Embed Size (px)
Citation preview
HP Provider Relations
February 2012
IHCP Updates
IHCP Updates February 20122
Agenda
– Objectives
– Revenue Code 513
– New provider types
– Dental cap
– 5010 implementation statistics
– Electronic Health Records (EHR)
– International Classification of Diseases, 10th Revision (ICD-10) implementation
– Return to provider claims
– Claim denials
– Helpful tools
– Questions
IHCP Updates February 20123
Objectives
– Understand billing requirements for revenue code 513
– Learn about new provider types and specialties, including birthing centers
– Know the current status of the ICD-10 implementation
– Be aware of the most recent changes to coverage and reimbursement
– Understand how to avoid returned claims

LearnBilling Requirements for Revenue Code 513
IHCP Updates February 2012 5
Revenue Code 513 – Clinic/PsychiatricSee bulletin BT201157
– Applies to claims for dates of service on or after January 1, 2012 for therapy services rendered in an outpatient facility and billed on the UB-04 claim form.
– For outpatient claims with dates of service on or after January 1, 2012, providers will no longer bill individual, group, or family therapy with revenue code 510 – Clinic.
– Providers that continue to bill revenue code 510 for outpatient individual, group, or family therapy will be subject to post-payment review by the Indiana Health Coverage Programs (IHCP) Program Integrity Department.
IHCP Updates February 2012 6
Revenue Code 513 – Clinic/PsychiatricSee bulletin BT201157
– For family and group therapy codes, the IHCP will reimburse the lesser of the billed amount or a statewide flat fee of $20.40, per member, per session.
– Individual therapy codes will be reimbursed the lesser of the billed amount or a statewide flat fee of $40.80, per member, per session.
– The 5% reduction in effect for provider type 01 will apply to these rates at the time of processing.
IHCP Updates February 2012 7
Revenue Code 513 – Who does it affect?See bulletin BT201157
– This change applies to claims for Traditional Medicaid and Care Select members.
– For members enrolled in managed care, providers must contact the member’s managed care entity (MCE) for guidelines on billing outpatient therapy services, including instructions regarding billing bridge appointments using revenue code 513.
– This change does not apply to claims for members who are dually eligible for Medicare and Medicaid.• Providers must continue to bill Medicare for dually eligible members following Medicare
claim submission policy, which may include revenue code 510.

ExplainNew Provider Types
IHCP Updates February 2012 9
Birthing Center/CORF/IDTF/IDTF mobileSee bulletin BT201158
– In 2012, the IHCP will expand its list of eligible providers to allow birthing centers, comprehensive outpatient rehabilitation facilities (CORFs), independent diagnostic testing facilities (IDTFs), and mobile independent diagnostic testing facilities (IDTFs) to enroll as IHCP providers.
IHCP Updates February 2012 10
New Provider Types and SpecialtiesSee bulletin BT201158
– Birthing centers• Type 08 – Clinic
• Specialty 088 – Birthing Center
– Comprehensive Outpatient Rehabilitation Facility (CORF) • Type 04 – Rehabilitation facility
• Specialty 041 – Comprehensive Outpatient Rehab Facility
– Independent Diagnostic Testing Facility (IDTF)• Type 28 – Laboratory
• Specialty 282 – Independent Diagnostic Testing Facility
– Independent Diagnostic Testing Facility – mobile (IDTF)• Type 28 – Laboratory
• Specialty 283 – Independent Diagnostic Testing Facility Mobile

InformDental Cap
IHCP Updates February 201212
Dental Cap Removed
– Effective November 4, 2011, the U.S. District Court for the Northern District of Indiana issued a preliminary injunction enjoining the agency from enforcing 405 IAC 5-14-1(b).
– The monetary cap of $1,000 for dental services has been removed in accordance with the Court’s order, subject to all other requirements, pending further order of the Court.

Inform5010 Implementation status
IHCP Updates February 201214
Status Update
• On November 17, 2011, the Centers for Medicare & Medicaid Services (CMS) announced that it will delay enforcement of the required HIPAA new ASC X12 Version 5010 and the NCPDP D.0
• Delay was set for electronic healthcare claims until March 31, 2012.
• This was not a delay of the January 1, 2012 compliance date. It was a delay in enforcing penalties associated with providers' noncompliance.
• The process to be considered for the grace period for 5010 noncompliance was to submit an email containing the request to the [email protected] mailbox by December 27, 2011.

