Embed Size (px)
Citation preview

610 lAce \'01 7, No 3 March I'iX6 61 O-b
Hypoplastic Left Heart Syndrome: Is Echocardiography Accurate Enough to Guide Surgical Palliation?
STEPHEN E. BASH, MD, JAMES C. HUHTA, MD, FACC, G. WESLEY VICK III, MD, PHD,
HOWARD P. GUTGESELL, MD. FACC. DAVID A. OTT. MD, FACC
HOl/stoll. Texas
Two-dimensional echocardiography can diagnose hy•poplastic left heart syndrome. However, with the advent of the possibility of palliative open heart surgery, com•plete anatomic diagnosis is necessary. The anatomic find•ings of 15 neonates with hypoplastic left heart syndrome (age 1 to 10 days, mean 4.1) who had two-dimensional Doppler echocardiographic studies were compared with the results obtained by angiography (6 cases), surgery (11 cases) and autopsy (8 cases). Complete two-dimen•sional echocardiographic examination of the aortic arch, pulmonary and systemic venous return, atrial septum, ductus arteriosus and proximal coronary arteries was possible in all 15 neonates and correctly diagnosed hy•poplastic left heart syndrome in each. Anatomic two-
M-mode echocardiography can diagnose hypoplastic left heart syndrome (1.2); however. false positive and false neg•ative results can occur (3,4). Lange et a!. (5) demonstrated that the diagnosis of hypoplastic left heart syndrome could be made with two-dimensional echocardiography. Before the onset of palliative surgery, this was all that was nec•essary because no further intervention was planned. How•ever. with the reports of Norwood and Lang and coworkers (6.7). which showed that palliative surgery could be per•formed successfully in neonates with hypoplastic left heart syndrome. not only is the diagnosis important but all other aspects of the cardiac anatomy must be known.
The purpose of this study was to answer the following question: Can the anatomy of hypoplastic left heart syn-
From The LIIlte Frank Abercrombie Section of Cardiology. Department of PedIatric" Baylor College of Medicme and Texas Children's Hospital, Houston. Texas. This study was supported m part by Grant RR-05425 from the NalIonallnstitutes of Health. United States PublIc Health SerVIce, Bethesda, Maryland and Grant RR-OOI88 from General Clinical Research Branch, Nallonal Inslllute, of Health. Bethesda. Dr. Huhta was supported by New Investigator Research Award HL31153 from the National Heart, Lung. and Blood Inshtute, Publtc Health ServICe, Bethesda. Maryland
Manuscript receIved August 6. 1985: revised manu,cript receIved Oc•tober 8. 1985, accepted October 23, 1985.
Address for reprints. James C Huhta, MD, Pedlatnc Cardiology. Texa, Children's Hospital, 6621 Fannin Street, Houston. Texas 77030,
'!" 1986 hy the Amencan College of CardIOlogy
dimensional echocardiographic assessment was accurate in 13 (86%) of the 15 neonates and there were no false positive results. Undiagnosed associated abnormalities were hypoplasia of a left pulmonary artery in one patient and left superior vena cava in another. Accurate quan•titation of the size of the tricuspid valve anulus, ascend•ing aorta, pulmonary anulus and right and left pulmo•nary arteries was possible. Doppler examination was performed in seven patients and confirmed retrograde aortic arch flow and right to left systolic shunting in the patent ductus arteriosus. In selected neonates, surgical palliation can be attempted without angiography.
(J Am Coli CardioI1986;7:610-6)
drome be diagnosed accurately by two-dimensional Doppler echocardiography without resorting to cardiac catheteriza•tion before surgical palliation? We attempted to assess the diagnostic accuracy of two-dimensional Doppler echocardi•ography and the quantitative morphologic measurements obtained with echocardiography compared with measure•ments obtained at autopsy.
