Embed Size (px)
Citation preview

52 THE CANADIAN MEDICAL ASSOCIATION JOURNAL [July 1941
technique of the operation is described byWhipple4 who emphasizes the following points.(1) Adenomas of the islands of Langerhansrarely measure more than 2 cm. in diameter, andif they are embedded in the pancreas they maybe very difficult to find. (2) In a considerablenumber of cases more than one tumour is pres-ent. (3) If no tumour is found after carefulexamination of the whole gland, the body andtail of the pancreas, to the left of the superiormesenteric vessels, should be resected. In several
TABLE I.
OPERATIVE REMOVAL OF A TUMOUR OR TUMOURS OF THEISLANDS OF LANGERHAN
Total cases ......................... 56Islet-cell adenoma ...... ... .. 43Islet-cell carcinoma 13Died post-operatively....... 5Died from other causes. 5Unimproved (1 year). 1Insufficient data ................... 4
Cases with relief ofLength of follow-up of hypoglycxemia
8 years... 17 to 8 years 26 to 7 years 15 to 6 years 34 to 5 years 13 to 4 years ....... .. 62 to 3 years ....... 91 to 2 years ...... 8Less than 1 year ............. 10
41 (89 per cent)
cases in which such resection failed to relievethe symptoms, an adenoma was found in thehead of the pancreas at a second operation.The results of the surgical treatment of 90
cases of hypoglyciemia are summarized byWhipple in Tables I and Ii.
TABLE II.
RESECTION OF BODY AND TAIL OF PANCREAS(No TUMOUR FOUND)
Total cases ................. 34Died post-operatively ........ 4Insufficient data ............ 3
Length of Relief offollow-up symptoms Improved Unimproved
10 years... .. 16 to 7 years. 15 to 6 years. .. .. 24 to 5 years 4 1 23 to 4 years 12 to 3 years ..... 1 .. 21 to 2 years 3 15Less than 1 year. 3 1
10 4 13
REFERENCES1. HARRIS, S.: Gastro-intestinal manifestations of hyper-
insulinism, Ant. J. Digest. Dis. & Nutrition, 1935, 2:557.
2. JOHN, H.: Treatment of hyperinsulinism with insulin;further observations, Endocrinology, 1935, 19: 689.
3. LAIDLAW, G. F.: Nesidioblastoma, the islet tumour ofthe pancreas, Am. J. Path., 1938, 14: 125.
4. WHIPPLE, A. 0.: The surgical treatment of hyper-insulinism, J. Internat. de Chirurgie, Mai-Juin 1938.
5. WILDER, R. M., ALLEN, F. N., POWER, M. H. ANDROBERTSON, H. E.: Carcinoma of the islands of thepancreas; hyperinsulinism and hypoglycaemia, J.Am. M. Ass., 1927, 89: 348.
CASCADE STOMACH
BY V. D. SCHAFFNER, Kentvitle, N.S., AND G. V. BURTON, Yarmouth, N.S.
ALTHOUGH cascade stomach as an entity isnot rare the American and Canadian litera-
ture has made little mention of it. Slightlymore is to be found in the British and French.A recent case in which cascade stomach was apart of multiple gastro-intestinal abnormalitiesprompted the writing of this short article. Anew type of surgical treatment of possible valueis also suggested. So far as can be ascertainedthe operation proposed has not before beentried.
Cascade stomach may be defined as an abnor-mality of the organ in which the upper portionor fundus is turned, or flopped, backward insuch a manner as to form tw,o parts. It couldbe likened to, a beret pulled backward. Thecondition is not to b,e confused with hour-glass
stomach, in which one division of the stomachlies directly above the other. In cascade stomachthe upper and posterior portion consists of the"flopped over" fundus, which exists as an inertsac devoid of peristaltic motion. The lowerportion consists of the main body of the stomachwhich exhibits normal peristaltic motion andemptying ability. In the upright position theupper and posterior portion fills with food orliquid, and nothing enters the lower portionuntil this part overflows or spills into the lowerpart, thus giving it the name of "cascade" or"cup-and-spill " stomach.In reviewing the available literature it would
appear that there are almost as many theoriesof etiology as there are authors. In this paperit is not proposed to enter into any discussion

July 1941] SCHAFFNER AND BuRTON: CASCADE .T0MACH 53
of etiology, beyond enumerating some of theprincipal theories suggested. A few are asfollows: (1) spasm of oblique muscle fibres(Barclay); (2) short mesocolon and short gastro-hepatic ligament with adhesions (Feissley andFried) ; (3) increased pressure due to swallowedair (Malarque and Baize) ; (4) lateral displace-ment of the spleen with a resulting posteriorpocket, the stomach folding backward over thepancreas and splenic artery (His, and, later,Upham); (5) displacement of splenic flexureupward with consequent pressure on the fundus(Upham); (6) abnormal mobility of fundusfrom lack of support, due to absence or elonga-tion of the phrenico-gastric ligament. Othercauses are suggested, and it would appear that,in general, no definite etiology has yet beenestablished. It is probable that in various casesvarious factors, or combinations of factors, areat work, and for this reason no one treatmentcan be universally applied with success.
