Embed Size (px)
Citation preview
Risk Analysis, Vol. 29, No. 6, 2009 DOI: 10.1111/j.1539-6924.2009.01202.x
Human Health Risk Assessment of Penicillin/Aminopenicillin Resistance in Enterococci Dueto Penicillin Use in Food Animals
Louis Anthony (Tony) Cox, Jr.,1,2,∗ Douglas A. Popken,1,3 and Jeremy J. Mathers4
Penicillin and ampicillin drugs are approved for use in food animals in the United States totreat, control, and prevent diseases, and penicillin is approved for use to improve growthrates in pigs and poultry. This article considers the possibility that such uses might increasethe incidence of ampicillin-resistant Enterococcus faecium (AREF) of animal origin in hu-man infections, leading to increased hospitalization and mortality due to reduced responseto ampicillin or penicillin. We assess the risks from continued use of penicillin-based drugs infood animals in the United States, using several assumptions to overcome current scientificuncertainties and data gaps. Multiplying the total at-risk population of intensive care unit(ICU) patients by a series of estimated factors suggests that not more than 0.04 excess mor-talities per year (under conservative assumptions) to 0.14 excess mortalities per year (undervery conservative assumptions) might be prevented in the whole U.S. population if currentuse of penicillin drugs in food animals were discontinued and if this successfully reduced theprevalence of AREF infections among ICU patients. These calculations suggest that currentpenicillin usage in food animals in the United States presents very low (possibly zero) humanhealth risks.
KEY WORDS: Animal antimicrobials; enterococcus; penicillin; resistance; risk assessment
1. INTRODUCTION
Penicillin drugs (specifically, Penicillin G, Pro-caine subtype) are approved for use in food animalsin the United States to treat, control, and preventdiseases and to improve growth rates (FDA-CVM,2007; Sechen, 2006; AHI, 2006). Concerns havebeen expressed that penicillin use might increasethe risk of antibiotic resistance in human entero-
1 Cox Associates.2 University of Colorado.3 Systems View.4 Alpharma Animal Health Division.∗ Address correspondence to Tony Cox, 503 Franklin Street,
Denver, CO 80218, USA; tel: 303-388-1778; fax: 303-388-0609;[email protected].
coccal infections from nonhuman sources, leadingto increased morbidity and mortality (WHO, 2005,2007; FAO/WHO/OIE, 2008). Approved feed usagesof penicillins in food animals have been a controver-sial topic for several decades in the United States,with many reviews and initiatives undertaken to ad-dress resistance concerns (IOM, 1989; FDA, 2000;FDA, 2003). Regulatory approvals have been givenfor administration to animals via drinking water andfeeds for therapeutic uses, including disease preven-tion and control, as well as for feed efficiency/growthpromotion uses in food animals (FDA-CVM, 2007).The amounts of penicillins sold for use in food an-imals in the United States remain relatively lowcompared to other antimicrobials, with sole growthpromotion uses representing a small subfraction ofthe total (AHI, 2006). Penicillin drugs have been
796 0272-4332/09/0100-0796$22.00/1 C© 2009 Society for Risk Analysis
Human Health Risk Assessment of Penicillin/Aminopenicillin Resistance 797
identified as “critically important” to animal health(FAO/WHO/OIE, 2008).
The only penicillin drug type approved for non-therapeutic uses in the United States is PenicillinG (Procaine subtype), which is given primarily toswine and chicken; none is given to cattle. A USDA(2002) survey indicated that, in grower/finisher pigs,over 99.5% of all penicillin is administered (primar-ily via injection) for disease treatment and preven-tion. A relatively small amount of ampicillin is alsoused for disease treatment. In a large-scale study of82 poultry farms in the eastern United States, Hayeset al. (2004) measured resistance levels of entero-cocci found in chicken litter. E. faecalis represented53% of the isolates and had 0% penicillin resistance.E. faecium represented 31% of the isolates. Seventy-one percent of the E. faecium (71 out of 104 isolates)had penicillin resistance, but only 1% (1 out of 104)had ampicillin resistance.
This article quantifies the potential for continueduse of penicillin drugs in food animals to harm hu-man health by increasing the number of ampicillin-resistant enterococcal infections in human patients.After summarizing relevant background for the haz-ard of greatest concern—infection of intensive careunit (ICU) patients with ampicillin-resistant Ente-rococcus faecium (AREF) bacteria—the followingsections focus on quantifying the fraction of such re-sistant infections that might be prevented by discon-tinuing the use of penicillin drugs in food animals.
2. BACKGROUND, HAZARDIDENTIFICATION, AND SCOPE:REDUCING AMPICILLIN-RESISTANTE. FAECIUM INFECTIONS INICU PATIENTS
Enterococci are commensal gram-positive bac-teria found in the intestinal flora of most healthybirds and mammals, including people (Biavascoet al., 2007; Willems, 2000). In humans, entero-cocci typically comprise not more than 1% of themicroflora of adults (FDA-CVM, 2004) and arenormally harmless; however, they can cause oppor-tunistic infections in ICU patients or others withweakened immune systems. The Enterococcus genushas 17 species, but most human clinical isolates areeither E. faecalis (74–90%) or E. faecium (5–16%)(Varman et al., 2006).
E. faecalis infections are responsible for mostclinical enterococcal infections, but penicillin (orampicillin) resistance is rare in E. faecalis isolates
from food animals and almost nonexistent in E.faecalis isolates from retail meats (Hayes et al.,2003, 2004; McGowan et al., 2006; NARMS, 2005);none of the meat-borne E faecalis samples isolatedfrom retail meats in a national surveillance program(NARMS, 2002–2005) exhibited resistance to peni-cillin. Furthermore, ampicillin remains highly effec-tive against clinical E. faecalis (Jones et al., 2004).Therefore, our risk assessment focuses on the iden-tified hazard of ampicillin resistance among humanE. faecium infections.
