Embed Size (px)
Citation preview
How Should We be Assessing and Documenting Endoscopies in IBD:
Incorporating Standard Scoring Systems into Patient Care
Gary R Lichtenstein, MD
Director, Center for IBD
University of Pennsylvania School of Medicine
Hospital of the University of PA
Philadelphia, PA
Uses of Endoscopy in IBD
Diagnosis Disease extent Prognostication Assessment of Activity/Healing Stricture evaluation and dilation Dysplasia Surveillance Diagnose/Control Bleeding Pouch Evaluation Endoscopic Ultrasound Video Capsule Endoscopy

I. Mucosal Healing UC and Crohn’s disease characterized by the
presence of gut inflammation accompanied by areas of ulceration
Mucosal healing is becoming increasingly important in the clinical management of UC and Crohn’s disease, as well as being used as an end point in clinical trials.
Achieving mucosal healing has unequivocally been associated with better outcomes, and for these reasons, it has become an important treatment goal.
I. Mucosal Healing Multiple methods to score endoscopic disease
activity in both UC and Crohn’s disease. Those used most frequently or that have been
validated: • Mayo Endoscopic Score
• Ulcerative Colitis Endoscopic Index of Severity (UCEIS)
• Crohn’s Disease Endoscopic Index of Severity (CDEIS),
• Simple Endoscopic Score for Crohn’s Disease (SES-CD),
• Rutgeerts Postoperative Endoscopic Index for Crohn’s disease.
II. Definition of Mucosal Healing
Mucosal healing in the context of IBD refers to the endoscopic assessment of disease activity.
Simply stated, mucosal healing should imply the absence of ulceration and erosions.
There is currently no validated definition of mucosal healing in IBD.

III. Inflammation in UC The pattern of inflammation in UC is associated
with several mucosal changes, initially vascular congestion, erythema, and granularity.
As inflammation becomes more severe, friability (bleeding to light touch), spontaneous bleeding, and erosions and ulcers develop.

What Is the Definition of Mucosal Healing?

AGA Consensus on Efficacy End Points: Endoscopic Healing
in Ulcerative Colitis
“Absence of friability, blood, erosions, and ulcers in all visualized segments are the required components of genuine endoscopic healing.”
D’Haens G et al. Gastroenterology 2007;132(2):763–86.

Mucosal Healing in Ulcerative Colitis Disease:
The Issues• What is the definition of mucosal healing?
– Depends on finding a scoring system of your choice
– some studies allow erythema and friability in the
definition of mucosal healing 1
Many different endoscopic indices for UC have been
used in clinical trials, only one UCEIS - validated in prospective studies; this creates problems when comparing trials.
1.) Dave M, et al Gastroenterol Hepatol 2012;8(1):29–38.

