Embed Size (px)
Citation preview
1
HYPOTHETICAL ANATOMY/VALUES
Shoulder/cervical The Petitioner was born in 1985. He is 5’10” and weighs 200 pounds. He has been employed for the past 12 years as a full-time (40-hour per week, $52K per year salary) maintenance employee for a municipal board of education. He is right-hand dominant. He has no prior history of medical conditions, except he was involved in a motor vehicle accident in June 2005, when he sustained a trauma to his cervical spine and was diagnosed as having a mild C5-6 bulge, for which he only had axial cervical spine pain with conservative management for four weeks, following which there was a basic complete resolution of his condition. At the time of his compensable accident of June 2012, he was not having any ongoing neck and/or back pain; he was not treating for any spinal or shoulder condition; and had no limitations performing the essential functions of his job duties. On June 1, 2012, he was descending a 12-foot ladder during the course of his employment. Approximately half-way down, he lost his footing on the ladder and started falling directly downward. He reached upward with his right upper extremity (he is right-hand dominant), and grabbed onto a rung which forcibly pulled his entire right upper extremity and right shoulder in a sudden and forceful way, causing him to twist and lose his grasp, after which he fell in a somewhat horizontal fashion onto his right side, striking concrete, with his right arm outstretched to attempt to brace the fall, causing the head of his right humerus to jam into his shoulder, after sustaining direct trauma to his right hand, right wrist, and right elbow. He developed immediate severe pain in his right shoulder, beginning at the right side of his neck, radiating into his right trapezius/right triceps regions, with bruising and contusions of his right elbow and right wrist. He was taken to the emergency room. His neck, right shoulder, right elbow, and right hand were all imaged. The diagnostics were negative for fracture, but he was diagnosed as having a Grade 1 dislocation of his acromioclavicular joint. No CT scan or any MRI study was performed to any part of his body. His right upper extremity was immobilized, and he was referred for orthopedic management. The authorized orthopedist who saw him diagnosed “moderate sprain/strain of right shoulder with Grade 1 dislocation at AC joint.” He was immobilized for two weeks, and thereafter started on a course of eight weeks of physical therapy, during which time almost all of his physical therapy was designed towards decreasing pain in the shoulder joint itself, with increasing range of motion. Ultimately, he was discharged on October 1, 2012, to full duty, notwithstanding that the discharge office note states he is complaining of intermittent pain in the neck, right shoulder, radiation into his right triceps, with a VAS 3/10 average pain. He was advised to minimize overhead reaching and overhead lifting, and to return if there was any “significant” change in symptomatology. He was assured by the orthopedist that the pain would subside “after a while,” but that it could take “up to a year” to “fully heal.” He was evaluated by the permanency physicians on February 15, 2013. His evaluating physician found 35% permanent partial total referable to the right shoulder; 15% with respect to
2
the cervical spine (the physician found some spasm in the right-sided cervical spine, with some limitation with bilateral rotational range of motion). The physician found no permanency for “resolved elbow and wrist contusions.”
Respondent’s evaluating physician found no objective evidence of permanent orthopedic disability with any of the Petitioner’s injuries, with the only diagnosis representing a “minor” right shoulder “sprain and strain,” with subjective complaints disproportionate to objective findings.
You may assume that the matter has come up for pretrial conference, at which time the
Petitioner had credible complaints of right-sided cervical pain, primarily in the lower cervical region, with radiation to the right trapezius, with general radiation into the right shoulder joint itself, with impingement type of pain on abduction at 90 degrees, forward flexion 150 degrees, and extension limited to 35 degrees. The Petitioner’s overhead lifting was self-restricted to not greater than 40 pounds (prior to this accident, he could lift more than 100 pounds overhead utilizing both arms). The Petitioner limited the amount he could repetitively reach overhead without weight and the amount he would push and pull with his right upper extremity because of pain, primarily in the right shoulder region, but also, secondarily, the right side of his neck. He conceded that his right wrist pain had resolved, as had his right elbow pain. He described “occasional sleep interference” (approximately four nights per week), where he would have some difficulty getting to sleep and staying asleep with respect to primarily right shoulder pain. He would take over-the-counter Tylenol or Advil approximately four days per week (mostly work days), one 200 mg. tablet in the morning and one in the evening. He was able to perform the essential functions of his job duties. However, anything that involved any significant exertion or repetitive exertion of his right upper extremity was painful (both the right side of his neck and in his shoulder joint, with radiation into the triceps region).
The physical therapy notes do confirm the locations of pain which the Petitioner
described, and the physical therapist’s diagnoses included right shoulder, first degree AC separation with right-sided cervical pain.
The Petitioner has not undergone any MRI study of either his neck or shoulder, nor has
any further diagnostic study (such as a CT scan) been performed.
A. What is the value of this case? Assume that the parties had agreed to a 12½% permanent partial total award confined
solely to the right shoulder sprain and strain, with first-degree AC separation, with the award “silent” as to any cervical spine disability (meaning that any disability was neither “ruled in” nor “ruled out” for re-opening purposes).
The Petitioner then re-opens his claim and ultimately obtains an authorized MRI study on
November 1, 2013, demonstrating full thickness rotator cuff tear; SLAP tear; subacromial bursitis; first-degree AC separation; with moderate glenohumeral osteoarthritis. The proximal biceps is partially torn/frayed.
3
On February 1, 2014, the Petitioner undergoes a mini open rotator cuff repair; SLAP repair; acromioplasty with distal clavicle excision. Surgery does not significantly improve the Petitioner’s overall condition. In fact, the Petitioner has greater symptomatology following the surgery than prior thereto. He fails undergoing meaningful physical therapy rehabilitation, and ultimately he is diagnosed as having moderately severe adhesive capsulitis for which he undergoes May 1, 2014, lysis of adhesions, with a subsequent July 1, 2014, MRI study demonstrating small recurrent partial thickness rotator cuff tear, with moderate osteoarthritis throughout the shoulder joint. No further treatment is recommended, either on a surgical basis or on a pain management basis.
He then undergoes a functional capacity evaluation concluding that he is capable of
performing “medium duty employment,” with no repetitive overhead lifting, with no lifting to the chest level with his right arm beyond 40 pounds, with occasional pushing and pulling not greater than 25 pounds. The Petitioner is able to perform the essential functions of his job duties with modifications and reasonable accommodations regarding the same. He is worried about maintaining his employment due to his restrictions. He does not feel that he could resume this type of employment if he were to be terminated. His primary care physician has diagnosed him as having mild anxiety/depression regarding his “chronic pain” and “limitations.”
The Petitioner’s overall functionality has now significantly deteriorated. Abduction is
now limited to 70 degrees, and extension is now limited to 20 degrees. He has inadequate extension to put his wallet in his right back pocket. He now keeps it on his left side. The Petitioner describes his typical pain in his shoulder joint at 7/10, with occasional spiking to 10/10. He is now taking triple his former dosage of Tylenol and Advil. His sleep is significantly interrupted. Normally, he does not get more than four hours of sound sleep at night. He has been prescribed Ambien by his PCP, but he discontinued it because of side effects.
The same evaluating physicians are utilized. His evaluating physician finds an increase
of 40% permanent partial total “over the award.” Respondent’s evaluating physician concedes the existence of 7½% permanent partial total solely related to the Petitioner’s shoulder. The Petitioner’s evaluating physician finds no change in the cervical spine, but suggests that the Petitioner “may have a radicular component” and a cervical MRI study “is advised.” No additional treatment is sought. No psychiatric claim is pursued.
