Embed Size (px)
Citation preview

hyperglycemic hyperglycemic control in the control in the
emergency roomemergency room
Myrna Buenaluz- SeduranteUniversity of the Philippines
Dept of MedicineSection of Endocrinology

TopicsTopics
Diabetic Ketoacidosis Epidemiology Pathophysiology Diagnosis Treatment
Hyperosmolar Hyperglycemic State AKA Nonketotic Hyperglycemia, Hyperosmolar Nonketotic Coma

DKA StatisticsDKA Statistics
Type 1 Diabetes Type 1b Ketosis prone Diabetics Occasionally in Type 2
Infection, Trauma, Cardiac Newly diagnosed Type 2 DM
Cost Annual hospital cost $1 billion ¼ of health care dollars spent on Type 1 diabetics

DKA MortalityDKA Mortality
Mortality primarily due to precipitating illness
Prognosis worse with old age, coma and hypotension

HHS StatisticsHHS Statistics
<1% of all diabetes-related admissions More common in elderly diabetics
frail poor access to water Decreased GFR
Mortality Variable 10-50% Most often due to the precipitating illness

Role of InsulinRole of Insulin


KetoacidosisKetoacidosis
Lipolysis→Increased FFA→Converted to Ketones in Liver
Three ketones Acetoacetic Acid; Beta-Hydroxybutyric Acid; Acetone
Accumulation leads to acidosis (↓pH) & formation of anion gap
Differential Diagnosis Alcoholic Ketoacidosis Starvation Ketosis

Diagnostic criteriaDiagnostic criteriaDKA HHS
• blood glucose >250 mg/dl,
• arterial pH <7.3,
• bicarbonate <15 mEq/l, and
• moderate ketonuria or ketonemia
• blood glucose >600 mg/dl •
• arterial pH >7.3, •
• bicarbonate >15 mEq/l, •
• mild ketonuria or ketonemia, and •
• effective serum osmolality >320 mOsm/kg H2O.• longer time for development of the disease

cytokines, markers of oxidative stress, cytokines, markers of oxidative stress,
lipid peroxidation and cardiovascular lipid peroxidation and cardiovascular
riskrisk
• All increased even in the absence of infection• CRP and homocysteine do not go back to normal
levels with resolution of DKA/HHS

Causes of DKA/HHSCauses of DKA/HHS New diagnosis of Diabetes Infection: Pneumonia, Gastroenteritis, UTI Pancreatitis Acute MI/ACS Stroke Trauma Alcohol/Drugs/Medications Missed Insulin/Compliance

In between type 1 In between type 1 and type 2 and type 2
•Unprovoked ketosis
•Absent islet cell antibodies
•Frequent evolution to Insulin independence over time

Flatbush or ketosis Flatbush or ketosis prone diabetesprone diabetes
• ADA classification: type 1a (Ab+) and type 1b (Ab-)
• AβClassification based on presence of antibodies (GAD65 autoantibody) and cell reserve (C peptide levels)

Symptoms of DKASymptoms of DKA
Develops rapidly Earliest symptoms are due hyperglycemia
Polyuria, Polydipsia, Weight loss
Neurologic symptoms Abdominal pain, nausea, vomiting
Up to 50% of DKA Associated with degree of acidosis ?Delayed gastric emptying/ileus

Physical Exam in DKAPhysical Exam in DKA
Signs of dehydration Tachycardia, hypotension
Neurologic exam “Acetone breath” Kussmaul Respirations Fever is rare, even with infection

Evaluation Evaluation
Laboratory Glucose Electrolytes CBC Serum Ketones Plasma Osmolality ABG (venous pH 0.03
lower) Urinalysis ?Amylase/Lipase
• Othero Electrocardiogramo Chest X-Rayo Blood Cultureo Urine Cultureo Sputum Culture

Labs in DKA: ABG and Labs in DKA: ABG and ketonesketones

Labs in DKA: GlucoseLabs in DKA: Glucose
Usually between 300-500 mg/dl “Euglycemic DKA”
Nutritional deficiency Pregnancy Prior use of insulin en route to the E.R.

Labs in DKA: SodiumLabs in DKA: Sodium Variable sodium levels Direct effect of hyperglycemia leads to
hyponatremia (↓1meq/L for every 62 mg/dl rise in BS) due to fluid shift from intracellular to extracellular space
Need to compute for corrected sodium Corrected Na = serum sodium +1.6 for ever 100 mg/dl above 100
Secondary effect of osmotic diuresis which causes loss of free water→hypernatremia
Most are mildly hyponatremic

Labs in DKA: Labs in DKA: PotassiumPotassium
Overall potassium deficit Renal loss with osmotic diuresis & ketone excretion GI loss
However, on initial evaluation, K level is usually normal or elevated Hyperosmolarity Insulin deficiency ?Acidemia
Take great care in monitoring/repleting K for fear of arrythmias