Methods Patients. Between February 1983 and July 1984. 15
patients with hypoplastic left heart syndrome underwent two-dimensional echocardiography and corroboration of their anatomy by cardiac catheterization, surgery or autopsy. Cri•teria for entry into the study included situs solitus of the atria and viscera. atrioventricular (A V) concordance, single outlet right ventricle with aortic atresia, an aortic valve anulus that was 3 mm or less in diameter or not detectable and a left ventricular cavity that was too small to support the systemic circulation on the basis of our previous ob•servations (8). One patient with critical aortic stenosis and a markedly underdeveloped left ventricle was therefore in•cluded. Patients with left ventricular hypoplasia who had double inlet ventricle. double outlet right ventricle or A Y septal defect were excluded from the study. Patients' ages
0735-1097/86/$350
lACC Vol 7, No 3 March 1986 610-6
ranged from I to 10 days (mean 4) and their weights ranged from 2.4 to 4.4 kg (mean 3,3), Palliative surgery was per•formed in II of the 15 patients, Autopsy was performed in 8 and cardiac catheterization in 6 of the 15,
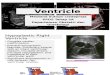
Two-dimensional echocardiographic studies. These studies were performed in all 15 neonates using 5 or 7,5 MHz scanning (Advanced Technology Laboratories 600 MK), The heart and cardiovascular anatomy were interrogated using a systematic approach, Special attention was paid to extracardiac structures, Including aortic arch configuration, pulmonary artery anatomy, pulmonary and systemic venous connection and atrial and ventricular morphology (Fig, I to 3), Imaging was used to confirm the presence of a left coronary artery (Fig, 4),
In the eight patients who had autopsy examination, quan•titative morphologic measurements were made using two-
Figure 1. Two-dimensional echocardiogram taken from the subxi•phoid position (upper panel) showing the site of measurement of the tricuspid valve (TV) anulus (arrows), The transducer was then angled more posteriorly (lower pane\) to a four chamber view where the mitral valve (MV) anulus (arrows) and left ventricle (bold arrow) are visualized, I '" infenor; L = left; LA = left atrium; R = right; RA = right atrium; RV = right ventricle; S '" superior.
_.
BASH ET AL HYPOPLASTIC LEFr HEART ECHOCARDlOGRAPHY
,-1IY ,'J I
~:II"':: •
0It:" I
h:~ •. -"
611
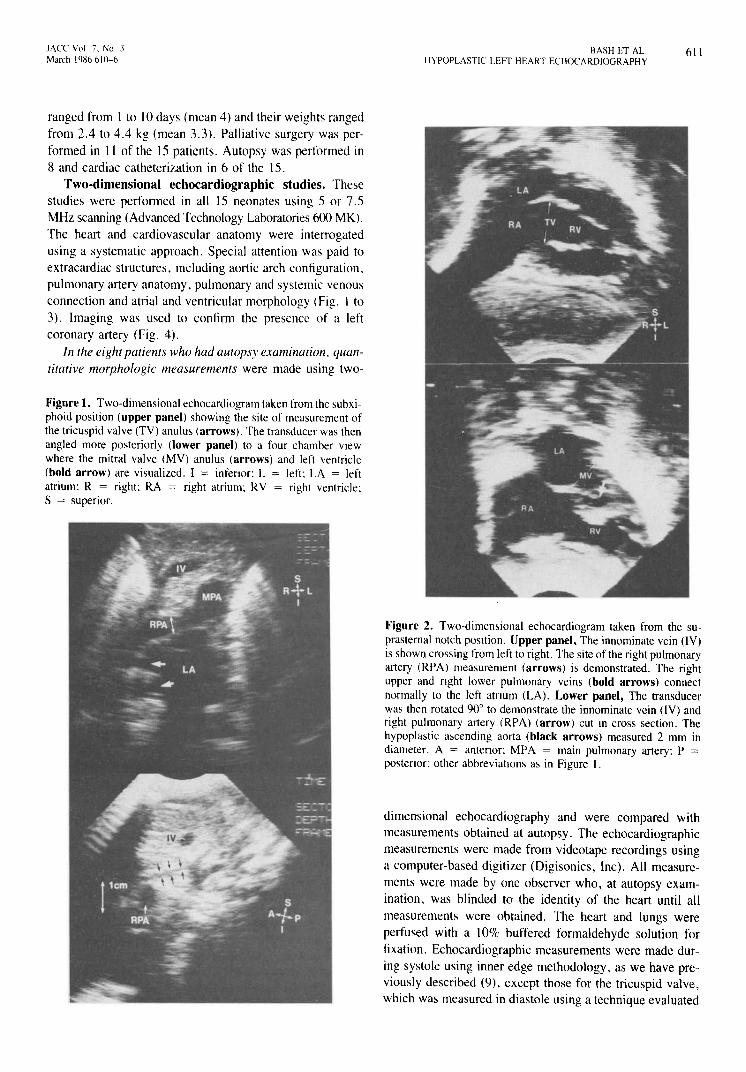
Figure 2. Two-dimensional echocardiogram taken from the su•prasternal notch posItion. Upper panel, The innominate vein (IV) is shown crossing from left to right. The site of the right pulmonary artery (RPA) measurement (arrows) is demonstrated, The right upper and nght lower pulmonary veins (bold arrows) connect normally to the left atnum (LA), Lower panel, The transducer was then rotated 90° to demonstrate the innominate vein (IV) and right pulmonary artery (RPA) (arrow) cut In cross section, The hypoplastic ascending aorta (black arrows) measured 2 mm in diameter. A '" antenor; MPA = main pulmonary artery; P posten or; other abbreviattons as in Figure 1.
