Embed Size (px)
Citation preview

1128
cases the crime for which the prisoner is convictedis not the cause of his going wrong and is not thecondition which requires treatment. For instance,women convicted of theft are often inebriates andonly steal to get money for drink. In the case of ayoung girl convicted of stealing, analysis showedthat the reason she had taken to theft was thatshe was in an uncongenial occupation. She wantedto be a pupil-teacher and ultimately become aschool-mistress, but her mother insisted on workin a factory. As the work was distasteful to hershe stayed away from it. As she required moneyand did not earn it, she stole from her parents,against whom she had a grudge. Imprisonment insuch cases would be disastrous ; the only chanceis a properly regulated life with change of occupa-tion and possibly some psycho-therapy as well.Anyone who has to deal with these young
criminals cannot help being struck by their extra-ordinary suggestibility ; they are just as open togood suggestions as to bad, and if only they can beplaced in proper surroundings their character canbe greatly influenced by suggestive treatment ofone kind or another.
I can give you no better illustration of theimportance of thorough medical investigation inthese criminal cases than a boy I saw since thispaper was written.A gentleman brought for my advice his son, as he
had been stealing, and no cause for this abnormalitycould be discovered. He was an intelligent well-set-upboy of 16, very keen on his training in farming, whichhe had just started. I found that for three years hehad been the victim of self-abuse, and in addition was ahystero-epileptic, and I suspected that true epilepsywas developing. He gave a clear account of momentaryforgetfulness, when he seemed to lose himself; heoften talked and even shouted in his sleep, had been asleep-walker, and on one occasion recently fell out ofbed during the night. I have put him on bromides andarsenic for a month, as I want to see the effectof medicinal treatment first ; if that is no use I
expect psycho-therapy will help him; it has greatpossibilities in hystero-epilepsy and even in incipientadolescent epilepsy. As the boy is leading a healthylife and has a good family record, the prognosis is fair.The self-abuse is an infantile complex which shouldbe dealt with as such, proper occupations being pro-vided, and ideals of development, manhood, and familylife being built up.
COnCl1.lSion.In conclusion, I should like to say I believe
psycho-therapy will furnish the explanation ofmany illnesses and diseases, and is a powerfulagent in relieving chronic pain, distress, andanxiety; it is also an important factor in promotingefficiency and in strengthening character.
V.A.D., SUSSEX 53.-Some interesting figureswere given at a gathering at Brighton on Dec. 3rd tocelebrate the end of the arduous war work of the Sussex 53Voluntary Aid Detachment, and the detachment’s settlingdown to peace conditions. During the war period no
fewer than 250 convoys arrived at Brighton containingjust over 38.000 sick and wounded, occupying the detach-ment 729 hours, or 91 eight-hour days. Service wasentirely voluntary, and Commandant C. G. Yates wasabsent on three occasions only. On orderly duty at the LadyGeorge Nevill, Larnach, and Red Cross hospitals, membersput in over 26,000 hours’ duty; and the detachment turnedout at the emergency stations fully equipped at all air-raidcalls, but, fortunately, were not needed. Tribute was paidto Mr. J. A. A. Orlebar, C.B., the medical officer of thedetachment, for his lectures, which were given gratuitously.Convoys of men broken in the war still arrive at Brightonat intervals of about a month, and are conveyed by thedetacbment to the Kitchener Hospital, Elm Grove, whilethe members still give attention to civilian cases whencalled upon.
HYSTERICAL SLEEPING ATTACKS :TREATMENT BY GROSS SUGGESTION, REINFORCED BY
THE OPERATION OF TREPHINING, WITH NOTESON BEHAVIOUR IN HYPNOTIC SLEEP.
BY HILDRED CARLILL, M.A., M.D. CANTAB.,M.R.C.P. LOND.,
SENIOR PHYSICIAN, WITH CHARGE OF OUT-PATIENTS, WESTMINSTERHOSPITAL ; ASSISTANT PHYSICIAN, WEST END HOSPITAL FOR
NERVOUS DISEASES ; PHYSICIAN, SEAMEN’S HOSPITAL,GREENWICH, ETC.
