Embed Size (px)
Citation preview
INTRODU
I N T R 0 D U C T I ~~ Traditional system of medicines i.e. Ayurveda etc., which formed the basis of
health care throughout the world since the earliest days of mankind are still
widely used, and have considerable importance in international trade. India is
sitting on a gold mine of well-recorded and well practiced knowledge of
traditional medicine. But, unlike China, India has not been able to capitalize this
wealth by promoting its use in the developed world despite their renewed
interest in herbal medicines. There are several reasons for this; one of the major
reasons is that our products are not backed by rigorous scientific studies to
establish their safety, efficacy and standards. The demand of ayurvedic medicine
is gearing up at a rapid rate and the scientific community worrying about the
quality, safety and efficacy of the traditional formulation (Bodekar, 2002).
With the widespread use of traditional medicine as well as complementary/
alternative medicine and the rapid expansion of international herbal medicine
markets, the development of national policies and regulations on traditional
medicine has become an important concern for both health authorities and the
public. National policies and regulations on traditional medicine could ensure the
safety, quality and efficacy of herbal therapies and products, and function as
important steps towards integrative health-care systems (WHO, 2001)
In order to promote global acceptance of traditional formulations, there is an
urgent need to evaluate the therapeutic potential of the drugs as per regulatory
guidelines. Ironically, not all of the herbal products are available in standardized
form, which is the minimum requirement for introducing a product in the global
market (WIIO, 2001).
Demand for high quality, safe, effective, and pure natural formulations with
various substances have been growing significantly in the industrial world. In the
J ·a/idation f'!j Preparation Pmau and rinr:rrrrintim: of \om('. tyun<·dit· rormulatiom
INTRODU
I h b d . I ·1 b . I b ~j past tme, er s an essenha 01 eanng p ants were largely arvested from the
wild and brought to the market without many questions asked about their origin,
method of cultivation, botanical identity, purity, safety, and efficacy. With
further improvement in communication and education, there has been a growing
consciousness in industrialized countries about personal health, environmental
safety, sustainable harvesting, and loss of genetic diversity (Herbal monographs,
1997).
Traditional formulations are medicinal preparations, containing a single plant or
a mixture of two or more different types of medicinal plants. For traditional
formulations, there is a need of scientific proof and clinical validation with
chemical standardization, biological assays, animal models and clinical trials.
Quality assurance of traditional formulations is the prerequisite of credible
clinical trials. According to the draft guidelines stated by the United States Food
and Drug Administration and the European Agency for the evaluation of
medicinal products, various aspects of analysis must be performed for the
purpose of certification of traditional formulations. Currently, there is a
common practice among natural products analysis to select one or more
compounds as either active or markers for purposes of identification and quality
assessment. This problem is compounded when one substance that contains a
specific class of compounds is combined with others containing the same or
different classes of compounds. It is necessary to develop a type of quality
assessment system that adequately meets the complex characteristics of herbals.
Fingerprint analysis by which multiple compounds in single herbal drugs and
finished formulation can be identified represents a rational approach for the
quality assessment of traditional fommlations (Martindale, 1999).
2
INTRODU
P f ' I . 'fi I . ffi . d ~1· f ~ rocess o preparatiOn p ays a s1gm !Cant ro e m e ectiveness an qua 1ty o
traditional/ ayurvedic formulation. Process validation is "A documented program
which provides a high degree of assurance that a specific process will
consistently produce a product meeting its predetermined specification and
quality attributes". The quality of pharmaceuticals has been a concern of the
World Health Organization (WHO) since its inception. Many international
authorities and agencies like European agencies for the evaluation of medicinal
product, European Scientific Co-operation of phyto-medicine, U.S. Agencies for
Health Care Policy and Research, European Pharmacopoeia Commission,
Department of Indian System of Medicine have been started creating a new
mechanism to induce a quality control and standardization of botanical and
ayurvedic medicine. It is absolutely necessary to develop reliable analytical
methods in order to control the quality of herbal medicines. Fingerprint
technique was introduced and accepted by WHO, as a powerful tool for
identification and quality evaluation of multi-component herbal/traditional
medicines (WHO Guidelines 1991)
The system of ayurveda, although at present mainly confined to India, but it has
had a much wider reorganization and having prevalence from the past since the
dawn of human civilization. This system has undergone many vicissitudes in the
course of its long and chequered history. However, it still remains the mainstay
of medical relief among the majority of the people in this country. Even in the
neighbouring countries the system of ayurveda is reported to be fairly prevalent
(The Ayurvedic formulary of India, 2003).
In ancient time when the ayurvcdic medicines were developed, preparation,
standardization and quality control of ayurvcdic fommlation maintained by fully
J ·a/idatian (1! Prrrnration rnlct"H and rim:crprintinr: nf \(Jnlt' Ayunt•dic rrmnulatiom
3
INTRODU
~! ----~~----~~~~~~--~~------~----~~--~~--~ IN committed professionals. Either failing compliance of complete ayurvedJC
process or adopting short-cuts can result into compromised therapeutic gains in
the present scenario (Patwardhan, 2000, Jain et.al, 2007).
On account of process evolution, commercialization and environment pollution
quality of the ayurvedic formulation declined and they are not as effective as
prehistoric formulation (Mukharjee, 2002).
The traditional ayurvedic text claims that ayurvedic formulation prepared
according to the method given in ayurvedic text will always be superior in
quality, safety, and efficacy (The Ayurvedic formulary of India, 2003,
Bhaisajyaratnawali, 1961 ).
· Ayurvedic formulary of India states that, if the raw materials to be used in a
medicine and stage by stage processes of preparation are standardized, the final
formulation or compound formulation can be expected to confirm the uniform
standards (The Ayurvedic formulary ofindia, 2003).
The proposed work hence is an effort to standardize/ translate the method as
mentioned in the Ayurvedic texts and to develop certain parameters which can
be used as fingerprinting parameter for validation of preparation process and
standardization of ayurvedic formulation.
l'a/idation flj Preparation Prnau and fi,,::crrn·nrin.r: of 't'"''" A.1un <·die rormulatiom
4
INTRODU
----~~ 1.1 Market Potential of traditional! herbal medicine
In developed countries, a resurgence of interest in traditional medicines has
resulted from the preference of many consumers towards products of natural
origin. Recognition of their clinical, pharmaceutical and economic value is still
growing, although this varies widely between cotmtries .The percentage of the
population, which has used CAM at least once, is 48% in Australia, 70% in
Canada, 42% in USA, 38% in Belgium and 90% in Germany. Studies show that
in Africa up to 80% people use traditional medicines, in China TM accounts for
around 40%, and in India 48% of the population having faith in traditional
system of medicine particularly in ayurvedic system of medicine (WHO, 2002-
2005).
It has been postulated that by 2010 at least two-thirds of the United States
population will be using one or more of the alternative therapeutic approaches.
Use of indigenous drugs of natural origin forms a major part of such therapies;
more than 1500 herbals are sold as dietary supplements or ethnic traditional
medicines (WHO, 2001).
Total Indian market for the ayurvedic formulation is of 1000 million dollars a
year while the exports of ayurvedic medicines have reached a value of 100
million dollars a year. About 60% of this is crude herbs (to be manufactured into
products outside India), about 30% is finished product shipped abroad for direct
sales to consumers, and the remaining I 0% is partially prepared products to be
finished in the foreign countries. (Dhannananda, 2004).
1.2 Regulatory control of herbal medicines world-wide
The World Health Organization (WHO) has reviewed the regulatory control of
hcrhal medicines in 50 countries and summarized the wide differences in the
5
INTRODU
---;-----:----:--:---c----:-----~~~ approach of regulations between these countries. Herbal products are well
established as phytomedicines in some countries, whereas in others their
therapeutic claims are not allowed and regarded as foods.
