent
surgery and patients with life-threatening bleeding (n=503).32
This multicenter, prospective, open-label, single-arm Phase
III study included patients with life threatening bleeding
(Group A) and patients who required emergency surgery
or procedures (Group B). Patients received idarucizumab
at hospital arrival. The primary endpoint was complete
dabigatran reversal within 4 hours of idarucizumab admini-
stration. The secondary endpoints at follow-up were
hemostasis within 24 hours (Group A), and hemostasis during
procedure (Group B), and thrombotic events, and mortality
in 90 days in all patients. Results showed efficacy for all
Figure 4. RE-VERSE AD efficacy of idarucizumab in patients with life-threatening bleeding (Group A) and requiring surgery (Group B)32
Group A Group B
NOAC_ESOC.indd 38 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 39
normalizing levels of anticoagulant activity, controlling
blood pressure, and all this treatment should be initiated
rapidly. Strategies for achieving these goals do not differ
among different NOACs or OACs. ICH is a rare compli-
cation associated with NOACs, with clinical trials for NOACs
showing an improvement over warfarin, but still an annual
residual risk of approximately 0.5% for ICH and approxi-
mately 3% per year for major bleeding.2,4,5,15
A subanalysis of 98 ICH patients treated with dabigatran in
the RE-VERSE AD study, which represented 32.6% of the full
trial cohort, suggests a rapid-acting benefit for idarucizumab
in the management of such patients.32 Complete reversal
of the diluted thrombin time and ecarin clotting time was
observed in 100% and >90% of evaluable patients, respec-
tively after the administration of idarucizumab. The diluted
thrombin time was reversed to normal levels, and none
of these patients required two doses of idarucizumab.39
Mortality was 16.4%, which is lower than mortality observed
in the RE-LY study.40
Results from a retrospective national case series study
provide additional clinical insight in the use of idarucizumab
in patients treated with dabigatran who present with ICH
(Figure).41
Forty patients presented with signs of stroke at 59 stroke
centers in Germany; 27 patients presented with ICH, 11
baseline in both groups. Twelve hours after infusion, clinical
haemostasis was adjudicated as excellent or good in 82% pf
patients. At 30 days, thrombotic events had occurred in 10%
of patients (Figure 5).36
Andexanet alfa is currently approved in Europe and the US
for the reversal of rivaroxaban and apixaban in patients with
life-threatening or uncontrolled bleeding;37 however, this
agent is associated with some challenges in clinical practice
including its limited availability, the lack of approved anti-FXa
assays, and the lengthy time required for preparation and
administration.38
In summary, it is important to consider the characteristics of
NOAC reversal agents when selecting initial OAC therapy.
Idarucizumab provides immediate, sustained, and predic-
table reversal of dabigatran’s anticoagulant effect, it is easy
to use, widely available, and has no contraindications, no
procoagulant effect. Andexanet alfa provides reversal of
apixaban and rivaroxaban but it is not approved for use in
patients requiring surgery or procedures.
MANAGING DABIGATRAN AND IDARUCIZUMAB IN NEUROLOGICAL EMERGENCIESBleeding Reversal in ICH
Treatment goals for patients who present with OAC-
associated ICH include preventing hematoma growth,
Figure 5. Reversal of Rivaroxaban or Apixaban in Patients with Bleeding
NOAC_ESOC.indd 39 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 40
no contraindications. Andexanet alfa provides reversal of
apixaban and rivaroxaban, although it is not approved for
use in patients requiring surgery or procedures. Finally, an
ICH subanalysis of RE-VERSE AD showed that idarucizumab
provides immediate reversal of dabigatran anticoagulation
for patients with ICH, which was supported by a growing
body of clinical practice data. In patients with acute
ischemic stroke, idarucizumab can be administered prior
to IV thrombolysis in dabigatran-treated patients. The wide
availability of this rapid-acting specific reversal agent for
dabigatran adds further support to the safety and efficacy
profile of dabigatran.
References1. Chugh SS, Roth GA, Gillum RF, Mensah GA. Global burden of atrial
fibrillation in developed and developing nations. Glob Heart 2014;9:113-9.
2. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. New Engl J Med 2009;361:1139-51.
3. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. New Engl J Med 2011;365:883-91.
4. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. New Engl J Med e 2011;365:981-92.
5. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. New Engl J Med 2013;369:2093-104.
patients had subdural hemorrhage, and 2 had subarachnoid
hemorrhage. Clinical improvement for most patients was
observed following idarucizumab administration, including
median NIHSS improvement of 4 points and modified Rankin
Scale (mRS) 0-3 in 60% of patients. Hematoma expansion
occurred in three patients; overall, mortality was low at 15%.
