Embed Size (px)
Citation preview

How to Read a Chest X Ray13 authors | 52 revisions | Last updated: September 25, 2012
Article
Edit Discuss
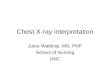
Normal chest x-ray. A=Airway; B=Bone, C=Cardiac silhouette, D=Diaphragm, E=Edge of the heart, F=Field of lung, G=Gastric bubble, H=Hilum of lung.
You have probably seen a chest x-ray (chest radiograph), or might even have had one taken. Have you ever wondered how to read a chest x-ray? Here is a quick and easy approach by following these simple steps and using the mnemonic 'A,B,C,D,E,F,G,H,I'.When looking at a radiograph, remember that it is a 2-dimensional representation of a 3-dimensional object. Height and width are maintained, but depth is lost. The left side of the film represents the right side of the individual, and vice versa. Air appears black, fat appears gray, soft tissues and water appear as lighter shades of gray, and bone and metal appear white. The denser the tissue, the whiter it will appear on x-ray. Denser tissues appear radiopaque, bright on the film; less dense tissues appear radiolucent, dark on the film.
Edit Steps1.1

Check the patient's name. Above all else, make sure you are looking at the correct chest x-ray first.
2.2
Read the date of the chest radiograph. Make special note of the date when comparing older radiographs (always look at older radiographs if available). The date the radiograph is taken provides important context for interpreting any findings. For example, a mass that has become bigger over 3 months is more significant than one that has become bigger over 3 years.
3.3
Note the type of film (while this article assumes you are looking at a chest x-ray, practice noting if it is a plain film, CT, angiogram, MRI, etc.) For chest x-ray, there are several views as follows:
o The standard view of the chest is the posteroanterior radiograph, or "PA chest." Posteroanterior refers to the direction of the x-ray traversing the patient from posterior to anterior. This film is taken with the patient upright, in full inspiration (breathed in all the way), and the x-ray beam radiating horizontally 6 feet away from the film.
o The anteroposterior (AP) chest radiograph is obtained with the x-ray traversing the patient from anterior to posterior, usually obtained with a portable x-ray machine from very sick patients, those unable to stand, and infants. Because portable x-ray units tend to be less powerful than regular units, AP radiographs are generally taken at shorter distance from the film compared to PA radiographs. The farther away the x-ray source is from the film, the sharper and less magnified the image. (You can confirm this by placing your hand about 3 inches from a desk, shining a lamp above it from various distances, and observing the shadow cast. The shadow will appear sharper and less magnified if the lamp is farther away.) Since AP radigraphs are taken from shorter distances, they appear more magnified and less sharp compared to standard PA films.

o
Lateral chest x-ray.
The lateral chest radiograph is taken with the patient's left side of chest held against the x-ray cassette (left instead of right to make the heart appear sharper and less magnified, since the heart is closer to the left side). It is taken with the beam at 6 feet away, as in the PA view.
o An oblique view is a rotated view in between the standard front view and the lateral view. It is useful in localizing lesions and eliminating superimposed structures.
o
Right lateral decubitus chest x-ray showing pleural effusion. The A arrow indicates "fluid layering" in the right chest. The B arrow indicates the width of the right lung. The volume of useful lung is reduced because of the collection of fluid around the lung.
A lateral decubitus view is one taken with the patient lying down on the side. It helps to determine whether suspected fluid (pleural effusion) will layer out to the bottom, or suspected air (pneumothorax) will rise to the top. For example, if pleural fluid is suspected in the left lung, check a left lateral decubitus view (to allow the fluid to layer to the left side). If air is suspected in left lung, check a rightlateral decubitus view (to allow the air to rise to the left side).
4.4

Look for markers: 'L' for Left, 'R' for Right, 'PA' for posteroanterior, 'AP' for anteroposterior, etc. Note the position of the patient: supine (lying flat), upright, lateral, decubitus.
5.5
Note the technical quality of film.
o Exposure: Overexposed films look darker than normal, making fine details harder to see; underexposed films look whiter than normal, and cause appearance of areas of opacification. Look for intervertebral bodies in a properly penetrated chest x-ray. An under-penetrated chest x-ray cannot differentiate the vertebral bodies from the intervertebral spaces, while an over-penetrated film shows the intervertebral spaces very distinctly.
To assess exposure, look at the vertebral column behind the heart on the frontal view. If detailed spine and pulmonary vessels are seen behind the heart, the exposure is correct. If only the spine is visible, but not the pulmonary vessels, the film is too dark (overexposed). If the spine is not visible, the film is too white (underexposed).
o Motion: Motion appears as blurred areas. It is hard to find a subtle pneumothorax if there is significant motion.
o Rotation : Rotation means that the patient was not positioned flat on the x-ray film, with one plane of the chest rotated compared to the plane of the film. It causes distortion because it can make the lungs look asymmetrical and the cardiac silhouette disoriented. Look for the right and left lung fields having nearly the same diameter, and the heads of the ribs (end of the calcified section of each rib) at the same location to the chest wall, which indicate absence of significant rotation. If there is significant rotation, the side that has been lifted appears narrower and denser (whiter) and the cardiac silhouette appears more in the opposite lung field.
6.6