The condition occurs, for the most part, innervous or neurotic types, of sedentary habits.By some even neurosis has been described as acause. Certainly, nervous instability is not tobe found in all the cases. One of us (V.D.S.)now has a typical case of cascade stomach withits typical syndrome of symptoms in a child sixYears of age who is quite active and not of anervous type. The symptoms are those of epi-gastric distress, consisting of a feeling of full-ness or even pain coming on during eating.There is considerable swallowing and belchingof gas. This distress can be relieved by lyingdown after a meal, thereby allowing the uppersac to empty. The taking of alkalis or othermedicine, of course, gives no relief.
There is nothing characteristic about thephysical examination. The abdomen may besomewhat distended, especially in the upperhalf. By some it is stated that there is an un-usual prominence of the seventh, eighth, andninth ribs on the left side, with an abnormalfullness in the left hypochondrium.The diagnosis is made, of course, by means of
fluoroscopic and x-ray examination, which isvery definite and characteristic. Flat plate ex-amination, without the use of contrast media,is very suggestive. In practically all eases alarge collection of gas is to be seen in the regionof the splenic flexure and under the left dia-phragm. During the ingestion of an opaquemeal the picture is absolutely characteristic.The barium flows from the aesophagus into a
large, inert, globular sac. This sac exhibits noattempt at peristaltic action and, in the uprightposition, will not empty itself. It is not untilit is completely filled and distended that thebarium spills over its anterior wall, like a water-fall, into the body of the stomach, which exhibitsactive or hyperactive peristaltic action and, asa rule, empties quickly. By rotating the patientit becomes obvious that the upper sac lies to theleft, and posterior to the main body of thestomach.No attempt will be made to describe or discuss
in detail the many forms of treatment suggested,beyond stating that they have ranged all theway from the field of psychiatry to surgery.Various diets and medicines have been used and,it would appear, with very little success. Breath-ing exercise during and after meals is probablyas helpful as anything, but it must be rathertiresome and, at times, somewhat embarrassing,to take a swallow of food and then three or fourlong breaths. Resting in the prone position aftereating is helpful. The surgical attempts at cor-rection, in so far as can be made out, haveconsisted chiefly in the freeing of adhesions, andremoving various pathological conditions withinthe abdomen, and attempts at fixing the fundusunder the diaphragm in order to prevent drop-ping. From the reading of these attempts oneis again left with the impression that no greatdegree of success was attained.The case herein reported represents one in
which marked cascade stomach was a componentof multiple gastro-intestinal abnormalities.
CASE REPORTJ.M.S., aged 35, clergyman, was admitted to hos-
pital on March 27, 1940.Complaints.-Epigastric distress; difficulty in swallow-
ing; lower abdominal pain; abdominal distension.History of present illness.-The patient stated that
for the past four or five years he had had epigastricdistress during and after meals, with a feeling offullness and gas. Eructations gave little or no relief.The condition had been unrelieved by alkalis, specialdiets, and other types of medical treatment. He him-self had learned that by lying down for a half- tothree-quarters of an hour after meals some relief wasattained, but this was not complete. At times theupper abdomen felt tense and hard.
For a somewhat shorter length of time he had alsonoted that he had had difficulty in swallowing foodsand some substernal distress. Eating had to be donevery slowly or this distress was marked with a feelingthat the food was stuck in the aesophagus.
