Embed Size (px)
Citation preview

aInformation Paper: Human Health Vulnerability to Climate Change in Fiji
Human Health Vulnerability to Climate Change in Fiji

1 Introduction 12 Background- Key Health Indicators for Fiji 23 Observed Impacts of Historical Climate Variability on Human Health in Fiji 3 3.1. Communicable Disease 3 A. Dengue Fever 3 B. Diarrhoeal illnesses 5 C. Typoid Fever 7 D. Leptospirosis 8 E.SexuallyTransmittedInfections 9 3.2 Non- Communicable Diseases 10 A. Heart-related illness 10 B.Malnutrition-relatedillness 10 C. Death and Injury from extreme events 11 D. Psychological impacts 11 3.3 Access to Health Services 124 Projected Impacts of Climate Change on Human Health in Fiji 135 AdaptationMeasures 14 A.Healthsectoradaptationmeasures 14 B.Naturaldisaster-specificmeasures 14 C.Adaptationinothersectors-water,agriculture, 15 ruraldevelopment,housing,environment,communityempowerment andlivelihoods,energy,etc.6 Conclusion 167 References 17
Contents
This information paper is an output from the Piloting Climate Change Adaptationto Protect Human Health (PCCAPHH) project in Fiji, 2013”.

1Information Paper: Human Health Vulnerability to Climate Change in Fiji
Climate changenegatively impacts thebasic determinants of humanhealth- clean air, safe and sufficient
water,foodandshelter.Directimpactsofclimatechangeonhealthincludeinjury,diseaseanddeathfrom
extremeheatandcold, cyclones,floodsanddroughts. Indirect impacts include increases in vector-borne,
water-borne, cardiovascular, respiratoryand renaldiseasesandpsychosocial impacts from increase in the
rangeandnumberofdiseasespreadingvectors,compromisedfoodandwatersources,livelihoodlossesand
populationdisplacement.Fijiisespeciallyvulnerabletoadversehealthimpactsofclimatechange,duetoits
smallgeographicalsize,exposuretoextremeclimateeventsandasmalleconomythatdependslargelyon
natural resources.
This information paper demonstrates the impacts of climate variables, like temperature and rainfall and
extremeeventsonhumanhealthinFijiandlistssomeadaptationmeasuresthatneedtobeimplemented.
Thereareclear linksbetweenclimateandcommunicablediseases(CDsor infectiousdiseases) likedengue
and typhoid fevers, leptospirosis anddiarrhoeal illnesses andbetweenextremeclimateevents likefloods
anddroughtsandmalnutrition.Anecdotalevidencefromhealthpractitionersalsosuggestsalinkwithnon-
communicablediseases(NCDs),particularlythoserelatedtonutritionaldeficiencies.Whilefurtherresearchis
requiredtoidentifythetrueburdenofclimate-attributablehealthrisksinFiji,enoughevidenceexistsglobally
tounderscoreadaptationandmitigation inthehealthandrelatedsectors(inparticular,energy,transport,
water,housingandagriculture).
1. Introduction

2 Information Paper: Human Health Vulnerability to Climate Change in Fiji
Inrecentyears,Fiji’spopulation(868,000in2011)hasincreasedat1%peryear.Inthepast50years,therural
populationhasdecreasedfrom70%tojustunder50%ofthetotal,whichhasputsignificantstrainonservices
inurbanareas,inparticularwaterandsanitation.Grossnationalincomepercapitahasbeenstableataround
$4500overthepast5years.Overall,23%ofthepopulationliveonlessthat$2perday(US$PPP);43%ofrural
populationand18%oftheurbanpopulationlivebelowthepovertyline.Incomeisunequallydistributed:the
top20%ofearnersreceive50%oftheincome,whilethepoorest20%receiveonly6%(WorldBank,2012).
Governmenthealthexpenditureisapproximately3.7%ofgrossdomesticproductannually(Snowdon,2012).
In2010,thetop2causesofmortalitywerediseasesofthecirculatorysystemandendocrine,nutritionaland
metabolicdiseases.Childmortalityfellfrom23.2/1000livebirthsin2009to17.7/1000livebirthsin2010.
Maternalmortalityfellfrom27.5/100,000livebirthsin2009to22.6/100,000livebirthsin2010(Ministryof
Health,2011).Poverty,theinabilityofmanytobuysufficientfoodandunhealthydietshavecausedsignificant
amountsofmicronutrient(especiallyiodineandiron)malnutrition(Snowdon,2012).Asurveyofyouthinthe
Suva-Nausoricorridorrevealedthat26%offemalesand17%ofmaleswereoverweight,morethan30%of
Indo-Fijianstudentswereunder-weightandlessthan30%ofstudentsengagedinanyphysicalactivity(Tuiketei
etal.,2010).
Approximately 82% of all deaths in Fiji are attributed to NCDs (WHO, 2011). Of these, 42% are from
cardiovasculardiseasesalone.AspertheFijiNCDSTEPSSurveyreport2002,theprevalenceofdiabeteswas
16.2%andprevalenceofhypertensionwas19.1%(MinistryofHealth,2005).Theseratesareanticipatedto
haveincreasedinthe2011NCDSTEPSSurvey.Interestingly,thoughunfortunately,mortalityduetodiabetes
for2011wasrecordedtobe53.5%morethanin2010.Theprevalenceofcancersin2011wasnotedtobe
10.9%withthefemaletomaleratiobeing3:1(MoH,2012a).
WithregardstoCDs,theincidenceoftuberculosis,adiseaseofpoverty,declinedbetween2009and2010
(MinistryofHealth,2011).Inthelast50years,aboutsixdistinctoutbreaksofdenguewereexperiencedin
thecountry.Onaverage,about20-100casesofleptospirosisarereportedinthecountryannually.Whiledata
showsthattheincidence(numberofcasesper100,000ofpopulation)oftyphoidfevermaybeincreasing,
improveddiagnosisandreportingsince2005mayhelpexplaintheriseinnumbers.Together,denguefever,
leptospirosisandtyphoidfeverareconsideredthecountry’s“ThreePlagues”andwithdiarrhoea,aremajor
publichealthconcerns(PCCAPHH,2012).In2010,19,234casesofdiarrhoeawererecordednationally(Ministry
ofHealth,2011).Between1995and2010,theincidenceofdiarrhoeawasnearlyalwaysmorethan500cases
permonth(PCCAPHH,2012).Whilediarrhoeaisknowngloballytobesensitivetoclimateconditions,poor
waterandsanitationconcernsalsoplayamajorrole.Nearlyallofthepopulationissaidtohaveaccessto
improvedwatersources,but70%oftheruralpopulationdonothaveimprovedsanitation(WorldBank,2012).
2. Background- Key Health Indicators for Fiji