Risk to human health arises because some strainsof enterococci may become opportunistic pathogens,potentially resistant to multiple drugs, that infect pa-tients who are already seriously ill (typically in ICUs)with immune systems weakened by organ trans-plants, chemotherapy, AIDS, or other causes. In-deed, enterococcal infection is the second most com-mon hospital-acquired infection in the United States(Varman et al., 2006). These infections can prolongillness and increase patient mortality. Vancomycin-resistant enterococci (VRE) are of particular con-cern because of their virulence and resistance to evensome recently developed antibiotics. Vancomycin-resistant E. faecium (VREF) can cause serious andoften fatal disease in vulnerable populations, such asliver transplant patients and patients with hemato-logic malignancies (Leavis et al., 2003; Rice, 2001).
Many enterococcal infections, including VRE,resolve without antimicrobial treatment (Varmanet al., 2006; Rice, 2001). In severe cases forwhich antimicrobial treatment is provided, peni-cillin and ampicillin are often the leading choices.Other drugs that are also effective against hu-man enterococcal infections include gentamicin,vancomycin, quinupristin-dalfopristin (Synercid R©),linezolid (Zyvox R©), tigecycline (Tygacil R©), and ni-trofurantion. These can be used in patients with al-lergy or high-level resistance to penicillin and ampi-cillin. Many ampicillin-resistant cases can also betreated successfully with high doses of ampicillin,either alone or in combination with drugs such asgentamicin or streptomycin (Varman et al., 2006;Murray, 2000).
Most E. faecium infections in ICU patients inthe United States are now resistant to vancomycin(Edmond et al., 1999; Jones et al., 2004; Leaviset al., 2003). Patients with VREF have worseoutcomes than those with vancomycin susceptiblestrains—longer hospital stays and higher mortality(Webb et al., 2001). As noted by Rice (2001), vir-tually all VREF are also ampicillin resistant: “More

798 Cox, Popken, and Mathers
than 95% of VRE recovered in the United Statesare E. faecium; virtually all are resistant to high lev-els of ampicillin.” Hence, our risk assessment treatsVREF as being (at least approximately) a subset ofAREF. One suggested explanation is “that the closeassociation of the vancomycin and ampicillin resis-tance phenotypes, at least in VanB-type VRE, is ex-plainable by their inclusion within large, transferablegenetic elements” (Hanrahan et al., 2000, p. 1350).However, widespread ampicillin resistance appearedin 1982 (Fortun et al., 2002), while vancomycin re-sistance appeared in the early 1990s in E. faecium(Murray, 2000).
Since most VREF are AREF (although manyAREF are not VREF), and assuming that changesin animal penicillin use would not significantly af-fect vancomycin resistance (consistent with histori-cal data), we focus on human (ICU patient) infec-tions with vancomycin-susceptible strains of AREF.Presumably, this is the subpopulation that might ex-perience decreased ampicillin resistance if discontin-uing animal penicillin drugs were to replace someAREF cases with ampicillin-susceptible cases. Forpatients with VREF, we assume that AREF wouldpersist (due to the observed co-occurrence of AREFin VREF strains), so that no benefit from reducedAREF would be achieved for these patients.
The following sections seek to quantify poten-tially preventable AREF cases and the human healthbenefits that might be created if these AREF caseswere prevented (made ampicillin-susceptible) by dis-continuing penicillin drug uses in food animals. Thisapproach draws on recent advances in sequencingtechnology that enable more precise strain groupingsand epidemiological analyses than have previouslybeen possible.
3. METHODS AND DATA: UPPER BOUNDSFOR PREVENTABLE MORTALITIES
Recognizing that a farm-to-fork (forward chain-ing) approach is not practical for AREF due to dataand knowledge gaps in release, exposure, and dose-response relations, we instead start with more readilyavailable human data on ICU case loads and resis-tance rates, similar to the approach in Cox and Pop-ken (2004). We then work backward to estimate aplausible upper bound on the annual number of hu-man patient mortalities that might be prevented bydiscontinuing penicillin use in food animals.
For purposes of conservative (i.e., upper-bound)risk assessment, we define a potentially preventablemortality to occur whenever the following condi-
tions hold: (1) an ICU patient dies, following (2) anE. faecium infection that (3) is resistant to ampi-cillin (AREF) (and hence might have benefited hadampicillin resistance been prevented). The infectionwas (4) vancomycin-susceptible (and hence mighthave also been ampicillin-susceptible, had it not beenfor penicillin use in food animals); (5) not knownto have been contracted from the hospital environ-ment (and hence might have been prevented by ac-tions external to the hospital, such as elimination ofAREFs from food animals); (6) could have comefrom food animals (i.e., has a genotype or resistancedeterminants of the types found in food animals).(7) The patient tolerated penicillin (i.e., was not aller-gic, and hence might have benefited from ampicillin,had it not been for resistance). We propose that theconjunction of these seven conditions should be in-terpreted as necessary for a mortality to have beencaused (with nonnegligible probability) by resistancedue to use of penicillin in food animals, even thoughit is not sufficient (e.g., the infecting strain might havehad some other origin than food animals, or the pa-tient might have died anyway, even if the infectionhad been ampicillin-susceptible).
Accordingly, the following sections estimate aplausible upper bound on annual preventable mor-talities from AREF infections based on the followingproduct of factors:
Preventable AREF mortalities per year ≤ (to-tal number of ICU infections per year) × (fractioncaused by E. faecium) × (fraction of ICU E. fae-cium infections that are AREF and exogenous, i.e.,not known to be of nosocomial origin) × (fractionof these exogenous AREF cases that are vancomycin-susceptible) × (fraction of vancomycin-susceptible ex-ogenous AREF cases that might have come from foodanimals) × (fraction of these cases that are penicillin-tolerant)× (excess mortality rate for AREF cases com-pared to ASEF cases).
That is, we first quantify the expected annual numberof AREF cases in the United States that might ben-efit from ampicillin treatment if food animal uses ofpenicillin were halted (i.e., cases that are penicillin-tolerant and vancomycin-susceptible and that mighthave been caused by resistance determinants fromfood animals). Then, we multiply this number by theexcess mortality rate for resistant as opposed to sus-ceptible cases.
3.1. Estimated Number of ICU Infections Per Year
Enterococcal infections are generally limitedto already hospitalized individuals. E. faecium
Human Health Risk Assessment of Penicillin/Aminopenicillin Resistance 799
infections are frequently associated with nosoco-mial bloodstream infections occurring within ICUs.A recent FDA risk assessment for virginiamycin(FDA-CVM, 2004) provided the following two ap-proximate estimates:
(1) N = annual number of ICU infections =104,372.5 based on blood-stream infections.
