Embed Size (px)
Citation preview

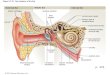
How To Rapidly and Effectively Examine the Ear Canal and Tympanic Membrane Clark W. Walker, MD, FACS
Lone Tree, CO

Audiologists and Otolaryngologists
• Denver Hearing Specialists, Lone Tree, Colorado– Diane Krieger-Arenberg, Au.D.– Lindsay Ward, Au.D.– Amanda Clark, Au.D.
• Naval Hospital, Great Lakes, Illinois– Michael Zenz, Au.D.
• The University of Colorado Health Sciences Center, Aurora, CO• Barbara Bell-Lehmkuhler, Au.D

Skill in OtoscopyClinical Skill Set
• Essential part of every exam.• Anticipate audiometric findings and know
when they do not correlate with your expectations.
• Predict when findings will interfere with accuracy of testing. Testing may need to be delayed until treated.

Skill in OtoscopyKnowledge of Terminology
• Know accepted terms to describe pathology.• Communicate to surgeons with confidence
about findings.• Be able to tell patients about findings and
anticipated options for treatment.• Document accurately for care consistency and
medico-legal purposes.

Skill in OtoscopyClinical Decision Making
• Identify patients that require ENT referral.• Know when it does and does not require
urgency.• Must be done rapidly in busy clinic setting.

Objectives
• Review a quick and easy method for a thorough otoscopic examination
• Describe confusing or problematic findings on otoscopy for each of the following anatomic areas and situations:– Ear canal – Tympanic membrane– Ossicles and middle ear structures– Post-operative appearance and findings






• El Sw

Acute Otitis Media• Purulence• Inflammation demonstrated
by engorged vessels• After infection resolves, it
will leave an effusion which takes weeks to months to resolve
• The decision of when to treat with antibiotics is complex and depends on the age of the patient and severity of symptoms

Blood Flow in the TM• Am J Otol. 1990 Jul;11(4):266-71.• Analysis of blood flow in the tympanic membrane: the use of intravital fluorescence microscopy.• Triana RJ, Prazma J, Carrasco VN, Pillsbury HC.• Source
• Division of Otolaryngology/Head and Neck Surgery, University of North Carolina School of Medicine, Chapel Hill 27599-7070.
• The blood supply of the TM is derived from the manubrial plexus and the peripheral plexus of vessels.
• The manubrial artery divides and branches into a series of arcading vessels that extend towards the periphery of the TM

Blood Flow in the TM• The vascular supply of the rat tympanic membrane• Nils Albiin, • Sten Hellström, • Bengt Salén, • Lars-Eric Stenfors, • Staffan Wirell• Article first published online: 8 FEB 2005• DOI: 10.1002/ar.1092120103
• The branches of the external carotid artery in the external auditory meatus were found to vascularize (1) the pars flaccida, (2) the manubrial part of the pars tensa, and (3) the junction between the fibrocartilaginous ring of the TM and the tympanic sulcus of the temporal bone.
• Even under mechanical stimulation, a large portion of the pars tensa seemed to be devoid of vessels. The nutrition of this part may be served by diffusion, with nutrients originating from the vessels in the tympanal rim and along the handle of the malleus

TM Injection/Inflammation




Tympanosclerosis
• A complication of otitis media in which acellular hyalin and calcified deposits accumulate within the tympanic membrane and the submucosal middle ear. In most patients, these plaques are clinically insignificant and cause little or no hearing impairment.
• Tympanosclerotic plaques within the tympanic membrane appear as a semicircular crescent or horseshoe-shaped white plaque within the tympanic membrane
• otologytextbook.com/tympanosclerosis.htm

Scar Plaque
Tympanosclerosis
• Bright white• Usually surrounded by
normal appearing TM• Move with
pneumotoscopy when TM intact
• Does not affect tympanogram