3Information Paper: Human Health Vulnerability to Climate Change in Fiji
3. Observed Impacts of Historical Climate Variability on Human Health in Fiji
Evidenceisgrowinggloballyofvarioushealthoutcomesbeingsensitiveto,ornegativelyaffectedby
climatevariabilityandchange.Globalevidencealsoshowsthatclimatechangewillnegativelyimpact
environmentalandsocio-economicdeterminantsofhealth,whichinturnwillresultinahigherglobal
burdenofcommunicableandnon-communicablediseases(WHO,2009).Resultsofstudiesonthe
climate-sensitivityofdiseasesandhealthdeterminantsinFijiaresummarisedhereafter.

4 Information Paper: Human Health Vulnerability to Climate Change in Fiji
3.1 Communicable Diseases
A. Dengue fever
Inastudyconducted in1999,positivecorrelationswere indentified fordengueandLaNinaconditions in
thePacific(Halesetal.,1999).OftheeightdengueoutbreaksthatoccurredinFijioverthelast50years,7
occurredduringperiodsofLaNina(wetconditions),whilethe1998outbreakoccurredduringtheanElNino
(dryconditions)period(PCCAPHH,2012). It isthoughtthiswasduetopeoplestoringwater inun-covered
containersclosetotheirhomesandthatthesecontainerswereidealbreedingsitesfortheAedesmosquito
(FMS,2003a).FollowingthefloodsinJanuaryandMarch,2012,theincidenceofdenguefeverwasveryhighin
theWesternDivision.Vectorindicesanddenguecasenumbersbothpeakedamonthfollowingtherespective
floods.ThehighestnumberoflaboratoryconfirmedcaseswerenotedintheLautokaandNadisub-divisions
(MinistryofHealth,2012b).DengueoutcomesinLautokafollowingthefloodswereconsistentwiththeresults
forLautokainTable1below.
ThejointMinistryofHealth-WHO-UNDPPilotingClimateChangeAdaptationtoProtectHumanHealthutilised
historical monthly climate and communicable disease data from 1995-2009 and identified the following
associationsbetweendengueandclimateconditions.
Table 1: Summary of Poisson Regression Between Monthly Dengue Fever Cases and Monthly ClimateVariables in Four Medical Sub-Divisions in Fiji
Medical Sub-division
Climate variable/modela Strength of Association (pseudo r2 value)b
Notes:a Seasonallyadjusted,usingadummy variable for months.bAllresultsaresignificanttothe5%level(p-values≤0.05)c Lagsrefertotherelationshipbetweendiseasenumbersinaparticularmonthandclimateconditionsofthesamemonth(lag0),or1,2,3monthsprior(lags1,2,3)respectively.d Maximum temperaturee Minimum temperature
Ba Rainfall(mm)-lagc1,2,3Maxtemp(°C)d-lag0,1,2,3Mintemp(°C)e- lag 2RelativeHumidity(%)-lag1
BestModel:Rainfall,Maxtemp,Humidity at lag 1
0.3,0.27,0.320.29,0.38,0.32,0.290.250.340.39
Bua Rainfall-lag0,1,2Maxtemp-lag0,2,3Mintemp-lag0,1,2,3Humidity- lag 0
Bestmodel:Rainfall,Maxtemp,Mintemp at lag 0
0.4,0.3,0.370.37,0.33,0.310.35,0.30,0.32,0.310.330.52
Lautoka Rainfall- lag 1Maxtemp- lag 1Mintemp- lag 1
Bestmodel-Rainfall,Maxtemp,Mintemp at lag 1
0.420.530.270.54
Suva Rainfall- lag 2Maxtemp- lag 3Mintemp-lag0,2Humidity- lag 2
Best model- All four climate variables at lag 2
0.470.500.57,0.520.470.6
(Source:PCCAPHH,2012)