(2) N = 315,000 based on septicemia cases.
The study does not weight these alternatives. To beconservative (i.e., to maximize estimated risks), wewill use the larger estimate, N = 315,000 cases/year.(Patients with severely complicated urinary tract in-fections (UTIs) are also sometimes treated withintravenous antibiotics, including combinations ofgentamicin and ampicillin, but ceftriaxone may besubstituted for ampicillin if needed, and oral an-tibiotics (e.g., trimethoprim, cephalosporins, nitro-furantoin, or ciprofloxacin) are used in the vastmajority of cases (http://adam.about.com/reports/000036 7.htm). We therefore do not include UTIcases in this assessment.)
3.2. Fraction of ICU Infections Causedby E. faecium
The proportion of ICU infections that are causedby E. faecium can be estimated with the help of thefollowing two fractions from the same FDA-CVMstudy:
(1) Pent = 0.10 = fraction of ICU infectionscaused by Enterococcus. (Wisplinghoff et al.,2004 provide an estimate of 0.09. To be con-servative, we use the higher estimate of 0.10.)
(2) PEF,ent = 0.25 = fraction of enterococcal in-fections caused by E. faecium.
The product of these two factors, fEF = Pent ∗PEF,ent = 0.025, is the estimated fraction of ICU in-fections caused by E. faecium. An approximate valuefor the expected annual rate of E. faecium infectionscan then be obtained via the equation:
Expected annual number of E. faecium infections =N ∗ fEF = N ∗ Pent ∗ PEF,ent ≤ 315,000 ∗ 0.025 = 7,875E. faecium infections/year.
3.3. Fraction of ICU E. faecium Infections that areAmpicillin-Resistant and Exogenous(Nonnosocomial)
Most AREF infections are contracted nosoco-mially. Indeed, it is possible that few or none orig-inate in food animals. For example, as stated by
Kuhn et al. (2005), in Europe “it seems that animal-associated VRE probably reflect the former use ofavoparcin in animal production, whereas VRE inhuman-associated samples may be a result of antibi-otic use in hospitals.” Since nosocomial transmissionis a hospital-specific problem that can often be elim-inated by rigorous control measures, we restrict ourrisk assessment to exogenous (nonnosocomial) casesthat are potentially attributable to food animals. (Ifthis restriction is dropped in sensitivity analysis, theeffect is simply to divide estimated annual impacts bythe nonnosocomial fraction of cases, which increasesthem approximately sixfold.)
Cox and Popken (2004) used data from severalstudies in the 1990s to estimate an approximate meanvalue of 0.17 for the fraction of exogenous cases inthe United States. (This is the mean of a range of val-ues, extending from a low of 0.089 based on data inBischoff et al. (1999) to a high of 25% based on esti-mates in Austin et al. (1999).) More recent investiga-tions of the molecular epidemiology of drug-resistantE. faecium infections suggest that, if anything, thisproportion may have decreased since the 1990s as aparticular hospital-adapted clone of E. faecium calledCC17 has spread widely in hospitals in the UnitedStates and elsewhere (Leavis et al., 2006; Top et al.,2007; Willems, 2001). Approximately 88% of E. fae-cium isolates from hospital outbreaks (n = 32) be-long to Complex-17, compared to 59% of all clini-cal isolates (n = 162), 23% of isolates from hospi-tal surveillance in Australia, Europe, and North andSouth America (n = 64), 5% of community isolates(n = 57), and 1% of isolates from animal surveil-lance (n = 96, including bison, calves, cats and dogs,ostriches, poultry, pigs, and rodents in Africa andEurope) (Leavis et al., 2006). In the United States,too, Complex-17 and a closely associated clade ofhospital-associated strains dominate the epidemiol-ogy of AREF (Leavis et al., 2007; Deshpande et al.,2007).
To be conservative, we continue to assume thatthe fraction of exogenous cases is 0.17, although ac-knowledging that this fraction may be declining sig-nificantly as these hospital-associated strains accountfor a higher proportion of all E. faecium infections.
The fraction of exogenous cases that areampicillin-resistant can be estimated from data inTable I of Willems et al. (2005). Pooling all nonout-break, non-Complex-17 cases (where “nonoutbreak”cases are the sum of clinical and hospital surveil-lance isolates) gives a total of 20 ampicillin-resistantcases out of 107 total cases, for a resistance frac-tion of: 20/107 = 0.187 ampicillin-resistant cases
800 Cox, Popken, and Mathers
per nonoutbreak case. In summary, the estimatedexpected annual number of ampicillin-resistant,exogenously caused (i.e., nonnosocomial) E. faeciuminfections in the United States is no more than:
(7,875 E. faecium infections/year) ∗ (0.17 nonnosoco-mial fraction) ∗ (0.187 ampicillin-resistant fraction) =7,875 ∗ 0.17 ∗ 0.187 = 250 exogenous AREF infectionsper year.
3.4. Fraction of Vancomycin-Susceptible Cases
Assuming that almost all vancomycin-resistantstrains of E. faecium in the United States are alsoampicillin resistant (but not vice-versa) (Rice, 2001),the relatively recent data of Jones et al. (2004) showthat, in the United States, about 14% of E. faeciumstrains are ampicillin resistant and vancomycin sus-ceptible. Specifically, 90.3% of E. faecium isolateswere resistant to ampicillin and 76.3% of E. fae-cium isolates were resistant to vancomycin. The dif-ference is 0.903 – 0.763 = 0.14. This is an estimateof the fraction of E. faecium isolates that are AREFbut not VREF—in other words, the vancomycin-susceptible AREF of interest for our risk assessment.Thus, 0.14/0.903 = 0.155 is the estimated fraction ofAREF that are vancomycin susceptible. Using thispoint estimate yields:
Expected exogenous ampicillin-resistant andvancomycin-susceptible cases per year ≤ 250 ∗ 0.155 =38.75 vancomycin-susceptible AREF infections/year.
This should be considered an upper bound. For ex-ample, research by Suppola et al. (1999) suggestedthat Van A and Van B E. faecium incorporate intoan endemic vancomycin-susceptible AREF strain.
