Embed Size (px)
Citation preview
HOW SWEET IT IS:HOW SWEET IT IS:
Managing Diabetes For A Healthy Managing Diabetes For A Healthy Pregnancy And BeyondPregnancy And Beyond Ruth Ferrarotti, MSN, APRN-BC, Ruth Ferrarotti, MSN, APRN-BC, CDECDE Assoc. Clinical Prof., Univ. of Conn.Assoc. Clinical Prof., Univ. of Conn.
Discussion TopicsDiscussion Topics
Gestational Diabetes:Gestational Diabetes:Diagnosis and management Diagnosis and management
Postpartum recommendationsPostpartum recommendations
Established Diabetes:Established Diabetes:Pre-pregnancy counselingPre-pregnancy counseling
Management of diabetesManagement of diabetes
Postpartum recommendationsPostpartum recommendations
Diabetes After PregnancyDiabetes After Pregnancy
Classification of Classification of DiabetesDiabetes Type 1 DiabetesType 1 Diabetes – Beta cell – Beta cell
destruction destruction Type 2 DiabetesType 2 Diabetes – Progressive insulin – Progressive insulin
secretory defect and insulin resistancesecretory defect and insulin resistance OtherOther – genetic defects, diseases of – genetic defects, diseases of
exocrine pancreas and drug/chemical exocrine pancreas and drug/chemical inducedinduced
Gestational DiabetesGestational Diabetes
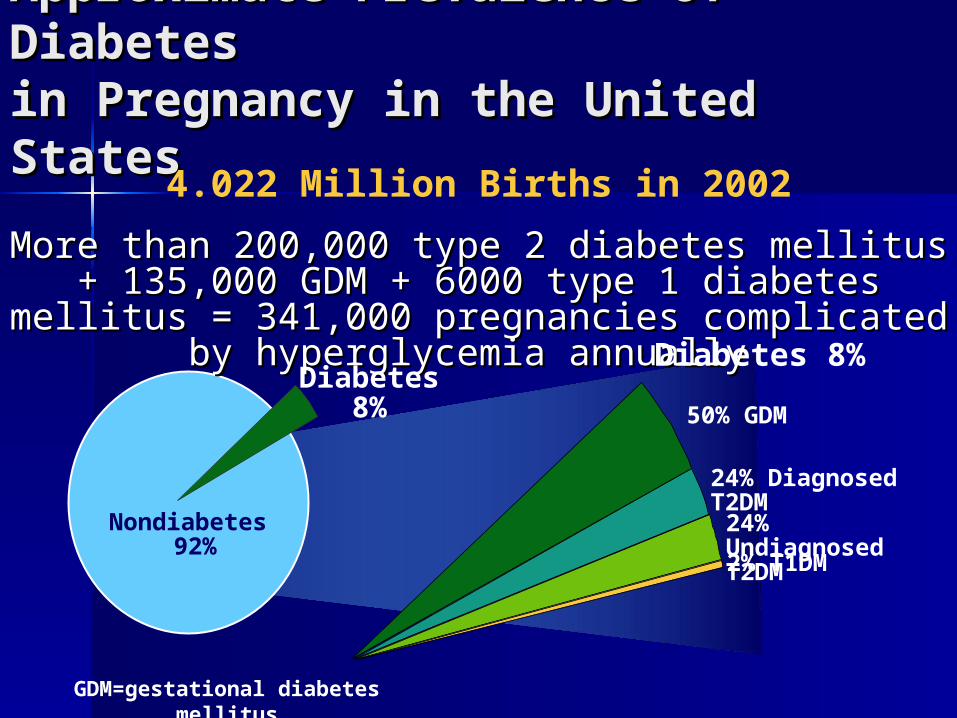
Approximate Prevalence of Approximate Prevalence of Diabetes Diabetes in Pregnancy in the United Statesin Pregnancy in the United States
GDM=gestational diabetes mellitus
Nondiabetes 92%
More than 200,000 type 2 diabetes mellitus + 135,000 GDM + 6000 More than 200,000 type 2 diabetes mellitus + 135,000 GDM + 6000 type 1 diabetes mellitus = 341,000 pregnancies complicated by type 1 diabetes mellitus = 341,000 pregnancies complicated by
hyperglycemia annually hyperglycemia annually
Diabetes 8%
4.022 Million Births in 2002
50% GDM
Diabetes 8%
2% T1DM
24% Diagnosed T2DM
24% Undiagnosed T2DM
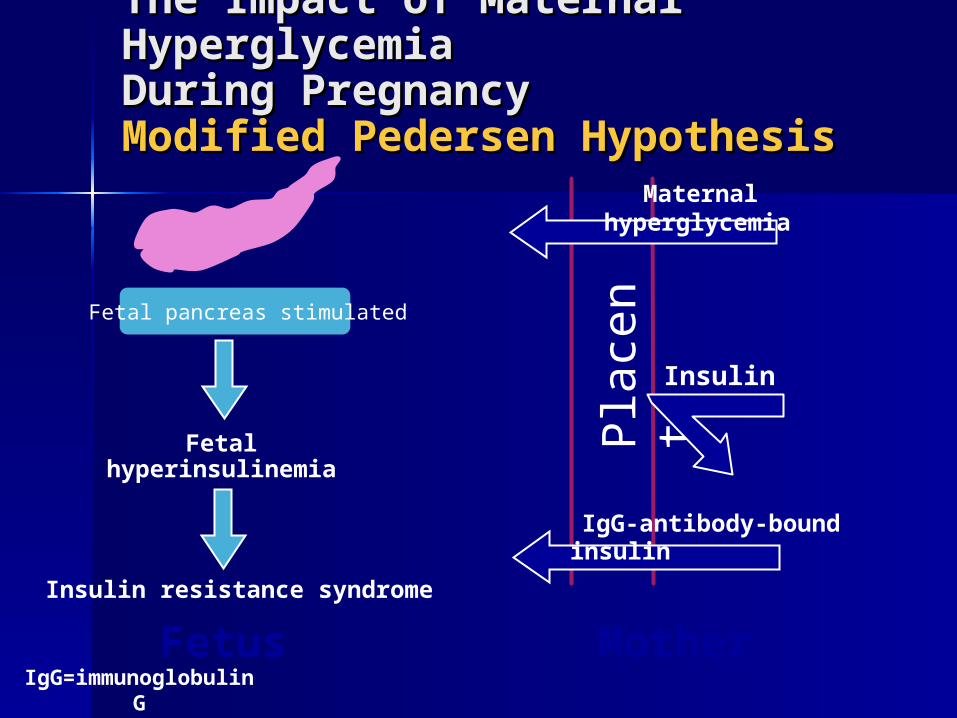
Fetalhyperinsulinemia