dimensional echocardiography and were compared with measurements obtained at autopsy, The echocardiographic measurements were made from videotape recordings using a computer-based digitizer (Digisonics, Inc), All measure•ments were made by one observer who, at autopsy exam•ination, was blinded to the identity of the heart until all measurements were obtained, The heart and lungs were perfused with a 10% buffered formaldehyde solution for fixation, Echocardiographic measurements were made dur•ing systole using inner edge methodology, as we have pre•viously described (9), except those for the tricuspid valve, which was measured in diastole using a technique evaluated
612 BASH ET AL HYPOPLAS flC LEFT HEAR r ECHOCARDIOGRAPHY
JACC Vol 7. No J March 1986610-6
'1\£:-'. :v-- -"" -
-_. ~-'~r~=-:' . . -~.~)t • T~_.;.. r
a c
.... ... .11-""
---
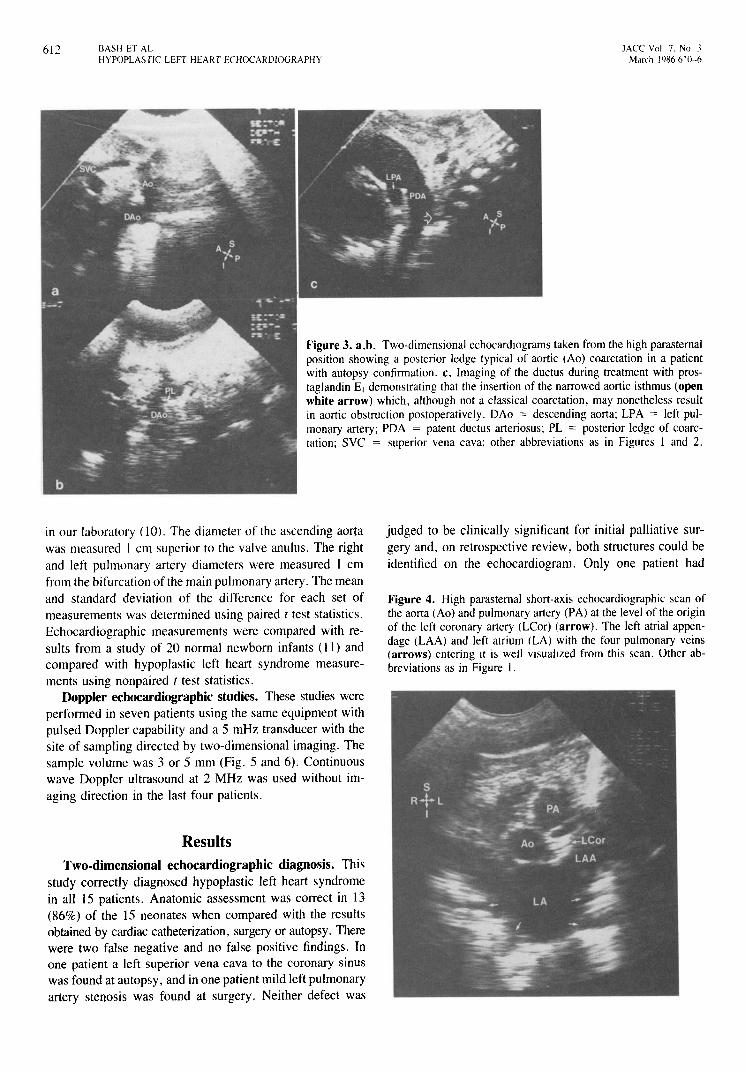
Figure 3. a,b. Two-dimensional echocardIOgrams taken from the high parasternal position showing a posterior ledge typical of aortic (Ao) coarctation in a patient with autopsy confirmation. c, Imaging of the ductus during treatment with pros•taglandin E, demonstrating that the insertion of the narrowed aortic isthmus (open white arrow) which, although not a classical coarctation, may nonetheless result in aortic obstruction postoperatively. DAo == descending aorta; LPA == left pul•monary artery; PDA == patent ductus arteriosus; PL = posterior ledge of coarc•tation; SVC = superior vena cava; other abbreviations as in Figures I and 2. ... ....