He had on occasions become nauseated but was neveral)le to vomit. Even when seasick, which he hadbeen on several occasions, he would become nauseatedand retch violently, but still emesis did not occur.Periodically, he had had sharp, crampy pains in thelower abdomen, associated with marked distension.These pains lasted from a very short time to severalhours. The longer they lasted, the greater was the
SCHAFFNER AND BURTON: CASCADE STOMACI-1 53July 1941]

54TECNDA EIA SOCAINJUNL[uy14
distension. There was no history of vomiting bloodor of passing tarry stools.
Personal family history.-Irrelevant, except that thepatient had had rheumatic fever as a child.
Physical examinatm-. The patient appeared paleand anwmic; thin and undernourished. A roughsystolic murmur was heard, transmitted into theaxilla; slight general distension of the abdomen.
Laboratory findings. -Urine: negative; red bloodcells 4,340,000; white blood cells 5,750; hgb. 76 percent. The Kahn test was negative.
X-ray findings.-The fluoroscopic and x-ray examina-tion of the gastro-intestinal tract, following the inges-tion of barium revealed the following. The bariumwas seen to flow through the upper portion of theaesophagus normally. At the lower portion there was
revealed the following findings. The barium enteredthe rectum and sigmoid without difficulty. Redundantloops of the sigmoid were coiled in the pelvis. (Inthe 24-hour plate a sigmoid loop extended high upunder the left diaphragm. Fig. 2). After some delaythe barium entered the descending colon and filledthe eeeum. The entire colon was flaccid and en-larged; no filling defects and no obstruction.
Drainage pictures showed the eceum to be dis-tended with barium. The ascending colon was freeof barium but distended with gas. There was amarked dilatation of the colon at the splenic flexurein which isolated patches of barium could be seen.The lower half of the colon contained some barium,and it was constricted and spastic. The redundantloops of the sigmoid were distended with barium, and
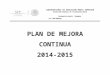
Fig. 1 Fig. 2Fig. 1.-X-ray of the stomach, showing large upper cascade portion with one fluid level, and the
main body of the stomach below showing another fluid level and peristaltic action. Fig. 2.-24-hourplate, showing long, redundant sigmoid loop.
marked delay, and ballooning of the oesophagus. Justbefore entering the hiatus the owsophagus was seento be kinked to more than 90 degrees. From theangulation the cesophagus extended in a lateral posi-tion for about one inch before passing through thehiatus. After complete ingestion of the meal in theupright position the barium was seen to pool in asac-like formation measuring 53/4 l)y 4 inches. Thisportion of the stomach was smooth and regular inoutline, and in it there was a total absence of peri-stalsis. In the prone position and on rotating thepatient the barium was seen to flow from the fundalsac and fill the remainder of the stomach (see Fig. 1).It was to be noted that the stomach was large andptosed. In the body of the stomach there was nofilling defects, and peristalsis was hyperactive. Theduodenal cap filled well and was regular in outline.The patient was immediately examined again in theupright position, and two barium levels were noted(Fig. 1). The barium pooled in the large sac of thefundus forming one level, and that in the body formedanother. On pressure the barium could be made toflow back and forth from one section to another.
Diagnosis.-Idiopathic dilatation of the oesophagus(cardiospasm); cascade stomach.
Fluoroscopic and x-ray examination of the largebowel, following an injection of a barium enema,
rested in the lower pelvis. The appendix was notvisualized.
Diagnosis. Long redundant sigmoid and atonic colon.From the examinations carried out it became
obvious that the patient was suffering from threegastro-intestinal abnormalities, all of which werecausing symptoms. First, there was the dilatation ofthe cesophagus; second, the cascade stomach; andthird, the large, atonic colon with an extremely longsigmoid loop. What causative relationship one condi-tion had to another is difficult to state.
The patient was temporarily discharged from thehospital on March 30, 1940, and readmitted on April11, 1940. Operation was performed under nupercainespinal anesthesia on April 13, 1940.
