Embed Size (px)
Citation preview

Hypercoagulable Syndromes

Risk Factors For Venous ThrombosisACQUIRED INHERITED MIXED/UNKNOWNAdvancing age Antithrombin Deficiency Homocysteine Obesity Protein C Deficiency Factor VIIIPrior thrombosis Protein S Deficiency APC resistanceImmobilization Factor V Leiden (FVL) in the absenceMajor surgery Prothrombin G20210A of FVL Malignancy Dysfibrinogenemias Factor IXEstrogens (rare) Factor XI (OCP, HRT, SERMs) TAFIAntiphospholipid Free TFPI antibody syndrome fibrinolytic activityMyeloproliferative disordersIBD, Nephrotic syndromeHeparin-induced thrombocytopeniaProlonged air travel

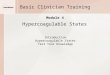
VTE Risk Factor Model
Intrinsic Thrombosis
Risk
Acquired Risk FactorsGenes ++
VTE
Triggering Factors
Prophylaxis+
–
Thrombosis Threshold
• Anticoagulant deficiencies• Factor V Leiden• Prothrombin 20210A
• Age• Previous VTE• Cancer• Obesity
• Estrogens• Pregnancy• Surgery• Immobilization
from Folsom A

CASCADEThe Protein C Pathway
From Esmon CT

Prothrombin Gene MutationG A Mutation at Position 20210 in 3´- UT Region
GENOTYPE PROTHROMBINRANGE
20210 AG 132% 95-178
20210 GG 105% 55-156
From Poort et al, Blood 1996
Mutation leads to increased efficiency of prothrombin mRNA 3’-end formation and increased prothrombin biosynthesis without
affecting the rate of transcription.


Prevalence of Defects in Patients with Venous Thrombosis
APC Resistance (Factor V Leiden) 12-40%
Hyperhomocysteinemia 10%
Prothrombin Gene Mutation 6-18%
Deficiencies of AT, Protein C, Protein S 5-15%
Antiphospholipid Antibody Syndrome 5-10%
Unknown 15-70%

The “Hypercoagulable Workup”
• Genetic test for Factor V Leiden mutation or coagulation assay for Activated Protein C Resistance (if abnormal, confirm genetically)
• Genetic test for Prothrombin G20210A mutation• Functional assay of Antithrombin*• Functional assay of Protein C*• Protein S assays*
• Functional assay• Measurements of total and free Protein S
• Tests for Antiphospholipid Antibody Syndrome
• ± Measurement of fasting plasma homocysteine (hcy) level• ± Factor VIII Coagulant Activity Level
*Can omit in patients with a first VTE at age > 50 and a negative family history

Hcy lowering by B-vitamin supplements does not lower risk of recurrent thrombosis
• Arterial Thrombosis• NORVIT Trial (N Eng J Med 2006)
• 3,479 patients with acute MI• Trend toward increased risk with combined B vitamin treatment
• HOPE 2 Investigators (N Eng J Med 2006)• 5,522 patients > age 55 with vascular disease or diabetes
• Venous Thrombosis• VITRO Study (Bos GMJ, et al. ASH Abstract 2004)
• Patients ages 20-80 with unprovoked proximal DVT or PE• Recurrences: 43/348 vitamins, 50/353 placebo

Antiphospholipid Antibody Syndrome (APLS)
• A clinical diagnosis characterized by a thrombotic event (venous or arterial thrombosis, recurrent fetal loss) in association with a persistent LA in specialized clotting assays or persistently elevated titers of cardiolipin (IgG or IgM) or 2-glycoprotein I antibodies
• Clinical manifestations include thrombocytopenia, and livedo reticularis.
• Associated with SLE, cancer, infections, drugs, idiopathic

Antiphospholipid Antibody Syndrome (APLS)
• LA result from the presence of immunoglobulins which bind to phospholipids and plasma proteins (2-glycoprotein 1, prothrombin) in vitro and prolong clotting times (critically dependent on the amount of phospholipid in assay). LA do not cause bleeding, but confer an increased risk for recurrent thrombosis.
• Retrospective studies indicated that patients with APLS require a target INR range of >3 to obtain adequate antithrombotic protection. Two randomized trials have shown that an INR of 2-3 is adequate in patients with venous thrombosis.