Hi.sto’J’!J of the case.-The patient, aged 19, wasadmitted to hospital in June, 1918, with a diagnosisof mental disease. He is a boy of average intel-ligence, and his home is in Lambeth. He is theeldest child of English parents, and he has five’brothers and two sisters, all of whom are well. Hismother is well. His father was killed in the war.His story was that since early childhood, for as longas he could remember, he had been liable to go offto sleep at any time and without any feeling offatigue, He had never been a week free from this.There is no history of fits in the patient, or in hisfamily. He does not walk in his sleep, and he isnever incontinent. Except for the sleeping attacks,which he is quite unable to resist, the boy feelsperfectly well in every way, and he has always beenin. good health. He has only once suffered injuryby reason of the attacks. He joined up in December,1915, and since February, 1.917, he has been at sea.On several occasions he has been punished forgoing to sleep on duty. He was very anxious to becured. As soon as he was seen, and his historyobtained, he was sent to the neurological ward.A more detailed account of his attacks prior to
his admission is as follows. He says that he hasfrequently fallen out of bed at night and been putback, but has known nothing about it until toldof it the next morning. When he was 15 he wentto sleep on the tail-board of a moving cart, and, beingthrown off, injured his knee slightly. On anotheroccasion he was on the top of a van and went tosleep just before the van reached a railway arch.The road was well known to him, he saw the arch-way, and knew that he would be struck if he didnot move, but in spite of all this he was unable toresist going to sleep. He was caught by the arch-way and thrown from the van, but escaped, fortu-nately, with a few bruises. He says that his parentshave always had great difficulty in rousing him inthe morning.Account of the sleeping attacks observed in
hospital.-The first attack was on the day follow-ing his admission. As dinners were being servedin the ward he walked to the chair by his bed, satdown, and immediately went to sleep. I found himsitting with his back to the ward, his head droppedover to one side. He held on to the bedclotheswith his hand, and when I removed it he fellheavily to the floor and would have hurt himselfhad his fall not been checked. For a few momentshe remained where he fell, then his eyes opened,and he got up, appearing to be very surprised at find-ing himself on the floor. He had no recollection offalling and could not explain the incident. Directlyafter dinner he lay on his bed, and during a sleepwhich was apparently normal he fell off and waslifted back. He did not wake for some time after,and he had no recollection of falling. Many similarattacks occurred both by day and night. Once hewent to sleep sitting on the stairs. On anotheroccasion he went off while sitting on a benchcleaning knives, and the following day he had an

1129
attack while he was scrubbing the floor. and Iremained motionless for ten minutes with his armimmersed up to the elbow in a bucket of water.I failed entirely to waken him in these or in anyof his attacks; neither did anyone else have the
Bslightest influence over him when he put himself Ito sleep. He made no sound and he did not replyto questions. His lids were closed. When he waslifted on to his feet he collapsed on to the floor,and as a rule in five or ten minutes he woke
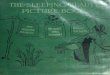
quietly of his own accord. On no occasion did hestruggle or show any of the manifestations of a fit.In all his own attacks, as also when he was under theinfluence of hypnotic suggestion, his eyes rotatedupwards at the moment the lids were raised. (SeeFig. B.) He was observed only on one occasion togo to sleep while he was walking about, but hetold us that this had happened fairly frequentlyin the past. The attacks had no relation to the
A, Awake. B, Hypnotised. C, Hypnotised. D, After operation.
company he was in or to the existing circumstances.He would go off to sleep when he was by himselfas readily as in a crowded ward.Night attacks.-Often it was reported that while
the patient was sleeping quietly he would suddenlysnore or breathe deeply and would then attemptto fall out of bed. More than once he did fall,and then he rolled under the next bed. On nooccasion did he wake during this performance.Sometimes he persisted in falling out of bed severaltimes in succession. As a rule he was very difficultto rouse in the morning.The total number of sleeping attacks which were
observed during four weeks was 33. The longestinterval of freedom was six days.Diagnosis.-Except for enlargement of one of the
turbinate bones examination revealed no evidenceof organic disease in any system. The boy’s physicalhealth was good, but his expression was rather bad-tempered and he looked worried (see Fig. A). Hewas not addicted to bad habits. The Wassermannreaction was negative in serum and cerebro-spinalfluid, and the fluid was in all other respects alsoperfectly normal.The only two possibilities as regards diagnosis
were hysteria and epilepsy. I was confident thatthe attacks were hysterical, due to his own sug-gestion ; in other words, I thought that he hypnotisedhimself. Many attempts were made, both when hewas himself and in hypnosis, to discover any under-lying cause for the condition, but all proved fruit-less. This failure to find a basis for the attacks
prompted a diagnosis of epilepsy from several
colleagues of experience. The patient, however,was never seen to hurt himself in his repeated falls,never had any loss of sphincter control, neveraltered in colour, and never showed an extensorplantar response during or after an attack. On theother hand, he had no manifest hysterical symptomsbetween his sleeping bouts or on waking fromthem.