B. What is the value of this case at this point?
Assume all of the above facts except now the Petitioner is no longer capable of performing the essential functions of his job duties with or without accommodation and resigns because he feels the job is simply “too much” for him. He is now working as a custodian for a private employer (his neighbor for the past 10 years) performing “light maintenance duty” at $15.00 per hour, eight hours per day, five days per week.
C. How, if at all, does this one single fact change your opinion as to the permanency value of this claim?
4
Assume all of the same facts as in example B, where the Petitioner has undergone two
surgical interventions, but is still working for the same employer, but has not yet had his second permanency entitlement addressed. Assume after he completes the aforementioned treatment with respect to the right shoulder, it is ultimately determined that he needs to undergo an authorized cervical MRI study, which is performed, and confirms a large right-sided C5-6 herniation with “moderate nerve root compression.” The Petitioner is referred to an authorized neurosurgeon for further assessment, who concludes that the Petitioner is not a surgical candidate (reasons not explained), but has him undergo a formal course of physical therapy with trigger point/epidural injections for his diagnosis of moderate right herniated nucleus pulposus, with right-sided radiculitis. The evaluating physicians have the same shoulder assessments, but the Petitioner’s evaluating physician now has an increase to 40% permanent partial total with respect to the cervical spine, whereas the Respondent’s evaluating physician finds no cervical increase, as the cervical condition is simply “progressive” and related to the pre-existing motor vehicle accident, for which a “mild bulge” was previously diagnosed. There was no workers’ compensation award regarding his prior claim. You may further assume that the Petitioner’s specific cervical complaints have increased moderately since the previous hearing. His range of motion has decreased with bilateral rotation, and also has some pain on extension, with a more pronounced cervical radiation of pain into his triceps region, with occasional numbness in his right hand, and tingling in his fingers “on occasion.”
D. What is the value of this case, assuming he maintains his employment with his first employer (with pain)? What is the value of this claim, assuming he can no longer perform the essential functions of his job duties, and he is limited to the additional employment as described in Part B (working in a lighter custodial position at $15.00 per hour on a full-time basis)?
Finally, assume that the authorized neurosurgeon decides that the C5-6 disc herniation is a surgical lesion and proceeds to perform a C5-6 microdiscectomy, which does not significantly change the Petitioner’s cervical complaints or range of motion, but does impact the radiation of pain into his triceps and hand. Assume that the Respondent’s evaluating physician finds compensable cervical disability in the amount of 7 1/2% ppt “mostly” due to the progressive worsening of the “pre-existing” condition apportioned 2½% compensable/5% pre-existing.
E. What is the value of this case, assuming the Petitioner maintains his employment with his first employer (with pain)?
F. What is the value of this claim, assuming he can no longer perform the essential
functions of his job duties and he is limited to the additional employment as described in Part B (working in a lighter duty position at $15.00 per hour on a full-time basis).
5
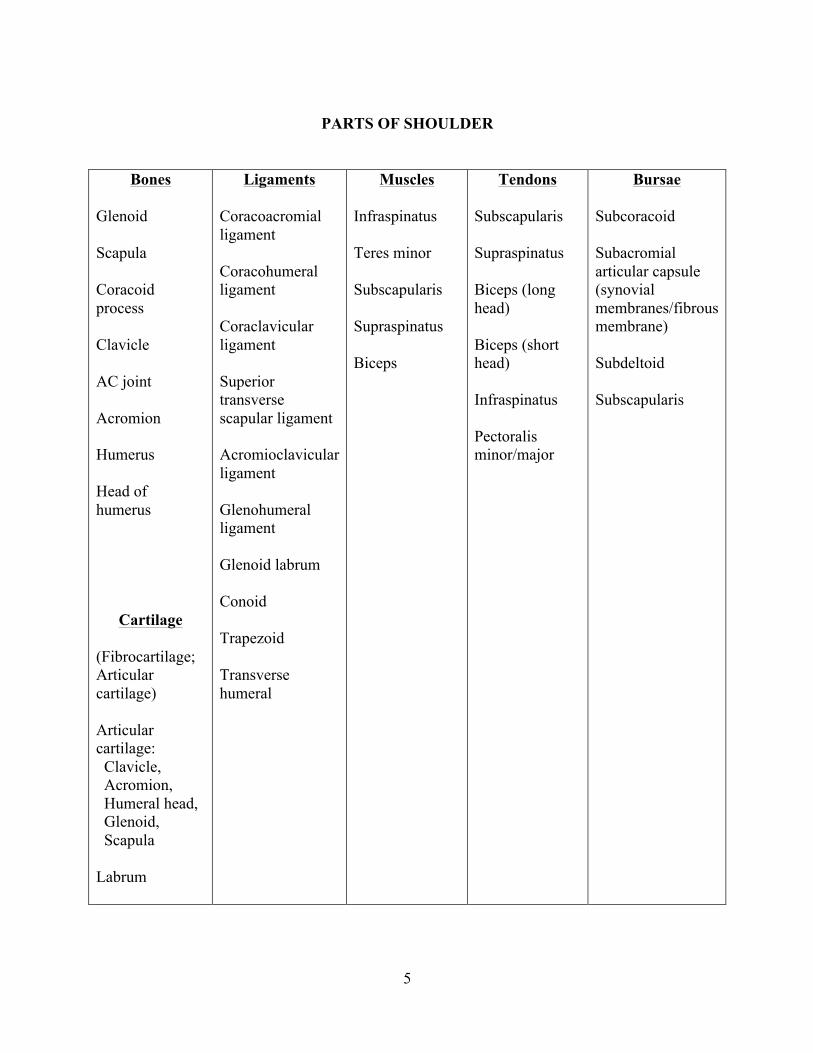
PARTS OF SHOULDER
Bones Glenoid Scapula Coracoid process Clavicle AC joint Acromion Humerus Head of humerus
Cartilage (Fibrocartilage; Articular cartilage) Articular cartilage: Clavicle, Acromion, Humeral head, Glenoid, Scapula Labrum
Ligaments Coracoacromial ligament Coracohumeral ligament Coraclavicular ligament Superior transverse scapular ligament Acromioclavicular ligament Glenohumeral ligament Glenoid labrum Conoid Trapezoid Transverse humeral
Muscles Infraspinatus Teres minor Subscapularis Supraspinatus Biceps
Tendons Subscapularis Supraspinatus Biceps (long head) Biceps (short head) Infraspinatus Pectoralis minor/major
Bursae Subcoracoid Subacromial articular capsule (synovial membranes/fibrous membrane) Subdeltoid Subscapularis
6
Shoulder 1. The rotator cuff is comprised of what four muscles?
a. Teres minor/infraspinatus/subscapularis/supraspinatus b. Deltoid/subscapularis/infraspinatus/supraspinatus c. Deltoid/teres minor/infraspinatus/supraspinatus d. Subscapularis/supraspinatus/infraspinatus/trapezius e. Teres minor/infraspinatus/biceps/supraspinatus
2. The labrum is: a. A cuff of thick cartilage encircling the glenoid that makes the shoulder socket deeper
and therefore the shoulder joint more stable than it otherwise would be b. A ligament which connects the acromion to the clavicle c. Articular cartilage that covers the head of the humerus that is similar to the articular
cartilage of the head of the femur d. A two-part tendon that connects the long head and small head of the biceps to the
humerus e. A capsule that envelopes the supraspinatus tendon which provides lubrication for the
shoulder joint. 3. A SLAP tear is a:
a. The least common labral tear b. A tear of the labrum that most commonly occurs with shoulder dislocations c. A tear of the labrum that is most commonly diagnosed by clinical examination rather
than MRI testing d. A tear of the labrum at its most lowest location in the shoulder joint e. A tear of the labrum with the long head biceps tendon anchors to the labrum
4. True or False: The shoulder is by far the human body’s joint with the greatest range of
motion.