Mucosal Abnormalities in Crohn’s Disease
The SB has limited ways to demonstrate injury:Mucosal Disruption
Erosions Ulcers
ErythemaVillous BluntingStrictures
These findings are easily captured by capsule endoscopy, but are not pathognomonic of IBD.
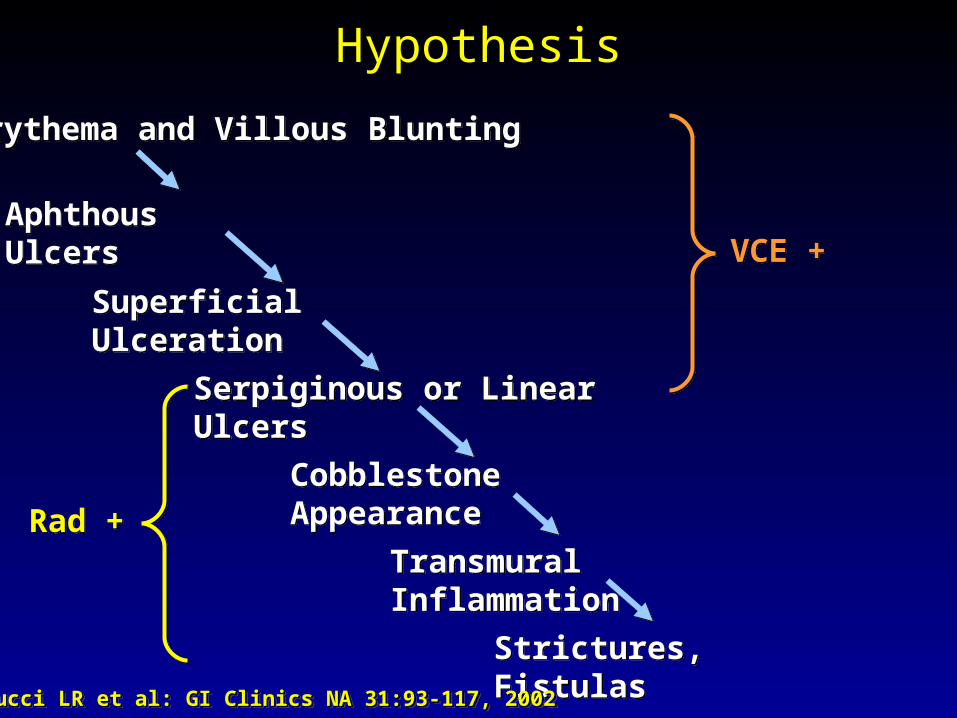
Hypothesis
Erythema and Villous BluntingErythema and Villous Blunting
Serpiginous or Linear UlcersSerpiginous or Linear Ulcers
Cobblestone AppearanceCobblestone Appearance
Transmural InflammationTransmural Inflammation
Aphthous UlcersAphthous Ulcers
Strictures, FistulasStrictures, Fistulas
Superficial UlcerationSuperficial Ulceration
VCE +VCE +
Rad +Rad +
Carucci LR et al: GI Clinics NA 31:93-117, 2002Carucci LR et al: GI Clinics NA 31:93-117, 2002Carucci LR et al: GI Clinics NA 31:93-117, 2002Carucci LR et al: GI Clinics NA 31:93-117, 2002
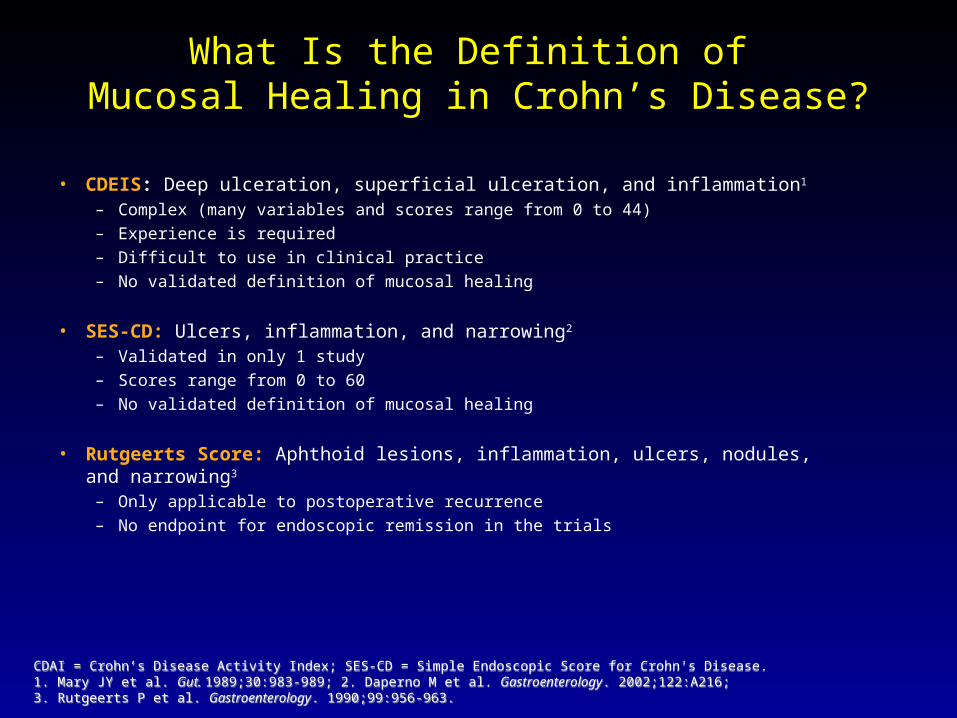
What Is the Definition of Mucosal Healing in Crohn’s Disease?
• CDEIS: Deep ulceration, superficial ulceration, and inflammation1
– Complex (many variables and scores range from 0 to 44)
– Experience is required
– Difficult to use in clinical practice
– No validated definition of mucosal healing
• SES-CD: Ulcers, inflammation, and narrowing2
– Validated in only 1 study
– Scores range from 0 to 60
– No validated definition of mucosal healing
• Rutgeerts Score: Aphthoid lesions, inflammation, ulcers, nodules, and narrowing3
– Only applicable to postoperative recurrence
– No endpoint for endoscopic remission in the trials
