Embed Size (px)
DESCRIPTION
HPB DAY. Plan today 4 cases Images Present range of approaches Discussion. 38 year old female, 6 month history of recurrent attacks of severe epigastric pain -> back. Possibly dark urine at times USS…. - PowerPoint PPT Presentation
Citation preview

HPB DAYHPB DAY
Plan todayPlan today
•4 cases4 cases
•ImagesImages
•Present range of approachesPresent range of approaches
•DiscussionDiscussion

38 year old female, 6 month history of 38 year old female, 6 month history of recurrent attacks of severe epigastric pain recurrent attacks of severe epigastric pain -> back. Possibly dark urine at times-> back. Possibly dark urine at times
USS…USS…
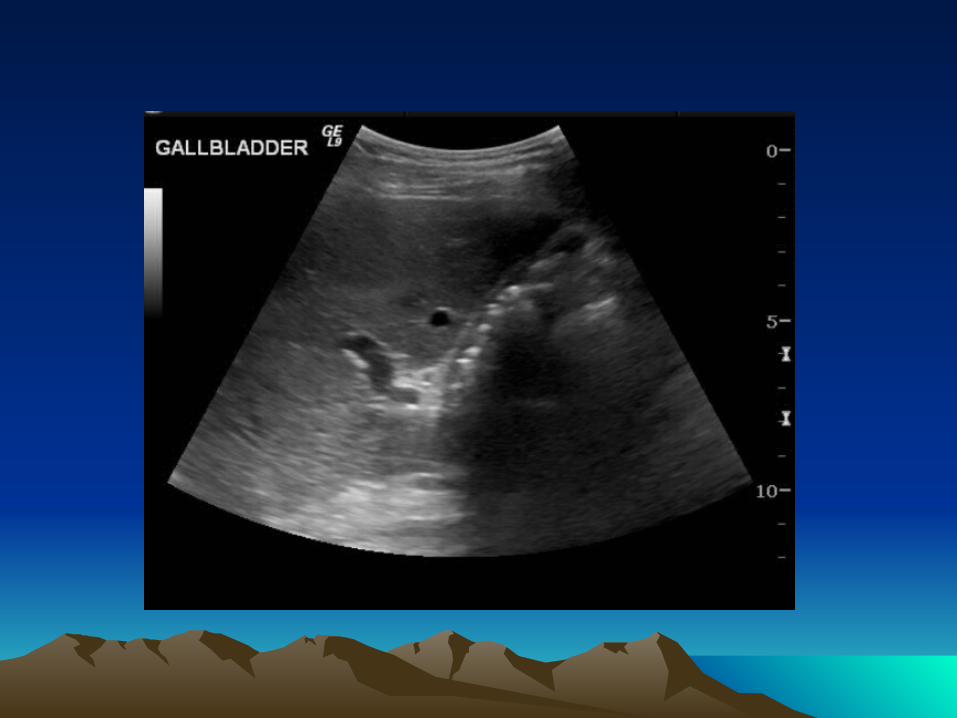

38 year old female, 6 month history of 38 year old female, 6 month history of recurrent attacks of severe epigastric pain recurrent attacks of severe epigastric pain -> back. Possibly dark urine at times-> back. Possibly dark urine at times
USS…USS…
Lap chole…Lap chole…

