Embed Size (px)
Citation preview

L I N N E A C O O P E R
Hypertension
Patient Information
Joseph Hill, 53 y/o black male
Recent BP readings of 210/122, 180/110, 192/108, 200/114, 182/106.
PMH
Excellent health, no physical exam since age 30 where he had elevated BP.
No meds/allergies
Family hx: unknown
Social: gardener, smokes 1-2 cigars/day, little ETOH, married with 3 grown children.
Review of Systems
General: considers himself “healthy”. From the South and primarily eats fried foods.
HEENT: Occasional occipital HA late in day , worse in evening. No visual disturbance, tinnitus, or vertigo.
Heart: no CP or tightness
Lungs: no dyspnea or cough

Physical Exam
General: moderately obese
VS: HR 72, RR 16, Temp 98.4, wt 224#, 6’0”, BP 204/116 RA, 204/144 LA lying
200/116 sitting, 194/118 standing.
HEENT: fundi have arteriole narrowing and AV nicking, hemorrhage and exudates.
Heart: no murmurs or rubs, S1 and S2 normal and S4 heard at the apex and L lateral position.
Neck: no JVD or bruits
Additional history
Question about stresses in life, weight control, physical activities, and dietary intake of sodium, caffeine, and cholesterol.
BMI? 30.4 Secondary causes of HTN
ETOH, psychogenic, arteriosclerosis, adrenal disorder, thyroid disorders, amphetamines/street drugs, NSAID long-term use, renal disease, acute stress,
EKG
Chest xray
Complete neuro exam
Pathogenesis
Force against the walls of the BV.
Systolic is pressure in arteries as heart contracts
Diastolic is pressure when heart relaxes (Breen, 2008).
Variable involving the volume of blood and degree of dilation or constriction
Regulation of body fluid volume, salt intake