The Impact of Maternal The Impact of Maternal Hyperglycemia Hyperglycemia During PregnancyDuring PregnancyModified Pedersen HypothesisModified Pedersen Hypothesis
Fetus
Fetal pancreas stimulated
IgG=immunoglobulin GMother
Plac
enta
IgG-antibody-bound insulin
Insulin
Maternal hyperglycemia
Insulin resistance syndrome
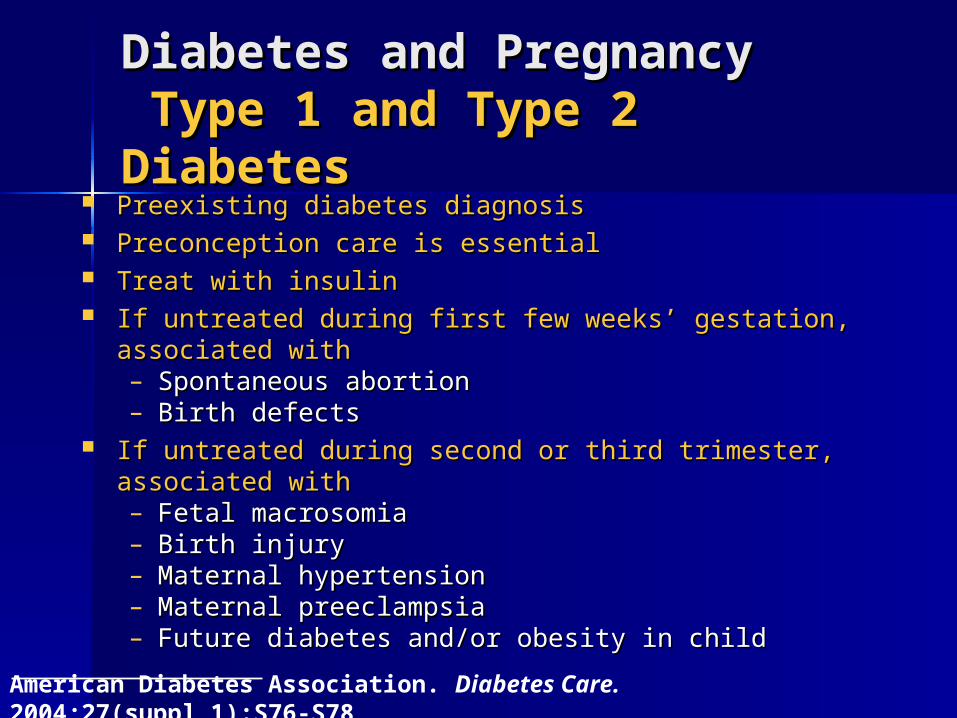
Diabetes and PregnancyDiabetes and Pregnancy Type 1 and Type 2 DiabetesType 1 and Type 2 Diabetes
Preexisting diabetes diagnosisPreexisting diabetes diagnosis Preconception care is essentialPreconception care is essential Treat with insulinTreat with insulin If untreated during first few weeks’ gestation, If untreated during first few weeks’ gestation,
associated withassociated with– Spontaneous abortionSpontaneous abortion– Birth defectsBirth defects
If untreated during second or third trimester, associated If untreated during second or third trimester, associated withwith– Fetal macrosomiaFetal macrosomia– Birth injuryBirth injury– Maternal hypertensionMaternal hypertension– Maternal preeclampsiaMaternal preeclampsia– Future diabetes and/or obesity in childFuture diabetes and/or obesity in child
American Diabetes Association. Diabetes Care. 2004;27(suppl 1):S76-S78
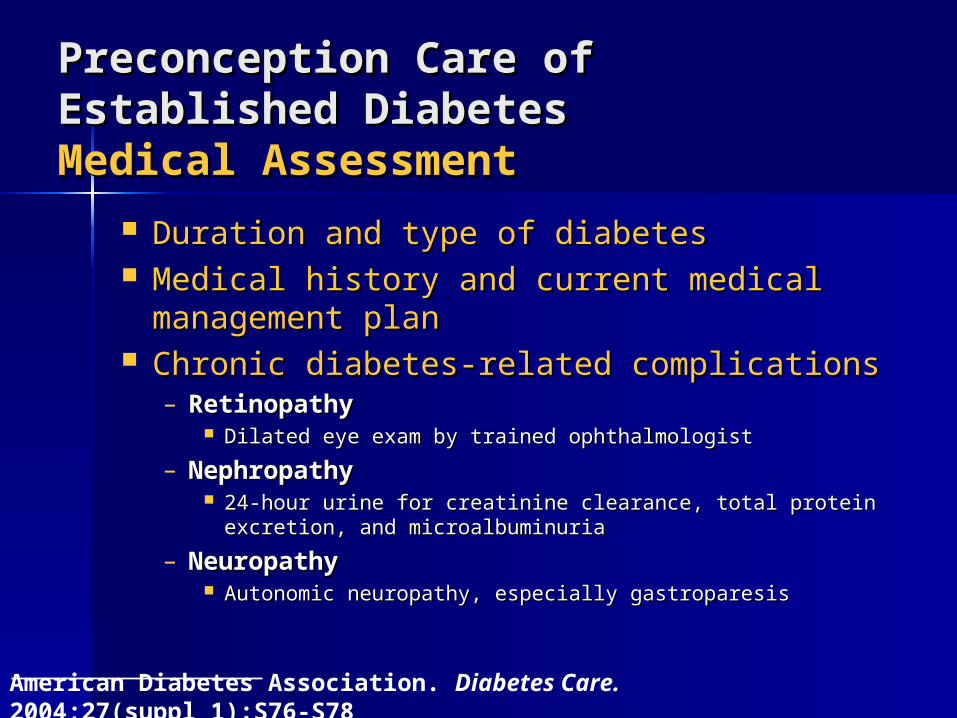
Preconception Care of Established Preconception Care of Established DiabetesDiabetesMedical AssessmentMedical Assessment
Duration and type of diabetesDuration and type of diabetes Medical history and current medical Medical history and current medical
management planmanagement plan Chronic diabetes-related complicationsChronic diabetes-related complications
– RetinopathyRetinopathy Dilated eye exam by trained ophthalmologistDilated eye exam by trained ophthalmologist
– NephropathyNephropathy 24-hour urine for creatinine clearance, total protein 24-hour urine for creatinine clearance, total protein
excretion, and microalbuminuriaexcretion, and microalbuminuria
– NeuropathyNeuropathy Autonomic neuropathy, especially gastroparesisAutonomic neuropathy, especially gastroparesis