Operation.-Marwedel incision. The seventh cartilagewas divided at the sternum. It was not necessary todivide the seventh, eighth, and ninth cartilages lateral-ly, as they were very soft and could easily be re-tracted. The left coronary ligament was divided, andthe left lobe of the liver depressed. The excessivelylong sigmoid loop lay up over the stomach. This wasdisplaced into the lower abdomen. The fundus of thestomach was very much larger than usual, somewhatthickened, but atonic and flaccid. The cascade de-formity was not apparent. (This is always so at thetime of operation). The spleen was small and dis-
54 THE CANADIAN MEDICAL ASSOCIATION JOURNAL [July 1941

July 1941] SCHAFFNER AND BURTON: CASCADE STOMACH 55
placed laterally. The space above the pancreas andbehind the fundus was deeper and larger than usual.The abdominal portion of the awsophagus was of nor-mal length and size. There was no muscle hyper-trophy, or other evidence of spasm. The peritoneumwas incised around the cesophagus, the crus of thediaphragm incised laterally, and the mediastinumentered. The lower portion of the aesophagus wasfreed with the finger, allowing about one and a halfor two inches of it to come through the diaphragminto the abdomen. In this case the vagi were notcut. The hiatus was of usual size. The freed portionof the cesophagus was fixed below the diaphragm.The fundus was then freed. Its superior attachmentsappeared elongated and lax. The entire fundus wasresected laterally to below the level of the splenicartery, leaving only a strip on the lesser curvatureside about one and one-half inches wide. This wasconverted into a tube not much larger than thecesophagus itself (see Figs. 3 and 4). The wound wasclosed in layers.
Pathological examination of the resected fundusrevealed no evidence of gastritis or other abnormality.
Progress.-The patient experienced immediate relieffollowing his operation. Diet was slowly increasedand eating produced no distress. The patient wasdischarged on his sixteenth post-operative day, and
redundant sigmoid existed. A few years agothe late Dr. F. A. C. Scrimger performed anddescribed his aesophagoplasty for idiopathic dila-tation of the aesophagus. His cases were ob-served. Since then one of us (V.D.S.) hasoperated upon two cases in.which the conditionexisted by itself, without other discoverable ab-normality, using the Scrimger operation withextremely satisfactory results. One of thesecases has been reported.
It appeared that in the present case underdiscussion the cesophageal lesion deserved surgi-cal correction, and that the stomach should atthe same time be dealt with by a method whichseemed most appropriate at the time of operation.As would appear from the operative report
and x-ray investigation, several factors might beat work to produce the cascade deformity of
Fig. 3 Fig. 4
Fig. 3.-Diagram of the stomach, showing normal and anatomical relations to the splenicartery and pancreas. Fig. 4.-Diagram representing the operation proposed: Resection of fundus andgreater curvature of the stomach to below a level of the splenic artery and pancreas.
at that time was able to eat a fairly liberal diet with-out distress of any kind.
Fluoroscopic examination, previous to discharge,revealed the following. The barium passed unob-structed to the stomach. There was very slight gen-eral aesophageal delay, but the kinking and dilatationpreviously noted had disappeared. Below the dia-phragm the barium passed through a narrow tube tothe lower portion of the stomach with no upper delayor cascade.
The patient has been followed by means of corres-pondence since discharge. He has had no return insymptoms, and has gained a considerable amount ofweight. He last wrote the first week in November,expressing extreme gratitude, and stated that he waswell for the first time in years, and able to carry onhis work without burden.
COMMENTA case presented itself in which a combination
of idiopathic dilatation of the aesophagus,cascade stomach, and atonic colon with a long
the stomach. First, the splenic flexure was highand distended with gas (a constant factor re-ported in other cases) ; secondly, in this casethere was a long distended loop of sigmoid whichfrequently lay over the upper portion of thestomach; thirdly, the spleen was small anddisplaced laterally, with a deep depression abovethe splenic artery and pancreas into which thefundus could be forced, thus flopping it overbackward to form the cascade. Finally, thesuperior support of the stomach was elongatedand lax, thus allowing of a dropping of thispart. Certainly enough real organic abnor-malities were present to make a neurotic basisof the condition more than doubtful, and to
justify surgical correction.
55SCHAFFNER AND BURTON: CASCADE STOMACHJuly 1941]

56 THE CANADIAN MEDICAL ASSOCIATION JOURNAL [July 1941
A reasonable surgical treatment would seemto be that which was done, namely, to removethe entire fundus laterally to below the level ofthe splenic artery, thus converting it into avery much elongated aesophagus to a point belowthe level named.