5Information Paper: Human Health Vulnerability to Climate Change in Fiji
Wherehigherr2valuesareseen(Lautoka,SuvaandBua)climateconditionscanbesaidtoexplaindengue
feveroutcomestoagreaterextent.Inothersub-divisions,theassociationswereweakerbutstillstatistically
significant.
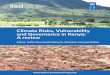
Relationshipsbetweendengueandclimateappearedtobenonlinear.Forexample,intheBuasub-division,
night-timetemperaturesaboveathresholdofapproximately25°Cappearconducivetodenguetransmission,
withatimelagof2months(Figure1).
Fig. 1: Monthly dengue cases vs. Average Monthly Minimum Temperature Two Months Prior in Bua

6 Information Paper: Human Health Vulnerability to Climate Change in Fiji
Furtherworkwasdonetodeterminetheassociationbetweendenguefeverandextremeclimateeventslike
droughts,cyclonesandfloods.ThelikelihoodofadengueoutbreakinBa,onemonthafterfloodscausedby
tropicaldepressionswas10timesmorethanmonthswhennotropicaldepressionoccurred.Furthermore,
thelikelihoodofadengueoutbreakinBaduringdroughtmonthswas5timesmorethanmonthswithout
droughts.
B. Diarrhoeal Illnesses
Singhetal.(2001)undertookastudyofdiarrhoeaininfantsinFijiandshowedpositiveassociationswithvery
lowandveryhighrainfallandincreasingtemperature(laggedbyonemonth).Singhetal.noteda3%increase
indiarrhoeacasesforevery1⁰Cincreaseintemperature,controllingforseasons.Highertemperaturescreate
conditionsthatallowpathogenstoproliferatewhilewatersupplyandsafety,aswellassanitationandhygiene
arecompromisedduringperiodsofdroughtsandfloods.FollowingtheMarch2012floods intheWestern
Division,watersupplyandsafetywerecompromisedinbothurbanandruralflood-affectedareas,resultingin
ahighincidenceofdiarrhoea.Inmanyareas,watertruckssuppliedwatertoaffectedfamilies;2779WASHkits
(containingwaterpurificationtablets,watercontainersandsoap),40largetanksandbladders,7,000water
containers,and9600sachetsofOralRehydrationSalts(ORS)werealsodistributed(UNOCHAPacific,2012).
AnalysisbythePCCAPHHproject(2012)producedthefollowingassociationsbetweenclimateanddiarrhoea.
Table 2: Associations Between Monthly Diarrhoeal Illnesses and Monthly Climate Variables in Three Medical Sub-Divisions in Fiji, 1995-2009
Medical Sub-division
Climate variable/modela Strength of Association (pseudo r2 value)b
Notes:aSeasonallyadjusted,usingadummy variable for months.bAllresultsaresignificanttothe5%level(p-values≤0.05)cLagsrefertotherelationshipbetweendiseasenumbersinaparticularmonthandclimateconditionsofthesamemonth(lag0),or1,2,3monthsprior(lags1,2,3)respectively.d Maximum temperaturee Minimum temperature
Ba Rainfall- lag 1Maxtemp- lag 3Mintemp-lag 3Humidity- lag 1
Bestmodel:Allforclimatevariablesabove
0.10.060.070.14
0.17
Bua Rainfall- lag 0Maxtemp-lag0,1,2Mintemp- lag 0-3Humidity- lag 2
Bestmodel:Rainfall,Maxtemp,Mintemp at lag 0
0.12All ~0.10All ~0.100.12
0.13
Suva Rainfall-lag1,3Maxtemp-lag0,3Mintemp- lag 3
Bestmodel:Threeclimatevariablesabove at lag 3
~0.4~0.4~0.4
0.41

7Information Paper: Human Health Vulnerability to Climate Change in Fiji
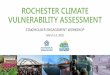
It is clear from theabove table thatother than in the Suva sub-division, the linear associationsbetween
monthlydiarrhoeaandmonthlyclimateconditionsarequiteweak.Whenthesamedatawasanalysedusing
theLowesssmoothingfortheSuvasub-divisionhowever,thefollowingU-shapedcurvewasnoted,similar
tofindingsbySinghetal.(2001)(Fig.2).ThisshowsthatintheSuvasub-division,diarrhoeacasesarehigher
duringperiodsofverylowandveryhighrainfall,butmorepronouncedduringdrierperiods(PCCAPHH,2012).
Fig. 2: Monthly Diarrhoea Cases vs. Average Monthly Rainfall in the same Month in Suva
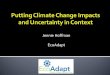
InterestingassociationswerealsonotedwithminimumtemperatureinSuvaforthesamemonthandaone-
monthlag(Fig.3below).Bothgraphssuggestthat25⁰Cisthethresholdminimum(night-time)temperature,
beyondwhichdiarrhoeacasesincreaseintheSuvasub-divisions(PCCAPHH,2012).Itisimportanttoconsider
minimumtemperaturesascoldertemperatureswillinhibittheproliferationofcertainpathogens.
Fig. 3. Association between Monthly Diarrhoea Cases and Minimum Temperature at Lags 0 (left) and 1 (right) in Suva