ivotes on the Behaviour of the Patient in Hypnosis.On the assumption that he hypnotised himself it
was probable that he would be an easy subject tohypnotise, and this proved to be the case. He hadnot been hypnotised before. On the first occasionhe reacted to my suggestion in about a minute, andafter this I had merely to tell him to look at me andgo to sleep and immediately he would be soundasleep. Several other medical men at differenttimes attempted to hypnotise him, but without
success. This was not due to any counter-sugges-tion of mine; in fact, I told the patient that I wishedhim to go to sleep at their bidding. He made noconscious effort to resist them, but said that be didnot feel sleepy.When he was hypnotised he obeyed all my
instructions promptly, and ate, danced, smoked,and sang songs to order, but he accepted commissionsfrom no one but myself unless directed to do so byme. He said that it was idle for me to tell anotherin his hearing that orders from him would be
obeyed, nor would he respond to my written ordersunless they were presented directly by myself.When told to fall off the bed he rolled over and fellvery heavily on to the floor, making no attempt tosave himself, and narrowly escaping injury. Thefall did not waken him. Before he was hypnotisedhe was shown a form of will made out so that hispossessions were left in a certain direction, and hewas asked to put his signature to it. He not onlyrefused but he wrote across the paper " I refuse tosign this." A moment later he was hypnotised andsigned without protest a precisely duplicate form.He said that he would shoot me or himself at mycommand, that he would jump from an upperwindow or remain in a burning room, and he leftno one in any doubt that he would be as good ashis word. He was told to strike an officer of highstanding (a court-martial offence), and did so.
Similar instructions when he was awake made himvery indignant. It is unnecessary to give furtherillustrations of the absolute power over hisbehaviour and actions which I was able so easily

1130
to exert when he was hypnotised, but there was anabundance of evidence to controvert the statementmade by Dr. J. A. Hadfield in
"
Immortality " that" the hypnotised person will refuse to do anythingthat is strongly repugnant to him ...... and is there-fore not the automaton some people would have ussuppose." All -my investigations were conducted inthe presence of medical witnesses.When the eyelids were passively raised it was
observed that the globes were rotated upwards(see Fig. B). Later it was noticed that this rotationoccurred at the moment the lids were raised. Thesame thing happened when he put himself to sleep.When he was told to do so he opened his eyesnormally and all ocular movements were correctlyperformed (see Fig. C). Awake, he was quite unableto rotate the eyeballs more than the normal amount.On one occasion cutaneous analgesia was found inthe absence of any suggestion. With this exceptionsensation was absolutely normal, but the mostextensive and profound analgesia and hyperaesthesiacould be produced and removed at a word, althoughI did not succeed in suggesting complete absence ofpain when he was touched with a hot iron. Pin-prickscaused the normal amount of heamorrhage. I wasunable to demonstrate hyperacuity of vision or ofhearing, but Dr. Craig Dunlop found that in
hypnosis the bone conduction was increased. Reflexblinking to the stimulus of bright light was presentuntil its abolition was suggested. The patient didnot rouse when water was thrown over him or
when he was stimulated in other ways. He wasoblivious to very loud noises close to his ears, suchas that made by banging a poker on a shovel,although no suggestion had been made that hewould not hear it.He was unable to make his respiratory move-
ments quite imperceptible, when told to simulate aman dead. Marked rigidity of the limbs was suggestedwith ease, but the suggestion of extreme continuedrigidity of the trunk as a whole was not successful.Attempts to produce thought transference wereunavailing. He said that he obeyed me merelybecause he heard my voice, even when I whispered.He would not admit any other reason. No one ofmany observers succeeded in waking him. Whenhe was awake he had no recollection of any of theincidents which had occurred, but most of thedetails were recalled in subsequent hypnosis. Hedid not remember in hypnosis occurrences duringthe periods when he put himself to sleep.On one occasion I hypnotised the patient at
11 A.M. and told him to remain asleep until Iwakened him at 4 P.M. I found on my return thathe had wakened himself at 1.30 P.M. Another timeI told him, when he was hypnotised, that he was totelephone to me two hours later when he wasawake. I then woke him up and he had his dinner.At the exact hour appointed he telephoned to meand carried on a conversation. I imagined that hewas awake, but when I saw him later he had norecollection of telephoning to me. I then found outthat he had laid down after dinner and presumablypassed into one of his own sleeping affairs, for hewas certainly asleep when he got up and askedwhere the telephone was and rung me up. Further
suggestions under hypnosis that he would do certainthings at a later hour when awake failed.The following incident was of interest. Dr. E. A.