CDAI = Crohn’s Disease Activity Index; SES-CD = Simple Endoscopic Score for Crohn's Disease. 1. Mary JY et al. Gut. 1989;30:983-989; 2. Daperno M et al. Gastroenterology. 2002;122:A216; 3. Rutgeerts P et al. Gastroenterology. 1990;99:956-963.
CDAI = Crohn’s Disease Activity Index; SES-CD = Simple Endoscopic Score for Crohn's Disease. 1. Mary JY et al. Gut. 1989;30:983-989; 2. Daperno M et al. Gastroenterology. 2002;122:A216; 3. Rutgeerts P et al. Gastroenterology. 1990;99:956-963.
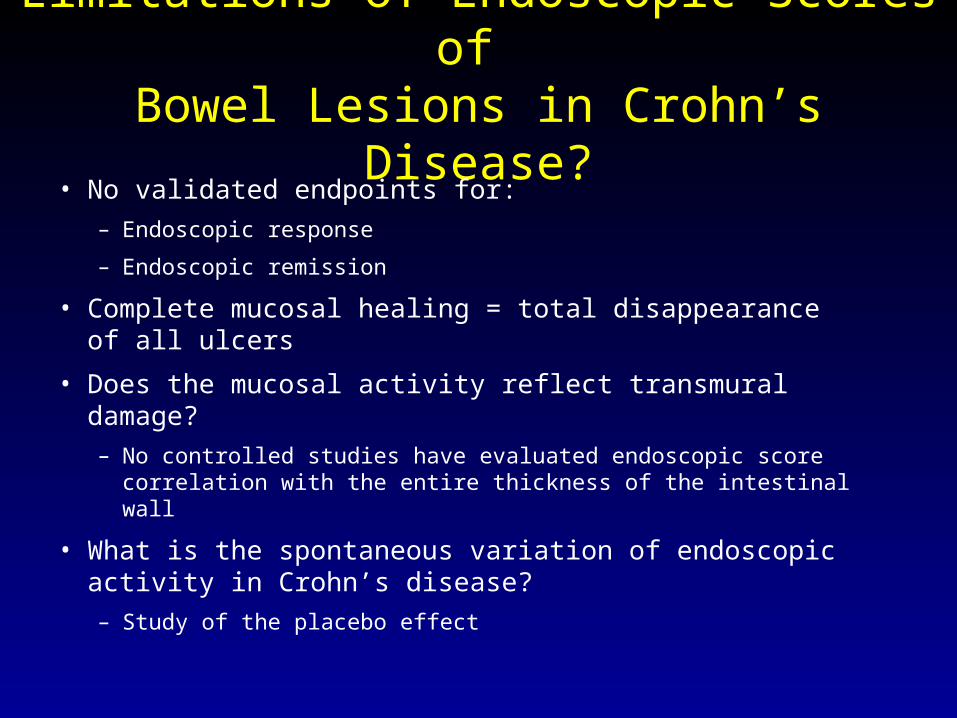
Limitations of Endoscopic Scores of Bowel Lesions in Crohn’s Disease?
• No validated endpoints for:
– Endoscopic response
– Endoscopic remission
• Complete mucosal healing = total disappearance of all ulcers
• Does the mucosal activity reflect transmural damage?
– No controlled studies have evaluated endoscopic score correlation with the entire thickness of the intestinal wall
• What is the spontaneous variation of endoscopic activity in Crohn’s disease?
– Study of the placebo effect
• Does not access small bowel other than terminal ileum
• Makes assumption that changes to the lesions in terminal ileum reflect what transpires in remainder of the small bowel
Limitations of Endoscopic Scores of Bowel Lesions in Crohn’s Disease?
Actual Endoscopic Indices
• Ulcerative Colitis– Mayo Score
– UCIEIS
• Crohn’s Disease
– UCEIS
– SES-CD
– Rutgeerts Score
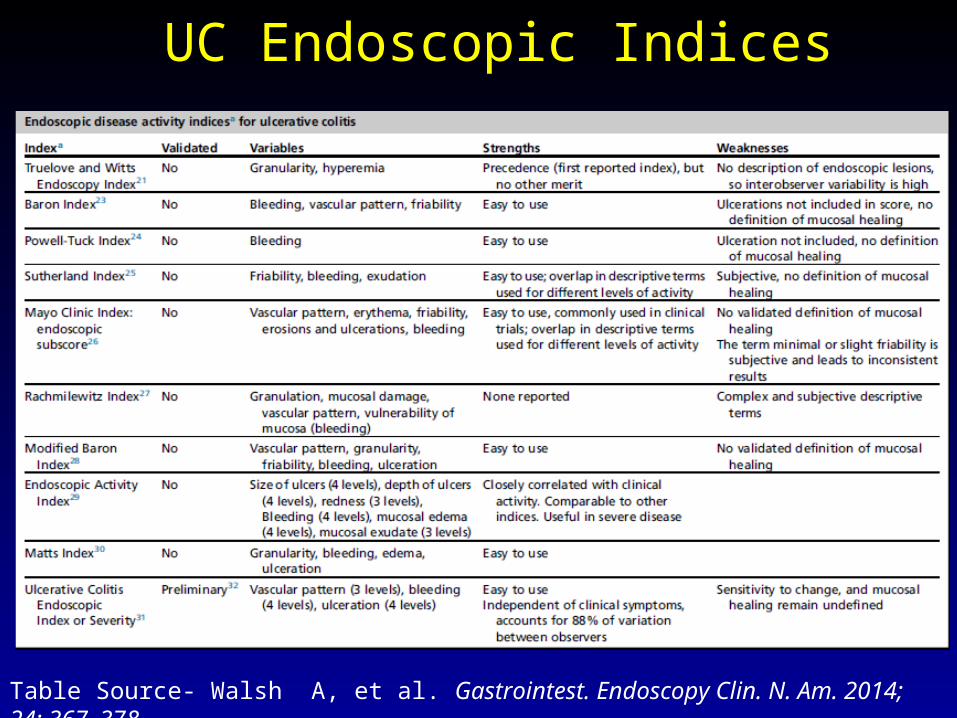
UC Endoscopic Indices
Table Source- Walsh A, et al. Gastrointest. Endoscopy Clin. N. Am. 2014; 24: 367–378