In Australia, Complementary medicines, including herbal medicines are
regulated under therapeutics goods legislation 1989. For the purpose of labeling
requirements, herbs are included in the list of Australian approved names for
pharmaceutical substances, which is published by the Therapeutic Goods
Administration. Herbal medicines are regulated as drugs in Canada and must
conform to labelling and other requirements as set out in the Food and Drugs Act
and Regulations (Hoppe, 1981 ).
Herbal remedies used for minor self-limiting conditions are allocated a Drug
Identification Number based on pharmacological rationale. In order to facilitate
registration of products containing herbs, a series of Standardized Drug
Monographs has been prepared. The Drugs Directorate has provided guidelines
for the manufacture and sale of botanical products which fall into three
categories: food supplements (no DIN required, no therapeutic claims);
phytopharmaceuticals with full drug status (approved therapeutic indications,
approved dosage, efficacy supported by scientific evidence, DIN required);
traditional herbal medicines (self-medication only, efficacy supported from the
herbal literature, approved therapeutic indications and dosage)(Leung, 1980). In
November 2001, the Natural Health Products Directorate published a series of
further developments on the working draft of the proposed regulatory framework
for Natural Health Products (Mabey, 1988). Product licences, compliance with
good manufacturing practice (GMP), and a definition of natural products are
currently being subject to a review procedure.
----- -----------~------ -------- ---I ·a!idation (If Preparation ProCC\\ and nm~crpn"ntin.r: nf \(I me l!un cdic f(/nrmlarioll\
6
INTRODU
Tire m'jodty ofmOOidmll h~b• ~d thoiT prodoot• 're regol,.od lo lh::Jl foods or food additives, and most of the regulatory action has been concerned
with safety (Hoppe, 1981). In 1990, the Food and Drugs Administration (FDA)
reported on over-the-counter drugs, including herbs (Martindale, 1999). Some
herbs (e.g. cascara, senna) were pronounced safe and effective, but the majority
were not. Overall, 250 herbs, primarily based on their use as food additives, i.e.
flavours and fragrances, were designated GRAS (Generally Regarded As Safe)
status; however, this does not mean that such herbs (e.g. ginger, liquorice) are
FDA-approved for therapeutic purposes. In 1994, the Dietary Supplement Health
and Education Act (OSHEA) became law. In theory, this Act allows
publications, book chapters and scientific reports to support the sale of dietary
supplements (Martindale, 1999). Although medicinal claims cannot be made for
such products, labelling may describe effects on general well-being. OSHEA
and its regulations seek to define herbs in the context of the modem market
place, but they can only be regarded as an interim legislative step (Martindale,
1999).
In India, the first National Health Policy 1983, mentions that India's rich
tradition of health care should be included in national programmes. The National
health Policy states that TM experts and medicines should be used to stabilize
the population. The department of A YUSH, which started in 1995, regulates TM
programmes. There are separate directorates of Indian systems of medicine and
homeopathy in state governments. The government of India has an explicit and
separate policy for Indian (traditional) medicine since 2002.Traditional medicine
is also governed by the Drugs and Cosmetics Act, 1940. Licensing of
manufacturers and the provisions of the Drugs Act arc implemented by the state
J ·ulid,uion (If frl."raratiort Procrn mrd ringl."rrrinting t~/ \{lmr .II un·t•dic fl1rmulatimn
7
INTRODU
--------;::;:~~~~~ governments. GMPs are mandatory smce 2002, although not exactly as
recommended by WHO, but still they are based on them. Central and state
governments are impressing upon manufacturing units to comply with GMP
norms and to ensure quality standards.
1.3 WHO regulation of herbals
1.3.1 The WHO traditional medicine programme (WHO, 1998)
The World Health Assembly (WHA) has adopted a number of resolutions
drawing attention to the fact that a large section of the population in many
developing countries still relies on traditional medicine, and that the work force
represented by traditional practitioners is a potentially important resource for
primary health care. In 1991, the Director-General of WHO, in a report to the
forty-fourth WHA, emphasized the great importance of medicinal plants to the
health of individuals and communities. Earlier, in 1978, the thirty-first WHA had
adopted a resolution (WHA31.33) that called on the Director-General to compile
and periodically update a therapeutic classification of medicinal plants, related to
the therapeutic classification of all drugs; subsequently, resolution of
WHA40.33, adopted in 1987, urged member states to ensure quality control of
drugs derived from traditional plant remedies by using modem techniques and
applying suitable standards and good manufacturing practices; and resolution
WHA42.43, of I 989, urged member states to introduce measures for the
regulation and control of medicinal plant products and for the establishment and
maintenance of suitable standards. Based on the relevant WHA resolutions, the
major objectives of the traditional medicine programme arc to facilitate the
integration of traditional medicine into national health care systems; to promote
the rational usc of traditional medicine through the development of technical
J ·a/idarion nf Prt'rnration Prnct''' and ri11gaprinring of wmt" A.1un·(·dic r nrmularimr~ 8
INTRODU
-g-u.,-id;-e-;cli:-n_e_s-an-d-;-i:-n-:-te-m-at:-;-io_n_a-;l-s-ta-n"""'d:-a-rd:-s--:-in-t7h-e--::fi:-e-:-ld-:----o-f::-:-h-e-=rb-a7l-m-e"""""dioi"< J acupuncture; and to act as a clearing house for the dissemination of information
on various forms of traditional medicine.
In resolution WHA42.43 (1989), the health assembly urged member states to
make a comprehensive evaluation of their traditional systems of medicine; to
make a systematic inventory and assessment (preclinical and clinical) of the
medicinal plants used; to introduce measures for the regulation and control of
medicinal plant products and for the establishment and maintenance of suitable
standards; and to identify those medicinal plants, or remedies derived from them,
which have a satisfactory efficacy/side-effect ratio and which should be included
in national formularies or pharmacopoeias.
1.3.2 Guidelines for the assessment of herbal medicines (WHO guidelines, 1991)
A WHO consultation in Munich, Germany, June 1991 drafted guidelines for the
assessment of herbal medicines (WHO/TRM/91.4), which were adopted for
general use by the 61h ICDRA in Ottawa, October 1991.
a. These guidelines contain basic criteria for the assessment of quality, safety,
and efficacy and important requirements for labeling and the package insert
for consumers' information.
b. The requirements for pharmaceutical assessment cover issues such as
identification, galenical forms, analysis and stability.
c. Safety assessment should at least cover the documented expenence of
safety and toxicological studies, where indicated.
d. The assessment of efficacy and intended use includes evaluation of
traditional usc through appraisal of the literature and evidence to support
the indication claims.
J "a/id.ztion (If frrpart.Jtion Pr(JCI"\S and fi'ngapn"ntin.f: of \ONI('. fyunw/ic r(lmUJfnthm\
9
INTRODU
----~~ 1.3.3 Guidelines for formulation of national policy on herbal medicines
(WHO guidelines, 1994)
The majority of the world population seeks treatment with traditional medical
practices, especially herbal medicine. The guideline was proposed to formulate
national policies on traditional medicines and to encourage co-operation between
member states. The aim of such national policies would be to develop regulatory
and legal reforms to ensure good practice, and to extend primary health care
coverage, while ensuring the authenticity, safety and efficacy of these medicines.
Main objectives include the recognition of traditional medicine as an integral
part of national health care systems, co-operation between modem and
traditional medicine, promotion of the rational use of products, introduction of
quality assurance systems, guarantee of regular supplies and to promote the
research and development of regulatory measures. It has been recommended to
countries that a National Expert Committee should be established, which would
be the appropriate authority to identify the steps and plans needed to formulate
national policy in this area and then to develop, direct and monitor the various
phases of its implementation.
1.3.4 Guidelines for the assessment of herbal medicines (WHO guidelines, 1996)
These guidelines for the assessment of herbal medicines are intended to facilitate
the work of regulatory authorities, scientific bodies and industries in the
development, assessment and registration of such products. The assessment
should reflect the scientific knowledge gathered in that field.