Cockayne attempted to hypnotise the boy in myabsence and was unsuccessful. I then told thepatient that it was my wish that Dr. Cockayneshould be successful and I went out of the room. The
second attempt was also without success and Dr.Cockayne came to tell me so. After a moment wewent into the room together and found the boy fastasleep and about to fall from the bed. The questionarose whether he was under the influence of Dr.Cockayne or of myself, but neither of us was ableto make the slightest impression upon him. Soonafterwards he woke up and sat on the side of thebed and spoke to us, and a moment later, in ourpresence but without a word of any sort from eitherof us, he leant forwards fast asleep and fell heavily,head first, on the floor. We were unable to wakenhim. Without speaking, I plunged pins into himand found him completely analgesic. Water thrownover him failed to rouse him, but when it wasdropped from a height on to his face it was obviousthat he appreciated it and shortly after he woke up.He was astonished, equally obviously, to find him-self wet through and he told us that he had notfelt the water at all. On another day very carefulexperiments, controlled by Dr. Cockayne, weremade by me to produce blistering of the skin bysuggestion. Dr. Hadfield described a series ofsuccessful tests of this nature in THE LANCET ofNov. 3rd, 1917. I failed completely to produce theslightest objective lesion by suggestion.
.
Treatment.
On July 2nd I told the boy that he was to resistmy suggestions of sleep. For a time he was successful, finally passing into a sleep in which I hadno influence over him. When he woke I told himthat soon I should be quite unable to send him tosleep and I explained very carefully to him that assoon as he was able to resist my efforts he wouldalso be able to resist his own suggestion to go tosleep. I told him that his own attacks had norelation to natural sleep and that although he didnot recognise the fact it was obvious that his ownattacks were the very rapid effect of a suggestionto sleep which had its origin in his own brain. OnJuly 8th he was hypnotised, but not very readily,and strong suggestion was made that in the futurehe would always be able easily to resist my influ-ence and also that he would have no difficulty inpreventing his own attacks. The next day I failedentirely to hypnotise him, but a few hours later hewent to sleep while leaning against the wall inanother ward. When the attendant, who did notknow him, went to_rouse him the boy fell heavilyon to the floor, still sound asleep. Thus the firstpart of my suggestion had proved successful, butnot the second part, and I was now deprived of auseful means of communicating with him.On July 10th he had a small operation on his
nose for obstruction. The sleeping attacks recurredwith some frequency. I made many furtherattempts to hypnotise him, but always withoutsuccess, although I told him that for a specialpurpose I wished to be successful, and that I hadreasons for retracting my previous statements. Iwas not able to get him even drowsy. He used totake pleasure in pretending that he was asleep,merely in order that he might watch my dismay.On July 25th he went to sleep during a game ofcards, sliding off the chair and rolling under a bed.He retained his cards in their proper positionbetween his fingers. For some weeks he took 90 gr.of bromide a day in deference to the opinions ofthose who thought that he might be epileptic,but the attacks continued without abatement,reaching a climax when he went to sleep in thebarber’s chair and resisted every attempt to waken

1131
him made by a frightened crowd. This attackoccurred on the day prior to the operation on hisskull. On August 2nd he volunteered to assist anillusionist on a stage, and did so without mishap.
Op’ctOM.—On August 9th, after some pre-liminary stage management, his head was X rayedand he was told that at last the real cause of hisillness had been discovered, and that an operationfor the removal of a piece of thickened bone wasnecessary in order to effect a complete and per-manent cure. At a demonstration of neurologicalcases I read out to the audience in his presence thenotes of a similar but purely imaginary case, inwhich operation on the skull had proved successful.He agreed readily to my proposals and wrote homeat once to say that a cure had been discovered, and ito obtain consent to undergo the operation. OnAugust llth Dr. L. Horsley gave him some open etherand with Dr. G. H. C. Griffith’s assistance I trephinedthe skull in the right parietal region and removedthe disc of bone. The dura mater was healthy andwas left alone. The bone was normal. Directlythe patient came round he was shown the piece ofbone and given it to feel, and he was told howsuccessful the operation had been. The bone wasdrilled and suspended round his neck, where itremained for many months. He wrote his initialson it and also the date of the operation. An attemptto suggest anaesthesia by substituting scent for theether was unsuccessful.