5. True or False: There are three main bones which comprise the shoulder joint.
6. True or False: The three glenohumeral ligaments are the ligaments most responsible for providing stability in the shoulder by connecting the glenoid to the humeral head.
7. True or False: A shoulder sprain is usually more serious than a shoulder strain.
8. True or False: A grade 2 strain is usually less serious than a grade 3 sprain.
7
9. A shoulder sprain is an injury to (a) ligament; (b) tendon; (c) muscle; (d) all of above
10. A shoulder strain is an injury to (a) muscle, (b) ligament, (c) tendon, (d) muscle or
tendon; (e) all of above.
11. True or False: The shoulder consists of three main joints.
12. The most important joint of the shoulder is (a) glenohumeral; (b) acromioclavicular; (c) AC/humeral; (d) rotator cuff.
13. True or False: The glenohumeral joint is the least stable joint in the body.
14. True or False: The glenohumeral joint is the most mobile joint in the body.
15. True or False: The shoulder cartilage is very vascular and therefore heals better than if it was avascular
16. True or False: The shoulder bone is very vascular and therefore heals better than if it was avascular
8
Low back The Petitioner was born in February 1975. She is 5’2” and weighs 210 pounds. She has been married for 20 years. She has three children, ages 20, 16, and 12. Her husband is disabled. with failed low back surgery and is receiving Social Security disability. She is employed as a casino housekeeper. She has an eighth grade education. She is a mono-lingual Latina, having been born in San Juan. She came to the United States in 1995, and has been employed for the last 15 years as Respondent’s casino housekeeper. She had no prior medical history, other than chronic low back pain over the past year (with no prior MRI study, no CT scan, and no radicular complaints). She has had intermittent chiropractic management of her low back over the past 10 years, with a probable average of anywhere between three to five adjustments on a yearly basis. She has had a few minor non-compensable/no-lost-time exacerbations of back pain during the course of her employment for the Respondent, for which no formal claim petitions were ever filed. By all accounts, she is a very credible hard-working individual. She is the sole “breadwinner” for her family. She suffers a compensable accident on March 1, 2010, at which time she is earning $500.00 per week. She is pushing a housecleaning cart while flexed forward at her waist, at which time she develops a severe onset of low back pain, causing her to drop to her knees. She is immediately taken to the nurse’s station. She is then transported to the emergency room of the local hospital, at which time she is diagnosed as having a “severe lumbosacral strain and sprain,” and she is prescribed anti-inflammatories and taken out of work for five days pending “orthopedic assessment.” She is referred by the Respondent to the in-house physician, who has her rest for a week and then commences a course of physical therapy for two weeks, which must be discontinued because of increased low back pain, which she describes as “unbearable.” During the interim, she is referred to “modified” duty employment, which basically involves sitting in a laundry room folding towels for the laundry department. She is having difficulty sitting for more than an hour. Her employer otherwise accommodates this problem by allowing her to stand or sit at her leisure. She is on Percocet. Her physical therapy is discontinued. She is prescribed muscle relaxants and narcotic pain medications and is permitted to continue employment at modified duty with no lifting greater than 10 pounds. The authorized physician discusses with her a referral to a pain management physician for “injection” modalities, but the Petitioner declines to consider the same because she is extremely fearful of any type of injections or possible low back surgery because of her husband developing a severe infection following his injection modalities for his back, which led to failed back surgery, which in turn led him to his present disability status. This is the first time in the Petitioner’s life that she has not been able to self-manage her rehabilitation to the point where she would be able to resume her normal course of employment in a relatively short period of time.
9
She is finally seen by an orthopedic surgeon as of May 15, 2010, who diagnoses severe low back sprain/mechanical/axial lumbar pain, and further recommends a pain management “assessment” for consideration of epidural/transforaminal injections, and such other “modalities” as a specialist would recommend. He concludes that “no MRI is necessary because the Petitioner does not have any clinical evidence of radiculopathy.”
The Petitioner is extremely fearful of considering any type of injection modalities and,
once again, she declines to undergo the same. The in-house physician therefore concludes that she has reached “maximum medical improvement,” and the Respondent advises that if she cannot return to perform her “full duties,” she will have to be “terminated.” She has not undergone any FCE, and therefore she resumes employment with the intent to resume her “full duties.” Fortunately, she is well-liked by her supervisor and co-workers, even though she is required to clean 12 rooms on a typical shift by herself. She describes her chronic low back pain as 5/10. She is taking over-the-counter strength Advil and Tylenol, two tablets in the morning and two tablets in the afternoon, plus wearing a brace to allow her to remain functional at work. She is also obtaining “some assistance” doing her job by either her supervisor or some co-workers on especially bad days where she has to do more bending and lifting. She does get “some assistance” with lifting of mattresses and anything which is “unusually” exertional. Her back pain continues to be primarily axial in nature. There is no clear chronic radicular symptomatology other than occasional more left than right radiation with pain to almost knee level, but not beyond. She avoids lifting more than 15 pounds. She is sedentary outside of work. She cannot sit more than 30 minutes without significant stiffness and, at times, spasm in her low back. She will walk approximately three to four blocks. Her symptoms remain relatively chronic. Sometimes, it is difficult for her to stand fully erect at work, but she is a very loyal and committed employee, and continues working with more frequent chiropractic adjustments at this point in time. She sleep is significantly interrupted. She is not sleeping more than three to four hours per night maximum because of significant back pain. She used to sleep on her stomach. She cannot sleep on her stomach anymore without her back going into great spasm. Each night, it seems to be a different type of an adjustment with pillows being propped in a position so that she can limit the amount of stress placed on her low back. Some nights, she does not even sleep in her bed, but rather will lie in a recliner with an adjusted back.
No further treatment is sought. Her evaluating physician (report dated November 10,
2010) finds 45% permanent partial total for a severe low back strain/sprain, with “mechanical back pain” with the “possibility of herniated pulposus not ruled out.” Respondent’s evaluating physician (report dated November 11, 2010) finds 2½% permanent partial total “regardless of cause,” and concludes that the Petitioner has a longstanding “progression” of lumbar pain with the compensable component merely representing a “minor” low back strain, which “fully resolved” upon her resumption of full-time employment to her “pre-injury” baseline.
A. What is the value of this claim based on the above? (Value should be “actual
value” from the perspective of a Judge of Workers Compensation hearing these facts.)
10
Assume the same facts as above, but the Petitioner is terminated from this employment
because she cannot perform the essential functions of her job duties because she has a permanent lifting restriction of not greater than 10 pounds. The Petitioner is presently on unemployment compensation and is “seeking employment.” She feels that she would be able to find some type of employment because she has a log of contacts, but she does not feel she will be able to resume housekeeping.