b
in our laboratory (10). The diameter of the ascending aorta was measured I em superior to the valve anulus. The right and left pulmonary artery diameters were measured 1 cm from the bifurcation of the main pulmonary artery. The mean and standard deviation of the difference for each set of measurements was determined using paired t test statistics. Echocardiographic measurements were compared with re•sults from a study of 20 normal newborn infants (11) and compared with hypoplastic left heart syndrome measure•ments using non paired t test statistics.
Doppler echocardiographic studies. These studies were performed in seven patients using the same equipment with pulsed Doppler capability and a 5 mHz transducer with the site of sampling directed by two-dimensional imaging. The sample volume was 3 or 5 mm (Fig. 5 and 6). Continuous wave Doppler ultrasound at 2 MHz was used without im•aging direction in the last four patients.
Results Two-dimensional echocardiographic diagnosis. This
study correctly diagnosed hypoplastic left heart syndrome in all 15 patients. Anatomic assessment was correct in 13 (86%) of the 15 neonates when compared with the results obtained by cardiac catheterization, surgery or autopsy. There were two false negative and no false positive findings. In one patient a left superior vena cava to the coronary sinus was found at autopsy, and in one patient mild left pulmonary artery stenosis was found at surgery. Neither defect was
judged to be clinically significant for initial palliative sur•gery and, on retrospective review, both structures could be identified on the echocardiogram. Only one patient had
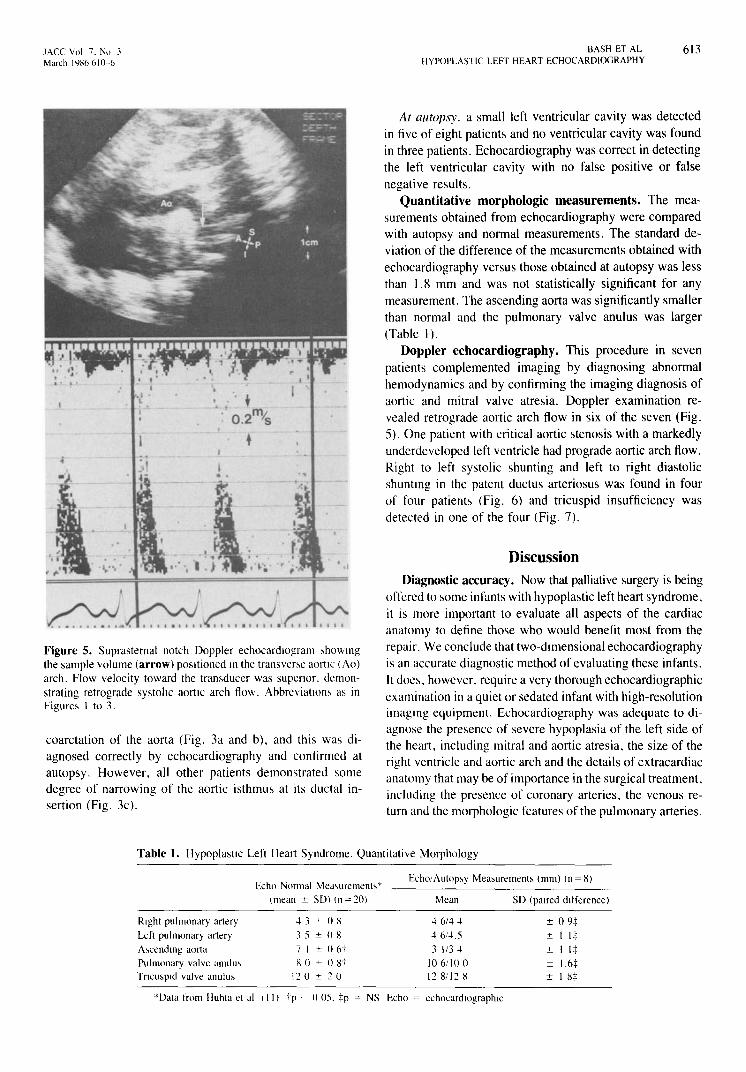
Figure 4. High parasternal short-axis echocardiographic scan of the aorta (Ao) and pulmonary artery (PA) at the level of the origin of the left coronary artery (LCor) (arrow). The left atrial appen•dage (LAA) and left atrium (LA) with the four pulmonary veins (arrows) entering It is well visualized from this scan. Other ab•breviations as in Figure I.