Srbseque2t Hist01’Y.From the date of the operation his sleeping
attacks ceased entirely and to all and sundry headmitted with great pride that he was absolutelycured. He did not relapse when I went on leave.On Sept. 12th the patient went on leave. Heremained perfectly well at home. He was late in
returning to duty on Oct. 2nd and he says thatwhile sitting in the guard-room he dropped off tosleep and required some shaking before he wasroused. There is some reason to think that thiswas not a recurrence but was assumed in order tolessen his punishment. In April, 1919, he was seenand examined in London. He was very pleasedwith himself and looked well and happy. He saidthat in December, 1919, he had gone to sleep at hiswork, but that it was natural sleep. He signed apaper saying that he was completely cured. With-out any preamble I tried to hypnotise him andfailed. In June, 1919, he was seen again. Heremained perfectly well and had no headache.He said that he was still difficult to rouse in themorning and had lost a job through being late.Unfortunately counter-suggestion to this particularphase of his illness had been omitted.With the two exceptions mentioned above, neither
of which was a proved recurrence, the patient hasremained perfectly well since his operation18 months ago, and this in spite of the fact thathis future was imperilled by a diagnosis of hysteriaon his discharge papers, and in spite of the factalso that in March, 1919, he lost his trophy. Reportswhile he remained in the hospital and since hisdischarge agree that in his behaviour he has i
changed markedly for the better. He is now politeand thoughtful of others, whereas prior to hisoperation he was inclined to be selfish and bad-tempered. His expression reflects this change inhis personality (see Figs. A and D). In July, 1919,the patient was shown before the Association ofPhysicians.Frequently I have been asked why I actually
removed a piece of bone, and my answer is that,
having committed myself to the statement of thethickened bone, and having told the patient thatits removal was necessary it was much in my mindthat I must leave him with a definite, tangibledepression in his skull to which he could point.It must be. remembered that when these conversa-tions took place the boy’s future was at stake anda cure problematical. In the few cases in which itis necessary to be unscientific in order to cure hys-terical symptoms it is necessary to be consistent.For. the same reason the boy was shown the
piece of bone at the earliest moment of his recoveryto full consciousness, and it was then that I realisedthat probably the cure would be made more certainif he could be persuaded to regard the bone as aprecious possession. My reason to the patient forwishing him to wear it round his neck was that itwould serve to remind himself and others that hisskull had been operated on, but it is clear that themental effect of constantly handling and showingoff his treasure was likely to be the strongestpossible suggestion against relapse.The only other patient I have seen who at all
resembled the above was a boy of 16 who wentinto trances, lasting as long as 24 hours. Theseall terminated in typical hysterical fits, in whichopisthotonos was a constant feature.
Hurley-street, W.
NOTES ON SOME
OCCASIONAL MANIFESTATIONS OFMALARIA.
BY D. W. CARMALT JONES, M.D. OXON.,F.R.C.P. LOND.,
PHYSICIAN TO WESTMINSTER HOSPITAL ; LATE CONSULTINGPHYSICIAN, EGYPTIAN EXPEDITIONARY FORCE.
MALARIA was the greatest of all causes ofadmission to hospital in Egypt during the recentcampaign, and probably also in Salonika and
Mesopotamia. The troops at Gallipoli were alsoheavily infected, and the Indian garrisons havesuffered exposure to the same risk. There musttherefore be in this country great numbers of menwho have had malaria, and of these a proportion arecertain to suffer from relapses. Probably every largehospital in the kingdom contains such cases, andrecurrent ague is a complaint constantly heard atPensions Boards.The common phenomena of malaria are familiar
enough, but there are other manifestations of thedisease of rare occurrence, and although recordedin the text-books, they may not be referred totheir proper cause unless their relationship tomalaria is borne in mind. Such errors are to be
regretted, because the symptoms are often alarm-ing in character, but yield readily to proper treat-ment with quinine.The following notes were made upon cases of
this kind, which occurred in patients to whomattention was drawn by medical officers in chargeof divisions and wards during routine visits tohospitals in Egypt. The majority of the sym-ptoms are referable to the effect of the diseaseupon blood-vessels, generally with the productionof haemorrhage from mucous membranes and intosolid organs ; thrombosis is also to be met with,though less frequently than haemorrhage.Unusual Sy7rzZrtoms of Malarial in the CirculatorytRespiratory, Excretot’Y, and Alimentat’y Systems.Apart from vascular symptoms, disorders also
arise in the circulatory, respiratory, and excretory