R-A-A system
Vascular autoregulation, SNS
Obesity, genetics
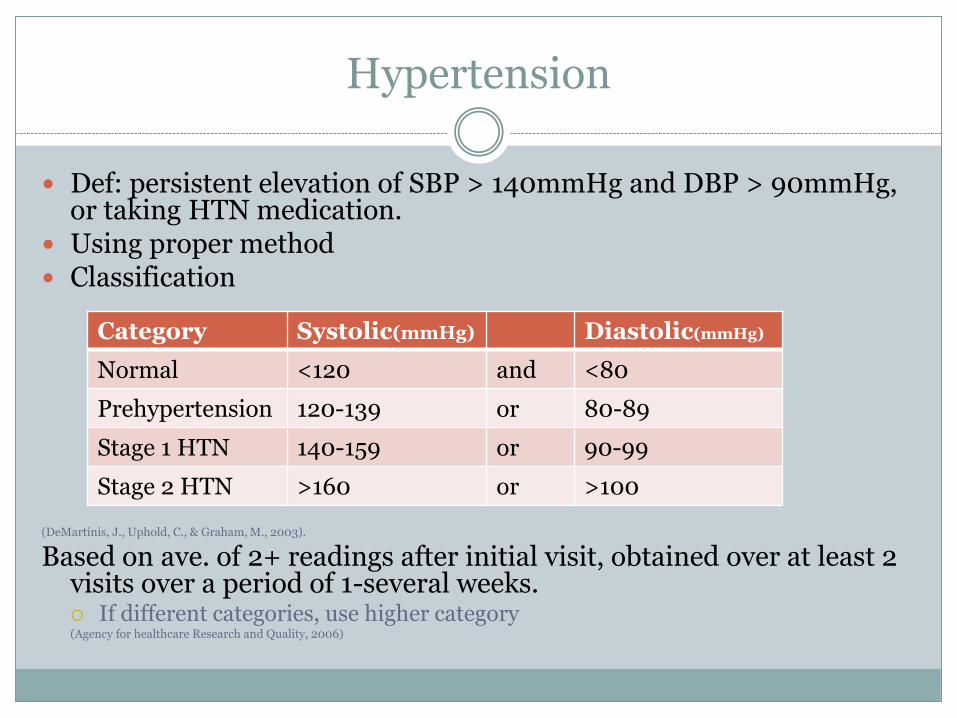
Hypertension
Def: persistent elevation of SBP > 140mmHg and DBP > 90mmHg, or taking HTN medication.
Using proper method Classification
(DeMartinis, J., Uphold, C., & Graham, M., 2003).
Based on ave. of 2+ readings after initial visit, obtained over at least 2 visits over a period of 1-several weeks. If different categories, use higher category (Agency for healthcare Research and Quality, 2006)
Category Systolic(mmHg) Diastolic(mmHg)
Normal <120 and <80
Prehypertension 120-139 or 80-89
Stage 1 HTN 140-159 or 90-99
Stage 2 HTN >160 or >100
Types of hypertension
Essential HTN (90-95%), no identifiable cause
Secondary HTN: identifiable cause.
Pheochromocytoma, renal artery stenosis, Cushings (DeMartinis,
J., Uphold, C., & Graham, M., 2003).
Factors that can increase BP:
Obesity, psychogenic stress, high fat and sodium intake, oral contraceptives, ETOH, insulin resistance, low birth weight, neurovascular abnormalities, “white coat” (Breen, 2008).
Differential diagnosis
Real HTN vs those who appear to be hypertensive due to incorrect measures.
Clinical manifestations
Central obesity, hirsutism, purple striae, ecchymosis
Widening pulse pressure, acute anterior chest and back pain, feeling of doom
Wt loss, nervousness, exophthalmia, tremors
Paroxysmal c/o headache, perspiration, palpitations, dizziness
ETOH, psychogenic, arteriosclerosis, adrenal disorder, thyroid disorders, amphetamines/street drugs, NSAID long-term use, renal disease, oral contraceptives (DeMartinis, J., Uphold, C., & Graham, M., 2003).