lACC Vol 7, No 3 March I<JX6 610-6
'~ ,"1:, ;--:; j .." .1 '-. ..,.;,. .,..
. , + ~·!o· 2mi . • S
+
......... ~. Figure 5. Suprasternal notch Doppler echocardlOgram ,hoWIng the sample volume (arrow) pOSitioned In the transven,e aortic (Ao) arch. Flow velocity toward the tram,ducer was supenor. demon•strating retrograde systohc aortic arch flow, Abbreviation!> as in Figure, 1 to 3.
coarctation of the aorta (Fig, 3a and b). and this was di•agnosed correctly by echocardiography and confirmed at autopsy, However. all other patients demonstrated some degree of narrowing of the aortic isthmu~ at its ductal in•sertion (Fig, 3c).
BASH ET AL HYPOPLASTIC LEFT HEART ECHOCARDIOGRAPHY
613
At autopsy. a small left ventricular cavity was detected in five of eight patients and no ventricular cavity was found in three patients, Echocardiography was correct in detecting the left ventricular cavity with no false positive or false negative results,
Quantitative morphologic measurements. The mea•surements obtained from echocardiography were compared with autopsy and normal measurements, The standard de•viation of the difference of the measurements obtained with echocardiography versus those obtained at autopsy was less than 1,8 mm and was not statistically significant for any measurement. The ascending aorta was significantly smaller than normal and the pulmonary valve anulus was larger (Table I),
Doppler echocardiography. This procedure in seven patients complemented imaging by diagnosing abnormal hemodynamics and by confirming the imaging diagnosis of aortic and mitral valve atresia, Doppler examination re•vealed retrograde aortic arch flow in six of the seven (Fig. 5), One patient with critical aortic stenosis with a markedly underdeveloped left ventricle had prograde aortic arch flow, Right to left systolic shunting and left to right diastolic shuntIng in the patent ductus arteriosus was found in four of four patients (Fig, 6) and tricuspid insufficiency was detected in one of the four (Fig, 7),
Discussion Diagnostic accuracy. Now that palliative surgery is being
offered to some infants with hypoplastic left heart syndrome, it is more important to evaluate all aspects of the cardiac anatomy to define those who would benefit most from the repair. We conclude that two-dimensional echocardiography is an accurate diagnostic method of evaluating these infants. It does. however, require a very thorough echocardiographic examination in a quiet or sedated infant with high-resolution imagIng equipment. Echocardiography was adequate to di•agnose the presence of severe hypoplasia of the left side of the heart. including mitral and aortic atresia, the size of the right ventricle and aortic arch and the details of extracardiac anatomy that may be of importance in the surgical treatment, including the presence of coronary arteries. the venous re•turn and the morphologic features of the pulmonary arteries.