Hepatobiliary PathologyHepatobiliary Pathology
Or how I learned to stop worrying Or how I learned to stop worrying and love the gallstone…and love the gallstone…
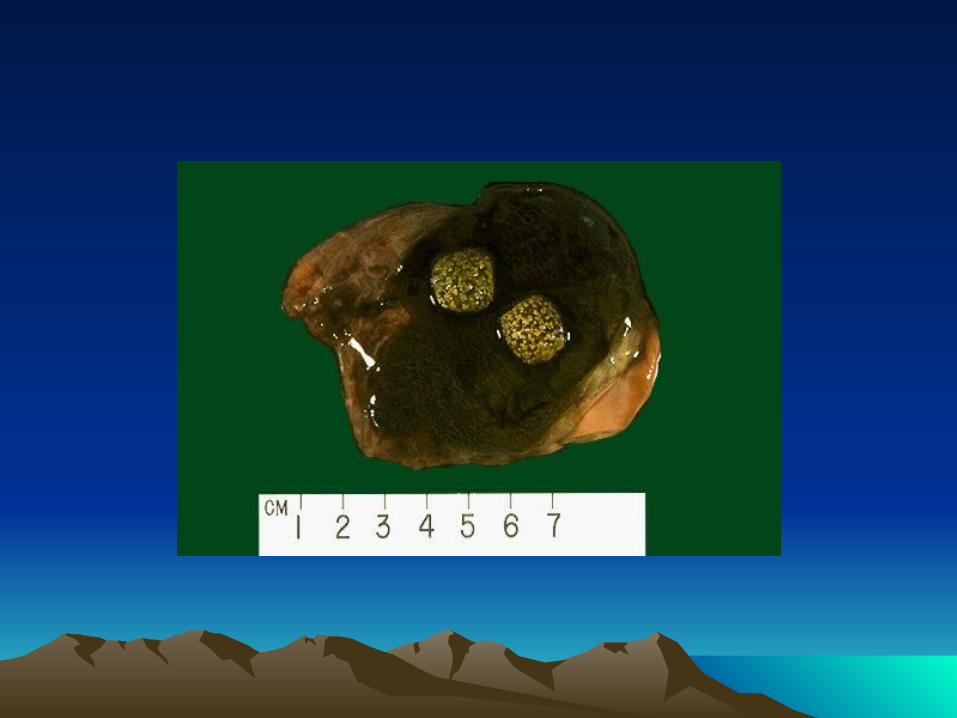
Cholesterol StonesCholesterol Stones
• Hypersecretion of cholesterol
• Decreased bile salt secretion
• Odd gallbladder
• Old, female, pregnant, obesity, rapid weight loss, ethnicity,impaired GB motility e.g. parenteral nutrition

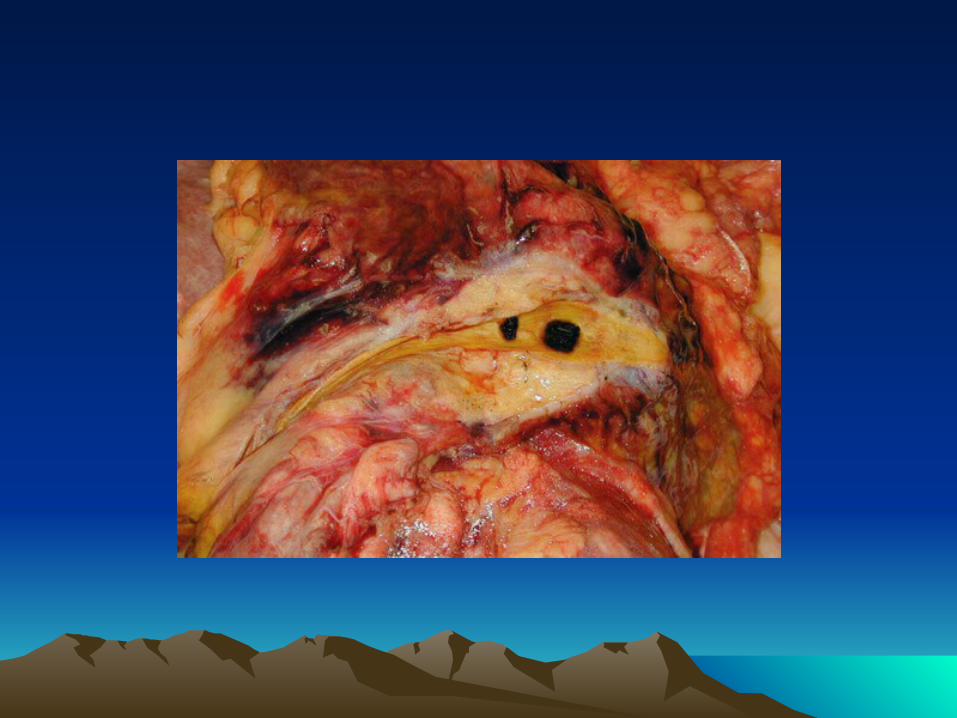
Pigment (haem) StonesPigment (haem) Stones
• Calcium bilirubinate
• Chronic haemolysis








38 year old female, 6 month history of 38 year old female, 6 month history of recurrent attacks of severe epigastric pain -> recurrent attacks of severe epigastric pain -> back. Possibly dark urine at timesback. Possibly dark urine at times
•USS…USS…
•Lap chole…Lap chole…
5 days postop readmitted with severe 5 days postop readmitted with severe abdominal pain….. abdominal pain…..
•Why, what investigationsWhy, what investigations

USS (CT)USS (CT)
Unremarkable
What else …




How might we identify preop which How might we identify preop which patients may harbour CBD stones….patients may harbour CBD stones….