DescribeEHR Incentive Program
IHCP Updates February 201216
EHR Incentive Program
– The American Recovery and Reinvestment Act (ARRA) of 2009 provides for incentive payments for eligible professionals (EP), and eligible hospitals (EH) who are meaningful users of certified electronic health record (EHR) technology.
– EPs include the following:• Doctor of medicine or osteopathy• Dentist• Certified nurse midwife• Nurse practitioner (advanced practice nurse)• Physician assistants (PAs) when practicing at a Federally Qualified Health Center
(FQHC) or rural health clinic (RHC) that is led by a PA
– EHs include:• Acute care hospital• Children’s hospital• Critical access hospital (CAH)
IHCP Updates February 2012 17
Meaningful use of EHR
– CMS has determined “meaningful use” focuses on establishing the functionalities in certified EHR technology that allow for the following:• Continuous quality improvement
• Ease of information exchange
– This includes:• Electronically capturing health information in a structured format
• Using that information to track key clinical conditions and communicating that information for care coordination purposes
• Implementing clinical decision support tools to facilitate disease and medication management using EHRs to engage patients and families
• Reporting clinical quality measures and public health information
EHR Incentive Program
IHCP Updates February 2012 18
– EPs and EHs register for the incentive program through a two-step process:1. Providers must register using the CMS Registration and Attestation system and
select Indiana as their state
2. Providers register their EHR system using the Provider Profile feature of Web interChange
EHR Incentive Program
IHCP Updates February 2012 19
EHR Incentive ProgramEligible Professional (EP)
– Per federal rule, EPs must register for EHR incentive payments no later than calendar year (CY) 2016.
– EPs must meet patient volume criteria as follows:• EPs, other than pediatricians, must have a minimum 30 percent patient volume
attributable to Medicaid funded services; for pediatricians, the patient volume minimum requirement is 20 percent.
• Practice predominantly in an FQHC or RHC and have a minimum 30 percent patient volume attributable to needy individuals.
– Hospital-based providers are not eligible for the EHR incentive program.• An EP is considered to be hospital-based when 90 percent of his or her services are
furnished in a hospital inpatient or emergency room setting.
IHCP Updates February 2012 20
EHR Incentive ProgramEligible Professional (EP)
– EPs may not receive EHR incentive payments from both Medicare and Medicaid programs in the same year.
– If an EP qualifies for EHR incentive payments from both Medicare and Medicaid programs, the EP elects to receive payments from only one program.
– After the EP qualifies for the EHR incentive payment under one program, but before 2015, an EP can switch between the Medicare and Medicaid programs one time.