8 Information Paper: Human Health Vulnerability to Climate Change in Fiji
Analysis also revealed strongpositiveassociationswithextremeevents likefloodsandcyclones in theBa
medicalsub-division.ThelikelihoodofadiarrhoeaoutbreakinBaonemonthafterfloodingcausedbytropical
depressions is 9timesmore thanmonths inwhich tropical depressionsdonotoccur. In comparison, the
likelihoodofadiarrhoeaoutbreakonemonthafterallfloods is3.5timeshigher thanallmonthswithout
flooding(PCCAPHH,2012).
Analysisaboveshowstheneedtodesignadaptationmeasurestobothabruptandon-goingchangesinthe
climate,notingallthewhilethecommunicablediseasestotendtorisefollowingnaturalclimatedisasters.
C. Typhoid Fever
Typhoidfever isendemic inFiji.Outbreakshavebeennotedfollowingfloodsand2monthsaftercyclones
(Jenkins, 2010;Ramet al., 1983) andmass fooddistributionevents.Outbreaks in Koroboya andNaitasiri
(Tavuamedicalsub-division)andNanoko(Nadroga-Navosasub-division)in2012demonstratedthatpoverty,
poorsanitationandhygieneandthemovementofhealthycarriersarealsosignificantriskfactors.TheWestern
Division experienced typhoid outbreaks following the January and March 2012 floods, with the highest
numberofcasesreportedintheBasub-division,followedbytheNadiandLautokasub-divisions.Particularly
followingfloodsandcyclones,thecloseproximityofpeopleinevacuationcentresandcompromisedsanitary
andhygienefacilitiesinevacuationcentresalsocontributestotransmissionoftyphoid.TheMinistryofHealth
launchedapubliccampaignfollowingthefloodsanddistributedmorethan8000information,educationand
communicationmaterialsonpreventingtyphoidfeverandonmaintaininggoodhealthduringnaturaldisasters
(MinistryofHealth,2012b).

9Information Paper: Human Health Vulnerability to Climate Change in Fiji
Medical Sub-division
Climate variable/modela Strength of Association (pseudo r2 value)b
Notes:a Seasonallyadjusted,usingadummy variable for months.bAllresultsaresignificanttothe5%level(p-values≤0.05)cLagsrefertotherelationshipbetweendiseasenumbersinaparticularmonthandclimateconditionsofthesamemonth(lag0),or1,2,3monthsprior(lags1,2,3)respectively.d Maximum temperaturee Minimum temperature
Ba Rainfall-lag1,2,3Maxtemp-lag0,3Mintemp-lag1,2,3Humidity-lag0,1,2,3
Best model- Rainfall and Mintemp at lag 2
0.47,0.63,0.490.47,0.490.46,0.52,0.460.48,0.46,0.47,0.5 0.66
Bua Rainfall- lag 0Mintemp-lag0,3Humidity- lag 3
Best model- Rainfall and Mintemp at lag 0
0.350.36,0.360.35
0.36
AnalysisbythePCCAPHHproject(2012)producedthefollowingassociationsbetweenclimateandtyphoid
fever.
Table 3: Summary of Poisson Regression Between Monthly Typhoid Fever Cases and MonthlyClimate Variables in Two Medical Sub-Divisions in Fiji, 1995-2009
Typhoid outbreaks in the Ba sub-division are explained to a significant extent by rainfall and minimum
temperature of the area. Results for the Bua sub-division illustrate that other socio-economic determinants
can explain typhoid outbreaks in the area.
D. Leptospirosis
Over the last 15 years, between 20-100 cases of leptospirosis have been reported in Fiji annually.While
leptospirosisisendemicinFiji,outbreaksalsooccur.Globally,leptospirosisisknowntobesensitivetohigher
temperaturesandhigherrainfallpatternsintropicalareas.InFiji,youngmalefarmersareathigherriskastheir
occupationsexposethemtoinfectedanimalsorsoilandwatercontaminatedbyfaecesofinfectedanimals.It
isthoughtthatespeciallyfollowingfloodsandcyclones,peopleandleptospirosisvectors(domesticanimals,
rats)comeintocloserproximity,increasingtheriskoftransmission(PCCAPHH,2012).
Forexample,leptospirosisoutbreakswerenotedfollowingfloodsinJanuaryandMarch2012intheWestern
Division. In some cases, outbreaks occurred in evacuation centreswhere peoplewere in close proximity.
Furthermore,rodentsinBatownarethoughttohavecausedoutbreaksintownareasfollowingtheJanuary
andMarchfloods in2012 (MinistryofHealth,2012c). Thehighestnumbersof cases following thefloods
werereportedfromtheLautokasub-division,followedbytheBa,NadiandNadroga-Navosasub-divisions.The
highestnumberofdeathsduetoleptospirosiswasalsofromtheLautokaDivisionalHospital.Healthpromotion
messages to prevent leptospirosis were aired on Fiji TV and FBC,while approximately 6200 information,
education and communicationmaterials on the same subjectwere distributed to the public (Ministry of
Health,2012b).