44 year old female with 2 week history of 44 year old female with 2 week history of obstructive jaundiceobstructive jaundice
OK LFTs but so whatOK LFTs but so what
USS: USS:

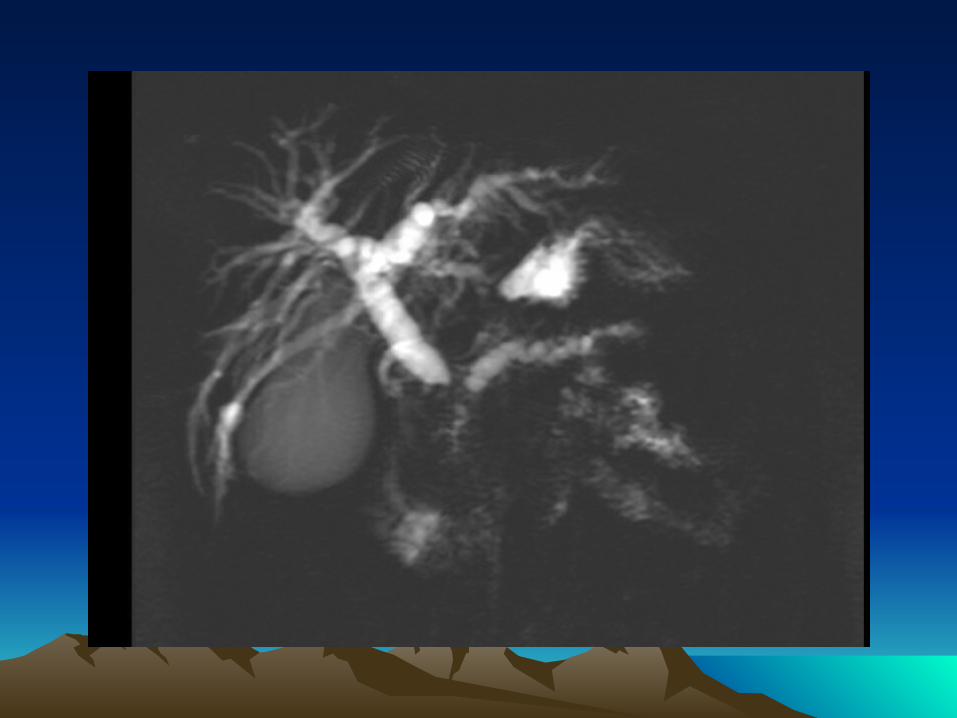













68 year old female with 2 week history of 68 year old female with 2 week history of obstructive jaundiceobstructive jaundice
USS: CBD 16mm GB distended, no stonesUSS: CBD 16mm GB distended, no stones
CT scan – unresectable ca pancreasCT scan – unresectable ca pancreas
Palliative R….Palliative R….
Stent - route Stent - route

ERCP StentERCP Stent


Percutaneous transhepatic Percutaneous transhepatic cholangiographycholangiography
Indications
•Determination of obstructive jaundice
•Level of obstruction
•Persistent pain after GB removal
Contraindications
Close to 100% sensitivity and specificity in identifying cause and level of obstruction

Self-expanding stent placed in the CBD of patient with non-resectable pancreatic tumour


Palliative Treatment:Palliative Treatment:
(Biopsy) – including EUS(Biopsy) – including EUS
GemcitabineGemcitabine



Pancreatic CancerPancreatic Cancer
• Adenocarcinoma
• Exocrine Pancreas
• Older, males > females, fags, booze, fat, carbs. BRACA-2, PJS
• 60, 10, 10% (Head, body, tail)
• 80% outside pancreas at diagnosis
• CA 19/9.




If it had been operable…If it had been operable…

47 year old male. 3 year history of 47 year old male. 3 year history of epigastric pain -> back. Rather constant. epigastric pain -> back. Rather constant. Worsening over 6 months. Stools recently Worsening over 6 months. Stools recently rather loose.rather loose.
Thoughts….Thoughts….
USS ….USS ….