Left tension pneumothorax. Note the large, well-demarcated area devoid of lung markings, and deviation of the trachea (airway) and the heart away from the affected side. The bright metallic spots are snaps for EKG readings.
Airway: Check to see if the airway is patent and midline. For example, in a tension pneumothorax, the airway is deviated away from the affected side. Look for thecarina, where the trachea bifurcates (divides) into the right and left main stem bronchi.
7.7
Fracture of the left clavicle.
Bones: Check the bones for any fractures, lesions, or defects. Note the overall size, shape, and contour of each bone, density or mineralization (osteopenic bones look thin and less opaque), cortical thickness in comparison to medullary cavity, trabecular pattern, presence of any erosions, fractures, lytic or blastic areas. Look for lucent and sclerotic lesions. A lucent bone lesion is an area of bone with a decreased density (appearing darker); it may appear punched out compared to surrounding bone. A sclerotic bone lesion is an area of bone with an increased density (appearing whiter). At joints, look for joint spaces narrowing, widening, calcification in the cartilages, air in the joint space, abnormal fat pads, etc.
8.8

Enlarged cardiac silhouette in a case of aortic dissection (blood fills the mediastinum). Note that the cardiac silhouette takes up more than half of the chest width. Characteristic of aortic dissection here is the enlarged mediastinum (labeled 1) and aortic arched (labeled 2).
Cardiac silhouette: Look at the size of the cardiac silhouette (white space representing the heart, situated between the lungs). A normal cardiac silhouette occupies less than half the chest width.
o Look for water-bottle-shaped heart on PA plain film, suggestive of pericardial effusion. Get an ultrasound or chest Computed Tomagraphy (CT) to confirm.
9.9
Left pleural effusion associated with left lower lobe pneumonia: note that the costophrenic angle is blunted, and the left diaphragm is raised compared to the right.
Diaphragms: Look for a flat or raised diaphragm. A flattened diaphragm may indicate emphysema. A raised diaphragm may indicate area of airspace consolidation (as in pneumonia) making the lower lung field indistinguishable in tissue density compared to the abdomen. The right diaphragm is normally higher than the left, due to the presence of the liver below the right diaphragm. Also look at the costophrenic angle (which should be sharp) for any blunting, which may indicate effusion (as fluid settles down). It takes about 300-500 ml of fluid to blunt the costophrenic angle.

10. 10
A) Normal chest radiograph; B) Q fever pneumonia affecting the lower and middle lobes of the right lung. Note the loss of the normal radiographic silhouette (contour) between the affected lung and its right heart border as well as between the affected lung and its right diaphragm border. This phenomenon is called thesilhouette sign.
Edges of heart; External soft tissues: Check the edges of the heart for the silhouette sign: a radioopacity obscuring the heart's border, in right middle lobe and left lingula pneumonia, for example. Also, look at the external soft tissues for any abnormalities. Note the lymph nodes, look for subcutaneous emphysema (air density below the skin), and other lesions.
11. 11
Right lower lobe pneumonia. Note the prominent air-bronchogram sign: air visualized in the peripheral intrapulmonary bronchi, due to an infiltrate or consolidation surrounding the bronchi.

Fields of the lungs: Look for symmetry, vascularity, presence of any mass, nodules, infiltration, fluid, bronchial cuffing, etc. If fluid, blood, mucous, or tumor, etc. fills the air sacs, the lungs will appear radiodense (bright), with less visible interstitial markings.
12. 12
Gastric bubble: Look for the presence of a gastric bubble, just below the heart; note whether it is obscured or absent. Assess the amount of gas and location of the gastric bubble. Normal gas bubbles may also be seen in the hepatic and splenic flexures of the colon.
13. 13
Enlarged lymph node in left hilum, in a case of carcinoid tumor.
Hila: Look for nodes and masses in the hila of both lungs. On the frontal view, most of the hilar shadows represent the left and right pulmonary arteries. The left pulmonary artery is always more superior than the right, making the left hilum higher. Look for calcified lymph nodes in the hilar, which may be caused by an oldtuberculosis infection.
14. 14

Breast implants.
Instrumentations: Look for any tubes, IV lines, EKG leads, surgical drains, prosthesis, etc.Ads by Google
The patient should be examined in full inspiration. This greatly helps the radiologist to determine if there are intrapulmonary abnormalities. The diaphragm should be found at about the level of the 8th - 10th posterior rib or 5th - 6th anterior rib on good inspiration.
Adequate penetration of the patient by radiation is also required for a good film. On a good PA film, the thoracic spine disc spaces should be barely visible through the heart but bony details of the spine are not usually seen. On the other hand penetration is sufficient that bronchovascular structures can usually be seen through the heart.
On the lateral view, you can look for proper penetration and inspiration by observing that the spine appears to be darken as you move caudally. This is due to more air in lung in the lower lobes and less chest wall. The sternum should be seen edge on and posteriorly you should see two sets of ribs.