B. What is the value of this claim, given this change of fact? Consider the same facts as above (per “A” - i.e., the Petitioner has continued employment
with Respondent), except that instead of resolving her claim for permanency following her orthopedic assessment, she is instead referred to a neurosurgeon on an authorized basis, who has her undergo a low back MRI study, which is positive for degenerative disc disease at L2 through S1, moderately severe at all levels, with a central protrusion at L4-5 and a central herniation at L5-S1, with moderately severe stenosis at both levels. However, the neurosurgeon finds a positive straight leg-raising, both in the sitting and supine position, with bilateral positive findings at 60 degrees.
The neurosurgeon recommends a provocative discography to better assess the source of
the Petitioner’s disc pain generators, but the Petitioner declines because she is not only afraid of the injection modality in and of itself, but she is adamantly opposed to considering surgery in view of what has happened to her husband. Consequently, she then returns to full-duty employment, but on December 10, 2010, she suffers a slip-and-fall on a wet bathroom floor at the same Respondent. She falls and twists onto her right side with a severe onset of low back pain (VAS 10/10), causing her to immediately be transported to the emergency room with progressively worsening radicular pain down each of her lower extremities. She returns to the original authorized neurosurgeon, who now has her undergo a further MRI study, which demonstrates a full-blown right-sided disc herniation at L4-5 with significant nerve root compression, and a significant left-sided herniation at L5-S1 with extrusion and nerve root compression. The neurosurgeon recommends a two-level instrumented fusion at L4 through S1. This recommendation terrifies the Petitioner. She seeks a “second opinion,” which is authorized. The second neurosurgeon agrees with the first, except that the nurse case manager discusses the Petitioner’s “prognosis” with the physician and urges a consideration of possible pain management injections as an “interim” modality, notwithstanding that as of this point in time the Petitioner has not only significant radiculopathy bilaterally, but she has developed a left-sided foot drop. The neurosurgeon has suggested that injection modalities “would not hurt,” but would not resolve the severity of the Petitioner’s bilateral nerve root compression, and that the delay in surgical decompression could compromise outcome.
At this point, the Petitioner develops a significant anxiety to the point where she is
developing chest pain, palpitations, and inability to sleep at night because she is worrying so much about her potential inability to support her family, and a possible surgical outcome similar to her husband’s. Her primary care physician refers her to a psychiatrist. She does not seek psychiatric treatment from the workers’ compensation insurance carrier. The psychiatrist who
11
sees her diagnoses a severe anxiety, with features of depression, and offers anti-anxiety psychotropics. She reluctantly undergoes a series of three epidural injections, which provide no relief. Her condition continues to worsen. She continues to receive temporary disability benefits following the second accident.
She returns back to the neurosurgeon following her three failed injections, and he advises
that her “only options” are to live with her present pain (with no resumption of employment because she cannot possibly perform the essential functions of her job duties), or undergo the recommended two-level fusion surgery to “stabilize” her spine, which “hopefully” will decrease her bilateral lower extremity pain and “improve” her left foot drop.
The Petitioner consults with her treating psychiatrist, who makes no specific
neurosurgical treatment suggestions, but ultimately the Petitioner feels that she is in a “desperate” situation and she has “no choice” but to undergo the surgery. Accordingly, she undergoes the L4-S1 instrumented fusion surgery with neurosurgeon No. 2, and develops a post-operative infection requiring a six-week IV PICC line for osteomyelitis, staph infection with sepsis complication, with a differential diagnosis of arachnoiditis. Following her infection treatment, she undergoes post-surgical rehabilitation with five additional pain management injection modalities, inclusive of radiofrequency lesioning at L4 through S1.
While her surgery ultimately was successful in terms of ameliorating the foot drop to
some extent and reducing her bilateral radiculopathy symptoms, the surgery did nothing to address her chronic and severe low back pain and, in fact, her range of motion functionality in terms of lifting is even more compromised following the surgery. She continues to have bilateral radiculopathy, with bilateral numbness in her feet, but the severity of the radiculopathy is somewhat improved compared to her immediate pre-surgical presentation.
Following the conclusion of her injection modalities, she undergoes yet another CT scan
which demonstrates “pseudoarthrosis L5-S1,” but there is no recommendation for any re-instrumented fusion. She undergoes an FCE, which gives her a permanent lifting restriction of no greater than 10 pounds, and consequently she is terminated because she is incapable of performing the essential functions of her job duties. She had not even been permitted to resume modified duty following the last compensable accident of December 10, 2010.
In the interim, she stopped treating with the psychiatrist, but continued with the anti-
anxiety medication. Since she stopped working, she loses her medical coverage. She is in a desperate financial situation. Her workers’ compensation lawyer advises her that if she seeks an award for permanent total disability, it will take at least nine months, and there is no guarantee she will be entitled to the same. This only increases her stress and she speaks to a neighbor who is a fellow church member, who owns a small housecleaning service. The neighbor employs the Petitioner on a part-time basis (15-20 hours per week, five hours per day, at $15.00 per hour) as a “supervisor” for two of her crews, which involve mostly Spanish-speaking employees. This is a somewhat “sheltered” situation in that the Petitioner is not expected to do any significant “hands-on” cleaning, but the owner wants to make certain that the crews are working to their optimal capacity. The Petitioner feels that this has been a “God-send,” and feels that she will be able to maintain at least this level of employment and hopes that if she “does a real good job,” she may
12
be able to perform this position for 40 hours per week if the business progresses. It is her intention to try to continue with employment “as long as my back holds out.”
Assume that the two claims remain pending. The Petitioner’s evaluating physician is
now 75% permanent partial total for the low back, 40% neurologically, 40% for anxiety, 25% for depression, with the Petitioner being “possibly unemployable” but for her “sheltered employment.” The Respondent’s evaluating physician finds overall 10% orthopedically for the spinal condition “regardless of cause” with no apportionment with the neurologic component representing 2½%, and psychiatric 2½% permanent partial total on an “unrelated” basis due to “pre-existing hysterical characterological disorder.”
C. What is the value of these two claims (assume wage is the same for each claim -
$500.00 per week)? Consider the same fact pattern, except a few days prior to the pretrial conference, the Petitioner loses her part-time employment after one year because the job was simply “too much.” She has not had any new accidents or injuries. She returns to her authorized neurosurgeon, who has a further MRI study with CT scan, which demonstrate further “degenerative changes,” significant “osteoarthritis” with increasing canal and bilateral foraminal stenosis at L2-S1, with a new disc protrusion at L3-4, representing “possible adjacent disc disorder,” but the neurosurgeon does not recommend any further treatment. She returns to the authorized pain management physician, who concludes that there is nothing further which can be done because the previous pain management modalities were ineffective. You may also assume that there has been a conclusion by the Petitioner’s evaluating physicians that overall the Petitioner is permanently and totally disabled and/or unemployable as a result of the two compensable accidents and that she’s now receiving SSD. You may further assume that the prior medical history varies slightly at this point with a 1997 low back MRI demonstrating moderate size disc bulge at L4-5 and L5-S1, with 1996 primary care physician history of referral to psychiatrist for depression due to “difficulties coping” with adjustment challenges in the United States with respect to finding adequate employment and language barrier.” There is further reference to further depression with respect to her responses to disability, which manifests itself in 2007. There is a Second Injury Fund pending.