These guidelines defines the criteria for assessment of quality involving
pharmaceutical assessment of crude plant material, plant preparations and
finished products particularly using chromatographic fingerprints if no other
----~-------- --~~-----------~------------- ---
10
INTRODU
~~------::----::----,-----,--:--~~ satisfactory criteria available; assessment of safety involving toxicological
studies with proper documentation and cited literature; assessment of efficacy
including the pharmacological and clinical effects of the active ingredients and
evidences to support the indications and Intended use of the guideline also
defines the information, which should be given to the consumers for use of the
preparation.
1.3.5 Guidelines for methodologies on research and evaluation of TM (WHO
guidelines, 2000)
The methodologies for research and evaluation of traditional medicine should be
based on the following basic principles. On the one hand, the methodologies
should guarantee the safety and efficacy of herbal medicines and traditional
procedure-based therapies. On the other hand, however, they should not become
obstacles to the application and development of traditional medicine.
The specific objectives of the guidelines are to. harmonize the use of certain
accepted and important terms in traditional medicine; summarize key issues for
developing methodologies for research and evaluation of traditional medicine; to
. improve the quality and value of research in traditional medicine and provide
appropriate evaluation methods to facilitate the development of regulation and
registration in traditional medicine.
1.3.6 WHO guidelines on GACP for medicinal plants (WHO guidelines, 2000)
The guidelines provide a detailed description of the techniques and measures
required for the appropriate cultivation and collection of medicinal plants and for
the recording and documentation of necessary data and information during their
processing. Good agricultural and collection practices for medicinal plants is the
first step in quality assurance, on which the safety and efficacy of herbal
11
INTRODU
d. . I d d. ld d . I . ~I . ~ me Icma pro ucts uect y epen upon and will a so play an Important ro e m
the protection of natural resources of medicinal plants for sustainable use.
1.3.7 The WHO traditional medicine strategy (WHO, 2002-2005)
The WHO recognizes that the traditional use of herbal medicines refers to the
long historical use of these medicines and that they may be accepted by national
authorities. As a result of this view, the WHO traditional medicines strategy
2002-2005 was developed to review a framework for action for WHO and its
partners aimed at enabling traditional medicine/ complementary alternative
medicine (TM/CAM) to play a far greater role in reducing excess mortality and
morbidity especially among impoverished populations, which is one of WHO's
strategic directions for 2002-2005. Specific objectives in TM/CAM for 2002-
2005 are accordingly to support countries to integrate TM/CAM with national
health care systems, as appropriate by developing and implementing national
TM/CAM policies and programmes; to promote the safety, efficacy and quality
of TM/CAM by expanding the knowledgebase on TM/CAM, and by providing
guidance on regulatory and quality assurance standards; to increase the
availability and affordability of TM/CAM, as appropriate, with an emphasis on
access for poor populations and to promote therapeutically sound use of
appropriate TM/CAM by providers and consumers.
1.4 Ayurveda
Ayurveda is the science of health and healing practiced by ancient Aryans,
which is based on Atharvaveda, one of the oldest scriptures of Hindus, about
3000 years old. Ayurveda believes that various materials of vegetable, animal,
and mineral origin have some medicinal value. The medicinal properties of these
materials arc time tested and have been used for centuries in ayurvedic
12
INTROOU
~~--~~ medicines to cure illness and/or help maintain health. Ayurvedic medicaments
are made from herbs or mixtures of herbs, either alone or in combination with
minerals, metals and other ingredients of animal origin. The metals, animals and
minerals are purified by individual processes before being used for medicinal
purposes. Impurified materials are not allowed to be used as medicine. The
object of ayurveda is to counteract the imbalance of three essential elements
vata, pitta and kapha (air, bile and phlegm respectively) which constitute the
tridosh from which the body originates. It is tridosha, which regularizes the
normal working of human body (Ayurveda Sar Sangrah, 2000). Ayurvedic
medicine is defined in Drugs and Cosmetic Act 1940, includes all medicines
intended for internal or external use, or in the diagnosis, treatment, mitigation or
prevention of disease or disorders in human beings or animals and manufactured
exclusively in accordance with the formula described in the authoritative books
of ayurvedic system of medicine specified in the first schedule of the act. In
ayurveda, the entire universe is composed of five basic elements called
panchmahabhuta and includes space (akasha), air (vayu), energy (teja), liquid
(jal) and solid (prithvi). The variable combinations of these principles make
tridosha in human body. These combinations are vata, pitta and kapha. They
have been interpreted in the following way.
Vata is composed of space and air (akasha and vayu). It is concerned with the
physical and mental activities which are activating or dynamic in nature. Vata
represents nervous system or nadichakra as per Ayurvedic terminology.
Pitta is composed of liquid and energy indicates biochemical/energy system. It
dominates nutritional and thermo genetic activities and also includes hormonal,
digestive and metabolic system.
J ·a!i.lation nf Prrparariotr rroccn and l"im:rrrrintim: nf wm(• A.lllnwlic r nrmulmiom
13
INTRODU
----~~ Kaplla is composed of solid and liquid indicates various tissues and organs. It is
concerned with intergration of structural elements of the body.
Ayurvedic therapeutics is based on five pharmacological principles (panchsheel)
of durg. These principles are rasa, gun, virya, vipaka and prabhava.
1.4.1 Ayurvedic formulations (The Ayurvedic Formulary of india, 2000, 2003, Ayurveda
Sar Sangrah, 2000)
Ayurvedic formulations are those, which are prepared in accordance with the
formulae and procedures described in above authoritative texts. Different
solvents (menstrum) used in preparations of ayurvedic formulations are water,
oils, milk, ghee, cow's urine, etc. The use of sweetening agents, binding agents,
colourants, flavouring principles and other adjuvants are also very common in
ayurvedic preparations. With an objective of obtaining maximum therapeutic
benefit and making the formulation palatable, different pharmaceutical process
are prescribed in ayurveda. The important once are as follows:
Arka: It is the liquid preparation obtained by distillation of crude drugs in water
e.g.: Ajamodarka, Jatamamsyarka etc.
Churna: Fine powder of drug/drugs is known as chuma e.g.: Triphala, Trikatu,
Bhaskar Iavan chuma etc.
Dravaka: The liquid preparations obtained from lavanas or ksharas are known
as Dravakas. These are prepared by distillation process with or without addition
of any fluidse.g.: Sankha dravaka etc.
Ksharas: Alkaline (basic) substances obtained from the ash of drugs are known
as ksharas e.g.: Apamarga ksara, Kalyana ksara etc.
Lcpa: The preparation in the form of paste meant for cxtemal application on the
body is known as !cpa e.g.: Dasanga !cpa, Pathyadi !cpa etc.
-~~~-~-----~-------------------
14
INTRODU
Vatika and Gutika: MOOk=ffiO ;, the form of illblet. of pill• = Jam~ li vatika or gutika e.g.: Bhuvneshvara vati, Drakshadi gutika, Prabhakara vati etc.
Netrabindu and Anjana : Netrabindu is processed by dissolving the specified
crude drugs in water or kasaya or honey and used as eye drops. Anjanas are very
fine powders of medicaments to be applied with netrasalaka e.g.:
Nayanarnrtanjana, Nagarjunanjana etc.
Sattva: Water extractable solid substance obtained from a drug is known as
sattva e.g.: Guduchi sattva etc.
Pisti: Pisties are obtained by triturating the drug with the specified liquids and
exposing the same to sun or moonlight e.g.: Pravala pisti, Mukta pisti etc.
Ghrita (Senehkalpa): Ghritas are the preparations in which ghee is boiled with
the prescribed quantity of the decoction (kasaya) and fine paste (kalka) of the
drug as specified in the formula e.g.: Amrta ghrta, Eladi ghrta, Tiktaka ghrta etc.
Taila: Tailas are preparation in which taila is boiled with prescribed decoction
according to the formula e.g.: Narayana taila, Triphaladi tailam etc.
Bhasma: The powdered form of the substance obtained by calcinations of
metals, minerals of animals products by a special process in closed crucibles or
in pits covered with cow dung cakes (puta), are known as Bhasma e.g.: Louha
bhasma, Vajra bhasma, Tarnra bhasm, Pravala bhasma etc.