3.5. Fraction of Exogenous Cases Potentiallyfrom Food Animals
As reviewed above, genetic similarities betweenampicillin-resistant strains found in nonoutbreakE. faecium infections among hospitalized patients(most of which carry the esp virulence gene and otherdistinctive genes) and strains found in food animals(most of which do not) is weak (Kuhn et al., 2005;Leavis et al., 2006, 2007). No clear empirical attribu-tion of hospital cases to food animals can be madebased on these data.
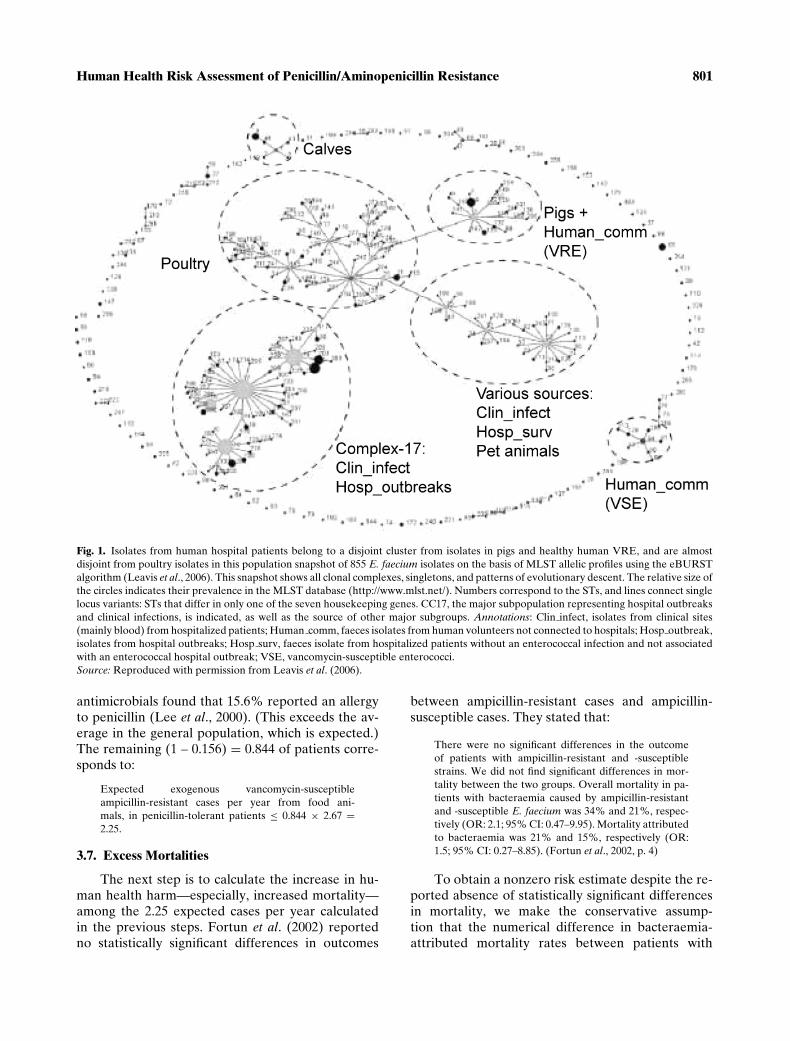
Fig. 1 summarizes data that suggest a possibleupper-bound quantitative estimate for the contri-bution of strains of E. faecium found in food ani-mals to strains found in nonoutbreak (non-Complex-17) human patient isolates. The figure representsinferred patterns of evolutionary descent among
multiple strains of E. faecium. Each numberrepresents a sequence type (ST). Lines connect STsthat differ in only one of seven “housekeepinggenes.” The relative sizes of the circles represent therelative prevalences of the STs. In the relatively fewcases where human patient and food animal (pig andpoultry) clusters overlap, the strains falling in theoverlap might have come from a common environ-mental source (e.g., soil or water), or might be dueto a “reverse causation” flow from humans to pigsvia surface water, flies, pets, or other paths (Guard-abassi & Dalsgaard, 2004; Macovei & Zurek, 2006;Rodrigues et al., 2002).
The Multi Locus Sequence Typing website(www.mlst.net—curator: Rob Willems) provides adatabase of 490 E. faecium samples—a subset ofthose used to generate Fig. 1 of Leavis et al.(2006). The data indicate 87 unique STs among“Clin˙Isol” and “Hosp˙Surv” (human, nonoutbreak,noncommunity) clusters. (We do not consider the“Hosp Outbreaks” category, since these are assumedto fall into the nosocomially transmitted group. Wealso do not consider the “Human comm” categoryas these are noninfectious strains found in healthyindividuals.) Two of these 87 STs (26 and 32) areshared with poultry and four (5, 6, 18, 133) areshared with pigs. If we assume, conservatively, thatall shared types represent transmission from food an-imals to human patients (rather than from peopleto animals, or to both from common environmentalsources such as soil, water, flies, or birds), then anestimate of the fraction of strains in human patientsthat might originate in food animals is: 6/87 = 0.069.This assumes that all shared types arise from food-borne transmission of resistant bacteria, originatingin food animals on the farm, to people via the foodchain. Using this point estimate reduces the above es-timate to:
Expected exogenous vancomycin-susceptible andampicillin-resistant cases per year from food animals≤ (38.75 exogenous vancomycin-susceptible andampicillin-resistant cases per year) ∗ (fraction of notmore than 6/87 from food animals) ≤ 2.67 exoge-nous vancomycin-susceptible and ampicillin-resistantinfections per year from food animals.