Case 3Case 3
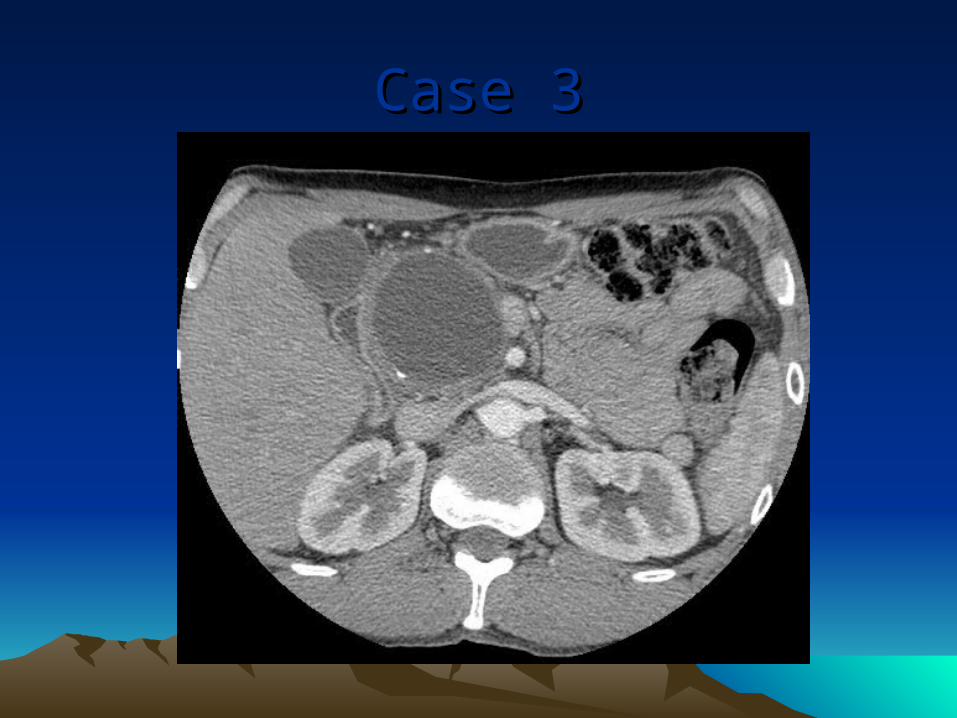
Case 3Case 3

Some other imagesSome other images


How to treat pseudocysts??How to treat pseudocysts??
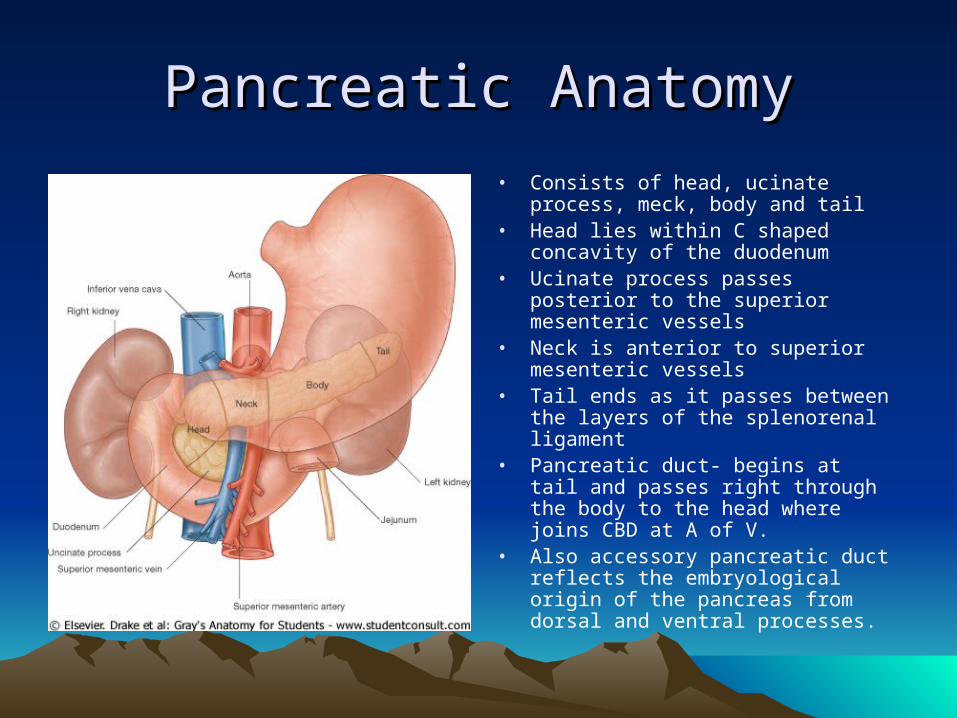
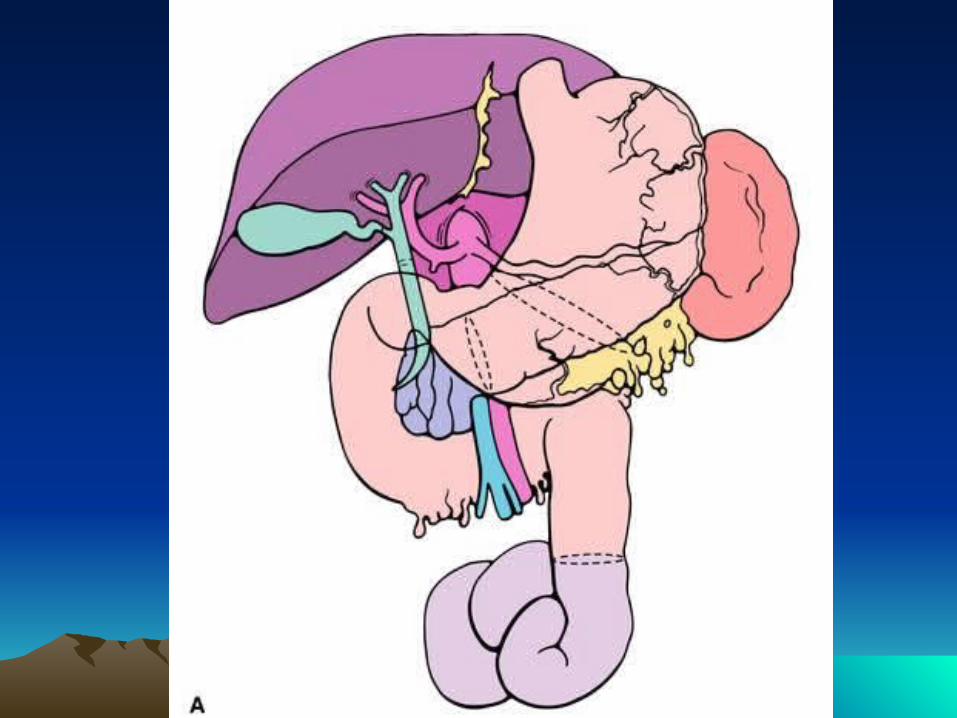
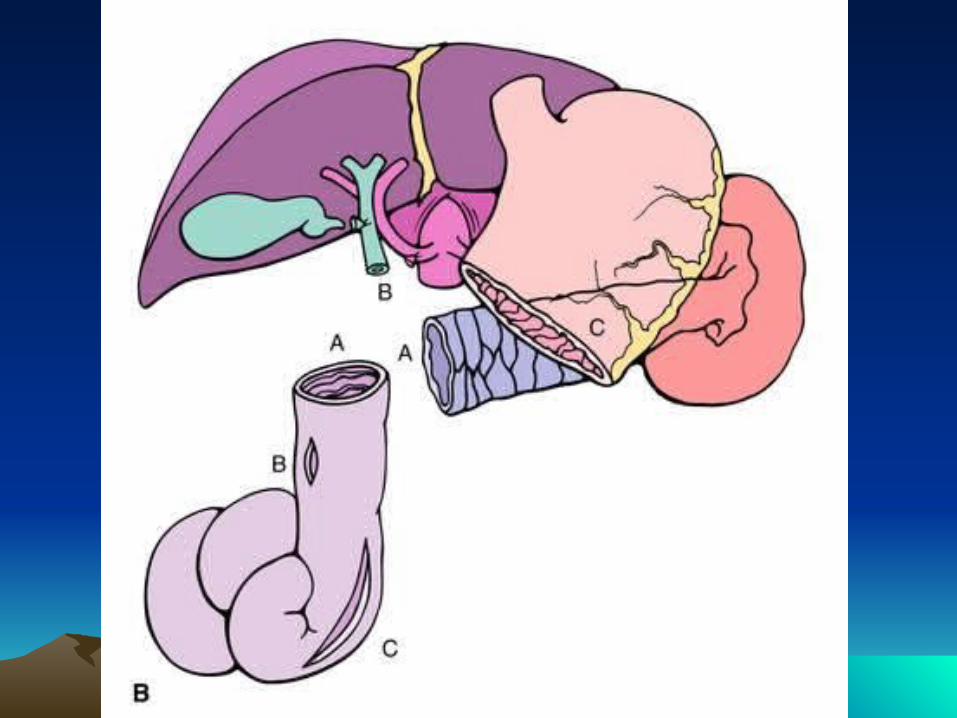
Pancreatic AnatomyPancreatic Anatomy
• Consists of head, ucinate process, meck, body and tail
• Head lies within C shaped concavity of the duodenum
• Ucinate process passes posterior to the superior mesenteric vessels
• Neck is anterior to superior mesenteric vessels
• Tail ends as it passes between the layers of the splenorenal ligament
• Pancreatic duct- begins at tail and passes right through the body to the head where joins CBD at A of V.
• Also accessory pancreatic duct reflects the embryological origin of the pancreas from dorsal and ventral processes.