Rasa-Yoga: The medicinal preparations containing mineral drugs as their main
ingredients in the form of powder or pills are known as Rasa-yoga e.g.:
Amlapittantaka rasa, Karpura rasa, Gangasundra rasa,
Fanta: These are prepared by pouring hot water over the dry crude drugs e.g.:
Kutja fanta.
J ·ali dation (If Prrparatimr ProccH and fingerprinting nf \(lnJ( Ayun·,•dic !PrmulotifJn\
15
INTRODU
----~~ Nikadha: The residue or marc obtained in Kadha or Kashaya is treated with
boiling water and strained. The filtrate thus obtained is known as Nikadha.
Ghana-saar : The decoction obtained in the preparation of kadha or nikadha is
further evaporated to solid mass is known as Ghana-saar.
Kalka: When fresh or dry crude-drug is powdered and pounded with water hot
or cold to give a very fine paste then it is termed Kalka. e.g.: Apamarga kalka
Swarasa: When the Kalka is pressed in between the palms of the hand or is
expressed through the layers of cloth to produce a thick juice then it is called as
swaras. (Swa-rasa).
Asava and Arishta: Asava and Aristas are the medicinal preparations processed
by soaking the drug in the powdered forms or in the form of their decoction
(kasaya), in a solution of sugar of jaggery (Gur), for a specified period of time.
During soaking, it undergoes fermentation generating alcohol and in process
facilitating extraction of active constituents contained in the drugs Alcohol so
generated also serves as a preservative in the product e.g.: Lohasav, Kumariasav,
Dasmularistha, Draksharistha etc.
Nassyas: These are the nasal preparations and may be very fine powders,
aqueous or oily preparations.
Avaleha or leba and paka :Avaleha or Leba is a semisolid preparation of drugs
prepared by addition of sugar, jaggery (gur) or sugar candy and boiled with
prescribed drug-juice or decoction e.g.: Vasavaleha etc.
1.5 Standardization of Ayurvcdic formulation (WHO, 1996; 1998)
Standardization is the process of agreeing on technical standards. A standard is a
document that establishes uniform engineering or technical specifications,
criteria. methods. processes. or practices. The standardization of ayurvedic
r "a/idation (If Preparation Prt•CCH and f"ingaprintinr: of'""'~. tyun·(·dic l"'nmrulation~
16
INTROOU
~---:---------:--~~~ preparations have many characteristic features and needs careful
considerations.In ayurvedic formulation, standardization refers to providing
processed plant material that meets a specified concentration of a specific marker
constituent.
Quality of raw materials is essential for the manufacture of standard drug. Raw
materials purchased from the market vary in quality almost from batch to batch.
Different manufacturers use different methods for their formulations. Thus, the
preparation will also vary being dependent on the nature of the method used.
Further from the academic standpoint, the knowledge of contents, constituents of
drugs and their uses always enrich the ayurveda materia medica and pharmacy.
Therefore it is necessary to give priority to the work of standardization of
ayurvedic research. Standardization of ayurvedic formulation is rendered
difficult because of specific methods are not available for identification of raw
materials, there are no standard uses prescribed in literature for finished products
and vaidyas in different states of the country had been selecting raw materials
and preparing drugs according to their own established methods.
The important stages of standardization of ayurvedic formulations are
I. Standardization of raw materials.
2. Standardization of preparation process
3. Standardization of the finished product
1.5.1 Quality control of traditional/ herbal formulations
The quality of phannaceuticals has been a concern of the WHO since its
inception. Quality Control is a term that refers to processes involved in
maintaining the quality of validity of a manufactured product. The safety and
efficacy of herbal medicines is closely correlated with the quality of the source
I ·alidatimt (If frrrllfatiml ProcC\\ and /lngcrprimim: of ~omc. tyun t•dic Fonrwlation~
17
INTRODU
~~=-----:-:------~~~ materials used in their production. The quality of source materials is, in its tum,
determined by intrinsic factors (genetic) and extrinsic factors (environmental
conditions, cultivation and harvesting, field collection and post
harvest/collection transport and storage). Therefore, it is very difficult to perform
quality controls on the raw materials of herbal Drugs (Cardellina, 2002).
Therefore, production of quality traditional medicines has become a challenge to
regulatory authorities, scientific organizations and manufacturers.
1.5.1.1 Quality control methods
Methods currently utilized in evaluating herbs, their extracts and formulations
include organoleptic, microscopic, physical, chemical, chromatographic,
fingerprinting, microbiological, and biological methods.
1.5.1.1.1 Macroscopic analysis (WHO, 1998a)
Medicinal plant materials are categorized according to sensory, macroscopic and
microscopic characteristics. It is the first step towards establishing the identity
and degree of purity of such materials and should be carried out before any
further tests are undertaken. Visual inspection provides the simplest and quickest
means by which the identity, purity and possibly quality can be established.
Macroscopic identity of medicinal plant materials is based on shape, size, colour,
surface characteristics, texture, fracture characteristics and appearance of the cut
surface. However, since these characteristics are genuine material, it is often
necessary to substantiate the findings by microscopy and or physicochemical
analysis.
1.5.1. 1.2 1\licroscopic analysis (WHO, 1998a)
Microscopic evaluation allows more detailed examination of a drug and it can be
used to identify organized drugs by their histological characters. It also covers
f 'a/idmion flj Prcraration Prncc\fi and llnr:crpn'ntin.r: nfwml' Arun,•dic /'omwlatiom
18
INTRODU
""'' of'""'""''"" by """"""" of oh=k& "'"' to •=II qow<i <i~ "' drug• I j in powdered form or to histological sections of the drugs. The characteristics of
cell wall, cell contents, trichomes, fibres, vessels, measurement of sizes of
tissues etc can be studied in details.
1.5.1.1.~.1 Quantitative microscopic analysis (The Pharmacopoeia of India, 1966)
In addition to the simple measurement of the sizes of tissues, cells and cell
contents, it is possible to estimate the % of foreign organic matter in powdered
drugs by a lycopodium spore method. Other microscopic determinations, which
may be useful in certain cases, include vein-islet number, vein termination
number, palisade ratios, stomatal numbers and stomatal indices.
1.5.1.1.3 Physicochemical analysis (The Pharmacopoeia oflndia, 1966)
Physical standards should be determined for herbal drugs. These are rarely
constant for crude drugs but may help in evaluation specially with reference to
moisture content, specific gravity, density, viscosity, solubility in different
solvents, ash value, extractive value, volatile oil content, foreign matter, acid
value, Iodine value, saponification value, unsaponificable matter, acetyl value,
ester value, crude fibre, swelling index, melting point, refractive index, foaming
index etc.
1.5.1.1.4 Chemical methods
Quality of drugs should meet the standards related to safety, potency and
efficacy. The aim of quality control is to evaluate whether the sample of drug
complies with the appropriate specifications. These tests involve chemical
analysis of active constituents and may vary from single entity or combination of
several potent drugs in formulation, finished product etc. These methods are
designed to set the permissive limits of tolerance for the product when it reaches
··alidation fJj rrrraration FrocrH and flngrrJ'dlltim: nfwme. h un·l'dic Tomwlatiom
19
INTRODU
~~~~~~ the patient. Official Pharmacopoeial standards are designed considering all
known methods of manufacture, safeguard against the varying standards of
purity, impurity patterns, stability etc.
1.5.1.1.4.1 Volumetric methods
In volumetric methods, assay is based on the measurement of volume of solution
of known strength that is required to react completely with the substance to be
analyzed. On the basis of this measurement of volume, quantity of pure
component is estimated in this method. This method is classified in to different
types depending upon the type of reactions involved in the reaction (Mendham et
al., 2002).