3.6. Penicillin Allergies
Hospitalized patients who are allergic to peni-cillin cannot have their enterococcal infectionstreated with penicillin or ampicillin. Since such pa-tients are not harmed by penicillin resistance, weneed to exclude them from risk calculations. Alarge U.S. study of hospitalized patients requiring
Human Health Risk Assessment of Penicillin/Aminopenicillin Resistance 801
Fig. 1. Isolates from human hospital patients belong to a disjoint cluster from isolates in pigs and healthy human VRE, and are almostdisjoint from poultry isolates in this population snapshot of 855 E. faecium isolates on the basis of MLST allelic profiles using the eBURSTalgorithm (Leavis et al., 2006). This snapshot shows all clonal complexes, singletons, and patterns of evolutionary descent. The relative size ofthe circles indicates their prevalence in the MLST database (http://www.mlst.net/). Numbers correspond to the STs, and lines connect singlelocus variants: STs that differ in only one of the seven housekeeping genes. CC17, the major subpopulation representing hospital outbreaksand clinical infections, is indicated, as well as the source of other major subgroups. Annotations: Clin infect, isolates from clinical sites(mainly blood) from hospitalized patients; Human comm, faeces isolates from human volunteers not connected to hospitals; Hosp outbreak,isolates from hospital outbreaks; Hosp surv, faeces isolate from hospitalized patients without an enterococcal infection and not associatedwith an enterococcal hospital outbreak; VSE, vancomycin-susceptible enterococci.Source: Reproduced with permission from Leavis et al. (2006).
antimicrobials found that 15.6% reported an allergyto penicillin (Lee et al., 2000). (This exceeds the av-erage in the general population, which is expected.)The remaining (1 – 0.156) = 0.844 of patients corre-sponds to:
Expected exogenous vancomycin-susceptibleampicillin-resistant cases per year from food ani-mals, in penicillin-tolerant patients ≤ 0.844 × 2.67 =2.25.
3.7. Excess Mortalities
The next step is to calculate the increase in hu-man health harm—especially, increased mortality—among the 2.25 expected cases per year calculatedin the previous steps. Fortun et al. (2002) reportedno statistically significant differences in outcomes
between ampicillin-resistant cases and ampicillin-susceptible cases. They stated that:
There were no significant differences in the outcomeof patients with ampicillin-resistant and -susceptiblestrains. We did not find significant differences in mor-tality between the two groups. Overall mortality in pa-tients with bacteraemia caused by ampicillin-resistantand -susceptible E. faecium was 34% and 21%, respec-tively (OR: 2.1; 95% CI: 0.47–9.95). Mortality attributedto bacteraemia was 21% and 15%, respectively (OR:1.5; 95% CI: 0.27–8.85). (Fortun et al., 2002, p. 4)
To obtain a nonzero risk estimate despite the re-ported absence of statistically significant differencesin mortality, we make the conservative assump-tion that the numerical difference in bacteraemia-attributed mortality rates between patients with
802 Cox, Popken, and Mathers
ampicillin-resistant and -susceptible strains reflectsa true causal effect (i.e., that resistance does causea 21% – 15% = 6% increase in absolute mortalityrisk, per patient per infection). In other words, wetreat the statistically nonsignificant difference as atrue difference caused by ampicillin-resistance (butacknowledge that this is not the original authors’ in-terpretation and that the true difference could beas small as zero). This assumption provides a possi-ble basis for calculating a nonzero human health riskfrom ampicillin resistance.
With this assumption, the expected annual ex-cess mortality risk caused by ampicillin resistancebecomes:
Expected excess mortalities per year (for the entireU.S. population) caused by exogenous vancomycin-susceptible and AREF infections, assumed to originatefrom food animals, in penicillin-tolerant patients ≤ 2.25∗ 0.06 = 0.135 excess mortalities/year.
In reality, annual mortality risks from AREFare likely to be much smaller than this, as patient-cultured isolates would typically be screened for re-sistance prior to treatment (standard procedure in-dicated for such infections) and then patients withAREF would be treated with other drugs suchas gentamicin, vancomycin, quinupristin/dalfopristin,linezolid, daptomycin, tigecycline, or nitrofuran-tion. In addition, the above mortality estimate doesnot address morbidity or quality-adjusted life years(QALYs) lost due to potentially preventable re-sistance. The patients at risk are already severelyill (usually, immuno-compromised) patients suchas leukemia, transplant, and AIDS patients. Thus,the hypothesized increased risk (per infection withampicillin-resistant vancomycin-susceptible E. fae-cium) represents fewer QALYs lost than wouldbe the case for otherwise healthy patients. Wehave therefore not attempted to quantify QALYimpacts.
4. RESULTS SUMMARY, SENSITIVITYAND UNCERTAINTY ANALYSIS
Table I summarizes key parameter estimates,calculations, assumptions, and resulting risk esti-mates from this study. It is traditional in presentingpoint estimates to also present interval estimates toinform decisionmakers about the plausible range ofestimated values. In the present analysis, however,the key uncertainties have little to do with statisticalsampling error, and are not adequately characterizedby confidence limits. Rather, they arise from uncer-
tainty about the validity and conservatism of the as-sumptions in Table I.
Qualitatively, the main uncertainty is aboutwhether there is a nonzero risk to human health fromanimal use of penicillin drugs. We have assumed thatthere is, but there is no clear empirical proof that therisk is nonzero. To bridge this knowledge gap, Ta-ble I incorporates several conservative qualitative as-sumptions that jointly imply that the risk is nonzero.Other quantitative parameter values presented, andtheir implied risk estimate of ≤0.135 excess mortal-ities/year, are intended to be realistic, data-drivenvalues (rather than extreme upper bounds or 95%upper confidence limits) contingent on these conser-vative qualitative assumptions.
The most important conservative elements in Ta-ble I are the following qualitative assumptions:
(1) Transfer of ampicillin resistance from food an-imal bacteria to bacteria infecting human pa-tient occurs. The assumption that ampicillin-resistant strains and/or determinants aretransferred from strains in food animals to hu-man ICU patients is fundamental to the as-sessment in Table I. Such transfer has neverbeen shown to occur, but may be possi-ble, based on the similarities described inFig. 1.
(2) Withdrawing animal drug use would imme-diately and completely prevent the problem.Table I assumes that halting penicillin usein food animals would immediately eliminateall ampicillin resistance from the cases inTable I. This is a deliberately extreme as-sumption. In reality, halting use might havelittle or no impact on the already very low lev-els of ampicillin resistance.
(3) Resistance increases patients mortality. The as-sumption that ampicillin resistance causes anincrease in the mortality rates of the patientsin Table I is made even though, in reality, nostatistically significant difference in mortalityrates has been found between resistant andnonresistant cases (Fortun et al., 2002).