Rotation
The technologists are usually very careful to x-ray the patient flat against the cassette. If there is rotation of the patient, the mediastinum may look very unusual. One can access patient rotation by observing the clavicular heads and determining whether they are equal distance
from the spinous process of the thoracic vertebral bodies.Rotation
The technologists are usually very careful to x-ray the patient flat against the cassette. If there is rotation of the patient, the mediastinum may look very unusual. One can access patient rotation by observing the clavicular heads and determining whether they are equal distance from the spinous process of the thoracic vertebral bodies.
This is a normal PA film without any rotation.

Magnification of clavicular head and spinous process alignment demonstrating a straight film.
Magnification of clavicular head and spinous process alignment demonstrating a straight film.

In this rotated film skin folds can be mistaken for a tension pneumothorax (blue arrows). Notice the skewed positioning of the heads of the clavicles (red arrows) and the spinous
processes.
In this rotated film skin folds can be mistaken for a tension pneumothorax (blue arrows). Notice the skewed positioning of the heads of the clavicles (red arrows) and the spinous
processes.

The basic diagnostic instance is to detect an abnormality. In both of the cases above, there is an abnormal opacity. It is most useful to state the diagnostic findings as specifically as possible, then try to put these together and construct a useful differential diagnosis using the clinical information to order it.
In each of the cases above, there is an abnormal opacity in the left upper lobe. In the case on the left, the opacity would best be described as a mass because it is well-defined. The case on the right has an opacity that is poorly defined. This is airspace disease such as pneumonia.
Mass vs. Infiltrate


Mediastinum and Lungs
The radiologist needs to know both the structures within the mediastinum forming the mediastinal margins and the lobes of the lungs forming the margins of the lungs along the mediastinum and chest wall. If a mass or pneumonia "silhouettes" (obscures) a part of the lung/mediastinal margin, the radiologist should be able to identify what part of the lung and what organ within the mediastinum are involved. The margins of the mediastinum are made up of the structures shown below. Trace the margin of the mediastinum with your eye all the way around the margin. Think of the mediastinal structures that comprise this interface. If the margin were abnormal you could diagnose the cause.

This image outlines the specific anatomy of the PA chest x-ray.
This image indicates the locations of each lung margin on chest x-ray.
Trace the margin of the lung with your eye in the image below thinking about what mediastinal structure and what lobe of the lung is present at
this margin.


Bronchi
A physician should absolutely know the anatomy of the bronchi. Look at the drawing on the left and compare it to the chest x-ray on the right. You can see that the major bronchi are visible if you look carefully. It may be beneficial to practice drawing the bronchi and labeling them until you are entirely familiar with their names and locations. The table below shows the segmental bronchi and their designated numbers.
A = Right Main Stem BronchusB = Right Upper Lobe Bronchus B1 = Apical Segmental Bronchus B2 = Anterior Segmental Bronchus B3 = Posterior Segmental BronchusC = Bronchus IntermediusD = Right Middle Lobe Bronchus D4 = Lateral Segmental Bronchus D5 = Medial Segmental BronchusE = Right Lower Lobe Bronchus E6 = Superior Segmental Bronchus E7 = Medial Basal Segmental Bronchus E8 = Anterior Basal Segmental Bronchus E9 = Lateral Basal Segmental Bronchus E10 = Posterior Basal Segmental BronchusF = Left Main Stem BronchusG = Left Upper Lobe Bronchus G1, G2 = Apicoposterior Segmental Bronchus G3 = Anterior Segmental BronchusH = Lingular Bronchus H4 = Superior Lingular Segmental Bronchus H5 = Inferior Lingular Segmental BronchusI = Left Lower Lobe Bronchus I6 = Superior Segmental Bronchus I7 = Medial Basal Segmental Bronchus I8 = Anterior Basal Segmental Bronchus I9 = Lateral Basal Segmental Bronchus I10 = Posterior Basal Segmental Bronchus
SMALP = "Suppose My Aunt Loves Peaches" is a helpful way to remember the segmental lower lobe bronchi.

Signs
Silhouette sign
One of the most useful signs in chest radiology is the silhouette sign. This was described by Dr. Ben Felson. The silhouette sign is in essence elimination of the silhouette or loss of lung/soft tissue interface caused by a mass or fluid in the normally air filled lung. In other words, if an intrathoracic opacity is in anatomic contact with, for example, the heart border, then the opacity will obscure that border. The sign is commonly applied to the heart, aorta, chest wall, and diaphragm. The location of this abnormality can help to determine the location anatomically.
Take a moment to review the makeup of the mediastinal margins and the lobes of the lungs that interface with the mediastinum. Use the back button on your browser to return here.
For the heart, the silhouette sign can be caused by an opacity in the RML, lingula, anterior segment of the upper lobe, lower aspect of the oblique fissure, anterior mediastinum, and anterior portion of the pleural cavity. This contrasts with an opacity in the posterior pleural cavity, posterior mediastinum, of lower lobes which cause an overlap and not an obliteration of the heart border. Therefore both the presence and absence of this sign is useful in the localization of pathology.

The right heart border is silhouetted out. This is caused by a pneumonia, can you determine which lobe the pneumonia affects?
(click image for answer)