D. What is the value of these two claims (inclusive of any potential SIF liability)?
13
Low back – quick values Assume “average results” for the “average” person with “expected” residuals. Give your best “average” number, recognizing that there is probably a general “range” of reasonableness for a person who is a 40-year-old (a) construction laborer, (b) nurse (in an orthopedic surgical unit), or (c) teacher (in a relatively sedentary position).
1. Low back strain/”normal” MRI/six weeks lost time/no radiculopathies/complains of mild intermittent axial back pain.
(a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
2. Low back strain/MRI moderate concentric disc bulge L5-S1/10 weeks lost time/no
radiculopathy with mild intermittent axial back pain. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
3. Strain with moderate concentric disc bulges L4-S1/10 weeks of lost time/two epidural
injections with moderate relief, with mild intermittent back pain. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
4. Low back strain/MRI L4-5/moderate left-sided disc protrusion with 10 weeks of lost
time/two epidural injections (with minimal relief), with moderate left-sided intermittent radiculopathy.
(a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
5. Low back strain with MRI L4-S5 moderate left-sided protrusion with L5-S1 left
moderate herniation, with 20 weeks of lost time, three transforaminal injections with moderate left-sided radiculopathy, with no surgical recommendation unless the Petitioner’s symptoms worsen to severe pain presentation.
(a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
6. Low back strain/MRI L4-S1 left-sided central herniations, status post bilateral
laminectomies/discectomies L4-S1 without radiculopathy. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
14
7. Low back strain/MRI L4-S1 left-sided central herniations, status post bilateral laminectomies/discectomies L4-S1 with radiculopathy.
(a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
8. L4-5 disc herniations status post failed pain management modalities with L4-S5
instrumented fusion without radiculopathy, with moderate chronic axial pain. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
9. L4-5 disc herniations status post failed pain management modalities with L4-S5
instrumented fusion with radiculopathy, with moderate chronic axial pain. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
10. L4-S1 instrumented fusion without radiculopathy.
(a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
11. L4-S1 instrumented fusion with radiculopathy.
(a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
12. L4-S1 compensable instrumented fusion with radiculopathy, with prior L4-S5 disc
bulge diagnosed three years prior, with occasional chiropractic management. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
13. L4-S1 instrumented fusion with radiculopathy, with three years prior L4-5 disc
herniation without radiculopathy, with no surgical recommendation. (a) Construction laborer (b) Nurse (in an orthopedic surgical unit) (c) Teacher (in a relatively sedentary position)
15
Cervical spine The Petitioner was born on July 7, 1958. He is 47 years of age. He is 6’2” and weighs 210 pounds. He is married with two children in college and two in high school. He was involved in a compensable motor vehicle accident on July 1, 2010. He was earning $2,000.00 per week, with maximum temporary disability benefit rate. He had worked for 20 years for this Respondent as an interstate tractor trailer driver. The accident was caused when he was struck head-on by a vehicle coming in the opposite direction and traveling at 50 miles per hour while attempting to pass another vehicle. This was a very serious accident. The driver of the other vehicle was killed. The Petitioner sustained a significant traumatic brain injury and was in a coma for two days. He had a significant post-concussion disorder, but did not receive any long-term cognitive treatment. He also had three cervical spine disc herniations (C3-6), for which he had a failed C3-6 fusion with pseudoarthrosis at C5-6, with failed post-surgical pain management modalities, with two years of temporary disability benefits paid through July 1, 2012.
There had been a recommendation for re-fusion of the cervical spine, but the Petitioner had lost confidence in the authorized surgeon, and therefore refused any additional surgery. He had chronic bilateral cervical spine pain, together with radiation into both of his upper extremities (with equal paresthesias in both hands), with chronic and severe cervical spine headaches running from the cervical spine to the occipital region of his skull into both temporal regions. He also had frontal headaches, which were separate and distinct in nature, with severe pain behind both of his eyes, which were described as “migraine-like,” occurring daily and lasting generally one to two hours. He never had any type of pre-existing headaches of any nature. He had continued with his commercial driver’s license, but was unable to continue with his existing employment with the Respondent because the employer felt that he was too much of a “risk.” Accordingly, he filed an ADA claim that was pending against his former employer. He also received a third party settlement for $750,000.00, for which there is no ongoing Section 40 lien.
The Petitioner was working part-time as a driver (approximately 20-30 hours per week
for the last six months) at less than half of the income he had previously earned. The Petitioner felt he could work “full time” “driving only” if he could find a “suitable situation.” The Petitioner’s evaluating doctor finds 66-2/3% ppt cervical, and 33-1/3% post-concussion disorder. The Respondent’s evaluating doctor finds 12½% ppt cervical, and 2½% post-concussion disorder.
A. What is the value of this claim?
The Petitioner then files an Application for Review or Modification and obtained a
further authorized neurosurgical opinion that he needed decompressive spinal surgery to address his pseudoarthrosis at C4-6, and needed a complete “re-do” at C4-6, together with now having an unoperated protruding disc at C6-7.
16
The Petitioner undergoes the recommended surgery on an authorized basis, which in turn has a 50% improvement on overall clinical functionality in terms of his bilateral radicular symptoms. There is also significant reduction of the chronic headache presentation. However, the trade-off has been a significant deterioration of his range of motion in almost all cervical spine spheres, together with a serious swallowing problem which developed post-surgery, for which there was no definitive diagnosis in terms of any type of esophageal or larynx injury, either at the time of the surgery itself or intubation in connection with the surgery. However, the problem is clearly documented throughout the medical record and, accordingly, the Petitioner has had a major alteration in his diet in terms of the manner in which he eats food, the quantity which he eats, and the amount of fluid that he must swallow with every meal.
In the meantime, however, he successfully pursues his ADA claim and is actually
reinstated in his former employment as part of the legal recovery. The Petitioner’s lifestyle outside of work is completely sedentary at this point in time. He is capable of performing the essential functions of his job duties. However, he takes 2400 mg. of Ibuprofen on a daily basis, together with Flexeril and hydrocodone on weekends when he is not working. The Petitioner has primarily tried to address his overall range of cervical motion which is challenging his ability to maintain employment. He has been able to pass both the physical and mental requirements for the continued CDL, but he feels that without his long-term experience, he would not be able to maintain this employment. He is able to create an ergonomically adequate environment in the cab that he utilizes every day. There is a special adjustment at the top of his seat that allows for his cervical spine to be slightly extended, but be braced in a manner that relieves pressure on his impaired cervical vertebrae.
The Petitioner’s evaluating physician finds a 50% orthopedic/neurologic increase solely
regarding the cervical condition. The Respondent’s evaluating physician finds a 0% increase and concludes that the Petitioner’s condition is actually “improved” on an overall clinical basis, but does not change his estimate.
You may assume that the Petitioner also has significant cracking and grinding sensation
in almost all spheres of motion. He now wears a cervical brace any time he is driving more than one hour, which is typically five days per week. He is now driving less than he was before. This has just been a result of an alteration of his routes rather than any type of “accommodation” which is being provided to the Petitioner.
You may further assume that there are no additional lien credits or third party recovery. B. What is the value of the Petitioner’s partial disability award (assume the original
award was 50% ppt (40% cervical; 10% concussion)?