With these assumptions, the calculations inTable I predict that excess mortalities per year inthe entire U.S. population could be as high as 0.135,i.e., an excess mortality expected roughly once ev-ery seven to eight years, if current conditions per-sist. This risk is concentrated among ICU patientsalready at high risk of such infections. With lessconservative assumptions, the estimated risk falls toabout 0.04 excess mortalities per year, i.e., about one

Human Health Risk Assessment of Penicillin/Aminopenicillin Resistance 803
Table I. Summary of Risk Calculation
PossibleFactor Base Case Value Alternative Value Source
N = ICU infections/year N = 315,000 N = 104,372.5 FDA-CVM, 2004Pent = fraction of ICU infections caused by
Enterococcus0.10 0.09 (Wisplinghoff et al.,
2004)FDA-CVM, 2004
PEF,ent = fraction of enterococcal infections causedby E. faecium.
0.25 FDA-CVM, 2004
Fraction of enterococcal infections caused byE. faecium that are exogenous (nonnosocomial)
≤ 0.17 Cox and Popken, 2004.(May be smaller now dueto spread of CC-17)
Fraction of exogenous cases that are ampicillinresistant
0.187 Willems et al., 2005
Fraction of exogenous ampicillin-resistant casesthat are vancomycin susceptible
0.155 Jones et al., 2004
Fraction of exogenous ampicillin-resistantvancomycin-susceptible cases possibly from foodanimals
0–0.069 (0.069 assumed) Data of Leavis et al., 2006
Fraction of exogenous ampicillin-resistant caseswith penicillin-tolerant host
0.844 Lee et al., 2000
Fraction of these cases that would becomeampicillin susceptible if penicillin use in foodanimals were terminated
0.00–1.00. (1 is assumed) Conservative assumption
Increase in mortality risk per case, due to ampicillinresistance
0.00–0.06. (0.06 is assumed) Fortun et al., 2002,conservative assumption
RISK ≤ 0.14 potential excess mortalities/year 315000 ∗ 0.10 ∗ 0.25 ∗ 0.17 ∗0.187 ∗ 0.155 ∗ 0.069 ∗0.844 ∗ 0.06 = 0.135
104372.5 ∗ 0.09 ∗ 0.25 ∗0.17 ∗ 0.187 ∗ 0.155 ∗0.069 ∗ 0.844 ∗ 0.06 ≈0.04 mortalities/year
Product of precedingfactors
excess mortality every 25 years in the United Statesunder current conditions. The multiplicative calcu-lation in Table I makes sensitivity analysis of theseresults to changes in the values of specific factorsespecially straightforward: the final risk estimate isdirectly proportional to each factor listed.
The more conservative risk estimate of 0.135 ex-cess mortalities per year equates to an average in-dividual risk rate in the most at-risk group (ICUpatients) of approximately 0.135/315,000 = 4.3 ×10−7 excess mortalities per ICU patient. For theU.S. population as a whole, this corresponds toan average individual risk of approximately 0.135/300E6 = 4.5 × 10−10 excess fatalities per person-year,or a lifetime risk of about 80(6 × 10−10) = 3.6 ×10−8 excess risk of mortality per lifetime (for an as-sumed 80-year lifetime). This is well below the risklevel of 1 × 10−6 (1 per million lifetimes) sometimescited as a threshold for concern for carcinogens in theenvironment. If the less conservative risk estimateof 0.04 excess mortalities per year is used, these in-dividual and population risks are reduced by a fac-tor of 0.04/0.135, or more than threefold. If one ormore of the key qualitative assumptions listed above
are violated, then the true risk could be as low aszero.
We have emphasized that the most importantuncertainty in this analysis is discrete—is the pre-ventable fraction of risk positive or is it zero?—andthat such uncertainty is not well characterized by aconfidence interval. Nonetheless, it may be useful toconsider a rough upper bound on how large the truerisk might be. A crude estimate is given by Markov’sinequality for nonnegative random variables if we as-sume that the risk estimates in Table I represent ex-pected values. In this case, a (possibly extreme) up-per bound on the true but unknown risk is that it hasat most a 5% probability of exceeding the point es-timates (0.135 or 0.04 excess mortalities per year) bymore than 20-fold. To the extent that these point esti-mates are biased upward by the assumptions listed inTable I, upper bounds based on Markov’s inequalitywill be even more conservative.
5. DISCUSSION AND CONCLUSIONS
Concerns about penicillin use in food animalsand potential transfer of resistance to humans have

804 Cox, Popken, and Mathers
been debated over several decades. However, cur-rent knowledge and data, as analyzed in Table I, sug-gest that ongoing penicillin usage in food animals inthe United States creates at most quite minor mortal-ity risks to human health. Quantitatively, it appearsthat these risks are unlikely to exceed one potentiallypreventable mortality in the U.S. population roughlyevery 7–25 years. The true value could be smaller(and is zero if any of our key conservative qualitativeassumptions are incorrect).
Removing penicillin drugs from the animal drugmarket is a possible risk management option (andhas actually been proposed). But significant base-line resistance among antibiotic-free animals (Pattonet al., 2006), along with small potential human healthbenefits even if removal immediately eliminatedall preventable cases of resistance in human pa-tients (as Table I assumes) suggests that even com-plete product removal would not detectably improvehuman health. Increased surveillance of food-animal-associated enterococci and tracking theirpenicillin and ampicillin resistances (NARMS, 2005),as well as compliance with judicious use guidelinesfor practitioners and producers (AVMA, 2008), maysuffice to protect human health against the currentsmall risks without compromising the health of foodanimals.
ACKNOWLEDGMENTS
We thank Alpharma for supporting the re-search reported here. The research questions ad-dressed, methods and models applied, and conclu-sions reached are solely those of the authors.
REFERENCES
American Veterinary Medical Association (AVMA). AmericanVeterinary Medical Association Judicious Therapeutic Useof Antimicrobials December, 2005. Available at http://www.avma.org/issues/jtua/default.asp, 2008 (accessed December31, 2008).
Animal Health Institute (AHI). Animal Health Companies MeetIncrease Market Need for Antibiotics. Washington, DC:News Release from the Animal Health Institute, Octo-ber 12, 2006. Available at http://www.ahi.org/mediacenter/documents/Antibioticuse2005REVISED.pdf (accessed De-cember 31, 2008).