Diagnostic testing
Before beginning therapy
UA, CBC, fasting dexi, CMP, Creatinine, fasting lipid panel, EKG, Hct
Plus whatever you are ruling out
TSH, urine VMA, triglycerides/cholesterol, BUN/Cr, drug screen

Target Organ Disease
Precipitates many diseases
CHD, Left ventricular hypertrophy, HF, TIA, stroke, dementia, PVD, retinopathy (Breen, 2008).
May not appear until 10-20 years after disease
Plan/Management
Maintain arterial pressure <140 SBP and <90 DBP
DASH diet
Lifestyle modification Maintain normal body weight (BMI 18.5-24.9)
Reduce dietary sodium
Limit ETOH one drink/day, smoking cessation
Regular aerobic physical exercise most days of the week for 30 min, weight reduction.
Adequate intake of K+ (>3500mg)
Diet rich in fruits and vegies, low-fat dairy, and decreased fat (DeMartinis, J., Uphold, C., & Graham, M., 2003).
(Agency for Healthcare Research and Quality, 2006; US Department of Health and Human Services, National Institute of Health, 2003).

Screening
Family history of CHD
Smoking status, diet, ETOH, physical activity
Blood pressure, BMI, waist circumference, pulse (afib).
Fasting lipoprotein profile
Fasting glucose
Update regularly
At each routine visit
At each routine visit, at least every two years
At least every 5 years
If risk factor for hyperlipidemia or diabetes, every two years (Bickley, 2009)
Risk Factor Frequency
Screen every 2 years for <130/80, more frequent for higher
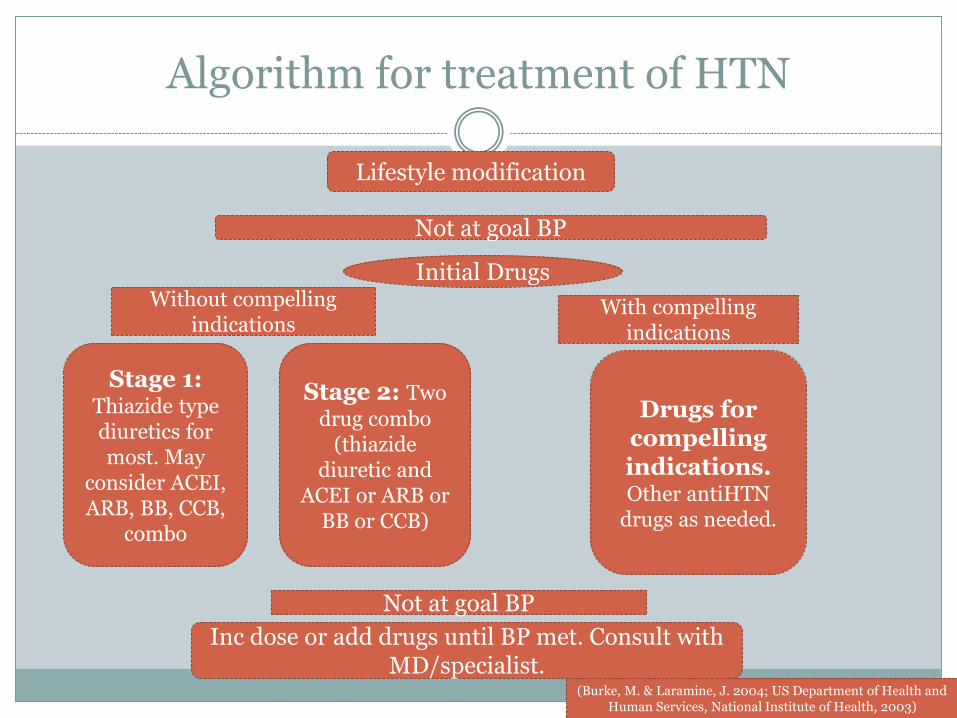
Algorithm for treatment of HTN
Lifestyle modification
Not at goal BP
Initial DrugsWithout compelling
indicationsWith compelling
indications
Stage 1:Thiazide type diuretics for most. May
consider ACEI, ARB, BB, CCB,
combo
Stage 2: Two
drug combo (thiazide
diuretic and ACEI or ARB or
BB or CCB)
Drugs for compelling indications.Other antiHTN
drugs as needed.
Not at goal BP
Inc dose or add drugs until BP met. Consult with MD/specialist.
(Burke, M. & Laramine, J. 2004; US Department of Health and Human Services, National Institute of Health, 2003)

Compelling indications
DM
Heart Failure
Heart failure with symptomatic vent dysfunction
CKD
Post-MI
Stable angina
ACS
Recurrent stroke prevention
African Americans
Elderly
Thiazide diuretic, ACE I, ARD, B-blocker, CCB
ACE I, B-blocker ACE I, B-blocker, ARB,
aldosterone blocker along with diuretic
ACE I or ARB ACE I, B-blocker, aldosterone
blocker B-blocker B-blocker, ACE I
ACE I and thiazide diuretic Diuretics and CCB have best
effect Thiazides or b-blocker + thiazide
(DeMartinis, J., Uphold, C., & Graham, M., 2003).

Controlling BP
If still uncontrolled after 2 weeks-2 months
Increase dose of initial drug
Switch drugs if no response/SE
If not taking diuretic, they should start.
Add another drug to regimen or use combination drug.