10 Information Paper: Human Health Vulnerability to Climate Change in Fiji
AnalysisbythePCCAPHHprojectproducedthefollowingassociationsbetweenclimateandleptospirosis.
Table 4: Summary of Poisson Regression Between Monthly Leptospirosis Cases and Monthly Climate Variables in Two Medical Sub-Divisions in Fiji, 1995-2009
Medical Sub-division
Climate variable/modela Strength of Association (pseudo r2 value)b
Notes:aSeasonallyadjusted,usingadummy variable for months.bAllresultsaresignificanttothe5%level(p-values≤0.05)cLagsrefertotherelationshipbetweendiseasenumbersinaparticularmonthandclimateconditionsofthesamemonth(lag0),or1,2,3monthsprior(lags1,2,3)respectively.d Maximum temperaturee Minimum temperature
Ba Rainfall- lag 2Maxtemp-lag1,2Humidity-lag1,2
Bestmodel:Rainfalllag2andMintemp lag 1
0.30.32,0.30.3,0.3
0.35
Bua
Rainfall-lag0,2,3Maxtemp-lag0,3Mintemp-lag0,1,2,3Humidity-lag0,1Bestmodel:Rainfall,Maxtemp,Mintempatlag3
0.42,0.4,0.480.38,0.450.4(all)0.45,0.40
0.59
Thestrongestcorrelationbetweenaveragemonthlyclimateconditionsandmonthlyleptospirosiswasnoted
fortheBuasub-division,withamodelthatcombinedrainfall,maximumtemperateandminimumtemperature
at a lag of 3 months.
E. Sexually Transmitted Infections
While no quantitative studies have been undertaken to determine the association between sexually
transmittedinfections(STIs)andtheclimateinFiji,someobservationsfollowingtheJanuaryandMarchfloods
intheWesternDivisionarenotedbelow.Medicalpractitionersnotedanincreaseinunsafesexualactivities,
particularlyamongteenagersandyouths,andespeciallysoinevacuationcentres.Asaresult,groupactivities
likeyaqonaconsumptionwerebannedinmostevacuationcentrestoencourageparentstosupervisetheir
children.Furthermore,casesof rapeand incestwerealsonoted,especiallyonunaccompaniedwomen in
evacuationcentres.Topreventfurthercases,policeofficerswerepostedatevacuationcentresandwhere
necessary,womenwerehoused in separate rooms inevacuations centresandprovidedpoliceprotection
(MinistryofHealth,2012c).

11InformationPaper:HumanHealthVulnerabilitytoClimateChangeinFiji
3.2 Non-Communicable Diseases
Whilenon-communicablediseases(NCDs)areknowngloballytobesensitivetodiet,noquantitativestudies
havebeenundertakentodemonstrateassociationsbetweenNCDsandtheclimateinFiji.Thus,thisisanarea
ofresearch,especiallyassomeexamplesofassociationsarestartingtobecomemorevisibleandasNCDs
aresignificanthealthproblems.SomeofthepathwaysinwhichclimatechangecanaffectNCDsareexplored
below.
A. Heat-related illnesses
WhileFijidoesnotexperienceheat-waveslikethoseexperiencedinmanytemperatecountries,hotterdays
areexpectedtocreateconditionswherepeopleengageinlessphysicalactivity(workingonfarmsorexercising
outside).Thiscanleadtoariseinobesity,whichisariskfactorformanyNCDslikediabetes,cardio-vascular
illnesses,musculo-skeletaldisorders(likegoutandosteoarthritis)andsomecancerslikeendometrial,breast,
rectalandcoloncancer(NationalFoodandNutritionCentreandMinistryofHealth,2009). Increasedheat
levelscouldalsocauseincreasedrestlessnessinhighbloodpressurepatients,creatingconditionsforincrease
in related illnesses.
B. Malnutrition-related illnesses
Perhapsthemost importantpotentialpathway linkingclimatechangeandNCDs isvia foodandnutrition.
Currently,endocrine,nutritionalandmetabolicdiseasesarethesecondmostcommoncauseofmortalityin
Fiji(MinistryofHealth,2011).Extremetemperatures,aswellasnaturaldisasterslikedroughts,cyclonesand
floodscausesignificantdamagetoagriculturaloutput.Morethan12,000farmers lost theircropsandthe
agriculturesectoroverallincurredalossofmorethanFJD16maftertheMarch2012floods(UNOCHAPacific,
2012).ThisresultedinfreshfruitandvegetableshortagesthroughouttheWesternDivision.TheMinistryof
HealthdistributednutritionalsupplementsthatincludedVitaminAandmicronutrientstoavoidmalnutrition
inflood-affectedfamilies(UNOCHAPacific,2012).Wherefarmsareunabletorecoverfromnaturaldisasters,
long-termshortagesoffresh,localfruitsandvegetablesareexperienced.Asaresult,peopleconsumecanned
andpreservedfood,whichareoftenhighinsaltandsugar.Excessiveamountsofsaltandsugarincreasethe