Wrinkling• Eur Arch Otorhinolaryngol. 1995;252(2):76-82.
• Structural changes in the rat tympanic membrane following repeated pressure loads .• Magnuson K, Hellström S, Magnuson B.• Source• Department of Otorhinolaryngology, University of Umeå, Sweden.
• Rats exposed to alternating negative pressure and atmospheric pressure to replicate the clinical situation found in patients with chronic sniffing habits and chronic middle ear disease.
• Histological studies demonstrated that the pars flaccida was wrinkled and the loose connective tissue contained large fibroblasts with their long axes lying in a disorganized manner.
• The cells of the keratinizing epithelium were thicker than normal and mitoses were seen. Epithelial crypts filled with keratin were numerous along the epithelium In the pars tensa, all layers were thicker than normal. These findings demonstrate that repeated pressure loading can create structural changes in the tympanic membrane

Wrinkled TM

Retractions• Present with persistent
eustachian tube dysfunction
• Middle ear gasses get resorbed
• When the TM retracts, it can put pressure on the ossicles leading to erosion and conductive hearing loss
• Skin must be able to slough and move out the canal with cerumen

Retraction• The surgical management of the pars tensa retraction pocket in the child — results following simple excision and ventilation
tube insertion • S. P. A. Blaney a, P. Tierneyb and D. A. Bowdler , b
a Department of Otorhinolaryngology, Royal Sussex County Hospital, Eastern Road, Brighton BN2 5BE, UKb Department of Otorhinolaryngology, University Hospital Lewisham, Lewisham High Street, London SE13 6LH, UK Received 28 January 1999; revised 29 June 1999; accepted 30 June 1999. Available online 20 October 1999.
• Retraction pockets of the pars tensa formed due to poor mesotympanic ventilation can result in chronic infection, ossicular damage and even acquired cholesteatoma




Retraction/Atelectasis

• Mi Po

Retraction/Atelectasis

Cholesteatoma• Trapped epithelium cannot
properly migrate out the ear canal.
• Persistent drainage• Skin trapped in deep retractions
cannot slough properly (Primary Cholesteatoma)
• Can arise from epithelial rests (remants) in the middle ear without a retraction behind an intact TM (Congenital cholesteatoma)
• Continues to enlarge and acts like a tumor
• Pressure and enzymes cause erosion of bone

Acquired Cholesteatoma• [Middle ear cholesteatoma: present-day concepts of etiology and pathogenesis]• [Article in Lithuanian] Lesinskas E, Kasinskas R, Vainutiene V.• Vilniaus universiteto ligonines Santariskiu klinikos Ausu, nosies, gerkles ligu klinika, Santariskiu 2, 2021 Vilnius. [email protected]
• J. Cruveilhier described cholesteatoma as the "pearly" tumor of the middle ear in 1828
• Four basic theories present the pathogenesis of acquired cholesteatoma: – Invagination of the tympanic membrane (retraction pocket
cholesteatoma)– basal cell proliferation– epithelial in-growth through a perforation (the immigration theory)– Squamous metaplasia of middle ear epithelium

Congenital Cholesteatoma• Congenital cholesteatoma: 20 years' experience at The Children's Hospital of Philadelphia • William P. Potsic MD, S. Bruce Korman MD, Daniel S. Samadi MD and Ralph F. Wetmore MD
The Children's Hospital of Philadelphia and the University of Pennsylvania School of Medicine.
• Objective: We report our experience with congenital cholesteatoma over a span of 20 years with an emphasis on presenting characteristics and predictors of outcome. Methods: We conducted a retrospective review from 1981 through 2000. Results: One hundred seventy-two congenital cases were identified in 167 patients. Five patients had bilateral disease. The majority (72%) were found in boys,
with an average age of 5.0 years. Hearing loss was slight to moderate. When confined to 1 quadrant, cholesteatoma was anterosuperior in 82% of cases; 47% had cholesteatoma in 2 or more quadrants. Ossicular chain involvement was found in 43% of all cases, and mastoid extension was evident in 23%. The rate of recurrent disease was directly related to the extent and number of quadrants involved. Conclusion: To our knowledge, this is the largest series of congenital cholesteatomas to be reported. This review confirms the male predominance and predilection for the anterosuperior quadrant. The extent of cholesteatoma and its relation to residual disease should be used as a guide for planning a second-look procedure. (Otolaryngol Head Neck Surg 2002;126:409-14.)