1.5.1.1.4.1.1 Neutralization titration
Neutralization or aqueous acid-base titrations are usually reactions in which H+
in solution is titrated by OH- and this can be applied regardless of whether strong
acids, strong bases, weak acids, weak bases, weak acid salts, weak base salts in
the titration reaction (Mendham et al., 2002).
1.5.1.1.4.1.2 Non aqueous titration
This technique has now occupied a prominent place in analysis of drugs and
chemicals. The non aqueous titration has replaced the aqueous titration for many
substances which are either too weekly acidic or too weekly basic. It is based
upon the Bronsted-Lowrey and Lewis theory of acid and base and the nature and
influence of leveling effect of non-aqueous solvents on substances (Mendham et
al., 2002).
1.5.1.1.4.1.3 Precipitation titration
Precipitation is the combination of two ionic species to form a very insoluble
product. Precipitation of this product forces the reaction to completion, although
J ·alidation nf Preparation ProccH an,f rim:crl'n.nting nf wmc Ayunwlic T nrmu/atinm
20
INTRODU
~-~---~~ such reactions are not uncommon. Their use in titrations is limited because not
all precipitation reaction meets the specifications. For titrimetric analysis the
precipitate must be practically insoluble, the precipitation reaction should be
rapid and quantitative, the results should not be hampered by adsorption effects
and it must be position to detect the equivalent point during titration (Beckett
and Stenlake, 2000).
1.5.1.1.4.1.4 Oxidation reduction titration
These reactions are the chemical processes in which a change in valency of
reacting elements or ions takes place. The reaction is thus a process involving
the transfer of electrons from one element or ion to another resulting in the
change of valency of reacting atoms or ions. An oxidation-reduction indicator
marks the sudden change in oxidation potential in the neighborhood of the
equivalence point in an oxidation-reduction titration. The ideal redox indicator
will be one with an oxidation potential intermediate. A sharp, readily detectable
colour change occurred at the end point (Jerry, 1992).
1.5.1.1.4.1.5 Complexometric titration Complexometric titrations are those
reactions in which simple metal ions are transformed into complex ion by
addition of the reagent which is known as ligand. The complex formed is stable
and water-soluble. Disodium ethylenediamine tetra-acetic acid (EDTA) is very
versatile complexing agent (Beckett and Stenlake, 2000).
1.5.1.1.4.2 Gravimetric methods
Gravimetric analysis or quantitative analysis by weight is the process of isolating
and weighing the compound of knovm composition i.e. purest form. The
separation of compound is affected by number of ways like precipitation,
volatilization electro analytical etc. In these first two methods are important in
21
INTRODU
~~:--:---:--:--------:------:---~~ practice. Although gravimetric analysis is time-consuming, the constituent may
be examined for the presence of impurities and correction (Agarwal and
Agarwal, 1979).
1.5.1.1.4.3 Spectroscopic analysis
Spectroscopic analysis is concerned with the capacity of certain molecules to
absorb electromagnetic radiation at specific wavelength. This absorption or
emission is associated with changes in the energy states of the interacting
chemical species, and since each species has characteristic energy states,
spectroscopy can be used to identify the interacting species. Technique most
commonly employed in analytical field includes ultra violet, visible infrared and
atomic absorption spectrophotometry. The radiations utilized in spectroscopic
analysis can be roughly divided according to wavelength into the ultraviolet
(185-380 nrn), the visible (380-780 nm), the near infra red (780-3000 nm), and
the infra red regions (3-40 Jlm) (Willard eta!. 1986).
1.5.1.1.4.3.1 Colorimetric analysis
Colorimetry is concerned about the measurement of light in the visible region.
The basic principle of colorimetric analysis is the measurement of color of a
solution and its correlation to the determination of its concentration. The
measurement is made by comparing or reading the colour produced for the
substance with the same colour produced by a known amount of standard
material under well-defined conditions (Willard et a!. 1986).
1.5.1.1.4.3.2 Fluorescence analysis
When certain molecules are exposed to the electromagnetic radiation they
exhibit fluorescence. Fluorescence is a process of re-emission of radiant energy
absorbed in the form of visible light. In this process the light emitted is always of
l"a!id.Jtion (If Prrpararion Proccn and rinr:crpn·minr: of 5nmt. fyunw/ic r flrnmlatiom
22
INTRODU
high" ~wiffigili Jhm <hru •hrorl>ol. lo fl=•=re, 'b"'""'" md =i~ioo I j of light takes place in very short time (10-12 to 10-9 seconds). Ifthere is delay in
the emission of light then the phenomenon is called as phosphorescence. Both
these processes of re-quantitative determination of fluorescence are the basis of
fluorimetric analysis (Braun, 1987 and Willard et al. 1986).
For the quantitative studies their should be a definite relationship (linear)
between the concentration of species and the fluorescent intensity, which is
emitted such a relationship exists for very dilute solutions and fluorescent
intensity.
1.5.1.1.4.3.3 Infrared spectroscopy
The infrared absorption spectroscopy is concerned about the absorption of
infrared radiation by a molecule and exhibits characteristics absorption spectra.
Infrared spectrophotometer is a very important tool used in qualitative
identification and quantitative estimation of many drugs and chemicals. The
instrument is practically useful in pharmaceutical industry in identification of
drugs and detection of impurities (Bhal and Bhal 2001, Willard et al, 1986).1n
the infra red spectrum the fingerprint region (7-11 flm) is utilized to authenticate
and recognize many functional groups. British Pharmacopoeia involves
comparison of IR spectra of phytochemicals with European Pharmacopoeia
Chemical Reference Substances (EPCRS) as a test of identity (Evans 1996).
1.5.1.1.4.3.4 Nuclear magnetic resonance spectroscopy
NMR is designed for structural determination of organic compounds of natural
or synthetic origin. Use of H1 NMR spectroscopy and C13 NMR spectroscopy
have been described for assay of compounds described by TLC and HPLC and
confim1ation of certain groups and radicals position. It is concerned with the
J "a/idatimr (Jf Prt'raration rr(J('('H and llnr:crprilllin_r: (}I \(}nr(' A) un·cdic l"nmwlatiom
:23
INTRODU
~~ -:-ab;:-s:--o-rp---;:ti_o_n_o-;;f-c_e_rt-:-a-=-in_e_n_e_r_g_y--;-b-y-sp--:i-nn-I:-. n_g_n_u_c::-Ie-=i---=-in_a_m_a_g_n_e""ti:-c----;:-field when
irradiated by certain energy radiation perpendicular to it. Thus it permits
identification of atomic configurations in a molecule. Absorption occurs when
nuclei undergoes transitions from one alignment in the applied field to the
opposite one. The NMR spectroscopy enables us to record differences in
molecule and it also enables to know the positions of these nuclei within a
molecule. It enables to deduce different kinds of environment present in a
molecule and also about the atoms present in neighboring groups (Robert and
Francis, 2002, Willard et a!. 1986).
1.5.1.1.4.3.5 Mass spectroscopy
Like other spectroscopic techniques has been used as a routine method for
dealing with many analytical stable isotopes, examining ionization phenomena
studying free radicals etc. The mass spectrometer is an instrument in which the
substance in gaseous or vapour state is bombarded with a beam of electrons, to
form positively charged ions (captions) which are further sorted according to
their mass to charge ratio to record their masses and relative abundances. Both
positive and negative ions can be studied using mass spectrometer but usually
positive ions are analyzed since they are produced in large amounts as compared
to negative ions. The mass spectrum is a plot of relative abundance versus mass
to charge ratio. Each line upon the mass spectrum indicates the presence of
atoms or molecules of a particular mass (Willard et a!. I 986, Mendham et a!.
2002).