C. Would you consider a Section 20 settlement and, if so, what would be the amount and why?
17
Multiple injuries
The Petitioner was born on September 15, 1980. He is 34 years of age. He is 5’10” and
weighs 180 pounds. He has been married for three years and has twin girls, one year of age. He has been an English teacher for a high school, which has been his employment during the past 10 years. He is an extraordinarily talented part-time musician, who is both a virtuoso guitarist and pianist, and performs part-time employments in various capacities to supplement his school teacher income anywhere between $25,000.00-50,000.00 per year by performing in various union bands, studio appearances in Philadelphia and New York, and Washington, D.C. song-writing and scoring opportunities. His only past history is that he has been an alcoholic for most of his adult life, but has been sober for the past five years, after having successfully participated in Alcoholic Anonymous for the past eight years.
He is right-hand dominant, although he is relatively ambidextrous, especially with respect
to most of his physical activities, other than “writing.” On October 1, 2013, he fell down a stairwell at school. He was earning $1,500.00 per
week at that time. He suffered a non-displaced fracture of left distal radius, a non-displaced fracture of the left distal phalanx of his fourth statutory finger; moderate left carpal tunnel/median nerve denervation un-operated with numbness and tingling in his palm, thumb and first two fingers (the Petitioner was too afraid to undergo the surgical decompression which was being recommended); a three-part comminuted non-displaced fracture of the left olecranon; a second-degree sprain/dislocation of the right thumb (status post closed reduction); a 30% compression fracture of his coccyx; with a similar compression fracture of his L3 vertebrae. He received six months of temporary disability with conservative management. However, during the six months of his temporary disability, he was completely incapable of playing either the piano or the guitar, during which time he developed a severe anxiety and returned to using alcohol, which has continued, but which is “more in control since he has resumed employment. He did not seek authorized psychiatric care, as he was fearful that he would “lose his job” if his employer were to find out the level of his anxiety. He sought active psychotherapy for three months with anti-anxiety medication. All of this represented unauthorized treatment due to what clinically was a compensable aggravation of his pre-existing psychiatric condition.
Once the Petitioner was capable of resuming employment, he continued to have chronic
pain with respect to all of the injuries in question. His left wrist was probably his biggest problem because his entire hand would become very easily fatigued, even with relatively modest repetitive stress. He was incapable of playing the keyboard of his piano and/or the fretboard of his guitar at anywhere near the level which he had performed pre-injury. In combination with the problem which he had with his left elbow (chronic pain on exertion with 10 degrees short of full extension and 10 degrees short of full flexion), and his right thumb (inability to oppose the thumb to his fourth finger, with loss of strength and chronic pain in the base of the thumb), he went from still being a “professional” guitar player and pianist at the top end of his craft to an “average” musician (with a reduction of income of at least 50% of what he had previously earned).
18
He had chronic low back pain, axial in nature (not radicular), VAS scale 5/10. He could only sit for 30 minutes without stiffness and spasm. His range of motion with respect to flexion was limited. He used to be able to touch his toes easily. He now can barely bend forward beyond halfway between his knees and feet.
He no longer engages in any sports at all for fear of re-injury. He had previously been an
avid runner, normally training at least 20 miles per week. He had participated in six marathons over the past three years. He now rides a stationary bike only, although he had planned to consider road biking, but has been far too fearful of possible re-injury to either of his upper extremities and/or his back, which he cannot “afford” to have happen.
At the present time, he continues to drink, but is in more “control.” His wife is not aware
of his enhanced drinking, but he feels that he is not “abusing” alcohol, but rather recognizing that he “needs” a “shot or two” normally before bedtime to “take the edge off” so that he can get a good night’s sleep. He is not taking any prescription medications, but he is taking three over-the-counter Advil or Tylenol every morning and every night, every day of the week.
His evaluating physician finds permanency in the amount of 50% of the left hand for his
left wrist and left finger injury. The doctor finds a bona fide reduction of range of motion in all spheres of the wrist by 20%, and range of motion deficit of the left finger of 50%. There is a clear carpal tunnel sensorineural presentation in the areas of the hand classically impacted by median nerve compression; 35% of the left arm for the fractured cuboid; range of motion deficits; tenderness and loss of strength (the Petitioner has at least a 20% loss of strength in terms of lifting with respect to the left hand strength and left arm strength); 35% of the right hand in view of the right thumb injury; 40% permanent partial total for the coccyx/L3 fractures.
The Respondent’s evaluating physician finds permanency in the amount of 5% of the left
hand; 5% of the left fourth finger; 7½% of the left arm; 15% of the right thumb; 7½% partial total with respect to the lumbar spine. The Petitioner’s evaluating psychiatrist finds 40% permanent partial total for anxiety/depression, of which 20% is pre-existing. Respondent’s evaluating physician finds 0% neuropsychiatric related (5% solely pre-existing.).
A. What is the value of this claim? B. Assume all of the above, except that the Respondent’s evaluating physician finds
7½% psychiatric disability, 5% pre-existing, and 2½% compensable. How does this affect overall value?
C. Assume the Part A set of facts, except that the Petitioner’s full-time position is
as a musician earning between $50,000-125,000.00 every year during the past five years, with the specific employer question earnings of $50,000.00, and the balance supplemented by his part-time teaching position, where he earns $35,000.00 per year. You may assume that the injury occurs when he is working as a substitute teacher, not as a musician. You may assume, as in Part B, the Respondent’s evaluating physician concedes compensable psychiatric permanency. How does this affect your opinion regarding permanency value?

19
Legs
The Petitioner was born on April 15, 1955. He is 60 years of age. She is 5’5”, weighs 200 pounds, and is married with a medical history of insulin-dependent diabetes for the past 30 years; diabetic retinal neuropathies last 10 years; non-compensable bilateral carpal tunnel decompression of January 10, 2003; chronic hypertension for the past 20 years; bipolar disorder, medicated the past 10 years; left knee arthroscopy (non-compensable), May 1, 2005 (partial medial meniscectomy); July 1, 2007, left lateral release; and Charcot-Marie-Tooth disease, with AFO bracing since diagnosed 15 years ago. It is within this background that the Petitioner suffers a compensable accident of February 1, 2008, when she falls on her left side exiting the bus (she has been a bus driver for the past 25 years). She was diagnosed as having a completely ruptured anterior cruciate ligament which required open repair, with allograft on February 2, 2008, with a chronic pain presentation. She was also diagnosed as having tarsal tunnel disorder, together with Achilles tendon rupture, which also required surgical repair.
Immediately prior to the accident of February 1, 2008, she continued to have some level of chronic pain with respect to her left leg and symptomatology in connection with her statutory foot associated with her Charcot-Marie-Tooth disease, which did require AFO bracing on a daily basis. She was also on Celebrex for her chronic left knee joint pain, which gave her relatively chronic discomfort in the area of a 2/10. She had some difficulty sitting for long periods of time with stiffness in the knee, and she would occasionally walk with a slight limp, and she did not wear high-heeled shoes. She was incapable of running, except for a very short distance, but did not require any type of orthopedic device. She was somewhat challenged going up and down stairs, and took a Celebrex tablet on a daily basis consistent with her primary care physician’s recommendation. She would occasionally wear a brace at work, but this was a relatively rare event (two times per month). She would experience knee swelling one or two times per month during a typical month.