12 Information Paper: Human Health Vulnerability to Climate Change in Fiji
riskofillnesseslikehigh-bloodpressure,strokesandcardio-vasculardiseases,diabetesandobesity.Anecdotal
evidencesuggestsanincreaseindiabeticfoot-sepsisamongpeopleintheEasternDivisiontwoyearsafter
CycloneTomas’destructionoffarmsinthearea.
Climate change is also causing sea surface temperatures and sea levels to rise and altering the mixing of ocean
layers which reduce nutrient availability and fish supply. Rising sea surface temperatures, and increasing
variabilityintheformoftheElNinoSouthernOscillationwillnegativelyimpactcoralreefs,leadingtofurther
reductioninfisheries(FAO,2008).SeafoodisanimportantsourceofproteininFijiandthelackoffreshfishwill
furtherpushconsumerstobuycannedfish,whicharenormallyhighinsalt.
Inthelong-term,damagessufferedbytheagricultureandfisheriessectorsmaycreatesignificantfoodsecurity
issues,includingverylargeincreasesinNCDsandveryhighdependenceonimportedfoods.
C. Death and injury from extreme events
Drowning fromswimming infloodedrivers,or trying tocrossfloodedcrossings isamajorcauseofdeath
duringfloodsandcyclones.Asummaryofdeathsfromrecentmajorcyclonesandfloodsispresentedbelow.
Table 5: Deaths During Major Recent Cyclones and Floods
Deathscausegriefandsorrowinaffectedfamiliesandiffamilieslosetheirbread-winners,thentheirlossesare
greater. Related impact on the mental health of family and friends is varied yet quite notable. The possibility
ofdepressionandstressincreasesduringsuchtimes.
D. Psychological impacts
A largely neglected health impact of climate change and extreme climate events, the UNOCHA Pacific
coordinatedHumanitarianResponseTeamrecognisedthisasan importantareafollowingtheMarch2012
floods (UNOCHAPacific,2012).Psychological stressanddepressioncanarise from lossof livelihoods (e.g.
droughtdamagetocrops),deathoforimmobilisinginjurytofamilymembers,lossofhomestofloodsand/or
cyclones,theinabilitytorecoverfromdisasters,conflictoverlimitedresourceslikewater/productivelandand
therelocationordisplacementofpopulationstolessvulnerable,andinsomecasesmorevulnerableareas.
Itcanaffectadults,childrenandyouthandcantaketheformof“socialisolation,mentaldisorders,reduced
socio-economicstatusandassociatedhealthproblems”(WHO,2009:12).
Extreme Event No. of deaths Source
HurricaneAmi(January2003) 17 FMS,2003b.
FloodsduetoTropicalDepression(January2009) 11 McGreeatal.,2010.
TropicalCycloneMick(December2009) 9 ABCNews,2009.
FloodsduetoTropicalDepression(March2012) 4 UNOCHAPacific,2012.

13Information Paper: Human Health Vulnerability to Climate Change in Fiji
3.3 Access to Health Services
HurricaneAmi(January2003)causedFJD857,000ofdamagetohealthinfrastructure(FMS,2003b).TheMarch
2012 floods caused FJD607,000 damage to health infrastructure (UNOCHA, 2012). Buildings, equipment,
drugsandrecordsgetdamagedfromwaterandwindandreplacementcostsareveryhigh.Electricityand
watercutsalsoseverely limit theoperabilityofhealth facilities. Inaddition,access tohealth facilitiesand
affectedcommunitiesisalsocut-offbyfloodedroadsandbridges.Transportingemergencycasestohospitals
becomesdifficultduringsuchtimes(MinistryofHealth,2012c)andhealthpractitionersareforcedtoattend
toemergencycasesatgreatpersonal risk.TheMinistryofHealthrecently reviewed itsHealthEmergency
andDisasterManagementActionPlan (HEADMAP),which includesStandardOperatingProcedures (SOPs)
toaddresssomeoftheissuesraisedhere.Currentpracticeduringdisastersisforhealthteams,comprising
medicalofficers,nurses,environmenthealthofficersanddieticians,toundertakeshiftclinicsandoutreachin
evacuationcentresandcommunitiestomaintainpopulationaccesstohealthservices.

14 Information Paper: Human Health Vulnerability to Climate Change in Fiji

15Information Paper: Human Health Vulnerability to Climate Change in Fiji
4. Projected Impacts of Climate Change on Human Health in Fiji
Fiji’s climate is projected to continue towarmover the coming century.Days andnights are expected to
becomewarmer,with35⁰Cdaysandover16⁰C-21⁰Cnightsbecomingregularoccurrencesby2100.Generally,
thecountry isprojectedtogetdrierandsea levelsareexpectedtorise (GovernmentofFiji,2012).These
changeswillhaveprofoundimpactsonavailabilityofwater,agriculture,foodandlivingconditions.Inother
words,climatechangewillcontinuetocompromisethebasicdeterminantsofhumanhealth.
Studies undertaken using the PACCLIM model in 2005 (Government of the Fiji Islands, 2005) projected
increasesintheincidenceofdenguefever,diarrhoeaandnutritionrelatedillnessesinFiji.Using1990asthe
baseline,43%ofVitiLevuwasfoundtobeat lowriskofadengueoutbreak.By2100,evenundertheB2
(sustainabledevelopment)scenario,only21%ofVitiLevu(interioroftheisland)wasprojectedtobeatlow
riskofadengueoutbreak,withtheremainderofthepopulationestimatedtobeatmoderatetohighriskof
anoutbreak.Whentheworstcasescenario(A2)wasconsidered,45%ofVitiLevu’spopulationwasprojected
tobeathightoextremeriskofanoutbreakby2100.Thestudyalsoconcludedthatasaresultofwarming,the
frequencyofepidemicsmayincrease,epidemicsmayceasetobeseasonal(occuratanytimeoftheyear)and
evenbecomeendemic,andthemorbidityandmortalityfromepidemicscouldrisesignificantly.
ThesamestudyconcludedthatasFijitrendstowardsawarmerclimatewithmorefrequentdroughts,water
andsanitationwouldbecompromisedleadingtoincreaseddiarrhoealoutbreaks.Nutritionrelatedillnesses
werealsoprojectedtoincreaseasextremeeventsoccurmorefrequentlyandincreaseinintensity.Finally,
thestudyprojectedserioushealthimpactsifclimatechangedisruptedFiji’ssocial,economicandecological
systems(GovernmentoftheFijiIslands,2005).
Failure to adapt locally and mitigate globally would result in the above impacts being felt in Fiji. Some
adaptationmeasurestoprotecthumanhealthfromclimatechangearelistedbelow.