UpdateICD-10
IHCP Updates February 2012 22
ICD-10Implementation October 1, 2013
– January 16, 2009, the Department of Health and Human Services (HHS) released a final rule mandating Health Insurance Portability and Accountability Act (HIPAA)-covered entities to implement ICD-10 for medical coding by October 1, 2013.
– ICD-10 codes must be used on all HIPAA transactions including Outpatient and Professional claims with dates of service (DOS) and Inpatient claims with dates of discharge (DOD) on or after October 1, 2013.
– ICD-10 does not affect Current Procedural Terminology®1 (CPT) coding.
– To accommodate ICD-10, the new transaction standard X12 version 5010 must be operational.
1 Current Procedural Terminology (CPT) is copyright 2010 American Medical Association. All rights reserved. CPT® is a registered trademark of the American Medical Association
1 Source: Center for Medicare & Medicaid Services (CMS) at www.cms.gov/icd10
IHCP Updates February 2012 23
ICD-10CMS Mandate
– Providers will not be able to continue to report ICD-9 codes for services provided on or after October 1, 2013.
– The last regular annual update to both ICD-9 and ICD-10 code sets was made on October 1, 2011.
– After October 1, 2012, there will be only limited code updates to both ICD-9 and ICD-10 code sets to capture new technology and new diseases.
– After October 1, 2013, there will be only limited code updates to ICD-10 code sets to capture new technologies and new diseases.• There will be no updates to ICD-9 on or after October 1, 2013, as the code set will no
longer be a HIPAA standard.
– On October 1, 2014, regular updates to the ICD-10 code sets will begin.
IHCP Updates February 2012 24
ICD-10FAQs
– What is the current implementation timeframe?• HP has completed the assessment for the MMIS system and is on target for the
October 1, 2013, implementation of the ICD-10 Compliance Project.
– Is there going to be a system freeze? If so, when?• No. There are no plans at this time to freeze claims processing.
– Will there be vendor testing? When?• Yes, there will be vendor testing that will include MCEs. Vendor testing is scheduled
to begin January 1, 2013.
– Will providers/vendors be able to use the ICD-9 codes after the October 1, 2013, implementation?• No, you must use ICD-10 codes for DOS or DOD on or after the October 1, 2013,
implementation date. There is no grace period.
IHCP Updates February 2012 25
ICD-10Provider Readiness Surveys
– The second provider survey was released on February 7, 2012 and closed on February 21, 2012.
– Survey results will help us help you, by tracking your progress and capturing your issues.
– HP and the Family and Social Services Administration (FSSA) have committed to surveying contracted vendors and IHCP providers every 90 days through August 2013.
– The purpose of continuously surveying contracted vendors and IHCP providers is to understand where they are in preparation for the change to ICD-10 and to track progress.
– Information about these surveys is available in the IHCP Newsletters available on indianamedicaid.com.
IHCP Updates February 2012 26
ICD-10Advice to IHCP providers
– Now is the time to begin the ICD-10 planning process, if you haven’t already.
– If you have not been contacted by your software vendor and/or clearinghouse about ICD-10 readiness, be proactive and contact them.
– The IHCP has posted ICD-10 information pages at indianamedicaid.com which includes:• ICD-10 Information page with links to relevant websites.
• ICD-10 FAQs page with ICD-10 questions and answers posed by providers, vendors, and stakeholders.
• ICD-10 Decisions page with explanations of decisions that have been made and issues for your consideration. Providers, vendors, and stakeholders are encouraged to weigh in on these issues during the open (posted) discussion period.

ExploreReturned Claims
IHCP Updates February 2012 28
Claims Returned to ProvidersJanuary 2012
– 2,879 claims were returned to providers by the HP mailroom because of errors identified during the claim preparation process. • 32% - member number invalid
• 14% - Medicare Replacement Claims
– These claims do not get scanned or keyed by HP data entry
– 3,686 claims were returned by HP data entry due to missing or invalid information that is essential to processing the claim. • 53% - CMS-1500 claims with missing or invalid National Provider identifier (NPI),
taxonomy and ZIP Code.
IHCP Updates February 201229
How do you avoid returned claims?
– Verify Member ID when registering members.
– Include Medicare replacement plan billing information.
• CMS-1500 claim forms−Write “Medicare Replacement Plan” on the top of the claim and on the
replacement plan EOB.
−DO NOT complete field 22.
−Enter the replacement plan prior payment in field 29.
• UB-04 claim forms−Write “Medicare Replacement Plan” on the top of the claim and on the
replacement plan explanation of benefits (EOB).
−DO NOT complete field 39 with coinsurance or deductible information.
−Enter the words “Replacement Plan” in field 50b.
−Enter the amount paid by the replacement plan in field 54b.
IHCP Updates February 201230
How do you avoid returned claims?
– Verify the NPI, taxonomy and ZIP Code are correct.
• CMS-1500−Enter the ZIP Code + 4 in field 33 and verify the information entered
matches the service location found in Provider Profile on Web interChange.
−Enter the NPI for the Billing or Group Provider enrolled with the IHCP in field 33a.
−Enter the taxonomy code (if needed) in field 33b and verify the information entered matches the provider profile on Web interChange.