Mayo Scoring System1
for Assessment of UC Activity• Stool frequency: 0 = Normal number of stools for this patient
1 = 1 to 2 stools more than normal2 = 3 to 4 stools more than normal3 = 5 or more stools more than normal
• Rectal bleeding: 0 = None1 = Streaks of blood with stool less than half the time2 = Obvious blood with stool most of the time3 = Blood alone passes
• Endoscopic findings: 0 = Normal or inactive disease1 = Mild disease (redness, decreased vascular pattern visible, friability)2 = Moderate disease (redness, no vascular pattern visible, friability, erosions)3 = Severe disease (bleeding, ulceration)
• Physician’s global assessment of disease activity: 0 (normal) to 3 (severe)
1. Schroeder KW, et al. N Engl J Med. 1987;317(26):1625-1629.

Overlap in the features of the different levels of this endoscopic index, which causes high interobserver variation.
The most troublesome component of this index is friability, as this is subjective and leads to inconsistent results.1
This inconsistency has lead to an adaptation of the index to remove friability. 2,3
1.) D’Haens G, et al Gastroenterology2012;143(6):1461–9.
2.) Kamm MA, et al. Gastroenterology2007;132(1):66–75.
3.) Lichtenstein GR, et al Clinical Gastroenterol Hepatol. 2007; 2007;5: 95–102.
Mayo Score: Practical Points
The value of this index is its widespread use in clinical trials.
Mucosal healing – 0 or 1- or a deceases from the subscores of 2 or 3.1
In Active Ulcerative Colitis Trials, patients with a post-treatment Mayo score of grade 1 were no more likely to undergo a colectomy than those with a score of 0. 1
1.) Rutgeerts P , et al N Engl J Med 2005;353(23):2462–76.
Mayo Score: Practical Points
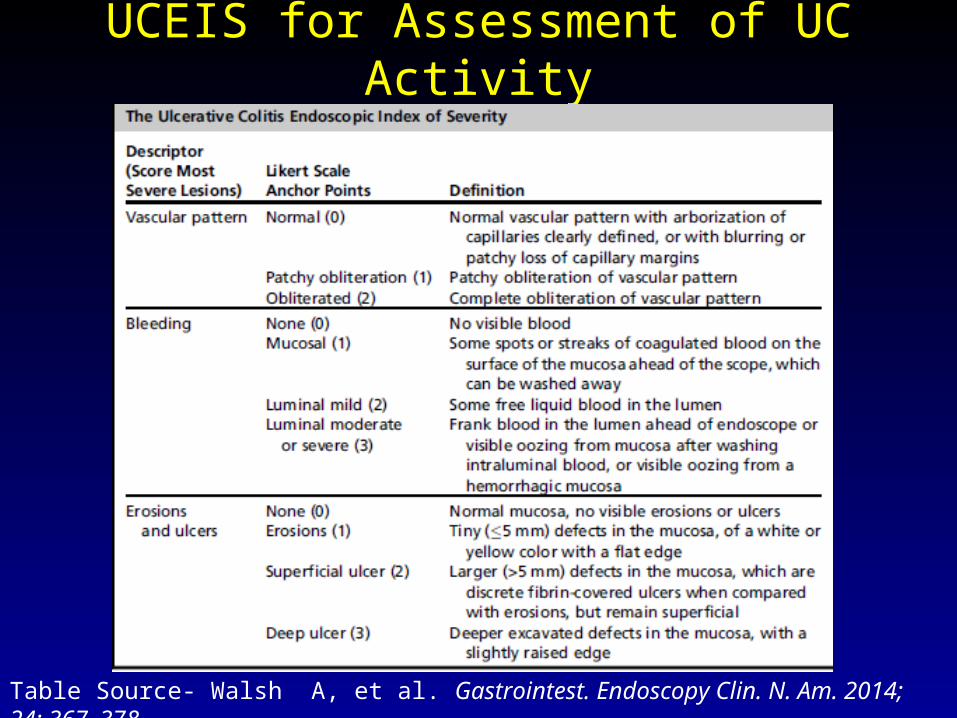
UCEIS for Assessment of UC Activity
Table Source- Walsh A, et al. Gastrointest. Endoscopy Clin. N. Am. 2014; 24: 367–378