16 Information Paper: Human Health Vulnerability to Climate Change in Fiji
5. Adaptation Measures
Somemeasures to protect human health against the impacts of climate change are outlined below. It is
important tonote that improvedhumanhealthoutcomeswilldependonadaptationandprogress inALL
developmentsectors.AtarecentglobalWebinaronclimatechangeandhealth,Prof.KrisEbi,aninternational
expertonthesubjectmadethefollowingcommentsabouthealthadaptation.Firstly,itwillhavetobeiterative
i.e.measureswillhavetomodifiedasclimatechangesinthefuture.Secondly,thereisenoughevidenceto
startimplementingadaptationactivities,includingmanywin-winactivities(AlertNet,2012).
A. Health sector adaptation measures
Manyadaptationoptionsforthehealthsectorinvolvestrengtheningexistingdiseasesurveillance,monitoring
andcontrolmeasureswhileothersrequiresystematicallyincorporatingclimateinformationinhealthplanning
andinterventions.SomehealthadaptationmeasuresforFijiinclude:
• Continuoushealthvulnerabilityassessmentforcommunicableandnon-communicablediseasesandfor
safetyandaccessibilityofhealthfacilities/healthcare.
• Improveaccesstoprimaryhealthcare.
• Integratedvectormanagementbybuildingorstrengtheningpartnershipswithrelevantstakeholders.
• Facilitaterapidandaccuratediseasenotification.
• Identifyandprotect thehealthof themostvulnerablemembersof society (elderly,disabled,women,
children,poor).
• Vaccinate humans against diseases like typhoid fever and livestock and pets against diseases like
leptospirosis.
• On-goingeducationandtrainingonclimatechange,disasterriskreduction,communityhealthadaptation,
etc.
• Incorporateclimatechangeintoexistinghealthpoliciesandplans.
B. Natural disaster-specific measures
• Strengthendisasterriskreduction,recoveryandresponseprogrammes.ThisincludesStandardOperating
Procedures and health staff and facilities being adequately resourced (funding, personal protective
equipment,foodrations,electricity,water,communications).
• Improvecoordinationamonginter-sectoralpartners(DISMACandUNHumanitarianAssistancegroup).
• Developorstrengthenearlywarningsystems.
• Climate-proofhealthinfrastructure.Thisincludesrelocatinghealthfacilitiesiftheyareinvulnerableareas,
ensuringfacilitieshaveback-uporrenewableelectricity,water(e.g.installationofwatertanks),sufficient
drugs and supplies during natural disasters and undertaking regular repair and maintenance.

17Information Paper: Human Health Vulnerability to Climate Change in Fiji
C. Adaptation in other sectors- water, agriculture, rural development, housing,
environment, community empowerment and livelihoods, energy, etc.
TheWHOarguesthathumanhealthshouldbethebottomlineofalladaptationactivitiesandprogrammes
(WHO,2009).Ahealthypopulationisaresilientpopulationandforthesereasons,ALLdevelopmentsectors
inFijimustaimtoimprovehumanhealthoutcomesthroughtheiradaptationactivities.Someprioritysectoral
andinter-sectoraladaptationmeasuresarehighlightedbelow.
• Providecleanwater, improvedsanitationandhouseholddisinfectionespecially inareaswheredisease
incidence is higher.
• Improvesocialindicatorslikeeducation,women’sempowerment,improvedhousingandequitableaccess
todevelopmentopportunities.
• Improveeconomicindicatorslikeemploymentrate,alternativelivelihoodsandaccesstomarkets.
• Enhancecommunityresilienceagainstclimatechangeanddisasters.
• Encourageagriculturaldiversificationandsustainableagriculture.Discouragefarminginmarginalareas.
• Thenaturalenvironmentisasourceoffood,shelter,medicine,cleanwaterandair.Italsoactsasabuffer
againstextremeclimateeventslikefloodsandcyclones.Moreover,anunpollutedenvironmentissafefor
humanhabitationwhereasanalteredenvironmentmaycreateconditionsfordiseasemicrobesandvectors
tospread.(Corvalanetal.,2005).Forthesereasons,ecosystemsmustbeprotectedfromunsustainable
use.
• Localmitigationmeasures like increaseduseofpublic transportation,walking/cycling insteadofusing
fossil-fuelpowered transport,useofefficientwood-stoves thatemit lesssmokecreateco-benefits for
healthwhilereducinggreenhousegasemissions.
(MinistryofHealth,2012c;WHO,2009)

18 Information Paper: Human Health Vulnerability to Climate Change in Fiji
6. Conclusion
Tosummarise,healthfacilitiesandhealthcareservices,communicableandnon-communicablediseasesandall
thebasicdeterminantsofhealtharesensitivetoclimateconditions.Impactsareprojectedtobecomeworseas
climatechangecontinues.Thishighlightstheneedforurgentadaptationinthehealthandotherdevelopment
sectorsandurgent,up-scaledmitigationofgreenhousegasesglobally.Toconclude,humanhealthshouldbe
thebottom-lineofalladaptationactivitiesandincreasedfundsarerequiredtosecurethenecessaryhuman
andotherresourcesforadaptationtotakeplaceattherequiredrate.