ReducePaper Claims
IHCP Updates February 201232
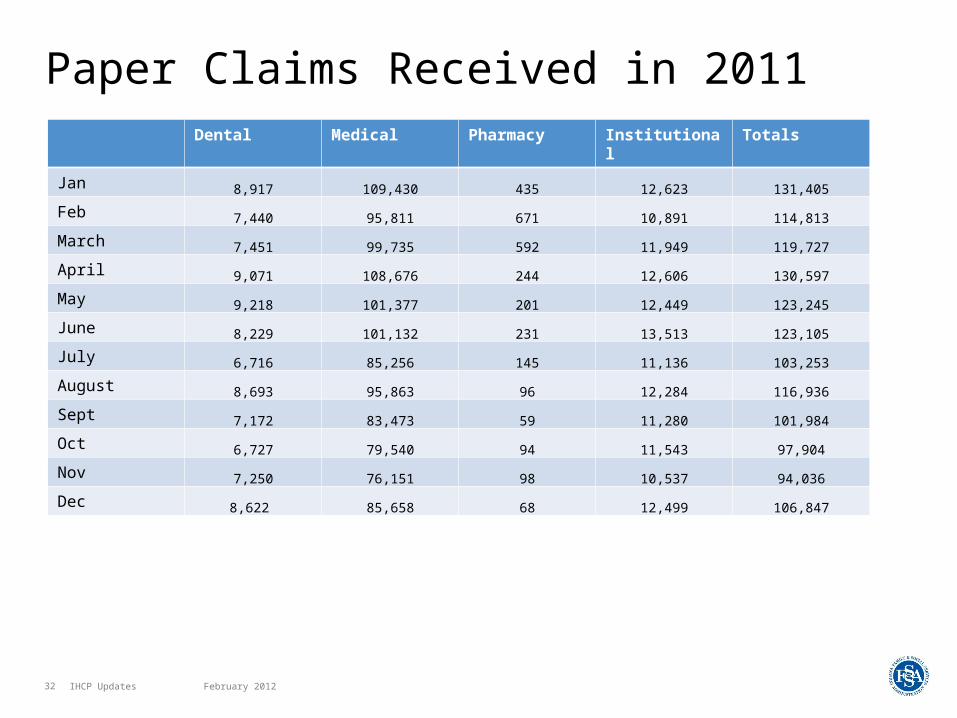
Paper Claims Received in 2011Dental Medical Pharmacy Institutional Totals
Jan 8,917 109,430 435 12,623 131,405
Feb 7,440 95,811 671 10,891 114,813
March 7,451 99,735 592 11,949 119,727
April 9,071 108,676 244 12,606 130,597
May 9,218 101,377 201 12,449 123,245
June 8,229 101,132 231 13,513 123,105
July 6,716 85,256 145 11,136 103,253
August 8,693 95,863 96 12,284 116,936
Sept 7,172 83,473 59 11,280 101,984
Oct 6,727 79,540 94 11,543 97,904
Nov 7,250 76,151 98 10,537 94,036
Dec 8,622 85,658 68 12,499 106,847

HelpTop Claim Denials
IHCP Updates February 201234
Top 5 Claim Denials
– EOB 558 - Coinsurance and deductible amount is missing indicating that this is not a crossover claim.• Coinsurance and deductible amounts must be included on all crossover claims.
– EOB 593 - At least one detail submitted contains Medicare COB data, resulting in a review of all detail COB data.• When submitting Medicare crossover claims, ensure that all Medicare coordination of
benefits (COB) information is on the claim for all details. This applies to CMS-1500 claims.
– EOB 5001 - This is a duplicate of another claim.• Review claims to see if any billed services were previously paid. Verify previous claim
payments and denials using Web interChange to avoid erroneous rebilling of paid claims.
IHCP Updates February 201235
Top 5 Claim Denials
– EOB 4021 - Procedure code is not covered for the dates of service for the program billed.• Verify that the procedure code is covered for the dates of service via the Fee Schedule
at indianamedicaid.com.
– EOB 2510 - Member is eligible for Medicare B/D.• Claim must be billed to Medicare before billing the IHCP.

Find HelpResources Available
IHCP Updates February 201237
Helpful Tools
– IHCP Web site at indianamedicaid.com
– IHCP Provider Manual (Web, CD-ROM, or paper)
– IHCP Fee Schedule
– Customer Assistance• 1-800-577-1278, or (317) 655-3240 in the Indianapolis
local area
– Written Correspondence• P.O. Box 7263
Indianapolis, IN 46207-7263
– Provider field consultant • provider.indianamedicaid.com/contact-us/provider-
relations-field-consultants.aspx
Q&A