American Diabetes Association. Diabetes Care. 2004;27(suppl 1):S76-S78
Preconception Care of Established Preconception Care of Established DiabetesDiabetesMedical AssessmentMedical Assessment
Comorbid conditions (in addition to Comorbid conditions (in addition to diabetic complications)diabetic complications)– HypertensionHypertension
Measure blood pressureMeasure blood pressure
– Coronary artery diseaseCoronary artery disease Stress testStress test
– Hyper- or hypothyroidismHyper- or hypothyroidism Free TFree T44 and TSH and TSH
– Other autoimmune diseasesOther autoimmune diseasesT4=thyroxineTSH=thyroid-stimulating hormone
American Diabetes Association. Diabetes Care. 2004;27(suppl 1):S76-S78
SMBGSMBG– Fasting/premeal: 70 to100 mg/dLFasting/premeal: 70 to100 mg/dL– 1 hour postmeal: <140 mg/dL1 hour postmeal: <140 mg/dL
A1CA1C– In normal range (<6%, but ideally <5%)In normal range (<6%, but ideally <5%)– Monitor until A1C is stable at <6%Monitor until A1C is stable at <6%
Preconception Care of Established Preconception Care of Established DiabetesDiabetesBlood Glucose GoalsBlood Glucose Goals
SMBG=self-monitoring of blood glucose
Jovanovic L, ed in chief. Medical Management of Pregnancy Complicated by Diabetes. 3rd ed. Alexandria, Va: American Diabetes Association; 2000:1-19
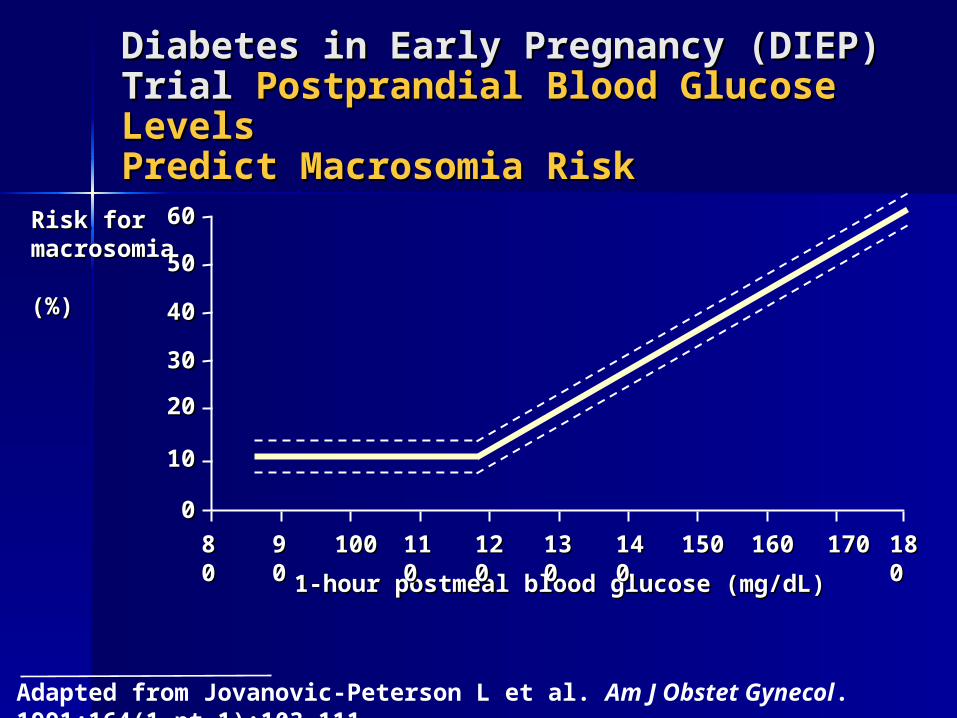
Diabetes in Early Pregnancy (DIEP) Diabetes in Early Pregnancy (DIEP) Trial Trial Postprandial Blood Glucose Postprandial Blood Glucose Levels Levels Predict Macrosomia RiskPredict Macrosomia Risk
Adapted from Jovanovic-Peterson L et al. Am J Obstet Gynecol. 1991;164(1 pt 1):103-111
1-hour postmeal blood glucose (mg/dL)1-hour postmeal blood glucose (mg/dL)
Risk for Risk for macrosomia macrosomia (%)(%)
8080
6060
9090 100100 110110 120120 130130 140140 150150 160160 170170 180180
5050
4040
3030
2020
1010
00
Management of Management of Diabetes in PregnancyDiabetes in Pregnancy Type 1 Type 1
– Multiple daily injectionsMultiple daily injections– Insulin pumpInsulin pump