19Information Paper: Human Health Vulnerability to Climate Change in Fiji
References:
ABCRadioAustralia.2009.DamagedandDisplacedafterFijiCyclone,15December2009.Accessedon3rd
November2011,viaURL:http://www.radioaustralia.net.au/pacbeat/stories/200912/s2771752.htm
AlertNet. 2012. Hunger Might be Largest Health Impact of Climate Change- Expert. Accessed on 2nd October
2012,viaURL:http://www.trust.org/alertnet/news/hunger-may-be-largest-health-impact-of-climate-change-
expert/
Corvalan,C.,Hales,S.andMcMichael,A.2005.EcosystemsandHumanWell-Being:HealthSynthesis:Areport
oftheMillenniumEcosystemAssessment.WHO,Geneva.
FijiMeteorologicalService.2003a.InformationSheetNo.126.ListofDroughtsthathaveOccurredinFijisince
1965.FMS,Nadi.
- 2003b.InformationSheetNo.123.ListofTropicalCyclonesinFiji.FMS,Nadi.
FoodandAgricultureOrganisation.2008.ClimateChangeandFoodSecurityinPacificIslandCountries.FAO,
Rome.
GovernmentofFiji.2012.RepublicofFijiNationalClimateChangePolicy.SPC,Suva.
- 2005.Fiji’sInitialNationalCommunications.PacificIslandsClimateChangeAssistanceProgramme,Apia.
Hales,S.,Weinstein,P.,Soures,Y.andWoodward,A.1999.ElNinoandtheDynamicsofVector-borneDisease
Transmission.EnvironmentHealthPerspectives107(2):99-102.
Jenkins,K.TyphoidfevercontrolinFiji.ProceedingsoftheEcohealthForum,Suva,Fiji26thNovember2010.
McGree,S.,Yeo,S.W.andDevi,S.2010.FloodingintheFijiIslandsBetween1840and2009.RiskFrontiers,
MacqaurieUniversity,Sydney.
MinistryofHealth.2005.FijiNonCommunicableDiseases(NCD)STEPSSurveyReport.MinistryofHealth,Suva
- 2011.AnnualReport2010.MinistryofHealth,Suva.
- 2012a.HealthInformationUnitData.MinistryofHealth,Suva.
- 2012b. Integrated Communicable Disease Report. Issue 1 Jan-May 2012. Ministry of Health, Suva
(unpublishedreport).
- 2012c.SWOTAnalysisoftheMinistryofHealth’sResponsetoFloodingintheWesternDivisioninJanuary
andMarch2012.MinistryofHealth,Suva(unpublishedreport).
NationalFoodandNutritionCentreandMinistryofHealth.2009.NutritionandNCDFactsheets.NFNCand
MinistryofHealth,Suva.
PCCAPHH. 2012. Fiji: Protecting Health from Climate ChangeWorking Paper: Climate-Sensitive Infectious
DiseasesinFiji.2011SummaryreportfromFiji’sPilotingClimateChangeAdaptationtoProtectHumanHealth
project.WHO-SPandFijiMinistryofHealth,Suva.

20 Information Paper: Human Health Vulnerability to Climate Change in Fiji
Ram,P.,Mataitoga,V.,Seruvatu,L.1983.TyphoidFeverinFijiin1982:EpidemiologicalAspects.FijiMedical
Journal1983(11):124-128.
Singh,R.B.K.,Hales,S.,deWet,N.,Raj,R.,Hearnden,M.andWeinstein,P.2001.TheInfluenceofClimate
VariationandChangeonDiarrhoealDiseaseinthePacificIslands.EnvironmentHealthPerspectives109(2):
155-159.
Snowdon,W. 2012. Legislation toMandate the Supply of Fortified Flour in Fiji: DesktopReviewof Policy
DevelopmentProcess.ConsultancyReportfortheNationalFoodandNutritionCentreandMinistryofHealth.
NFNCandMinistryofHealth,Suva.
Tuiketei,T., Snowdon,W.,Wade,G.,Kremer,P., Schultz, J.andVanualailai,N.2010.ObesityPrevention in
Community (OPIC) Project- Fiji Report 2004-2008. Deakin University, Melbourne and the Fiji School of
Medicine,Suva.
UNOCHAPacific.2012.Fiji.FloodingTropicalDepressionTD17F-2012.SituationReportNo.4.12thApril2012.
UNOCHAPacific,Suva.
WHO.2009.ProtectingHealthfromClimateChange:ConnectingScience,PolicyandPeople.WHO,Geneva.
WorldBank.2012.DataFiji.AccessedonSeptember28th2012viaURL:data.worldbank.org./country/Fiji

21Information Paper: Human Health Vulnerability to Climate Change in Fiji
Photoscourtesyof:Fiji Times LiveandLearn,FijiMinistry Of HealthWorldHealthOrganization
Designedby:PasifikaCommunication

22 Information Paper: Human Health Vulnerability to Climate Change in Fiji