• In practical terms, the most severely affected part of the mucosa is scored.
• Limitations-– Thresholds for remission and mild, moderate, and
severe disease have yet to be set.– The extent to which full colonoscopy may influence
the score compared with the flexible sigmoidoscopy on which it was based, has only started to be evaluated .1
1- Thia KT et al, Inflamm Bowel Dis. 2011;17(6):1257–64.
UCEIS: Practical Points
• Knowledge of symptoms does not materially influence the score, and a comparison with the Mayo Clinic endoscopy subscore shows that the UCEIS is less subject to variation by a central reader.
• UCEIS is simple enough to use in clinical practice and should achieve its goal of reducing variation in endoscopic assessment of activity between observers.
• Patients admitted with acute severe colitis with a score of 7 or 8 (out of 8) on admission predicted an inadequate response to intravenous steroids and the need for rescue therapy with cyclosporine or infliximab1.
• Easy for in office use
1.) Conte CJ, et al. Gastroenterology 2013; 144(5): S-102.
UCEIS: Practical Points
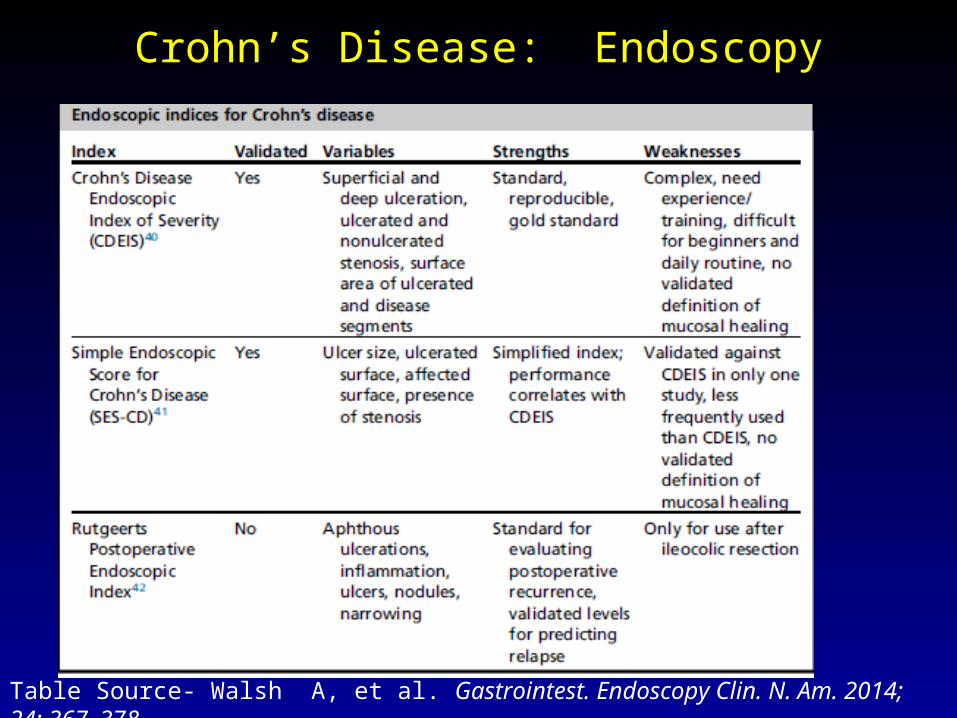
Crohn’s Disease: Endoscopy
Table Source- Walsh A, et al. Gastrointest. Endoscopy Clin. N. Am. 2014; 24: 367–378