Venous Thromboembolism in Cancer
• Common (~20% of all patients with VTE)• Increased risk of recurrent VTE
• Can occur with an adequate INR (“warfarin resistance”)
• Increased risk of bleeding during anticoagulant therapy
• Rx: Consider chronic low molecular weight heparin

• multicenter, randomized, open-label study
Initial Rx 6 months
RCancer patients with proximal DVT, PE or both
dalteparin
dalteparin
OAC
dalteparin
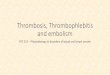
CLOT in Cancer Trial
Lee A. New Eng J Med 2003

Recurrent VTE
0
5
10
15
20
25
Days Post Randomization
0 30 60 90 120 150 180 210
Pro
bab
ility
of R
ecu
rre
nt V
TE
, %risk reduction = 52%
p-value = 0.0017
dalteparin
OAC

0
10
20
30
40
50
60
70
80
90
100
Days Post Randomization
0 30 60 90 120 180 240 300 360
dalteparin
OAC
Pro
bab
ility
of
Su
rviv
al, %
12-month MortalityAll patients
HR 0.94 (0.77 – 1.1)
P-value = 0.40

0
10
20
30
40
50
60
70
80
90
100
0 30 60 90 120 180 240 300 360
OAC
dalteparin
12-month MortalityPatients without metastases
Pro
bab
ility
of
Su
rviv
al, %
Days Post Randomization
HR 0.5 (0.27 – 0.95)
P-value = 0.03

Prandoni1992
0.012
0.043
0.04
<0.001
40
30
20
10
0
Idiopathic
SecondaryCancer
incidence %
Monreal1991
Monreal 1993
Bastounis1996
Detection of malignancy in the patient presenting with thrombosis

Evaluation for malignancy in the patient presenting with thrombosis
Available data do not support an extensive search for occult malignancy; it is however important to pursue symptoms or signs which suggest an underlying malignancy and to ensure that age-appropriate screening tests have been performed.

Sites of Thrombosis
ABNORMALITY ARTERIAL VENOUS
Factor V Leiden - +
Prothrombin 20210A - +
AT Deficiency - +
Protein C Deficiency - +
Protein S Deficiency - +
Hyperhomocysteinemia + +
Lupus Anticoagulant + +

Acquired Deficiencies in Antithrombin,Protein C, or Protein S
ANTITHROMBIN PROTEIN C PROTEIN SPregnancy PregnancyLiver Disease Liver Disease Liver DiseaseDIC DIC DICNephrotic syndromeMajor surgery InflammationAcute thrombosis Acute thrombosis Acute thrombosis
TREATMENT WITH:Heparin Warfarin WarfarinEstrogens Estrogens

Protein S Deficiency
PROTEIN S ANTIGEN PS
TYPE TOTAL FREE ACT
I Low Low Low
II Normal Normal Low
III Normal Low Low

Prevalence of the Factor V Leiden (FVL) and Prothrombin G20210A Mutations
POPULATION FVL (%) G20210A (%)
European
Northern 5-10 1.7
Southern 2-3 3
African
EXTREMELY RARE
Asian

Leiden Thrombophilia Study: A Population Based Study Koster T et al, Lancet 1993
• Patients: Inclusion Criteria• Consecutive outpatients < age 70 referred for
warfarin treatment to thrombosis centers with a first DVT
• Laboratory evaluation > 3 months after discontinuation of oral anticoagulants
• Patients: Exclusion Criteria• Malignancy
• Controls: Healthy matched unrelated subjects

First Episode of Deep Venous Thrombosis(Leiden Thrombophilia Study)
RISKNormal 1Prothrombin 20210A 2.8
heterozygotesOral contraceptives 4x Factor V Leiden 7x
heterozygotesOral contraceptives 35x
+ Factor V LeidenFactor V Leiden 80x
Homozygotes

First Episode of Deep Venous Thrombosis(Leiden Thrombophilia Study)
INCIDENCE/YEAR (%)Normal 0.008Oral contraceptives 0.03Factor V Leiden 0.06
heterozygotesOral contraceptives 0.3
+ Factor V LeidenFactor V Leiden 0.5 - 1
Homozygotes

Should we screen women for factor V Leiden prior to starting OCPs?
If all women with factor V Leiden did not take OCPs, their risk of VTE would decrease from 30 to 6 VTE events per 10,000 women/year.
prevent 1 event per 417 women
To find 417 women with factor V Leiden, you would have to screen 6,770 women given a prevalence of 6%.
Costs of screening exceed benefits.