Hypertensive Emergencies
Urgency
when desirable to reduce BP in hours, no significant TOD, may have HA or vision disturbance.
Emergency
prevent or limit TOD (hemorrhage, encephalopathy, papilledema, unstable angina, MI, HF, pulmonary edema, aneurysm, preeclampsia)
BP >200/120 with s/s
Parenteral
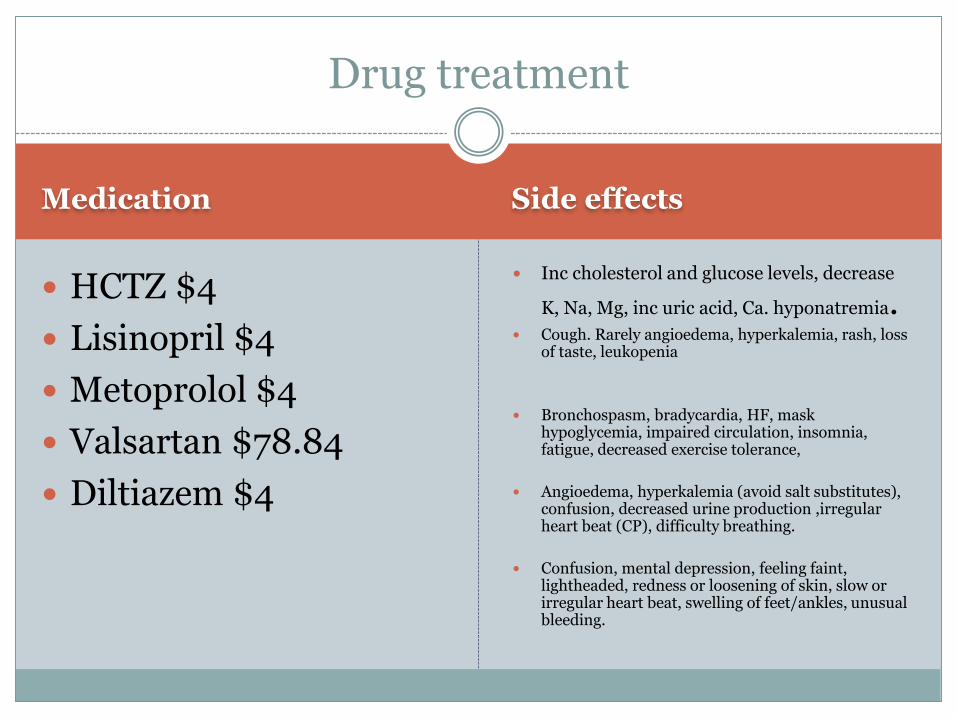
Medication Side effects
HCTZ $4
Lisinopril $4
Metoprolol $4
Valsartan $78.84
Diltiazem $4
Inc cholesterol and glucose levels, decrease
K, Na, Mg, inc uric acid, Ca. hyponatremia. Cough. Rarely angioedema, hyperkalemia, rash, loss
of taste, leukopenia
Bronchospasm, bradycardia, HF, mask hypoglycemia, impaired circulation, insomnia, fatigue, decreased exercise tolerance,
Angioedema, hyperkalemia (avoid salt substitutes), confusion, decreased urine production ,irregular heart beat (CP), difficulty breathing.
Confusion, mental depression, feeling faint, lightheaded, redness or loosening of skin, slow or irregular heart beat, swelling of feet/ankles, unusual bleeding.
Drug treatment

Newest trends, Ethical considerations
Trends
Increased focus on SBP and pulse pressure
Multiple drug therapy for faster control Diuretics included
Even slight elevations increase risk of CV disease. Strict adherence to numbers.
Ethics
Medication regimen and patient satisfaction/
participation emphasized.
Consider SE, pt goals. (DeMartinis, J., Uphold, C., & Graham, M., 2003).

Prevalence in United States
National Health and Nutrition Examination Survey
1988-1994 and 1999-2004
Prevalence rate increased 24.4% to 28.9%, largest inc in non-Hispanic women.
Attributed to increase in BMI
Treatment rates increased: 53.1% to 61.4%
Control rates increased: 26.1%-35.1% (Cutler et al, 2008).
Reference
Agency for Healthcare Quality and Research. (2006). Screening for high blood pressure. In The guide to clinical preventive services (pp. 67-70). Rockville, MD: Lippincott, Williams, & Wilkins.
Bickley, L.(2009). The cardiovascular system. In Bickley, L and Szilagyi, P (Eds.), Bates’ pocket guide to physical examination and history taking, 6th ed. Philedelphia: Lippincott, Williams, & Wilkins.
Breen, J. (2008). An introduction to causes, detection and management of hypertension. Nursing standard. 23(14): 42-46.
Burke, M. & Laramine, J. (2004) Cardiovascular system. In Burke, M. & Laramine, J. (Eds.) Primary care of the older adult: A multidisciplinary approach, 2nd Ed. (pp. 254-304). Philedelphia, PA: Mosby, Inc.
Cutler, J., Sorlie, P., Wolz, M., Thom, T., Fields, L., Roccella, E. (2008). Trends in Hypertension Prevalence, Awareness, Treatment, and Control Rates in United States Adults Between 1988–1994 and 1999–2004. Hypertension. 52: 818
DeMartinis, J., Uphold, C., & Graham, M. (2003). Cardiovascular problems. In Uphold, C. & Graham, M. (Eds.),
Clinical guidelines in family practice 4th ed. (pp 453-532) . Gainsville, Fl: Barmarrae books. US Department of Health and Human Services, National Institute of Health. (2003). Reference card from the seventh
report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Retrieved on March 11, 2009 from http://www.nhlbi.nih.gov/guidelines/hypertension/phycard.pdf.