Type 2 Type 2 – Change to insulin if on oral agentsChange to insulin if on oral agents– Insulin pumpInsulin pump
Multiple Daily Multiple Daily InjectionsInjections Combination of intermediate or Combination of intermediate or
longer acting insulin with rapid longer acting insulin with rapid insulininsulin– NPHNPH– LantusLantus– AnalogAnalog
Usually require 4-6 injections Usually require 4-6 injections dailydaily
Management of Management of Diabetes in PregnancyDiabetes in Pregnancy Monitor BG pre and 2 hrs post Monitor BG pre and 2 hrs post
mealmeal Calculate premeal rapid insulin Calculate premeal rapid insulin
based on carbohydrate intakebased on carbohydrate intake Calculate correction for premeal Calculate correction for premeal
elevated glucose elevated glucose Discourage postprandial correctionDiscourage postprandial correction
Insulin PumpInsulin Pump Advantages: Advantages: More physiologic than MDIMore physiologic than MDI
– Programmable bolus reduces risks for Programmable bolus reduces risks for hypoglycemia, post-meal hypoglycemia, post-meal hyperglycemia and glucose excursionshyperglycemia and glucose excursions
Allows for greater flexibility with Allows for greater flexibility with diet and lifestylediet and lifestyle
Increased motivation promotes Increased motivation promotes better controlbetter control
Insulin PumpInsulin Pump Disadvantages Disadvantages Requires increased patient Requires increased patient
responsibility and motivationresponsibility and motivation Risk of rapid onset ketoacidosis if Risk of rapid onset ketoacidosis if
catheter becomes dislodged or catheter becomes dislodged or site infectionsite infection
Mechanical problems with pumpMechanical problems with pump Infusion site limited in later Infusion site limited in later
pregnancypregnancy
Sensor Augmented Sensor Augmented PumpingPumping Advantages Advantages Decreased risk of glucose Decreased risk of glucose