Hereditary Thrombophilia andObstetric Complications
• Significantly increased risk for second and third trimester fetal loss (~3-fold )
• Conflicting data regarding association with other obstetric complications
• Few randomized trials of anticoagulant therapy

Treatment of DVT/PE
• Heparin• Unfractionated or Low Molecular Weight
Heparin for at least 5 days
• Warfarin• Start on day 1 to achieve INR of 2-3, treat for
3-6 months

Recurrent Venous Thrombosis is Common Following a First Episode of Symptomatic DVT
CumulativeIncidence (%)
Years
Prandoni et al, Ann Intern Med 1996;125:1-7
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8

Risk of Recurrent Venous Thrombosis in Patients with Hereditary Thrombophilia
• Heterozygosity for Factor V Leiden (FVL) or Prothrombin (PT) G20210A do not increase risk.
• Higher in heterozygotes with both FVL and PT G20210A (retrospective studies); probably higher in homozygotes with FVL
• Antithrombin, Protein C, Protein S Deficiency• High in selected kindreds with strong clinical
penetrance (retrospective studies)• Little data in unselected patients

Factors Influencing Duration of Anticoagulation
• Recurrent VTE• Risk ( % / year) ~10%• Consequences (case fatality) 0.5%
• Bleeding• Risk ( % / year) ~2%• Consequences (case fatality) 0.4%

Guidelines on Duration of Anticoagulant Therapy
• First event with reversible or time limited risk factor• 3-6 months at INR 2-3
• Unprovoked VTE, first or second event• 6 months at INR 2-3, then consider
indefinite anticoagulation at INR 2-3 weighing recurrence versus bleeding risk
• Special Situations - indefinite anticoagulation • First event with
• Cancer until resolved (consider chronic LMWH)• Antiphospholipid antibody syndrome• Antithrombin deficiency or multiple genetic defects, ?
deficiencies of protein C or protein S

Guidelines on Anticoagulant Therapy
RISK CLASSIFICATION MANAGEMENT
• Moderate-risk• 1 event with a stimulus Vigorous prophylaxis• Asymptomatic in high-risk settings

Criteria for Long-Term Oral Anticoagulation in Patients with
Venous Thrombosis
• Resolution of triggering risk factor• Sites and severity of thrombosis• Bleeding risk• Identification of a prothrombotic defect
coupled with family’s thrombotic history • PATIENT PREFERENCE (role of lifestyle
and occupation)

6 months6 months
After Initial AnticoagulationAfter Initial Anticoagulation
Accept the riskAccept the riskof recurrenceof recurrence
Extend inExtend inall patientsall patients
ExtendExtendwith newwith newstrategiesstrategies
Extend inExtend inhigh-risk high-risk patientspatients

D-dimer and Recurrent VTE (PREVENT)
0
2
4
6
8
10
12
14
Ddimer < 500 D-dimer > 500 D-dimer < 500 D-dimer > 500
Inci
den
ce (
% /
Yea
r)
Warfarin, INR 1.5-2 Placebo

Testing for Hereditary Defects in Patients with Thrombosis and No Family History
PROImprove understanding of pathogenesis of VTEIdentify and counsel affected family members
CONInfrequently Identify patients with defects carrying specific
management implications (multiple defects are uncommon)Potential for overaggressive management of propositus and
asymptomatic affected relativesNegative insurance implicationsCost of testing/consultations

Thrombophilia and Recurrent VTELeiden Thrombophilia Study (JAMA 2005)
Conclusions
“Prothrombotic abnormalities do not appear to play an important role in the risk of a recurrent thrombotic event. Testing for prothrombotic defects has little consequence with respect to prophylactic strategies. Clinical factors are probably more important than laboratory abnormalities in determining the duration of anticoagulation therapy.”














![Homocysteine-lowering interventions for preventing … · 2018. 12. 15. · [Intervention Review] Homocysteine-lowering interventions for preventing cardiovascular events Arturo J](https://img.pdfslide.net/doc/110x75/5ff89452656730039f05d58a/homocysteine-lowering-interventions-for-preventing-2018-12-15-intervention.jpg)