Pseudocyst drainagePseudocyst drainage




Pancreatic CystsPancreatic Cysts
• Non-neoplastic– Pseudocysts– others
• Neoplastic– Mucinous (cystadenoma)– Papillary/cystic tumours– Cystadenocarcinoma– Degeneration in any cancer
• FNAC– Steep learning curve
PANCREATITIS, PANCREATITIS, attempts to clarifyattempts to clarify
MARSEILLESMARSEILLES
• Chronic Pancreatitis
• Acute Pancreatitis
Acute PancreatitisAcute Pancreatitis
Acute Pancreatitis
• Mild - 80% ?management
• Severe – 20% total – manage carefully
• 6% mortality – what of, operations?
• How to identify the severes

Acute PancreatitisAcute Pancreatitis
Requires:•Small stones•Wide cystic duct•Decent common channel
1
2

Chronic PancreatitisChronic Pancreatitis
Chronic Pancreatitis
• Usually alcoholic aetiology
• Slowly progressive (1/4 if abstain)
• Will not recover
• Fibrosis, stone protein, calcification
• Some have pain
• Some have episodes of pancreatitis
Ok its chronic pancreatitisOk its chronic pancreatitis
Alcohol …Alcohol …
Pain …Pain …
Diabetes …Diabetes …
Steatorrhoea …Steatorrhoea …
69 year old male referred with an inguinal 69 year old male referred with an inguinal hernia. Looks terrible. Admits to 3 months hernia. Looks terrible. Admits to 3 months of anorexia, lethargy and weight loss.of anorexia, lethargy and weight loss.
Investigation …Investigation …

Case 4Case 4
Multiple Liver MetsMultiple Liver Mets
• Hunt the primary??
• Why??
• Most colorectal, upper GI, pancreas, lung
Inoperable liver mets.Inoperable liver mets.Hunting?Hunting?
• Clinical
• Imaging +/- biopsy
• Immunochemistry– Specific (ha ha) markers– Cytokeratin profiles

Tumours with specific therapiesTumours with specific therapies
• Breast
• Colorectal
• Other UGI
• (Prostate)
• (Thyroid)
• Oncology peer pressure


Potential treatments available for some Potential treatments available for some patientspatients
ResectionResection
Local treatments ….Local treatments ….