Austin DJ, Bonten MJM, Weinstein RA, Slaughter S, AndersonRM. Vancomycin-resistant enterococci in intensive-care hos-pital settings: Transmission dynamics, persistence, and the im-pact of infection control programs. Proceedings of NationalAcademy of Sciences of USA, 1999; 96:6908–6913. Availableat http://www.pnas.org/ (accessed December 31, 2008).
Biavasco F, Foglia G, Paoletti C, Zandri G, Magi G, GuaglianoneE, Sundsfjord A, Pruzzo C, Donelli F, Facinelli B. VanA-type
Enterococci from humans, animals and food: Species distri-bution, population structure, Tn1546-typing and location, andvirulence determinants. Applied and Environmental Microbi-ology, 2007; 73(10):3307–3319.
Bischoff WE, Reynolds TM, Hall GO, Wenzel RP, Edmond MBMolecular epidemiology of vancomycin resistant Enterococ-cus faecium in a large urban hospital over a 5-year period.Journal of Clinical Microbiology, 1999; 37(12):3912–3916.
Cox LA, Popken DA. Quantifying human health risks from vir-giniamycin used in chickens. Risk Analysis, 2004; 24(1):271–288.
Deshpande LM, Fritsche TR, Moet GJ, Biedenbach DJ, JonesRN. Antimicrobial resistance and molecular epidemiology ofvancomycin-resistant enterococci from North America andEurope: A report from the SENTRY antimicrobial surveil-lance program. Diagnostic Microbiology and Infectious Dis-ease, 2007; 58(2):163–170.
Edmond MB, Wallace SE, McClish DK, Pfaller M A, Jones RN,Wenzel RP. Nosocomial bloodstream infections in UnitedStates hospitals: A three-year analysis. Clinical Infectious Dis-eases, 1999; 29(2):239–244.
FAO/WHO/OIE. Joint FAO/WHO/OIE Expert Meeting on Crit-ically Important Antimicrobials. Report of a meeting held inFAO, Rome, Italy, 26–30 November 2007. FAO, Rome, Italy,and WHO, Geneva, Switzerland, 2008.
Fortun J, Coque TM, Martin-Davila P, Moreno L, Canton R, LozaE, Baquero F Moreno S. Risk factors associated with ampi-cillin resistance in patients with bacteraemia caused by En-terococcus faecium. Journal of Antimicrobial Chemotherapy,2002; 50(6):1003–1009.
Guardabassi L, Dalsgaard A. Occurrence, structure, and mo-bility of Tn1546-like elements in environmental isolates ofvancomycin-resistant enterococci. Applied and Environmen-tal Microbiology, 2004; 70(2):984–990.
Hanrahan J, Hoyen C, Rice LB. Geographic distribution of a largemobile element that transfers ampicillin and vancomycin re-sistance between Enterococcus faecium strains. AntimicrobialAgents and Chemotherapy, 2000; 44:1349–1351.
Hayes JR, English LL, Carr LE, Wagner DD Joseph SW Multiple-antibiotic resistance of Enterococcus spp. isolated from com-mercial poultry production environments. Applied and Envi-ronmental Microbiology, 2004; 70(10):6005–6011.
Hayes JR, English LL, Carter PJ, Proescholdt T, Lee KY, WagnerDD, White DG. Prevalence and antimicrobial resistance ofEnterococcus species isolated from retail meats. Applied andEnvironmental Microbiology, 2003; 69(12):7153–7160.
Institute of Medicine (IOM). Human Health Risks with the Sub-therapeutic Use of Penicillin or Tetracyclines in Animal Feed.Report by the Committee of Human Health Risk Assess-ment of Using Subtherapeutic Antibiotics in Animal Feeds,Institute of Medicine, IOM-88-89. Washington, DC: NationalAcademy Press, 1989.
Jones ME, Draghi DC, Thornsberry C, Karlowsky JA, Sahm DF,Wenzel RP Emerging resistance among bacterial pathogensin the intensive care unit—A European and North Amer-ican surveillance study (2000–2002). Annals of ClinicalMicrobiology and Antimicrobials, 2004; 3(14): 1–11. Avail-able at http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=509280 (accessed December 31, 2008).
Kuhn I, Iversen A, Finn M, Greko C, Burman LG, Blanch AR,Vilanova X, Manero A, Taylor H, Caplin J, Dominguez L,Herrero IA, Moreno MA, Mollby R. Occurrence and relat-edness of vancomycin-resistant enterococci in animals, hu-mans, and the environment in different European regions.Applied and Environmental Microbiology, 2005; 71(9):5383–5390.
Leavis HL, Bonten MJ. Willems RJ. Identification of high-risk en-terococcal clonal complexes; global dispersion and antibiotic
Human Health Risk Assessment of Penicillin/Aminopenicillin Resistance 805
resistance. Current Opinions in Microbiology, 2006; 9(5):454–460.
Leavis HL, Willems RJ, van Wamel WJ, Schuren FH, Caspers MP,Bonten MJ. Insertion sequence-driven diversification createsa globally dispersed emerging multiresistant subspecies of E.faecium. PLoS Pathogens, 2007; 3(1): e7.
Leavis HL, Willems RJ, Top J, Spalburg E, Mascini EM, FluitAC, Hoepelman A, de Neeling AJ, Bonten MJ. Epidemicand nonepidemic multidrug-resistant Enterococcus faecium.Emerging Infectious Diseases, 2003; 9(9); 1108–1115.
Lee CE, Zembower TR, Fotis MA, Postelnick MJ, GreenbergerPA, Peterson LR, Noskin GA. The incidence of antimicrobialallergies in hospitalized patients: Implications regarding pre-scribing patterns and emerging bacterial resistance. Archivesof Internal Medicine, 2000; 160(18):2819–2822.
Macovei L, Zurek L. Ecology of antibiotic resistance genes: Char-acterization of enterococci from houseflies collected in foodsettings. Applied and Environmental Microbiology, 2006;72(6):4028–4035.