These findings were comparable to results from the RE-VERSE
AD study. 2018 European Heart Rhythm Association guidelines
currently recommend idarucizumab as the reversal agent for
dabigatran-associated bleeding. Idarucizumab is also guideli-
ne-recommended as an on-label treatment for patients who
present with ischemic stroke and can be administered prior
to IV thrombolysis.37 A case series of patients who presented
with ischemic stroke and were treated with thrombolysis after
idarucizumab (n=80) showed clinical improvement in 78.1% of
patients and a median 7-point improvement in NIHSS.42 No
thrombotic events were observed; mortality was 3.75%.
Conclusionthis symposium reviewed reversal before surgery, reversal
in patients with intracerebral hemorrhage, and reversal
in patients presenting with ischemic stroke prior to
thrombolysis. First, real world analyses provide a reassuring
mirroring of results from randomized NOAC trials and
consistently demonstrate the safety and efficacy profiles
of dabigatran in patients with AF. Recent data from other
settings (ESUS and CVT) further support the safety profile of
dabigatran. Second, it is important to consider the charac-
teristics of NOAC reversal agents when making initial OAC
treatment selections. Idarucizumab provides immediate,
sustained, and predictable reversal of dabigatran’s antico-
agulant effect, it is easy to use, widely available, and has
Figure 6. Idarucizumab outcomes: intracranial bleeding case series
NOAC_ESOC.indd 40 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 41
18. Diener HC, Connolly SJ, Ezekowitz MD, et al. Dabigatran compared with warfarin in patients with atrial fibrillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE-LY trial. Lancet Neurol 2010;9:1157-63.
19. Hart RG, Diener HC, Coutts SB, et al. Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol 2014;13:429-38.
20. Behrouzi R, Punter M. Diagnosis and management of cerebral venous thrombosis. Clin Med (Lond) 2018;18:75-9.
21. Connolly SJ, Wallentin L, Yusuf S. Additional events in the RE-LY trial. New Engl J Med 2014;371:1464-5.
22. Ezekowitz MD, Eikelboom J, Oldgren J, et al. Long-term evaluation of dabigatran 150 vs. 110 mg twice a day in patients with non-valvular atrial fibrillation. Europace 2016;18:973-8.
23. Cannon CP, Bhatt DL, Oldgren J, et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. The New England journal of medicine 2017;377:1513-24.
24. Graham DJ, Reichman ME, Wernecke M, et al. Stroke, Bleeding, and Mortality Risks in Elderly Medicare Beneficiaries Treated With Dabigatran or Rivaroxaban for Nonvalvular Atrial Fibrillation. JAMA internal medicine 2016;176:1662-71.
25. Lip GY, Keshishian A, Kamble S, et al. Real-world comparison of major bleeding risk among non-valvular atrial fibrillation patients initiated on apixaban, dabigatran, rivaroxaban, or warfarin. A propensity score matched analysis. Thromb Haemost 2016;116:975-86.
26. Graham DJ, Baro E, Zhang R, et al. Comparative Stroke, Bleeding, and Mortality Risks in Older Medicare Patients Treated with Oral Anticoagulants for Nonvalvular Atrial Fibrillation. Am J Med 2019.
27. Huisman MV, Rothman KJ, Paquette M, et al. Two-year follow-up of patients treated with dabigatran for stroke prevention in atrial fibrillation: Global Registry on Long-Term Antithrombotic Treatment in Patients with Atrial Fibrillation (GLORIA-AF) registry. Am Heart J 2018;198:55-63.
28. Xian Y, O'Brien EC, Liang L, et al. Association of Preceding Antithrom botic Treatment With Acute Ischemic Stroke Severity and In-Hospital Outcomes Among Patients With Atrial Fibrillation. JAMA 2017;317:1057-67.
6. Turpie AG. New oral anticoagulants in atrial fibrillation. Eur Heart J 2008;29:155-65.
7. Khoo CW, Tay KH, Shantsila E, Lip GY. Novel oral anticoagulants. Int J Clin Pract 2009;63:630-41.
8. Hanley JP. Warfarin reversal. J Clin Pathol 2004;57:1132-9.
9. Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L. Newly identified events in the RE-LY trial. New Engl J Med 2010;363:1875-6.
10. Yao X, Shah ND, Sangaralingham LR, Gersh BJ, Noseworthy PA. Non–Vitamin K Antagonist Oral Anticoagulant Dosing in Patients With Atrial Fibrillation and Renal Dysfunction. J Am Coll Cardiol 2017;69:2779-90.