Table 1. Hypoplastic Left Heart Syndrome. Quantitative Morphology
Echo Normal Meawremenb T
(mean ± So) (n=20)
Echo/Autop,y Mem,urement, (mm) (n=8)
Right pulmonary artery Left pulmonary artery A,cendlng aorta Pulmonary valve anulu, Tncu'pld valve anulu,
43 ± 0 X 35 ± 0 g
7 I ± 06i" H 0 ± 08t
120 ± 20
Mean
46/44 46/4,5 3 1/34
to 6/10 0 12 8!l2 H
*Data from Huhta et al (II) tp' () 05. :j:p = NS Echo = cchocardlographlc
SD (paired difference)
± 091: ± I 1-1: ± I 1+ ± l.6:j: ± I 8:1:
614 BASH ET AL HYPOPLASTIC LEFT HEART ECHOCARDIOGRAPHY
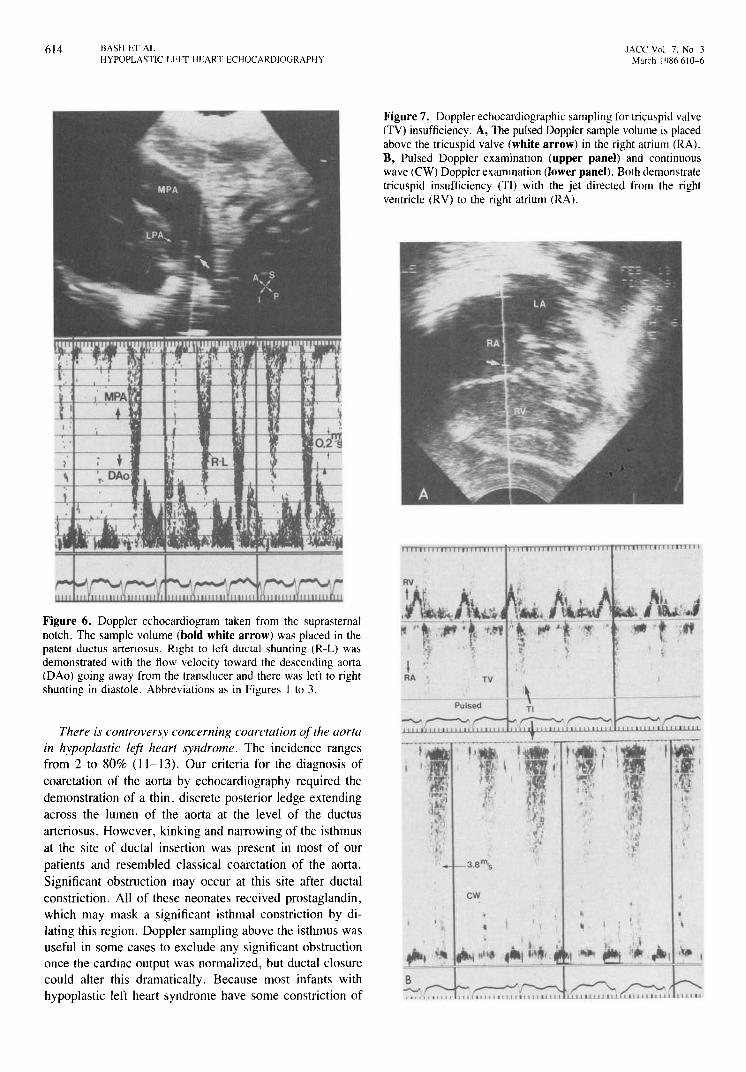
Figure 6. Doppler echocardiogram taken from the suprasternal notch. The sample volume (bold white arrow) was placed in the patent ductus artenosus. RIght to left ductal shunting (R-L) wa; demonstrated with the flow velocity toward the descending aorta (DAo) going away from the transducer and there was left to right shunting in diastole. Abbreviations as in Figures I to 3.
There is controversy concerning coarctation of the aorta in hypoplastic left heart syndrome. The incidence ranges from 2 to 80% (11-13). Our criteria for the diagnosis of coarctation of the aorta by echocardiography required the demonstration of a thin, discrete posterior ledge extending across the lumen of the aorta at the level of the ductus arteriosus. However, kinking and narrowing of the isthmus at the site of ductal insertion was present in most of our patients and resembled classical coarctation of the aorta. Significant obstruction may occur at this site after ductal constriction. All of these neonates received prostaglandin, which may mask a significant isthmal constriction by di•lating this region. Doppler sampling above the isthmus was useful in some cases to exclude any significant obstruction once the cardiac output was normalized, but ductal closure could alter this dramatically. Because most infants with hypoplastic left heart syndrome have some constriction of
lACC Vol 7, No 3 March 1486 610-6
Figure 7. Doppler echocardiographic sampling for tricw,pid valve (TV) insufficiency. A, The pulsed Doppler sample volume is placed above the tricuspid valve (white arrow) in the right atrium (RA). B, Pulsed Doppler examination (upper panel) and continuous wave (eW) Doppler exammation (lower panel). Both demonstrate tricuspid insufficiency (TI) with the jet directed from the right ventricle (RV) to the right atrium (RAJ.