Crohn’s Disease Endoscopic Index of Severity
Mary JY, et al. Gut 1989;30(7): 983–9.
Prospectively developed instrument constructed to detect changes in disease activity1.
Examines 4 endoscopic variables In each of the following locations: rectum, sigmoid
and left colon, transverse colon, and right colon and ileum
CDEIS scores range from 0 to 44.
Crohn’s Disease Endoscopic Index of Severity CDEIS Evaluates:
• Deep ulcerations: score 0 if absent or 12 if present.
• Superficial ulcerations: score 0 if absent or 6 if present.
• Length of ulcerated mucosa (0-10cm): score 0 to 10 according to length in centimeters
• Length of diseased mucosa (0-10cm): score 0 to 10 according to length in centimeters.
1.) Conte CJ, et al. Gastroenterology 2013; 144(5): S-102.

Crohn’s Disease Endoscopic Index of Severity
The numbers are added up in each segment and divided by the number of segments evaluated.
An additional 3 points is given if an ulcerated stenosis is present, and a further 3 points if a nonulcerated stenosis is present.
Mary JY, et al. Gut 1989;30(7): 983–9.

Crohn’s Disease Endoscopic Index of Severity
Table Source- Walsh A, et al. Gastrointest. Endoscopy Clin. N. Am. 2014; 24: 367–378

Crohn’s Disease Endoscopic Index of Severity
CDEIS Definitions:• Endoscopic remission (minor or no lesions) is
defined as a CDEIS score less than or equal to 6 or less than or equal to 7
• Complete endoscopic remission (mucosal healing, i.e., no lesions at all or scarred lesions only) is defined as a CDEIS score less than or equal to 3 or less than or equal to 4.
• Endoscopic response is a decrease from baseline CDEIS score of at least 4 or 5 points..
Mary JY, et al. Gut 1989;30(7): 983–9.