11. Freedman B, Potpara TS, Lip GY. Stroke prevention in atrial fibrillation. Lancet (London, England) 2016;388:806-17.
12. Mazurek M, Huisman MV, Rothman KJ, et al. Regional Differences in Antithrombotic Treatment for Atrial Fibrillation: Insights from the GLORIA-AF Phase II Registry. Thromb Haemost 2017;117:2376-88.
13. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:2893-962.
14. Ben Freedman S, Gersh BJ, Lip GYH. Misperceptions of aspirin efficacy and safety may perpetuate anticoagulant underutilization in atrial fibrillation. European Heart Journal 2014;36:653-6.
15. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. New Engl J Med 2011;365:883-91.
16. Lopes RD, Al-Khatib SM, Wallentin L, et al. Efficacy and safety of apixaban compared with warfarin according to patient risk of stroke and of bleeding in atrial fibrillation: a secondary analysis of a randomised controlled trial. Lancet (London, England) 2012;380:1749-58.
17. Lip GY, Clemens A, Noack H, Ferreira J, Connolly SJ, Yusuf S. Patient outcomes using the European label for dabigatran. A post-hoc analysis from the RE-LY database. Thromb Haemost 2014;111:933-42.
NOAC_ESOC.indd 41 26/07/2019 12:33

©ORUEN LTD
HOW NOAC SELECTION AND REVERSAL CAN HELP PROTECT OUR PATIENTS: YOUR QUESTIONS ANSWERED
CNS 2019: 5:(1). JULY 2019 42
39. Steiner T RP, van Ryn J, et al. . Reversal of Dabigatran Anticoagulation with Idarucizumab in Patients with Intracranial Hemorrhage: Subanalysis of RE-VERSE AD. International Stroke Conference. Los Angeles, CA: https://professional.heart.org/idc/groups/ahamah-public/@wcm/@sop/@scon/documents/downloadable/ucm_498744.pdf; 2018.
40. Hart RG, Diener HC, Yang S, et al. Intracranial hemorrhage in atrial fibrillation patients during anticoagulation with warfarin or dabigatran: the RE-LY trial. Stroke 2012;43:1511-7.
41. Kermer P, Eschenfelder CC, Diener H-C, Grond M. Abstract 84: Idarucizumab in Patients Treated With Dabigatran Suffering Cerebral Ischemia or Intracranial Hemorrhage: A Retrospective Case Series From Germany. Stroke 2019;50:A84-A.
42. Kermer P, Eschenfelder CC, Diener HC, et al. Antagonizing dabigatran by idarucizumab in cases of ischemic stroke or intracranial hemorrhage in Germany - A national case collection. Int J Stroke 2017;12:383-91.
29. Nielsen PB, Skjoth F, Sogaard M, Kjaeldgaard JN, Lip GY, Larsen TB. Effectiveness and safety of reduced dose non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. BMJ 2017;356:j510.
30. Goldstein JN, Refaai MA, Milling TJ, Jr., et al. Four-factor prothrombin complex concentrate versus plasma for rapid vitamin K antagonist reversal in patients needing urgent surgical or invasive interventions: a phase 3b, open-label, non-inferiority, randomised trial. Lancet (London, England) 2015;385:2077-87.
31. Schiele F, van Ryn J, Canada K, et al. A specific antidote for dabigatran: functional and structural characterization. Blood 2013;121:3554-62.
32. Pollack CV, Jr., Reilly PA, van Ryn J, et al. Idarucizumab for Dabigatran Reversal - Full Cohort Analysis. New Engl J Med 2017;377:431-441
33. Fanikos J et al. RE-VECTO: Idarucizumab drug administration surveillance program results. The Congress on Open Issues in Thrombosis and Hemostasis 2018 jointly with the 9th Russian Conference on Clinical Hemostasiology and Hemorheology. Abstract;68.
34. Lu G, DeGuzman FR, Hollenbach SJ, et al. A specific antidote for reversal of anticoagulation by direct and indirect inhibitors of coagulation factor Xa. Nat Med 2013;19:446-51.
35. Siegal DM, Curnutte JT, Connolly SJ, et al. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. New Engl J Med 2015;373:2413-24.
36. Connolly SJ, Crowther M, Eikelboom JW, et al. Full Study Report of Andexanet Alfa for Bleeding Associated with Factor Xa Inhibitors. New Engl J Med 2019;380:1326-35.
37. Steffel J, Verhamme P, Potpara TS, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J 2018;39:1330-93.
38. Culbreth SE, Rimsans J, Sylvester K, Pallin DJ, Connors JM. Andexanet alfa-The first 150 days. Am J Hematol 2019;94:E21-e4.
NOAC_ESOC.indd 42 26/07/2019 12:33