excursions and hypoglycemiaexcursions and hypoglycemia Provides instant informationProvides instant information Allows for greater flexibility to Allows for greater flexibility to
diet and lifestylediet and lifestyle Reduces number of self-Reduces number of self-
monitored glucose testsmonitored glucose tests
Sensor Augmented Sensor Augmented PumpingPumping Disadvantages Disadvantages Not as accurate as glucose results Not as accurate as glucose results
by fingerstickby fingerstick ““Too much data”Too much data” Expensive and not always Expensive and not always
covered by insurancecovered by insurance Requires another siteRequires another site AlarmsAlarms
American Diabetes Association. Diabetes Care. 2004;27(suppl 1):S88-S90Metzger BE, Coustan DR. Diabetes Care. 1998;21(suppl 2):B161-B167
Mainstay of treatment is medical nutrition therapy Mainstay of treatment is medical nutrition therapy (MNT)(MNT)
Add insulin if MNT does not maintain normoglycemiaAdd insulin if MNT does not maintain normoglycemia If untreated, associated with:If untreated, associated with:
– Late-term intrauterine fetal deathLate-term intrauterine fetal death– Fetal macrosomia Fetal macrosomia – Neonatal hypoglycemia and/or jaundiceNeonatal hypoglycemia and/or jaundice– Maternal hypertensionMaternal hypertension– Future diabetes and/or obesity in childFuture diabetes and/or obesity in child
Diabetes and PregnancyDiabetes and Pregnancy Gestational Diabetes Gestational Diabetes MellitusMellitus
Glucose intolerance of variable degree with onset or first recognition during pregnancy
Gestational DiabetesGestational Diabetes Approximately 7% of all Approximately 7% of all
pregnancies are complicated by pregnancies are complicated by GDMGDM
Translates to over 200,000 cases Translates to over 200,000 cases annually(1)annually(1)
Approximately 42,000 births in Approximately 42,000 births in Connecticut in 2008(2)Connecticut in 2008(2)
2980 complicated by GDM2980 complicated by GDM (1)(1) Diabetes Care, Vol.33, Supp. 1, Jan. Diabetes Care, Vol.33, Supp. 1, Jan.