Labs in DKA: OtherLabs in DKA: Other Phosphate
Usually body depleted, but initial levels may be normal or high
Amylase/Lipase May be elevated, even without pancreatitis
Elevated WBC Hyperlipidemia
Elevated TC & Trigs

FormulasFormulas
•Corrected Na = serum sodium +1.6 for ever 100 mg/dl above 100
•Fluid deficit = (Corrected Na- Goal of 140/ 140) x 0.6 x kg BW
•Anion Gap = Na – (Cl+HC03)
•Osmolarity = 2Na +glucose in mg/dl/18

Anion GapAnion Gap
AG= Na – (Cl + HCO3) Normal <12; DKA >20 Accumulation of BHB & AA Test in serum & urine Nitroprusside reaction converts AA to acetone
and (does not detect BHB) Test may be negative test if most of the anions are BHB Adding Hydrogen Peroxide to urine the urine converts BHB to AA &
allows NP reaction

Anion GapAnion GapHigh Anion Gap Normal Anion Gap
•Methanol•Uremia and RF•Diabetes and other ketotic states •Paraldehyde•INH•Ethylene glycol•Salicylate
add lactic acidosis
•ureteroenterostomies•Sulfamylon•Enteric fistulas•Diarrhea•Cholestyramine•Aldactone, acidifying agents,actazolamide•RTA
add HAL

Treatment of DKATreatment of DKA
Initial Evaluation: ABCs; Exam; Labs; Causes Close Monitoring Fluid Replacement Insulin Therapy Electrolyte Replacement Resolution & Conversion to home therapies


MonitoringMonitoring
ICU StatusBlood sugar monitoring q1 hrElectrolytes ,venous pH q2-4 hrsKetones q 6HClose evaluation of vitals & neuro statusConsider use of flowsheet

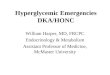
DKA/HHS flowsheet for the documentation of clinical parameters, fluid and electrolytes, laboratory values, insulin therapy, and urinary output.
et al. Dia Care 2003;26:s109-s117
Copyright © 2011 American Diabetes Association, Inc.

Fluid ReplacementFluid Replacement Mainstay of initial therapy Expand the intravascular volume & improve renal
blood flow Ave fluid loss for DKA: 3-6 Liters (8-10 in HHS) Isotonic saline
Rapidly infuse volume without acute lowering of plasma osmolarity
Switch to ½ NS in subacute phase if Na normal or high 15-20 ml/kg initially then decrease to
5-10ml/kg/hr Fluids alone my initially decrease BG by 35-70

ER doc’s recommendation: Hardern and ER doc’s recommendation: Hardern and
Quinn Emerg Med J 2003; 20:210-13Quinn Emerg Med J 2003; 20:210-13
• 500 ml x 4 hours then 250 x 4 hours
• Make sure lines are in
• Insert NGT and Urine catheter

Insulin TherapyInsulin Therapy Role of Insulin
Lower serum glucose (mainly by decreasing liver production)
Reduce ketogenesis in liver by reducing lipolysis and glucagon secretion
Increase ketone utilization Insulin IV bolus and continuous drip is standard of
care Some studies have looked at frequent, rapid-acting
insulin, but not enough data to support use except in mild DKA cases

Insulin TherapyInsulin Therapy
Check Potassium first! If K <3.3, delay insulin until begin K repletion May drive insulin into the cells and lead to life-threatening hypokalemia
IV bolus of regular insulin: 0.1 U/Kg Continuous infusion, start at 0.1 U/Kg/hr Goal is to decrease glucose by 50-70 mg/dl per
hour; will require further titration of drip Higher rates in the young compared to the old Higher rates in those with Type 2 diabetes

Insulin TherapyInsulin Therapy
Once BS < 200 (<300 in HHS) start dextrose (usually D5 ½ NS) and decrease insulin drip rate to 1/5 of previous
Addition of dextrose to IVF Avoid hypoglycemia Continue insulin drip while awaiting resolution of ketoacidosis Continue nutrition while patient NPO
Need to overlap IV drip with SQ insulin to avoid going back into ketosis

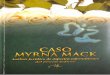
Comparison of the effects of iv, sc, and im low-dose insulin regimens on changes of plasma glucose and total ketone bodies in patients with DKA. Reprinted from Fisher et al.
Kitabchi A E et al. JCEM 2008;93:1541-1552
©2008 by Endocrine Society

SQ Aspart vs. I.V.Regular SQ Aspart vs. I.V.Regular insulininsulin
• BOLUS 0.3 u/kg/hour then
• Aspart SQ 0.1 u/hr until glucose is less than 250 mg/dl then decrease dose to 0.05 u/hr till DKA resolves
OR Aspart SQ 0.2 u/2hr until glucose is less than 250 mg/dl then decrease dose to 0.05 u/hr till DKA resolves

Aspart vs. Regular Aspart vs. Regular insulininsulin

Bicarbonate and pHBicarbonate and pH

A: Serum insulin levels before and after subcutaneous injection (at 0 min) of insulin aspart (•) or insulin lispro (○) in seven patients with type 1 diabetes.
Homko C et al. Dia Care 2003;26:2027-2031
Copyright © 2011 American Diabetes Association, Inc.