1.5.1.1.4.4 Methods for development of chromatographic fingerprints
Chromatographic methods represent the most useful and powerful technique for
the separation of components of a complex mixture. Because of the rapidity and
24
INTRODU
~~--,------------~~~ effectiveness, chromatography has been used in all the fields particularly in
chemistry, biology, medicine, dyes, forensic departments and clinical studies
with much advantage over other methods. A notable advantage of
chromatographic methods is that they are relatively 'gentle' methods and
decomposition of substances does not occur. One more advantage is that the
separations can be carried out in micro or semi micro scale i.e. a very small
quantity of mixture is required for analysis. The method used primarily for the
separation of the components of sample, in which components are distributed
between two phase, one of them is stationary while the other moves. The
stationary phase may be a solid or a liquid supported on a solid or a gel and may
be packed in a column spread as a layer or distributed as a film. The mobile
phase may be gaseous or liquid. Though fundamentally it is separation
technique, it provides identification of compounds and also the quantitative
estimation. It finds application in analysis of varied types gases and pollutants,
petroleum and petrochemicals, oils and fats, food and flavors, drugs and
vitamins, steroids and alkaloids, blood and serum, pesticides and fungicides,
radioactive isotopes and a number of miscellaneous purposes.
1.5.1.1.4.4.1 Column chromatography
The basic principle underlying in adsorption chromatography is adsorptions of
component at the solid liquid interface. For good separation, the components of
should have different degree of affinity for the solid support i.e. adsorbent and
the interaction between adsorbent and component should be reversible. The
component having strong adsorption for column material is held up while that
component having less affinity moves do\m the column at faster rate as the clute
passes through the column (Mendham ct a!., 2002).
··olidation of Preparation rroccH and fingcrprintin.r: of fi(lf71('. tyun·,·dic r omwlatiom
25
INTRODU
----~~ 1.5.1.1.4.4.2 Partition column chromatography
In partition column chromatography the solid adsorbent is replaced by a packing
material comprising as a support material coated with a stationary phase. The
stationary phase should be immiscible or at the most sparingly miscible with
mobile phase. In this technique the solute gets distributed itself between the two
phases depending on it's partition coefficient (Sharma, 1992).
1.5.1.1.4.4.3 Thin layer chromatography
Thin layer chromatography (TLC) is a simple and rapid method carried out using
thin layer of adsorbents on plates. TLC not only combines the advantages of
paper and column chromatography but in certain aspects it is found to be
superior to either method. As various materials of different adsorptive power are
used in TLC, the separation may result due to adsorption or partition or by both
phenomenon depending upon the nature of adsorbents used on plates and solvent
system used for development (Mukharjee, 2002).
1.5.1.1.4.4.4 Paper chromatography
Paper chromatography is the technique in which the separation of an unknown
substance is mainly carried out by the flow of solvents on the specially designed
chromatographic paper. In this case the solvent goes up by capillary action and
the separation is effected by differential migration of the substance due to
difference in distribution coefficients. The theoretical principle involved m
separation by paper chromatography is largely by partition coefficient.
The results are represented by Rr value which represent the movement or
migration of solute relative to the solvent front. This is indicating position of
migrated spots on chromatogram. R indicates the fraction of the solute molecules
in a solvent at any specified time (Sham1a, 1992).
J ·alitfation of rrcrnration Prncnt and llm:crpn·nlin.f! ()/ \Onlt!. trun,·Jic rormulatiom
26
INTRODU
----~~ 1.5.1.1.4.4.5 Ion exchange chromatography
The ion exchangers behave as a porous network, which carry a surplus electric
charge is compensated by the ions of opposite charge. When the ionization takes
place they are exchanged with the ions, which migrate into the solution
(Mukharjee, 2002).
1.5.1.1.4.4.6 High performance liquid chromatography
The obvious way to increase the flow rate and get efficient separation is to force
the liquid by a positive displacement pump or by gas pressure. This versatility
can be achieved by making certain modifications in columns and by using
smaller diameter and smaller surface area of column particles and by using other
suitable packing structure. HPLC is a high resolution and high-speed liquid
chromatography. It has several times more resolving power than open column
liquid chromatography. Hence it is used for speedy resolution of complex
mixtures (Edwards and Cobb, 1966).
1.5.1.1.4.4. 7 Gas chromatography
Gas chromatography is a widely used technique for separation of gaseous and
volatile substances, which are difficult to separate and analyze. It is a rather
simple and inexpensive method, generally efficient in regard to separation. The
gas as a moving phase is passed through a column containing adsorbent or a
liquid adsorbent supported on an inert solid. Thus adsorption or partition is
possible. In gas solid adsorption chromatography (GSC) the components of the
mixture distribute themselves between the gas phase and the adsorbent and the
separation is due to the difTcrcnces in adsorptive behavior. While in gas liquid
chromatography (GLC). the components of mixture distribute themselves
between gas phase and the stationary liquid phase according to their partition
J ·alidatimr of Prrparation ProaH and Tln_r:rrprintin.:: of.\nmt•. trun-,·1/ic ronnulatiom
27
INTRODU
ffi . Th ld fi . I b . .d . ~h ~ coe tctents. e so 1 unctwns on y as a support for t e hqm statwnary p ase,
enabling it to present a large surface to the gas. The GLC has a much greater
application in the analysis of the organic compounds, which has a measurable
vapour pressure at the temperature employed (Ewing 1995, Braun 1987).
1.5.1.1.4.4.8 Hyphenation procedures In the past two decades, combining a
chromatographic separation system on-line with a spectroscopic detector in order
to obtain structural information on the analytes present in a sample, has become
the most important approach for the identification and/or confirmation of the
identity of target and unknown chemical compounds.
1.5.1.1.4.4.8.1 GC-MS and herbal medicines
Mass spectrometry is the most sensitive and selective method for molecular
analysis and can yield information on the molecular weight as well as the
structure of the molecule (Zhang, et al. 2003 ). Combining chromatography with
mass spectrometry provides the advantage of both; chromatography as a
separation method and mass spectrometry as an identification method. In mass
spectrometry, there is a range of methods to ionize compounds and then separate
the ions. Common methods of ionization used in conjunction with gas
chromatography are electron impact (El) and electron capture ionization (ECI).
With the GC-MS, people could produce not only a chromatographic fingerprint
of the essential oil of the herbal medicine but also the information related to its
most qualitative and relative quantitative composition (Li, 2003, Velasco, 2003).
1.5.1.1.4.4.8.2 HPLC-DAD, IIPLC-MS and others
HPLC-DAD has become a common technique in most analytical laboratories in
the world now. With the additional UV spectral information, the qualitative
analysis of complex samples in herbal medicines turns out to be much easier
l·a/illlltion of rrc-raration Proct'H and nn~crprintim: nf Wm(' A_llln-ctlic f(lrmu/atiom
28
INTRODU
~---~~ than before, for instance checking peak purity and comparing with the available
standard spectrum of the known compound to the one in the investigated sample
(Zhang, et a!. 2003).
Moreover, combined HPLC-DAD-MS techniques take advantage of
chromatography as a separation method and both DAD and MS as an
identification method. DAD and MS can provide on-line UV and MS
information for each individual peak in a chromatogram. With the help of this
hyphenation, in most cases, one could identifY the chromatographic peaks
directly on-line by comparison with literature data or with standard compounds,
which made the LC-DAD-MS becomes a powerful approach for the rapid
identification of phytochemical constituents in botanical extracts, and it can be
used to avoid the time-consuming isolation of all compounds to be identified
(He, 2000).
1.5.1.1.4.4.8.3 Hyphenation of CE
The hyphenated CE instruments, such as CE-DAD, CE-MS and CE-NMR,
appeared in the past decades. The techniques have also quickly been used for the
analysis of the samples from herbal medicines (Strum, 1998, Hsieh, 1993). On-
line coupling of capillary electrophoresis to mass spectrometry and other
spectrometry allows both; the efficient separation of CE and the specific and
sensitive detection can be achieved. A "total analysis device" has been recently
demonstrated in the case of on-line HPLC-UV (DAD)-FT-IR-NMR-MS
analyses.