20102010 (2) Connecticut Vital Statistics, 2008 (2) Connecticut Vital Statistics, 2008
Gestational Diabetes Gestational Diabetes
Glucose intolerance of varying Glucose intolerance of varying severity, with onset or first severity, with onset or first recognition during the current recognition during the current pregnancy.pregnancy.
Currently diagnosed using two Currently diagnosed using two step methodstep method
Diagnostic screening between 24-Diagnostic screening between 24-28 weeks gestation28 weeks gestation
Diagnosis of GDMDiagnosis of GDM
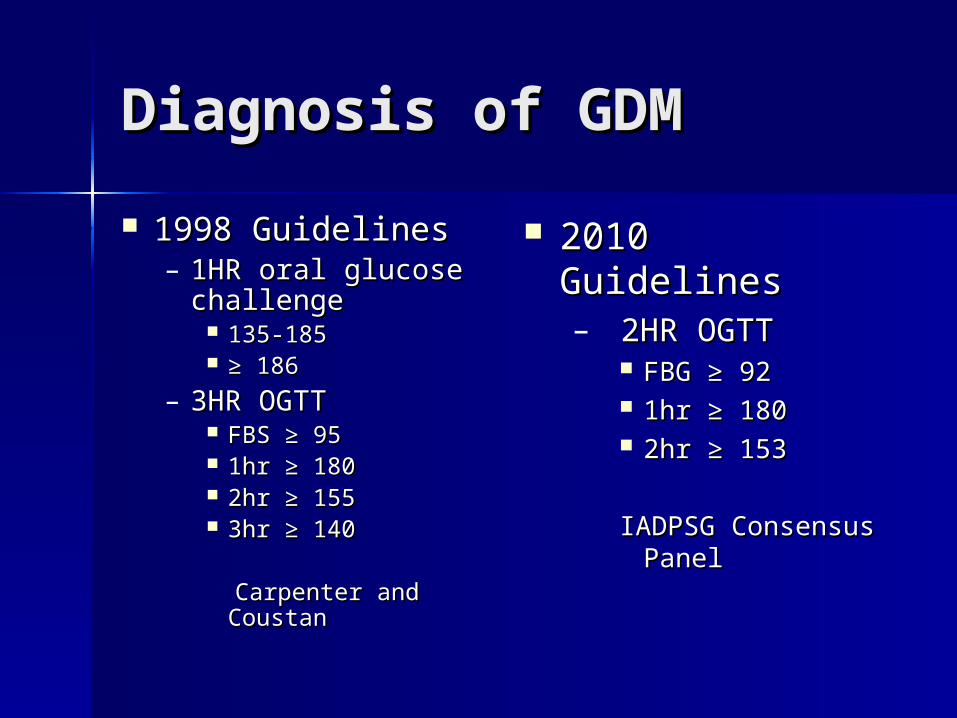
1998 Guidelines1998 Guidelines– 1HR oral glucose 1HR oral glucose
challengechallenge 135-185135-185 ≥ ≥ 186186
– 3HR OGTT3HR OGTT FBS FBS ≥ 95≥ 95 1hr ≥ 1801hr ≥ 180 2hr ≥ 1552hr ≥ 155 3hr ≥ 1403hr ≥ 140
Carpenter and CoustanCarpenter and Coustan
2010 Guidelines2010 Guidelines– 2HR OGTT 2HR OGTT
FBG FBG ≥ 92≥ 92 1hr ≥ 1801hr ≥ 180 2hr ≥ 1532hr ≥ 153
IADPSG Consensus IADPSG Consensus Panel Panel
Managing GDMManaging GDM
Lifestyle modifications:Lifestyle modifications:– Medical Nutrition TherapyMedical Nutrition Therapy– ExerciseExercise
Self-monitoring blood glucoseSelf-monitoring blood glucoseFBS < 90mg/dl 2 hr postprandial <120mg/dlFBS < 90mg/dl 2 hr postprandial <120mg/dl
MedicationMedication– Oral agentsOral agents– InsulinInsulin
Medications in GDMMedications in GDM
InsulinInsulin– NPHNPH– AnalogsAnalogs– LantusLantus
Oral agentsOral agents– GlyburideGlyburide– MetforminMetformin
Physical Activity in GDMPhysical Activity in GDM• Can improve peripheral insulin resistance Can improve peripheral insulin resistance
and glucose levelsand glucose levels• Can obviate need for insulin Can obviate need for insulin • Encouraged for women with no obstetric Encouraged for women with no obstetric
contraindicationscontraindications• Avoid physical activity associated with Avoid physical activity associated with
maternal hypertension or fetal distress (eg, maternal hypertension or fetal distress (eg, resistance training, lower-body weight-resistance training, lower-body weight-bearing exercise) bearing exercise)
• Upper-body cardiovascular training is a good Upper-body cardiovascular training is a good optionoption
Jovanovic L, ed in chief. Medical Management of Pregnancy Complicated by Diabetes. 3rd ed.Alexandria, Va: American Diabetes Association; 2000:111-132Jovanovic-Peterson L et al. Am J Obstet Gynecol. 1989;161:415-419
Immediate Postpartum Immediate Postpartum
Insulin requirements disappearInsulin requirements disappear
Diabetes will disappear in 90% of Diabetes will disappear in 90% of
GDM cases.GDM cases.