McGowan LL, Jackson CR, Barrett JB, Hiott LM, Fedorka-Cray.Prevalence and antimicrobal resistance of enterococci iso-lated from retail fruits, vegetables, and meats. Journal of FoodProtection, 2006; 69(12): 2976–2982.
Murray BE. Vancomycin-resistant enterococcal infections. NewEngland Journal of Medicine, 2000; 342(10):710–721.
National Antimicrobial Resistance Monitory System (NARMS).NARMS Retail Meat Annual Reports, 2002–2005. Avail-able at http://www.fda.gov/cvm/narms˙pg.html#Publications(accessed December 31, 2008).
Patton BS, Cast WR, Kocher ME, Matthews JO, Griffith RW,Hurd HS, Dickson JS. The Effect of Swine Production Systemon Bacterial Prevalence and Antibiotic Resistance. Procced-ings of the Poster Presentation at International Associationfor Food Protection (IAFP) 2006, Calgary, Alberta, Canada,August 13–16, 2006. Abstract available at http://www.foodprotection.org/meetingsEducation/IAFP%202006/IAFP%2006%20Poster%20Abstracts.pdf (accessed December 31,2008).
Rice LB. Emergence of vancomycin resistant enterococci. Emerg-ing Infectious Diseases, 2001; 7(2):183–187.
Rodrigues J, Poeta P, Martins A, Costa D. The importanceof pets as reservoirs of resistant Enterococcus strains, withspecial reference to vancomycin. Journal of VeterinaryMedicine B, 2002; 49(6):278–280.
Sechen S. The review of animal production drugs by FDA. FDAVeterinarian, 2006; 21(1):8–11. Available at http://www.fda.gov/cvm/Documents/FDAVetVolXXINo1.pdf (accessed De-cember 31, 2008).
Suppola J, Kolho E, Salmenlinna S, Tarkka E, Vuopio-VarkilaJ, Vaara M. VanA and VanB incorporate into an endemicampicillin-resistant vancomycin-sensitive Enterococcus fae-cium strain: Effect on interpretation of clonality. Journal ofClinical Microbiology, 1999; 37(12):3934–3939.
Top J, Willems R, Blok H, de Regt M, Jalink K, Troelstra A,Goorhuis B, Bonten M. Ecological replacement of Enterococ-cus faecalis by multiresistant clonal complex-17 Enterococcusfaecium. Clinical Microbiology and Infection, 2007; 13(3):316–319.
U.S. Food and Drug Administration—Center for VeterinaryMedicine (FDA-CVM). FDA Database of Approved Ani-mal Drug Products. FDA Center for Veterinary Medicine,VMRCVM Drug Information Lab, 2007, Available athttp://dil.vetmed.vt.edu/ (accessed December 31, 2008).
U.S. Food and Drug Administration—Center for VeterinaryMedicine (FDA-CVM). Risk Assessment of StreptograminResistance in Enterococcus Faecium Attributable to theUse of Streptogramins in Animals. Draft for Comment,November 23, 2004. Available at http://www.fda.gov/cvm/Documents/SREF RA FinalDraft.pdf (accessed December31, 2008).
U.S. Food and Drug Administration—Center for VeterinaryMedicine (FDA-CVM). Guidance for Industry # 152: Eval-uating the Safety of Antimicrobial New Animal Drugs withRegard to Their Microbiological Effects on Bacteria ofHuman Health Concern. U.S. Department of Health andHuman Services, Food and Drug Administration, Centerfor Veterinary Medicine, 2003. Available at http://www.fda.gov/cvm/Guidance/fguide152.pdf (accessed December 31,2008).
U.S. Food and Drug Administration—Center for VeterinaryMedicine (FDA-CVM). Review of Agricultural Antibi-otics Policies, 2000. Available at http://www.fda.gov/cvm/HRESP106 157.htm#nrdc (accessed December 31, 2008).
Varman M, Chatterjee A, Abuhammour W, Johnson WC.Enterococcal infection, 2006. Emedicine.com. Available athttp://www.emedicine.com/ped/topic2703.htm (accessed July26, 2006).
Webb M, Riley LW, Roberts RB. Cost of hospitalization for andrisk factors associated with vancomycin-resistant Enterococ-cus faecium infection and colonization. Clinical InfectiousDiseases, 2001; 33(4):445–452.
Willems RJ, Top J, van Santen M, Robinson DA, Coque TM,Baquero F, Grundmann H, Bonten MJ. Global spreadof vancomycin-resistant Enterococcus faecium from distinctnosocomial genetic complex. Emerging Infectious Diseases,2005; 11(6), 821–828.
Willems RJ, Horman W, Top J, van Santen-Verheuvel M,Tribe D, Manzioros X, Gaillard C, Vandenbroucke-GraulsCMJE, Mascini EM, van Kregten E, van Embden JDABonten MJ. Variant esp gene as a marker of a distinctgenetic lineage of vancomycin resistant Enterococcus fae-cium spreading in hospitals. Lancet, 2001; 357(9259), 853–855.
Willems RJ, Top J, Van Den Braak N, van Belkum A, Endtz H,Mevius D, Stobberingh E, Van Den Bogaard A, van Emb-den JDA. Host specificity of vancomycin-resistant Enterococ-cus faecium. Journal of Infectious Diseases, 2000; 182(3):816–823.
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP,Edmond MB. Nosocomial bloodstream infections in US hos-pitals: Analysis of 24,179 cases from a prospective nation-wide surveillance study. Clinical Infectious Diseases, 2004;39(3):309–317.
World Health Organization (WHO). Critically Important An-tibacterial Agents for Human Medicine for Risk ManagementStrategies of Non-Human Use. Report of a WHO Work-ing Group Consultation February 15–18, 2005. Canberra,Australia, 2005. Available at http://www.who.int/entity/foodborne disease/resistance/FBD CanberraAntibacterialFEB2005.pdf (accessed December 31, 2008).
World Health Organization (WHO). Joint FAO/WHO/OIEMeeting on Critically Important Antimicrobials. Report ofthe FAO/WHO/OIE Expert Meeting. FAO Rome Italy.November 26–30, 2007. Available at http://www.who.int/foodborne disease/resources/Report%20joint%20CIA%20Meeting.pdf (accessed December 31, 2008).





