1.5.1.1.4.5 1\ficrobiological methods
Medicinal plant materials normally carry a great number of bacteria and moulds,
often originating in soil. While a large range of bacteria and fungi form the
J ·alidation fl[ Prrparation Prnccn and rim:crprinting of 'i(li,Jt! Ayun·cdic ronnulariom
29
INTRODU
~~~~~~ naturally occurring microflora of herbs, aerobic spore-forming bacteria
frequently predominate. Current practices of harvesting, handling and production
may cause additional contamination and microbial growth. The determination of
Escherichia coli and moulds may indicate the quality of production and
harvesting practices. Therefore to ensure the safety and quality of the herbal
preparation, specific tests for microorganisms like Escherichia coli, Salmonella
spp., Pseudomonas aeruginosa, Pseudomonas aeruginosa are performed. In
addition the total viable aerobic count and test for aflatoxins are also performed
(WHO Guidelines, 2004).
1.5.1.1.4.6 Biological methods
Biological assays (bioassays) are prescribed where the potency of a drug or its
preparation carmot be adequately determined by chemical or physical mean but
where it may be possible to observe the biological effect of the drug on some
type of living matter. The principle of such assay is to compare dose of the
sample' being tested produces the same biological effect as a given quantity of a
standard preparation. It is also important that conditions, under which the sample
and the standard preparation are tested, are identical in all respects of time,
environmental factor and biological media used (Mukherjee, 1996).
1.5.1.1.4.7 Stability studies
Shelf life of any medicine can be defined as the time period or duration up to,
which it is expected to retain its active ingredients i.e. 90% of label claim when
stored at recommended condition. Every product has its definite shelf life which
depends on various factors such as the stability of its active ingredients,
manufacturing process, interaction between active and inactive ingredients,
dosage form container closure system, environmental conditions encountered,
J ·a!id.ttion fJ/ Prrrararion PrflCt'H and rirrgrrpn·nring fl/ wmc -i.lun·t•olic r onrmlatiom
30
INTRODU
---,------:--:--:-:-----:-----~~~~ contamination with metal and microbes etc., which cause the
degradation/spoilage of the product by initiating/accelerating certain chemical
reactions such as oxidation/reductions help to stabilize the drug and for
prediction of shelf life and its optimum storage conditions (Padiyar et a!., 1998).
1.5.2 Monographic approaches on quality control and standardization
The worldwide spread in the use of herbal medicines has produced various
attempts to develop herbal monographs to define identity and quality criteria as
well as therapeutic information. The German Commission E has been publishing
therapeutic monographs since 1984. The ESCOP has been developing
therapeutic monographs since 1991 and the WHO has initiated a project to write
monographs on widely used herbs around the world. In the United Kingdom
herbal monographs have been published since 1983 (Herbal Monographs, 1997).
The word monograph means a learned treatise dealing with one subject, usually,
in the scientific community, a plant or animal genus or particular species. In the
botanical world there are essentially three kinds of monographs: standards,
therapeutic, and combined. A standards monograph, the type usually found in a
pharmacopoeia, deals with information to determine the proper identity of a
plant genus or genus and species. This includes the taxonomy and nomenclature
of the plant (according to the linnean system of botanical classification and
nomenclature, including all synonyms), botanical description of the whole plant
and plant parts, microscopic descriptions of cellular structures of various plant
parts, and various chemical assays to determine identity and purity. USP
standards monographs arc examples of this type (Herbal Monographs, 1997). A
therapeutic monograph usually provides a definition of the plant drug (i.e. plant
part. nomenclature, etc.), a listing of key chemical compounds, uses and
J 'alidation nf Preparation froccn and rim:crpdntim: njJfJmt· Aruncdic l"flrmulariom
31
INTRODU
~~---:----:-:-:--------:---~~ indications, contraindications (i.e., what conditions may be present to preclude
use of the herb), side effects, dosage (including per unit and total daily intake),
form of administration (i.e., the dosage in tea, tablet or capsule, liquid extract,
etc.), duration of use, interactions with other medications. The Drug Information
Division ofUSP has also produced two in this area (Herbal Monographs, 1997).
Then, occasionally there are combined monographs, in which both the standard
information as well as therapeutics is included. The WHO monographs and the
AHP monographs are of this type (Herbal Monographs, 1997).
Internationally several Pharmacopoeias including Indian Pharmacopoeia, British
Pharmacopoeia, Pharmacopoeia of Republic of China, Japanese Pharmacopoeia,
United State Pharmacopoeia, European Pharmacopoeia and many more have
developed monographs and quality control tests for few of medicinal plants and
some products made out of these herbs. Looking at increasing interest in the
natural raw materials, the U.K. founded British Herbal Medical Association
(BHMA) in 1964 to advance the science and· practice of herbal medicines.
BHMA published I" British Herbal Pharmacopoeia (BHP) in 1971, then in 1983
and 1996, giving monographs and quality control tests for some of the common
herbs and herbal products. Japanese standards for herbal medicines first
published in 1993. In India the first Ayurvedic Pharmacopoeia Committee
(APC) founded in 1962 and the Ayurvedic Formulary of India, first published in
1978, without giving preliminary standards for single drugs and compound
formulations due to lack of sufficient scientific data. In 1989, the first Ayurvedic
Pharmacopoeia of India came into account provided Pharmacopoeial standards
of some single drugs of plant origin (Chaudhri, 1996). USP is currently
accumulating a database of botanicals that arc approved in other national
-- ----------- -----~-----------------------------, 0/idatimr of ruparation ProcrH and llnr:crprintin.r: fi[Wnl<' A.llln·ctlic rnnnulatiom
32
INTRODU
~~~~~~ pharmacopeias to make this information available to the USP General
Committee of Revision or its advisory panels in the event that questions
regarding botanicals arise during the 1995-2000 revision cycle (Herbal
Monographs, 1997). USP has moved forward and produced monographs that
creates a USP standard for various popular herbs in US commerce six draft
standards monographs for discussion purposes in the Pharmacopoeial Forum, a
bimonthly publication ofUSP
The German Commission E: The most widely acknowledged system for the
development of therapeutic monographs is that of the German Commission E.
Commission E is a division of the German Federal Health Authority (equivalent
to our FDA). Since 1978 when it was first organized and until it was terminated
by an amendment to the Medicines Act in August 1994, the Commission E
review published 330 monographs covering 324 herbs used in German folk
medicine, approving over 200 herbs as safe and effective for over-the-counter
drug use. The 330 monographs cover more than 80 percent of the herbal
medicine products in the German market (Keller, 1996). Commission E
monographs are geared toward therapeutic information on each herb, giving the
taxonomic nomenclature, botanical and chemical constituents, pharmacological
properties, and pharmacokinetics and toxicology (in more recent monographs),
as well as clinical information, including approved uses, contraindications and
side effects, special cautions, pregnancy and lactation information, interactions
with other drugs, dosage, overdosage information, special warnings, and so on, if
these are applicable.
One of most interesting developments in the area of herbal monographs is
ESCOP, an affiliation of national associations of phytothcrapy in Western
l·ali.latiml nf ruraratiml PwccH ami rirrr:crprintinr: nf .\(1111~. h unwlic rormulatiom
33
INTRODU
~~ ;:E:-u-ro_p_e_w--;h_o_c_o"""'al:-e-sc-e--;d:-:-in---:lc::9::;8:;;9-as-a-re-s-u""lt-of-;;-:t""h-e """"'E:::-u_r_o-pe-an-7h-arm-onization
process. ESCOP has produced a series of herbal monographs in order to respond
to the increasing integration of what was formerly called the European Economic
Community (now European Union, or EU). The need for harmonized drug
monographs for herbs was recognized so that there could be standards for
botanicals popularly used in medicine and pharmacy in Europe. Unlike a
Pharmacopoeial monograph which focuses on standards for identity and quality,
ESCOP monographs, like those of the German Commission E, deal with
therapeutic aspects of each phytomedicine. Thus, ESCOP monographs include
approved therapeutic uses and contain much of the format like recent
Commission E monographs, including recommended dosage, side effects and
contraindications (if any), and other specific instruction, to help guide health
professionals, industry, regulators, and patients (Blumenthal, 1991). ESCOP
monographs do not deal with quality issues; this is covered in other
Pharmacopoeial monographs. For example, the European Pharmacopoeia
includes 60 monographs on herbal drugs. An additional 45 draft monographs
have been published in the Pharmeuropa for comments.
