Embed Size (px)
DESCRIPTION
Hyperhomocyst(e)inemia and Thrombophilia. A major point of consensus was that no causal role of hyperhomocyst( e)inemia in venous or arterial thrombosis is not yet established. H omocysteine is a non–protein-forming sulfhydryl amino acid - PowerPoint PPT Presentation
Citation preview

Hyperhomocyst(e)inemia and Thrombophilia

• A major point of consensus was that no causal role of hyperhomocyst(
• e)inemia in venous or arterial thrombosis is not yet established

• Homocysteine is a non–protein-forming sulfhydryl amino acid
• Dietary methionine Homocysteine (Intracellular demethylation)
• Homocysteine methionine (remethylation)
• is derived from the reduction of• 5,10-methylene-tetrahydrofolate
Methyltetrahydrofolate (MTHFR). • Methionine excess homocysteine may
enter the transsulfuration pathway.


• Hyperhomocystinemia :marked increase in atherothrombotic CVD and VTE.
• 25% : vascular occlusive event by age 16 year & 50% by age 29 years.
• Of these events, 32% are CVA, 4% are MI , 11% are peripheral arterial
• occlusions, and 51% are VTEs.• The event rate is reduced by vitamin
therapy in B6-responsive individuals.

• The gene for MTHFR is located on chromosomal region 1p36.
• Thermolabile mutant. • 12% of the population in the United
States is homozygous• Estrogen-containing medications
result in lower plasma homocysteine levels

New Concepts inCongenital Thrombophilia
Galila Zaher(November 1999)

Congenital thrombophilia
Inherited thrombophilia can be defined as a
genetically determined tendency to venous
thromboembolism.
Genetic risk factors are now identified in 30-
50% of affected individuals.

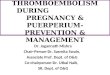
Table 1. Risk factors for inherited thrombophilia: prevalence and relative risk for venous theombosis
Risk factorYear describe
d
Prevalence in the general population
)%(
Relative risk
for VTE*
Antithrombin deficiencyProtein C deficiency
Protein S delivery (free PS)APC resistance
HyperhomocysteinaemiaFactor VIII levels > 150 IU/dlProthrombin gene G20210A
variant
1965
1981
1984
1993
1994
1995
1996
0.181
0.24
1.35
<156***
53
113
2.33
5.03**
6.53
2.45
6.63
2.53
4.83
2.83

Hyperhomocystinaemia
Homocysteine is a sulphur containing A A.
It is derived from methionine EAA.
Homocysteine metabolism:
Re methylation pathwayMTHFRTrans sulphuration pathwayC sTrans methylation pathway

Hyperhomocystinaemia
Interest in homocysteine as a risk factor for
vascular disease came from the earlyobservations that such diseases are
commonin cases of classical homocystinuria.

Hyperhomocystinaemia
Neural tube defects (NTPs)
Arterial vascular disease
Venous thromboembolism

HyperhomocystinaemiaNTDs.
Neuronal tube defects occur in 1/1000 birth in USA.
It has a complex trait interacting with environmental factors.
Homozygousity for TL-MTHFR has been clearly
shown to be a risk factor for spina bifida in 12% of the cases.
Pre conceptional supplementation of folic acid could preventup to 70% of NDTs.
Folic acid 4 mg reduces the recurrence of NTDs(MRC vit study research gp)
(Czei Zel, N Eng] Med 1992)

HyperhomocystinaemiaArterial vascular disease
Potential mechanismsOxidative damage to endothelial cells.
Enhanced plt adhesion to endothelial cellsEnhanced plt aggregation
Plt accumulation and the formation of plt rich thrombous
Inhibition of TM expressionIncreased procoagulant activity and reduced natural
Anticoagulant(Wetch. N. Eng] Med 1998)

HyperhomocystinaemiaArterial vascular disease
Metanalysis of published studies revealed that
elevation in total plasma homocysteine were
found to be an independent risk factor for all
forms of arterial vascular disease.
(Perry Advances in Haem. 1999)

HyperhomocystenaemiaArterial vascular disease
*15-40% of patients with conorary, cerebral of peripheral arterial disease have high
plasma level of homocysteine > 20 moL/L.
*The odd ratio for IHD is 1.4 for every 5 moL/L more than homocysteine median
fasting adult males.
*C677T mutation is a major cause of mild hyperhomocystinenia, but the mutation per
se does not increase cvs disease risk

Hyperhomocystinaemiavenouss thromboembolism
There is accumulating data to suggest that hyperhomocystinemia is a risk factor for VTE
that is independent of coexisting abnormalities of the naturally occurring
Anticoagulant.Homozygosity TL-MTHFR together
with low folate level confers moderate risk factor.Hyperhomocystinaemia defined as plasma level
>95% of control (18 M mol IL) was found in 16% ofcases.

HyperhomcystinaemiaLaboratory evaluation
Intra individual variability
Inter Laboratory variabilityELISAHPLCEIA

HyperhomocystinaemiaLaboratory evaluation
There is an urgent need to improve analytical
impression and decrease the difference amongmethods.
An ideal homocysteine reference range based
on targeting subject with highest serumFolate level is preferable to the population base
range.

HyperhomocystinaemiaLaboratory evaluation
Fasting total plasma homocysteine level
Methionin loading dose.
Serum Folate and B12 PevelPCRC677T

HyperhomocystinaemiaLowering vit dose
Plasma ThCY response to folic acid and Pyridoxin hydrochlorid
The optimal homocysteine lowering vitamin dose
and target ThCY are currently unknown.
Proposed does.Folic acid 500-650 gPyridoxin 100 mg
B 120.4 mg.

Issues to be addressed
What is the minimum dose of folic acid to prevent
NTDs?
Would grain fortification adapted in USA reduce
NTDs, protects against arterial vascular disease?
What is (are) the best test (s) to evalaute hyper homocystinemia?

Concluding Remarks
.1Folate supplementation reduces the occurance and recurrence of NTDs.
.2Elevated fasting plasma homocysteine is an independent risk factor for all forms of
arterial vascular disease.

Concluding Remarks(Continue)
.3Homozygonosity for TL-MTHFR is not a significant risk factor for VTE per se
.4There is currently no strong argument to include MTHFR C677T genotyping during routine thrombophilia screen.
.5Combination of hypercystinaemia and FvL abnormality significantly increase
the risk for VTE.

Thanks