cw
t, . , t
~=~~'~~~~-~~~~=~~~F==~~~-'~~~'~ B
,""-,,,
lACC Yol 7. No J March 19R6 h I O~h
-•;;t-,
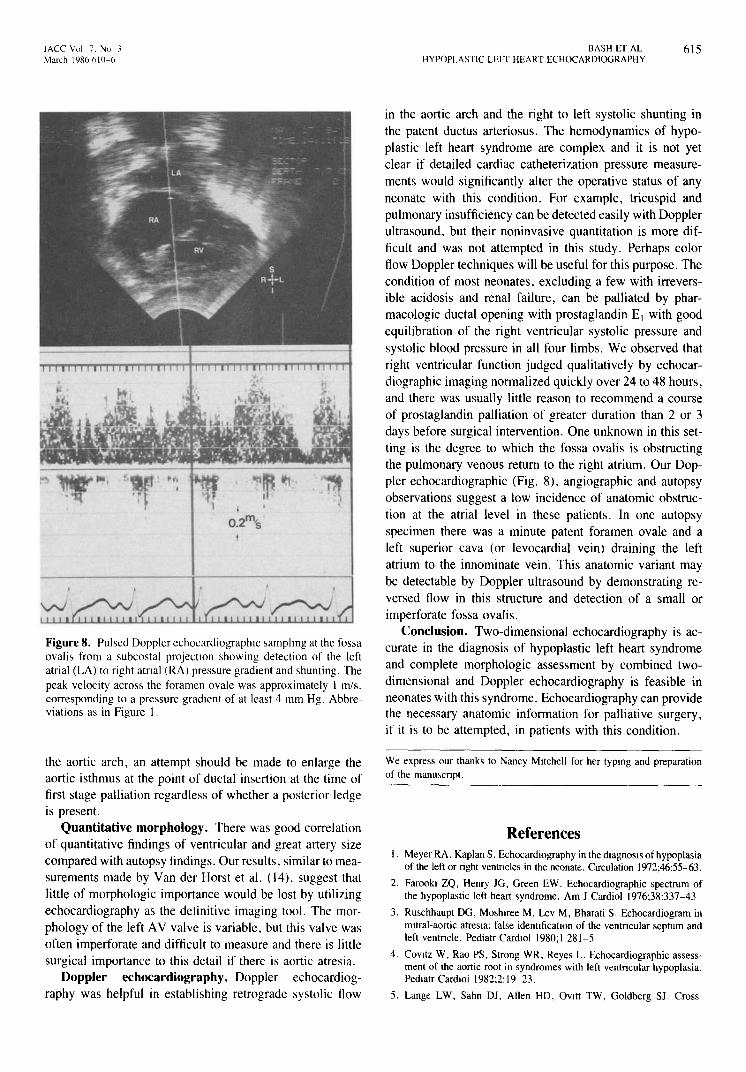
Figure 8. Pulsed Doppler echocardiographlc ,amphng at the fossa ovali, from a subcostal projectIon showing detection of the left atrial (LA) to right atnal (RAJ pres,ure gradient and shunting. The peak velocity across the foramen ovale was approximately 1 m/s. corresponding to a pressure gradient of at least 4 mm Hg. Abbre•viations as in Figure I.
the aortic arch, an attempt should be made to enlarge the aortic isthmus at the point of ductal insertion at the time of first stage palliation regardless of whether a posterior ledge is present.
Quantitative morphology. There was good correlation of quantitative findings of ventricular and great artery size compared with autopsy findings. Our results, similar to mea•surements made by Van der Horst et al. (14). suggest that little of morphologic importance would be lost by utilizing echocardiography as the definitive imaging tool. The mor•phology of the left A V valve is variable, but this valve was often imperforate and difficult to measure and there is little surgical importance to this detail if there is aortic atresia.