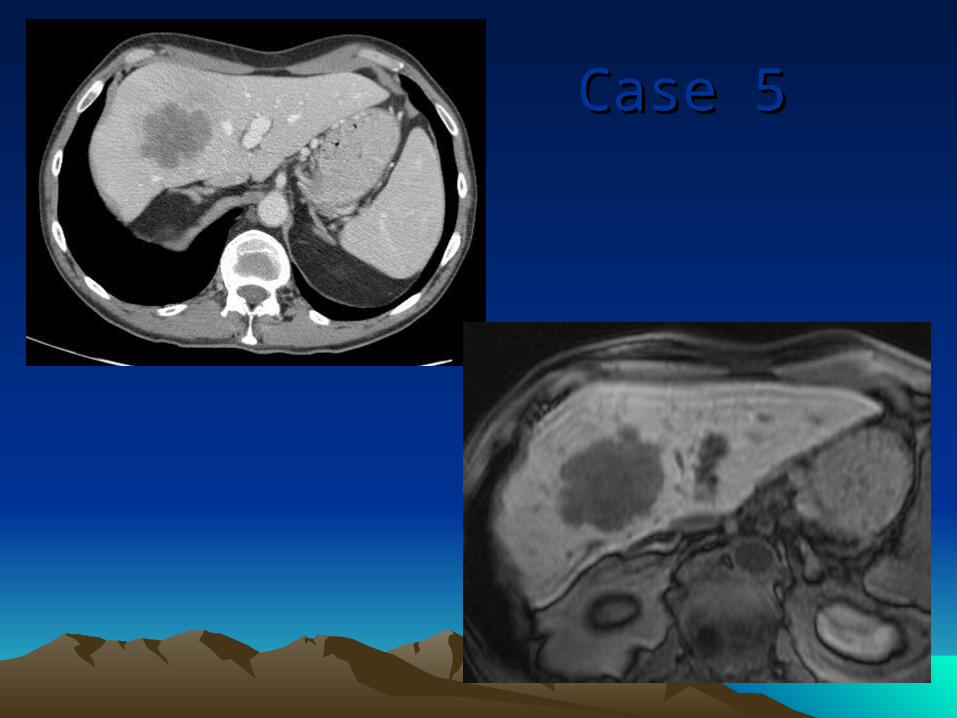
Case 5Case 5

Case 6Case 6
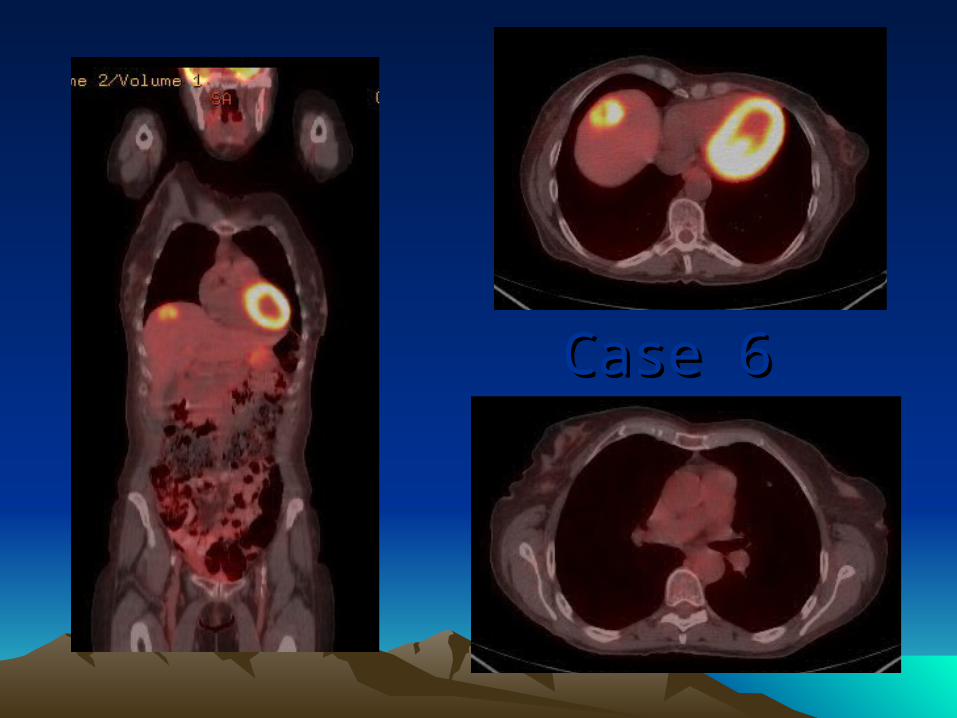
Case 6Case 6

A few messages to repeatA few messages to repeat::
• Don’t forget CBD stonesDon’t forget CBD stones
• ERCP is principally for therapy now ERCP is principally for therapy now
• Save time, do the right test, ask a radiologistSave time, do the right test, ask a radiologist
• Tissue diagnosis not always possible in Tissue diagnosis not always possible in pancreatic cancer pancreatic cancer
• Time is critical in obs jaundiceTime is critical in obs jaundice
• Good palliation from biliary decompression Good palliation from biliary decompression
• CA 19/9 for pancreatic cancer CA 19/9 for pancreatic cancer
• GEMCITABINE for pancreatic cancerGEMCITABINE for pancreatic cancer

Any questions about anythingAny questions about anything