Perforations• Shiny middle ear mucosa
visible through the perforation
• Be able to draw quadrant location and give percentage
• Refer acute injury immediately if vertiginous
• Even large perforations can spontaneously heal.
• Refer if not healed after two weeks

Perforation Healing• Otol Neurotol. 2005 Nov;26(6):1100-6.• Fresh tympanic membrane perforations heal without significant loss of strength.• Rahman A, Hultcrantz M, Dirckx J, Margolin G, von Unge M.• Source• Center for Hearing and Communication Research and Department of Otorhinolaryngology, Karolinska University Hospital and Institute, Stockholm, Sweden.
• The strength of the spontaneously healed tympanic membrane after myringotomy was not significantly impaired.
• The site of the perforation became significantly thickened at 2 and 4 weeks post-myringotomy.
• This information is of clinical importance, because recently closed perforations will be challenged by pressure gradient in everyday life

Healed Perforation

Epithelial Migration J Otolaryngol. 1991 Feb;20(1):30-2. Links
– Epithelial migration in the external auditory canal and the movement of the chondro-osseous junction.– Cecire AA, Gibson WP.– Department of Surgery (Otolaryngology), University of Sydney, New South Wales, Australia.
– Epithelial migration occurs in a lateral direction from the tympanic membrane to the external auditory canal. The underlying mechanism which determines the direction of this laterally directed movement has not been elucidated.
– Paralysis of the peri-auricular muscles does not alter the time taken for skin migration in the external auditory canal.


Cerumen Formation
• Roeser and Ballachanda (J Am Acad Audiol 1997 Dec; 8(6):391-400) are simplistically quoted in the abstract stating “Two types of glands are found in the outer third of the human earcanal: sebaceous glands that produce sebum and modified apocrine glands that produce sweat. Together these substances make up cerumen…”.

Cerumen Formation
• Roland et al (Otol Head and Neck Surg 2008 Sep; 139 (3 suppl 1) S1-21) in the article entitled “Clinical practice guideline: Cerumen Impaction” state “Cerumen forms when glandular secretions from the outer one-third of the ear canal mix with exfoliated squamous epithelium.” They also state “Cerumen is defined as a mixture of secretions (sebum together with secretions from modified apocrine sweat glands) and sloughed epithelial cells, and is a normal substance present in the external auditory canal. As cerumen migrates laterally, it
may mix with hair and other particulate matter.”

Cerumen Formation
• Guest et al. (Q J Med 2004; 97:477-488) state in “Impacted cerumen: composition, production, epidemiology and Management” that “Cerumen is composed of desquamated sheets of corneocytes, originating from the deep and superficial external auditory canal, mixed with glandular secretions.” They give an excellent summary of the composition of cerumen which includes, but is not limited to: fatty acids from sebaceous glands, keratin sheets, lipids, peptides, cholesterol, pigment granules, etc.

Epithelial Migration• Epithelial migration of the lining of the EAC is a well-known
phenomenon and is essential for the self-cleansing mechanism of this structure. In most cases, the epicenter of this migratory process appears to reside in the vicinity of the umbo of the tympanic membrane. The epithelial migration takes place at a rate of approximately 0.07mm/day and serves to cleanse the canal of debris, foreign bodies, and bacteria.
• TITLE: EXTERNAL AUDITORY CANAL LESIONSSOURCE: Department of Otolaryngology, UTMB: Grand Rounds Presentation DATE: April 9, 1997 RESIDENT PHYSICIAN: Kyle Kennedy, M.D. FACULTY PHYSICIAN: Jeffrey Vrabec, M.D.
SERIES EDITOR: Francis B. Quinn, Jr., M.D.


Post-Op Appearance


• Ma Wi