Crohn’s Disease Endoscopic Index of Severity
Critque:• It is the standard index and it is reproducible.
• It is complex
• Requires training and experience • To estimate ulcerated or disease mucosal surface
areas
• To distinguish between superficial and deep ulcerations.
• It is cumbersome to use in clinical practice.
Mary JY, et al. Gut 1989;30(7): 983–9.

Simplified Endoscopic Score for Crohn’s Disease
Daperno M, et al. Gastrointest Endoscopy 2004; 60: 505-512.
Crohn’s Disease Endoscopic Index of Severity
Critque:• The SES-CD correlates well with the CDEIS
• Correlation coefficient (r=0.920)
• Interobserver reliability (kappa- 0.791-1.000)
• Easy to use
• Less complex than the CDEIS
• No cutoff values have been determined for this
• Mucosal healing not defined.
Daperno M, et al. Gastrointest Endoscopy 2004; 60: 505-512.

The Natural Course of Postop CD
Recurrence is clinically silent initially
Surgery
Radiologic Clinical SurgicalEndoscopicHistologic
Within 1 week
70-90% by 1 yr
Tissue damage
30% 3 yr60% 5 yr
[1] D’Haens G, Geboes K, Peeters M, et al. Gastroenterology 1998;114:262-267.[2] Olaison G, S medh K, Sjodahl R. Gut 1992;33:331-335.[3] Rutgeerts P, Geboes K, Vantrappen G, et al Gastroenterology 1990;99:956-983.[4] Sachar DB. Med Clin North Am 1990;74:183-188.
50% by 5 yrs

• i0: no lesions
• i1: < 5 aphthous lesions
• i2: > 5 aphthous lesions with normal intervening
mucosa
• i3: diffuse aphthous ileitis with diffusely inflamed
mucosa
• i4: diffuse inflammation with large ulcers,
nodules, and/or narrowing
Rutgeerts P, Geboes K, Vantrappen G, et al Gastroenterology 1990;99:956-983.
Endoscopic Recurrence Score

>70% of Pts Have i2,3,4 Recurrence 1 Year after Surgery – Rutgeerts et al Gastro 1990
i1
i,3 i4
i0 and i1 remission-low likelihood of progression
i2,i3,i4 recurrenceLikely progressionto another surgery

Actuarial Rate of Symptomatic Recurrence
0 11 2 3 4
Those individuals with grade 3 and 4 lesions at one year postoperatively during
colonoscopy were more likely to have symptomatic recurrences earlier than
those with individuals with grade 1 and 2 lesions.
5 6 7 8 9 10
0.2
0
0.4
0.6
0.8
1.0
% s
ympt
om f
ree
surv
ival
Grade 4
Grade 0 and Grade 1
Grade 2
Grade 3
Rutgeerts P, Geboes K, Vantrappen G, et al Gastroenterology 1990;99:956-983.