She was out of work for almost a year and resumed employment February 1, 2009. She
was evaluated for permanency in May 2009 by both experts. Her expert found compensable disability of the left knee as 50% permanent partial total (overall greater), and 40% of the left foot (overall greater).
Respondent’s evaluating physician found compensable disability to the left knee as
representing 12½% of the leg, apportioned 7½% pre-existing, and 5% compensable, together with 7½% of the foot “solely related to the residuals of the unoperated tarsal tunnel and left Achilles repair.” Respondent’s expert also found “significant” pre-existing disability with respect to the two prior arthroscopic left knee repairs and the Petitioner’s Charcot-Marie-Tooth disease, primarily impacting the statutory foot.
The Petitioner was able to continue with employment following the compensable
accident, but she feels there is significant worsening of her pre-existing condition. Now, she has chronic pain in the knee on 6-7/10. Her left knee is “significantly” more unstable. She is very
20
“guarded” and “careful” with respect to any type of sudden movements or sudden stopping. Her knee is significantly swollen on a daily basis. Both evaluating physicians found a one-and-a-half-inch difference in circumference of the left knee versus the right (the Petitioner is left-handed and left leg dominant). The Petitioner can physically kneel, but never does so because of significant pain. She has difficulty performing a squatting maneuver, and can only squat half way down without assistance. The Petitioner has chronic pain in her foot, which is now more of a burning sensation, especially in the area where the surgery occurred, with an overall “weakness” of the foot, which feels “heavy” at times. Her foot will now occasionally drag. She cannot rise up on tip-toes on the left foot without support. She has a definite modest limp with respect to the left leg, and she has been altering her gait somewhat and placing much more weight-bearing on her right side. However, she is capable of performing the essential functions of her job duties, although she does so with pain. She cannot “afford” to not work. She has increased her Celebrex consumption by 50%, and she also supplements the same by over-the-counter medications on a daily basis.
A. What is the value of this claim?
Assume all of the above. The Petitioner then resumes employment and continues
working, but develops significant low back symptomatology following attempting to vacuum around the couch at home, at which time she was pushing the couch in a forward flexed position when she felt a “pop” in her low back with a severe radiation of pain down her left leg, resulting in a massive herniation at L5-S1, which required a microdiscectomy, performed on December 20, 2009.
She resumes employment on February 1, 2010, and on June 15, 2010, her left knee gives
way (it had been chronically unstable). While merely walking down the steps she falls, resulting in a comminuted fracture of the right patella, requiring a patellofemoral arthroplasty and subsequent thereto a right total knee replacement is performed in May 2012. All of this is treated as compensable. It can be assumed that following the low back surgical procedure, the Petitioner had resumed employment, but was having significant ongoing problems with her left knee, and also with radiating pain from the low back. The surgery initially helped the radicular symptomatology, but it returned much more pronounced and was giving the Petitioner significant ongoing symptomatology immediately prior to the derivative fall. In fact, she was then scheduled for further MRI study and EMG study to better assess the radicular complaints which she was experiencing.
Following the derivative fall of June 15, 2010, the Petitioner applied for and received
Social Security disability benefits. She was awarded an ordinary disability pension of $300.00 per week. Her wages at the time of the compensable accident of February 1, 2008, were $1,200.00 per week. At the time of the derivative fall, they were $1,250.00 per week.
Assume the comminuted fracture and the total knee replacement are both to the right leg.
21
You may also assume that the low back condition was further aggravated after the June 15, 2010, accident, with an L4-5 unoperated protrusion, with chronic L5-S1 radiculopathy, for which pain management only was recommended.
Prior to the compensable derivative fall of June 15, 2010, the Petitioner did receive an
award for her first claim in the amount of 40% permanent partial total, apportioned 45% of the left leg, credit for 25% pre-existing, and 42½% of the right foot, 20% pre-existing. You may further assume that a Second Injury Fund application is filed and that a formal Claim Petition is filed for the derivative accident, which bears a separate Claim Petition number.
The Second Injury Fund takes the position that the Petitioner is not permanently and
totally disabled but, if she is, the Respondent bears full responsibility because the condition as aggravated alone solely causes permanent total disability. The Second Injury Fund also argues that the bulk of the Petitioner’s low back disability cannot be considered as a Fund condition because it all happened after the date of the original accident, which is the controlling date for Fund liability, not the date of the derivative accident.
Respondent takes the position that Fund eligibility is determined from the disability
following the last derivative accident date (June 15, 2010), and not the date of the original accident (February 1, 2008).
The Petitioner’s attorney advises the Court that the Petitioner is “clearly” permanently
and totally disabled and so long as the Petitioner receives total disability benefits, the attorney does not really care whether or not the Fund pays.
The Petitioner’s evaluating physician finds that as a result of the “derivative”
compensable accident the Petitioner now has a 75% loss of function of the right leg, together with an overall disability of 50% permanent partial total with respect to the low back, apportioned 25% for the L5-S1 microdiscectomy, and 25% for the new unoperated disc herniation with increased radiculopathy. Respondent’s evaluating physicians finds disability in the amount of 15% of the right leg, and 10% permanent partial disability for the low back, 2½% compensable and 7½% pre-existing.
The Petitioner has not worked since the derivative fall of June 15, 2010. There is no
claim that her left leg has worsened. The Application for Review or Modification and the derivative claim solely seek additional compensation for the right leg and the low back condition. The Petitioner’s chronic low back pain with radiating pain in to the right lower extremity is now 7-8/10, with the Petitioner’s right knee complaints actually being worse than those with respect to her left. There is a burning sensation in the left knee joint that is “always” there. The right knee is not as swollen as the left, but she cannot kneel on the right knee at all. She has a four-wheeled walker that she uses “most of the time” when she has to go out. She rarely drives her car any longer, and only for short drives. She can only walk for a block or two at any given time because of both of her legs. She now has a significantly disrupted gait because of ongoing problems with both of her knees. She has gained 50 pounds since the derivative accident occurred. She is significantly depressed but, for some inexplicable reason, she has not been evaluated for psychiatric disability, despite the fact that she has been diagnosed as having
22
depression by her primary care physician, for which Wellbutrin has been prescribed. Her life is completely sedentary at this point in time. She will occasionally cook, but her husband does almost all of the “heavier” household chores, including the more significant cooking and all of the significant cleaning. The Petitioner has not worked in any capacity since the accident occurred, and Respondent has obtained videotape that demonstrates the Petitioner walking in a very guarded fashion after coming home from church service on a recent Sunday.
The Petitioner’s ability to sleep has been significantly impacted primarily because of her
back pain. She is now taking Oxycontin on a daily basis, together with Oxycodone. She cannot exercise. Her “pre-existing” mellitus, diabetic neuropathies, and Charcot-Marie-Tooth disease have all remained stable.
B. What is the value of this claim?
23
SECOND INJURY FUND This is a re-opening of a permanent partial disability claim, with a claim for Second Injury Fund liability, notwithstanding the occurrence of a subsequent partial total disability award.
The Petitioner was born January 10, 1955. He is 65 years of age. He is 5’10” and weighs 320 pounds. He has been married for 35 years and has two adult children. He has been morbidly obese for his entire life. He had been a very strong individual in his youth and after high school obtained a baseball scholarship and played on a professional baseball team for three years prior to suffering a career-ending injury when he was 23 years of age, involving three surgical interventions with respect to his left shoulder (non-dominant arm), inclusive of an eventual left shoulder replacement surgery. There was no compensation claim made in connection with that injury.