Continue monitoring 24-48 hrs after Continue monitoring 24-48 hrs after delivery, as indicateddelivery, as indicated
Postpartum ConsiderationsPostpartum ConsiderationsLactation and NutritionLactation and Nutrition
Breastfeeding is recommendedBreastfeeding is recommended – Decreased risk of type 1 diabetes and infection in infantDecreased risk of type 1 diabetes and infection in infant– Promotes infant growth and developmentPromotes infant growth and development
Maintain pregnancy meal plan or develop postpartum plan to Maintain pregnancy meal plan or develop postpartum plan to meet added caloric requirements of breastfeedingmeet added caloric requirements of breastfeeding
Rapid weight loss is not advised; exercise is recommended Rapid weight loss is not advised; exercise is recommended
Insulin use must be continued if postpartum normoglycemia Insulin use must be continued if postpartum normoglycemia cannot be maintained with MNTcannot be maintained with MNT
Blood glucose concentrations may be variable in women with Blood glucose concentrations may be variable in women with type 1 diabetestype 1 diabetes– Test glucose frequentlyTest glucose frequently– Snack and/or adjust evening insulin to avoid nighttime Snack and/or adjust evening insulin to avoid nighttime
hypoglycemiahypoglycemia– Watch for hypoglycemia due to missed or delayed mealsWatch for hypoglycemia due to missed or delayed meals
Jovanovic L, ed in chief. Medical Management of Pregnancy Complicated by Diabetes. 3rd ed. Alexandria, Va: American Diabetes Association; 2000:67-86
Postpartum Postpartum RecommendationsRecommendations Self-monitoring Self-monitoring
– Fasting <100Fasting <100– 2 hr post-prandial <1402 hr post-prandial <140
Glucose testing 6-12 weeks post Glucose testing 6-12 weeks post deliverydelivery
Reclassification of diabetesReclassification of diabetes
Diabetes After Diabetes After PregnancyPregnancy 40-60% risk of developing Type 2 40-60% risk of developing Type 2
DM within 5-15 yearsDM within 5-15 years Approximately 20% continue with Approximately 20% continue with
abnormal glucose after deliveryabnormal glucose after delivery 66% risk of developing GDM in 66% risk of developing GDM in
subsequent pregnancysubsequent pregnancy
Diagnosing DiabetesDiagnosing Diabetes
ADA 2010 Diagnostic CriteriaADA 2010 Diagnostic Criteria– A1C A1C ≥ 6.5% or:≥ 6.5% or:– FPG ≥ 126mg/dl or:FPG ≥ 126mg/dl or:– Two-hour plasma glucose ≥ Two-hour plasma glucose ≥
200mg/dl or:200mg/dl or:– Classic symptoms of hyperglycemia Classic symptoms of hyperglycemia
or hyperglycemic crisis, a random or hyperglycemic crisis, a random glucose ≥200mg/dlglucose ≥200mg/dl
Diagnosing DiabetesDiagnosing Diabetes
New classificationsNew classifications Pre-diabetesPre-diabetes
– A1C 5.7% to 6.4%A1C 5.7% to 6.4%– 2 hr OGTT2 hr OGTT
FPG 100-126FPG 100-126 2 hr 140-1992 hr 140-199
Refer for nutrition counseling, Refer for nutrition counseling, weight loss and ongoing careweight loss and ongoing care