BIBLIOGRAPHY1. BARCLAY, A. E.: Variations of the normal stomach
The Lancet, 1921, 1: 648.
2. CROHN, B. B.: Affections of the Stomach, Saunders,Phila., 1927, p. 175.
3. FEISSLEY, R. AND FRIED, A.: Etiology of cascades'omach, Fortschr. a. d. Geb. d. Rontgenstrahlen,1922, 29: 237.
4. UPHAM, A. M.: J. Diges. Dis. & Nutrit., 1935-1936, 2:38.
5. KAUFMANN, W.: Cascade stomach and its relationsto internal and cardiac disturbances, Deutschemed. Wchnschr., 1940, 66: 230.
6. McLEOD, J. W.: Cascade stomach, Canad. M. Ass. J.,1937, 36: 242.
7. BLACKERT: The cascade stomach, Deutsche med.lVchnschr., 1933, 59: 532. ffiffiffil
8. SCRIMGER, F. A. C.: Ann. Surg., 1931, 94: 801.9. SCHAFFNER, V. D.: A case of idiopathic dilatation
of the oesophagus, Canad. M. Ass. J., 1935, 33: 532.
RETROPERITONEAL PNEUMOGRAPHY*
BY N. W. ROOME
London, Ont.
VISUALIZATION of the contours of the struc-tures lying behind the peritoneal cavity by
insufflation of a gas about them and subsequentx-rays was introduced in 1921 by Carelli andSordelli,' and Rosenstein.2 Application of thismethod to demonstrate the adrenal glands andtumours thereof was made by Mosenthal,3 L6serand Israel,4 and its value in this connection waslater emphasized by Cahill.5
This technique is not one of wide or routineusage, but offers in certain selected cases in-formation otherwise unobtainable. The principalfield of usefulness is for adrenal visualization,as advances in pyelography have rendered it lessnecessary in the diagnosis of kidney lesions, inwhich field it was once considered a valuablediagnostic aid. In isolated cases, however, as invery small children, it may be used to outlinethe kidney; and it may also be useful in thediagnosis of retroperitoneal masses other thankidney and adrenal.
Essentially, the method consists of introduc-ing a quantity of air into the perirenal fat, andfilming the area during the following 24 to 36hours. About 200 c.e. are introduced, andusually 12 to 18 hours are required for sufficientmigration of the air about the solid structuresto visualize the kidney and adrenal most clearly.The normal adrenal is not always well defined,because of its flatness and irregular borders, butthe kidney and the various rounded tumours areusually quite visible.A number of modified techniques have been
described recently. Mencher6 suggested rowingexercises, after injection of the air, to aid in
* From the Departments of Surgery, the Universityof Chicago, and the University of Western Ontario.
Read at the Seventy-first Annual Meeting of theCanadian MIedical Association, Toronto, June 20, 1940.
its distribution. Giantureo and Drenckhahn7advised localization of the needle by punctureof the renal cortex, followed by withdrawal tothe proper position. Roome8 dispensed withfiltration of the air used, and otherwise simplifiedthe technique. Cope and Schatzki,9 in a studyin 78 patients, injected the air into the trian-gular fat-filled space below the lower pole of thekidney, feeling that this reduced the danger ofair embolism.The procedure is not one to be attempted too
lightly, for, as in all areas in which a gas isinjected into the body, air embolism is constantlya possibility. Fish'0 reported a death followinginjection into the substance of a large necrotictumour, and Weyrauch1" recently reported an-other fatal case. The latter author deprecatesthe use of vigorous exercise, or of renal punc-ture as a part of the technique because of thisdanger. No details of technique will be reviewedhere, as these are already fully described in theliterature.5' 8, 9
My experience with the method consists ofobservations on 17 cases, in 12 of which the in-jections were bilateral. All the films werethought to be of diagnostic value. The patientsusually complained of a feeling of fullness inthe abdomen (one describing it as if havingswallowed a tennis ball), but this usually wasnot severe, and rapidly disappeared. Threepatients had somewhat severe pain, which wethought was due to elevation of the peritoneumfrom the anterior aspect of the kidney. Therewere no serious complications of any kind.Most of the examinations were made in
hirsute women with varying degrees of Cush-ing's syndrome, in which adrenal cortex virilismwas suggested. No tumour was found in any