The Petitioner had been very well-known because his career-ending injury occurred as a result of a bench-clearing brawl after he charged the mound after three consecutive fast balls were thrown at his head by the opposing team’s pitcher, the third of which struck his left shoulder.
The Petitioner found employment as a corrections officer and worked for a New Jersey prison from January 1, 1980, through May 1, 2001. He was employed as a casino host from January 1, 2005, through December 1, 2013. He has not worked since December 1, 2013, as a result of a number of medical conditions which he alleges has cumulatively resulted in his being “permanently disabled.” He is receiving Social Security disability as of June 1, 2014.
He filed four separate compensation claims throughout his life. By way of significant background, the first was C.P. No. 98-1234, which involved a compensable accident of March 15, 1998, resulting in a severely comminuted displaced fracture of the right femur, requiring open reduction internal fixation with intramedullary rod, with 10-screw fixation, for which he received an Order Approving Settlement on February 5, 2001, in the amount of 40% of the right leg, strictly for the orthopedic and cosmetic residuals. He then suffered a non-compensable myocardial infarction on February 6, 2001, resulting in lifetime cardiovascular medication, with two separate angioplasties performed in 2007 and 2008.
His second compensable accident was May 1, 2001 (C.P. No. 2001-4321), for which he received an Order Approving Settlement on July 1, 2003, in the amount of 50% permanent partial total for the orthopedic and cosmetic residuals of the right hip labral tear status post arthroscopic repair with unoperated torn right medial meniscus, with moderately severe chronic right peroneal nerve injury, which award was apportioned approximately 20% permanent partial total for the right hip surgery, and 57½% of the right leg, credit 40% pre-existing for the right lower extremity pathology. In connection with this accident, the Petitioner was unable to continue the essential functions of his job duties, and therefore he was terminated. He received
24
an award of accidental disability pension amounting to approximately $650.00 per week for the disability portion of his award, with pension taking the offset.
Following the accident of May 1, 2001, the Petitioner’s uncle (who was an executive at a casino) helped him obtain a position at one of the casinos as a “host” for “player development.” This was a position where the Petitioner was to market the casino in certain gambling demographics (in this case, professional athletes), which was a “natural” for the Petitioner in view of his prior experience in Major League Baseball. He had always been involved with the MLB players’ union.
In the interim, he also underwent bilateral carpal tunnel decompression in November 2005 (non-compensable). While working for the casino, he suffered his third compensable accident of January 1, 2006 (just after midnight). He had slipped on champagne, which was spilled by a co-worker, resulting in his suffering two cervical herniated discs of significance at C5-7, with moderate spinal cord compression, with EMG evidence of cervical myelopathy (for which two-level instrumented fusion surgery was recommended, but declined by the Petitioner because of a “fear” of surgical outcome).
He also aggravated his previous right knee condition, for which a total knee replacement was recommended and, again, the Petitioner declined surgery because he was “afraid of outcome.” Additionally, there were a number of issues ongoing in his personal life that was causing him a great deal of stress, and he did not feel that he could “afford” to be out of work for an extended period of time.
On March 1, 2009, he received an Order Approving Settlement of 52% permanent partial total (C.P. No. 2006-3214), apportioned 15% for the cervical disability, and 66-2/3% for his right leg, with a 12d credit of 57½% of the leg for his pre-existing condition.
He then had his fourth compensable accident on May 1, 2009 (C.P. No. 2009-9876), resulting in a right shoulder scapular fracture, unoperated, with an unoperated right shoulder rotator cuff tear, with a fracture of the distal humerus of the right arm, with non-operated lateral epicondylitis, and un-operated biceps tear. He returned to work following the compensable accident on January 1, 2010. He received an Order Approving Settlement on May 1, 2011, in the amount of 30% permanent partial total, apportioned approximately 15% with respect to the right shoulder and 27½% with respect to the right arm.
He continued working for the casino until December 1, 2013, which was the last day he ever worked. At that time, he went out of work because his previous compensable cervical spine and right knee conditions were progressively worsening and authorized surgeries had been scheduled on December 2, 2013 (cervical spine – C5-7 fusion), and February 1, 2014 (right total knee replacement).
He received Social Security disability with an onset date of June 1, 2014. The above references his entire significant medical history. He also treats on an unauthorized basis for depression because of his “inability” to continue with any type of gainful employment. He had

25
always been a very vital individual and has not earned any money whatsoever since he stopped working at the casino.
His evaluating physician finds a 50% increase of the cervical spine pathology, primarily on the basis of the one-time two-level surgery, for which there was subsequent MRI evidence of pseudoarthrosis at C6-7 and adjacent disc herniation at C4-5, for which no surgery was deemed recommended. He had a significantly reduced range of motion in all spheres of his spine (30 degrees left and right cervical rotation; 10 degrees cervical extension; 20 degrees cervical flexion; 10 degrees cervical tilt bilaterally); with bilateral clinical evidence of radiculopathy in both upper extremities, but no further evidence of myelopathy. The Petitioner could no longer do any type of overhead work. His ability to sleep was significantly compromised. He was taking chronic pain medication both for his neck and left knee primarily, as his left knee replacement did not go particularly well either. There was a post-surgical infection, which required three months of intravenous antibiotic treatment, in addition to a 13-inch vertical scar above and below his knee. He experiences chronic swelling in the knee itself, with a complete inability to kneel or squat. He walks with a moderate antalgic gait, which was not evident before the surgery. He will occasionally use a cane to help his support because the knee feels unstable. He has gone to three different specialists, all of whom agree that he has a chronic pain disorder with respect to the leg, but there is nothing mechanically unsound with the knee replacement, and there is no need for further revision surgery. All of this has been very “depressing” for the Petitioner. His evaluating psychiatrist finds a 25% anxiety disorder with depression, for which he is taking both Xanax and Wellbutrin. The Petitioner’s evaluating physician finds a 50% increase with respect to his cervical spine, a 50% increase with respect to the right leg, and 25% neuropsychiatric disability referable to the Petitioner’s compensable disability. Both evaluating physicians conclude that the Petitioner is permanently and totally disabled. The Petitioner has undergone an FCE, which only allows him to perform completely sedentary employment with no lifting at all and no standing more than two hours.
The Respondent’s evaluating expert finds a 10% increase with respect to the cervical spine, a 15% increase with respect to the Petitioner’s right leg, and 2½% permanent partial disability with respect to a compensable depression referable to these two medical conditions. The Respondent’s expert agrees with the restrictions found by way of FCE. The Petitioner’s attorney files a Second Injury Fund application on the basis that the Petitioner is now permanently and totally disabled as a result of the “worsened” disability which he now has resulting from his next to last compensable accident of January 1, 2006. There is no Application for Review or Modification referable to the last compensable accident of May 1, 2009 (No. 09-9876).
The Respondent’s evaluating physician indicates in his report that the Petitioner will likely be challenged to resume sustained gainful employment as a result of “all of his medical conditions.”
In addition to finding permanent partial disability as above indicated, Respondent’s evaluating physician feels that the Petitioner is permanently and totally disabled not solely because of the accident of January 1, 2006, but as a result of the increased disability associated
26
with that accident and “all pre-existing medical conditions” which existed prior to January 1, 2006.
What is the value of this claim? How should the Second Injury Fund claim be resolved?