Doppler echocardiography. Doppler echocardiog•raphy was helpful in establishing retrograde systolic flow
BASH ET AL HYPOPLASTIC LEFr HEART ECHOCARDIOGRAPHY
615
in the aortic arch and the right to left systolic shunting in the patent ductus arteriosus. The hemodynamics of hypo•plastic left heart syndrome are complex and it is not yet clear if detailed cardiac catheterization pressure measure•ments would significantly alter the operative status of any neonate with this condition. For example, tricuspid and pulmonary insufficiency can be detected easily with Doppler ultrasound, but their noninvasive quantitation is more dif•ficult and was not attempted in this study. Perhaps color flow Doppler techniques will be useful for this purpose. The condition of most neonates, excluding a few with irrevers•ible acidosis and renal failure, can be palliated by phar•macologic ductal opening with prostaglandin EI with good equilibration of the right ventricular systolic pressure and systolic blood pressure in all four limbs. We observed that right ventricular function judged qualitatively by echocar•diographic imaging normalized quickly over 24 to 48 hours, and there was usually little reason to recommend a course of prostaglandin palliation of greater duration than 2 or 3 days before surgical intervention. One unknown in this set•ting is the degree to which the fossa ovalis is obstructing the pulmonary venous return to the right atrium. Our Dop•pler echocardiographic (Fig. 8), angiographic and autopsy observations suggest a low incidence of anatomic obstruc•tion at the atrial level in these patients. In one autopsy specimen there was a minute patent foramen ovale and a left superior cava (or levocardial vein) draining the left atrium to the innominate vein. This anatomic variant may be detectable by Doppler ultrasound by demonstrating re•versed flow in this structure and detection of a small or imperforate fossa ovalis.
Conclusion. Two-dimensional echocardiography is ac•curate in the diagnosis of hypoplastic left heart syndrome and complete morphologic assessment by combined two•dimensional and Doppler echocardiography is feasible in neonates with this syndrome. Echocardiography can provide the necessary anatomic information for palliative surgery, if it is to be attempted, in patients with this condition.
We express our thanks to Nancy Mitchell for her typmg and preparation of the manw,cript.
References I. Meyer RA. Kaplan S. Echocardiography in the diagnOSIs of hypoplasia
of the left or right ventncles in the neonate. Circulation 1972;46:55-63.
2. FarookI ZQ, Henry JG, Green EW. Echocardiographic spectrum of the hypoplastic left heart syndrome. Am J Cardiol 1976;38:337-43
3. Ru~chhaupt 00, Moshlree M. Lev M, Bharati S. Echocardiogram in mitral-aortic atresia: false identIficatIon of the ventncular septum and left ventncle. Pediatr CardlOl 1980;1281-5
4. COVltz W. Rao PS, Strong WR, Reyes L. Echocardiographic assess•ment of the aortic root in syndromes with left ventricular hypoplasia. Pedlatr CardlOi 1982:2:19-23.
5, Lange LW. Sahn OJ. Allen HD, OvItt TW. Goldberg SJ, Cross-

616 BASH ET AL HYPOPLASTIC LEFI' HEART ECHOCARDlOGRAPHY
sectIonal echocardlOgraphy 10 hypoplastic left ventncle: echocardlO•graphIC-anglographlC-anatomic correlations. PedIatr Cardlol 1980: 1.287-99
6 Norwood WI, Kirklin JK, Sanden, SP. Hypoplastic left heart ,yn•drome: expenence with palliatIve surgery Am J CardmI1980:45:87-91
7. Lang P, Norwood WI. HemodynamiC assessment after palliative sur•gery for hypoplastic left heart syndrome. Circulation 1983,68: 104-S
8. Latson LA, Cheatham JP, Gutgesell HP. RelatIon of the echocardio•graphiC estimate of left ventncular Size to mortality m infants with severe left ventricular outflow obstructmn. Am J Cardlol 1981,48:887-91.
9. Gutgesell HP, Huhta JC, Cohen MH, Latson LA. Two-dimensional echocardlographlc assessment of pulmonary artery and aortic arch anatomy m cyanotic mfants. J Am Coli Cardlol 1984:4: 1242-6.
JACC Vol 7, No } March 1'18(1 b10-6
10. Kmg DH, Smith EO, Huhta JC, Gutgesell HP Mitral and tncw,pld valve anular diameter 10 normal children determmed by two-dimen•sional echocardlography Am J Cardiol 1985:55:787-9.
II. Huhta JC, Cohen M, Gutgesell HP. Patency of the ductus artenosus in normal neonates: two-dimensional echocardlography versus Dop•pler assessment J Am Coli Cardlol 1984;4:561-4.
12 BharatI S, Lev M. The surgical anatomy of hypoplaSia of aortic tract complex. J Thorac Cardiovasc Surg 1984,88:97-101.
13 Hawkms JA, Doty DB. Aortic atresia: morphologic charactenstlcs affecting surVival and operative palliation J Thorac Cardiovasc Surg 1984.88:620-6.
14. Van der Horst RL, Hastreiter AR. DuBrow lW, Eckner FA. PathologiC measurements in aortic atresia. Am Heart J 1983:106:1411-5.