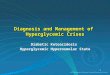
Plasma levels of FFA (A) and total ketone bodies (β-hydroxybutyrate plus aceto-acetate, B) before and after subcutaneous injection (at 0 min) of either insulin aspart (•) or insulin lispro
(○) in seven patients with type 1 diabetes.
Homko C et al. Dia Care 2003;26:2027-2031
Copyright © 2011 American Diabetes Association, Inc.

Changes in metabolic profile in patients with DKA treated with intravenous glulisine (○) and regular insulin (●).
Umpierrez G E et al. Dia Care 2009;32:1164-1169
Copyright © 2011 American Diabetes Association, Inc.

IV Glilusine vs. IV IV Glilusine vs. IV Regular insulinRegular insulin

Potassium Potassium ReplacementReplacement
If initial K high, should not need more therapy than insulin, which will drive K into the cells
To prevent hypokalemia, add KCl to IVF if K<5.3 If K normal, 20-30 meq/liter of IVF is adequate If K low, may need more aggressive rx If using 40 meq KCl in saline, may use ½ NS as this will create isotonic
solution NS = 154 cation equiv ½ NS = 77; ½ NS + 40 meq KCl = 117 (~3/4 NS)

Effects of acidosis in Effects of acidosis in experimental studiesexperimental studies
• Initially acidosis from ketones, lactic acidosis and renal dysfunction
• Subsequently, Hyperchloremic acidosis due to preferential excretion of ketones over chloride and from saline administration
• Impairs myocardial contractility• Reduces cardiac output• Affect oxyhemoglobin dissociation and tissue
oxygen delivery• Inhibit intracellular enzymes• Alter cellular metabolism


Marked heterogeneity and Marked heterogeneity and NO clear evidenceNO clear evidence
Parameter Benefit No difference
Harm
Hospitalization 2 1
Mortality
Resolution of Acidosis/ketosis 8 7
Insulin sensitivity/ glucose 11
Potassium balance 3 5
Tissue oxygenation 1 1
CSF acidosis 2
Cerebral edema 1 2
Neurological outcomes 3
Hemodynamic outcomes 1

Bicarbonate TherapyBicarbonate TherapyConcerns with use:
Rapid rise in pH will shift the O2 dissociaiton curve to the left. This results in decrease tissue oxygenation. The rise in pCO2 results in an increase in lactate and acidosis
The rise in lactate may lead to fall in cerebral pH contributing to edema
Consider use with: pH <7.0, especially if decreased cardiac function Life-threatening hyperkalemia
Dose: 50-100 meq NaHCO3 (1-2 amps) over 2 hoursDoes not apply to HHS

Phosphate TherapyPhosphate Therapy Most patients phosphate depleted Usually level will fall with initial therapy
Driven into the cells with resolving acidosis Improved renal perfusion→excretion
Most patients do not have symptoms related to hypophosphatemia
Routine use not necessary If evidence of cardiac dysfunction, hemolytic
anemia, or respiratory depression in pts with phos <1.0 mg/dl 20-30 meq/L of Potassium Phosphate, added to IVF

ResolutionResolutionDKA•Blood glucose <200 mg/dl•PLUS 2 0f the following:
o Bicarbonate ≥15 mEq/mlo Venous ph 7.3o Anion gap ≤12 mEq/l
HHS•Normal osmolality•Normal mental status

ComplicationsComplications
Related to underlying illness
Cerebral edema Decreased arousal, Lethargy after initial improvement, headache,
vomiting, relative bradycardia and hypertension, seizures, incontinence,pupillary changes 4-12 hrs after tx
0.5-1% of cases, mostly in children, case rate constant across 6 decades
Mortality 20-25%

Cerebral edemaCerebral edema Theories:
Hypoxia induced damage to blood brain barrier
Saline bolus increases capillary hydrostatic pressure resulting in interstitial edema
Fluid shift along the osmolar gradient secondary to overzealous hydration/insulin use
Activation of the Na-H exchanger by insulin

Cerebral edemaCerebral edema
Reduce risk bySlow rehydration in 48 hours, gradual replacement of Na & H2O deficits in hyperosmolar patients & adding dextrose
to IV solution once appropriate,supplemental oxygen

Cerebral edemaCerebral edema
Treatment3% Nacl 5-10 ml/kg or
mannitol 0.25-1 g/kg over 20 mins
I case report:octreotide at 3.5 ug/kg/hr (suppresses IGF 1 and GH levels leading to lower glucose values)

PreventionPrevention
Improved access to medical care
Education When to contact doctor if illness occurs Increased use of short-acting insulin during illness Continued use of insulin & BS monitoring when illness prevents eating Continued nutrition during times of illness