POCER Study: Postoperative Crohn’s Disease POCER Study: Postoperative Crohn’s Disease Endoscopic Recurrence Endoscopic Recurrence
SURGERY: Curative resection
RISK Stratification: Low or High(High risk: smoker,≥ second operation,perforating disease)
No Endoscopy (“Standard”)Risk driven best drug therapy
Endoscopic Intervention
(“Active”)
18 M
onth
Col
onos
copy
2/3 of patients
1/3 of patients
6 Month Colonoscopy
Step up Rx if ≥ i2 on Rutgeerts scale
All patients: Metronidazole: 0-3 months
High risk: Thiopurine or adalimumab if thiopurine intolerantLow risk: No further treatment
Methods: Multicentre RCT
De Cruz P, et al. Presented at DDW; May 21 2013. Abstract 925J.
Randomization
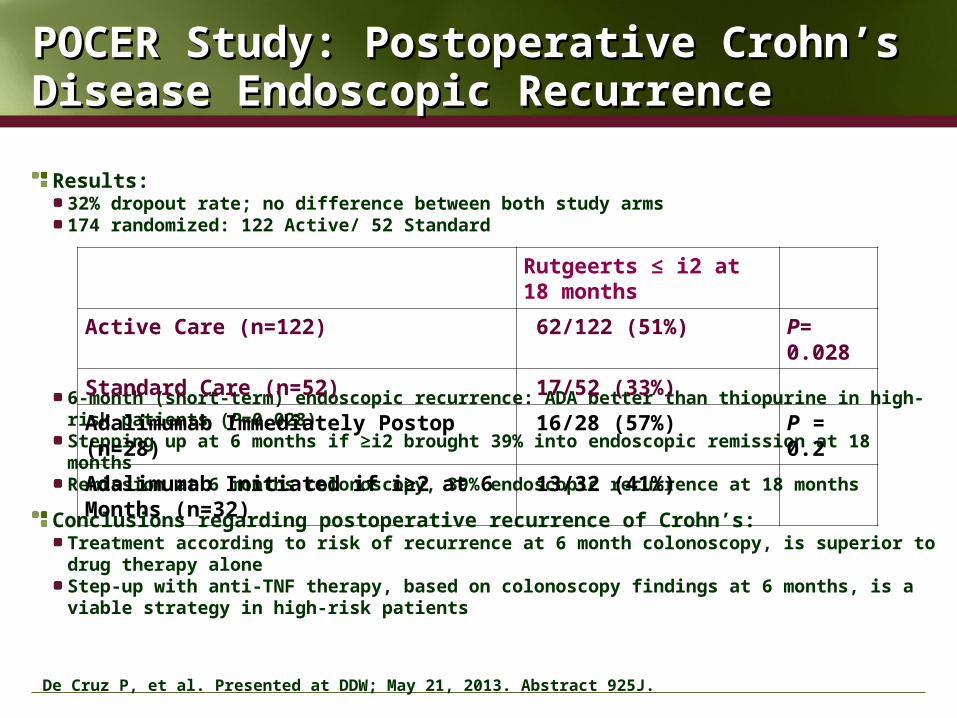
Results: 32% dropout rate; no difference between both study arms174 randomized: 122 Active/ 52 Standard
6-month (short-term) endoscopic recurrence: ADA better than thiopurine in high-risk patients (P=0.028)Stepping up at 6 months if ≥i2 brought 39% into endoscopic remission at 18 monthsRemission at 6 months colonoscopy, 39% endoscopic recurrence at 18 months
Conclusions regarding postoperative recurrence of Crohn’s: Treatment according to risk of recurrence at 6 month colonoscopy, is superior to drug therapy aloneStep-up with anti-TNF therapy, based on colonoscopy findings at 6 months, is a viable strategy in high-risk patients
POCER Study: Postoperative Crohn’s Disease POCER Study: Postoperative Crohn’s Disease Endoscopic Recurrence Endoscopic Recurrence
Rutgeerts ≤ i2 at 18 months
Active Care (n=122) 62/122 (51%) P= 0.028
Standard Care (n=52) 17/52 (33%)
Adalimumab Immediately Postop (n=28) 16/28 (57%) P = 0.2
Adalimumab Initiated if i≥2 at 6 Months (n=32) 13/32 (41%)
De Cruz P, et al. Presented at DDW; May 21, 2013. Abstract 925J.
CONCLUSION The colonoscopic assessment of mucosal inflammation
and healing is important for assessment of patients with UC and CD
All clinicians should try to achieve mucosal healing in patients with IBD
Multiple endoscopic indices for UC exist but only one, the UCEIS is validated
The CDEIS and SES-CD are validated in CD The Rutgeerts postoperative endoscopic index is useful for
predicting the clinical course in patients with ileocecal CD undergoing ileocecal resections




![Lichtenstein v. Lichtenstein · [Cite as Lichtenstein v.Lichtenstein, 2020-Ohio-5080.] COURT OF APPEALS OF OHIO EIGHTH APPELLATE DISTRICT COUNTY OF CUYAHOGA RYAN LICHTENSTEIN, : Plaintiff-Appellee,](https://img.pdfslide.net/doc/110x75/60903f096995511fe42a0d9e/lichtenstein-v-cite-as-lichtenstein-vlichtenstein-2020-ohio-5080-court-of.jpg)