WHO monographs: In 1994 WHO began the compilation of a list of herbs that
are widely used in primary health care in various countries around the world in
order to consider developing monographs on each botanical (Herbal
Monographs, 1997). This move is consistent with WHO's previous publication
of its "Guidelines for the Assessment of Herbal Medicines," calling for the
development of monographs to help define the quality of herbal medicines used
as either "traditional medicines" and/or as approved nonprescription (over-the-
counter) drugs. A list of 30 plant species is being considered for the second
------------------------------J "a!idarimr nf rrcraration Pr(JCC\\ an.lli"m:rrrrinrin.r: nf \nmt•. fyun·cdic rormu/atiom
34
INTRODU
~~~,------------,-~~ volume (Herbal Monographs, 1997). 25 monographs encompassing 28 plant
species on WHO's "Widely Used Medicinal Plants" list are scheduled to be
published in book form as Volume I in 1997. The herbs represent widely used
herbs and medicinal plants from various geographical regions.
American Herbal Pharmacopoeia: In 1977 Prof. Farnsworth proposed to the
American Society of Pharmacognosy (ASP) that it develop a Botanical Codex, a
listing of monographs describing and offering analytical standards for the herbs
and medicinal plants that were becoming increasingly popular in folk medicine
and commerce in the U.S. The AHP monographs are combined monographs;
they include much of the standard definitional and analytical information found
in conventional Pharmacopoeial monographs on standards, plus therapeutic and
clinical information. However, AHP goes a step further with the inclusion of the
Chinese and Ayurvedic energetic information not found in standard Western
pharmacopeias and clinical literature on herbs (Herbal Monographs, 1997).
The availability of various types of herbal monographs will fill up the current
need for information on quality control and safe, responsible uses of herbal
products. As the industry continues to grow at record levels, the industry's use of
the information in herbal monographs will ultimately help health consumers by
making available herbal products of increased quality and reliability.
l·alhlation (If frrparation Procrn m~;J firrr:aprinting of wmt-• A.Jun·t•dic romrulatiom
35
INTRODU
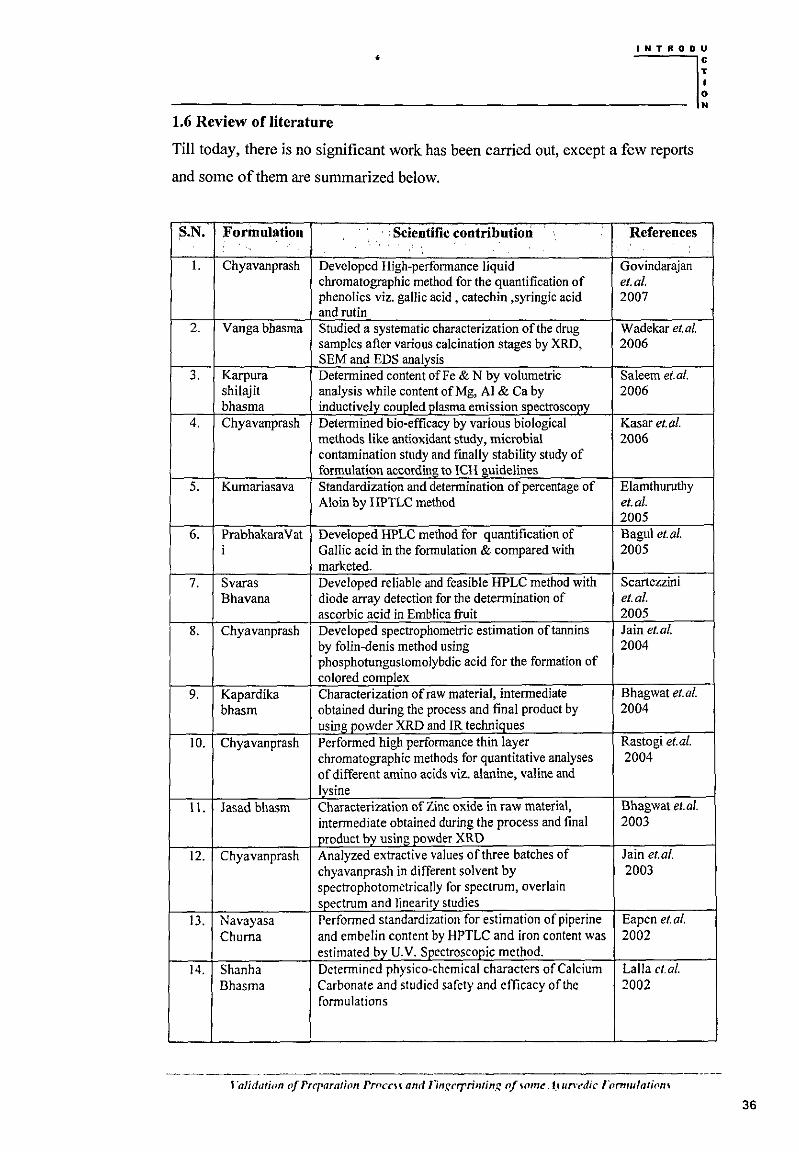
---------·-----------~~ 1.6 Review of literature
Till today, there is no significant work has been carried out, except a few reports
and some of them are summarized below.
S.N. Formulation · • Scientific contribution References
I. Chyavanprash Developed High-performance liquid Govindarajan chromatographic method for the quantification of et.al. phenolics viz. gallic acid , catechin ,syringic acid 2007 and rutin
2. Vanga bhasma Studied a systematic characterization of the drug Wadekar et. a/. samples after various calcination stages by XRD, 2006 SEM and EDS analysis
3. Karpura Determined content of Fe & N by volumetric Saleem et. a/. shilajit analysis while content of Mg, AI & Ca by 2006 bhasma inductively coupled plasma emission spectroscopy
4. Chyavanprash Determined bio-efficacy by various biological Kasar et.al. methods like antioxidant study, microbial 2006 contamination study and fmally stability study of formulation according to ICH guidelines
5. Kurnariasava Standardization and determination of percentage of Elamthuruthy Aloin by HPTLC method et.a/.
2005 6. Prabhakara Vat Developed HPLC method for quantification of Bagul et.al.
i Gallic acid in the formulation & compared with 2005 marketed.
7. Svaras Developed reliable and feasible HPLC method with Scartezzini Bhavana diode array detection for the determination of et.a/.
ascorbic acid in Emblica fruit 2005 8. Chyavanprash Developed spectrophometric estimation of tannins Jain et.al.
by folin-denis method using 2004 phosphotungustomolybdic acid for the formation of colored complex
9. Kapardika Characterization of raw material, intermediate Bhagwat et.al. bhasm obtained during the process and final product by 2004
using powder XRD and IR techniques 10. Chyavanprash Performed high performance thin layer Rastogi et.a/.
chromatographic methods for quantitative analyses 2004 of different amino acids viz. alanine, valine and lysine
11. Jasad bhasm Characterization of Zinc oxide in raw material, Bhagwat et.a/. intermediate obtained during the process and final 2003 product by using powder XRD
12. Chyavanprash Analyzed extractive values of three batches of Jain et.al. chyavanprash in different solvent by 2003 spectrophotometrically for spectrum, overlain spectrum and linearity studies
13. Navayasa Performed standardization for estimation of piperine Eapen et.al. Chuma and em be lin content by HPTLC and iron content was 2002
estimated by U.V. Spectroscopic method. 14. Shanha Determined physico-chemical characters of Calcium Lalla ct. a/.
Bhasma Carbonate and studied safety and efficacy of the 2002 formulations
l'alidation (If Prt'raration Prnccu anrl lln.r:crrrimin,r: nf \Om<!. t.1 un-cdic /Omrulathm\
36
INTRODU
~! N
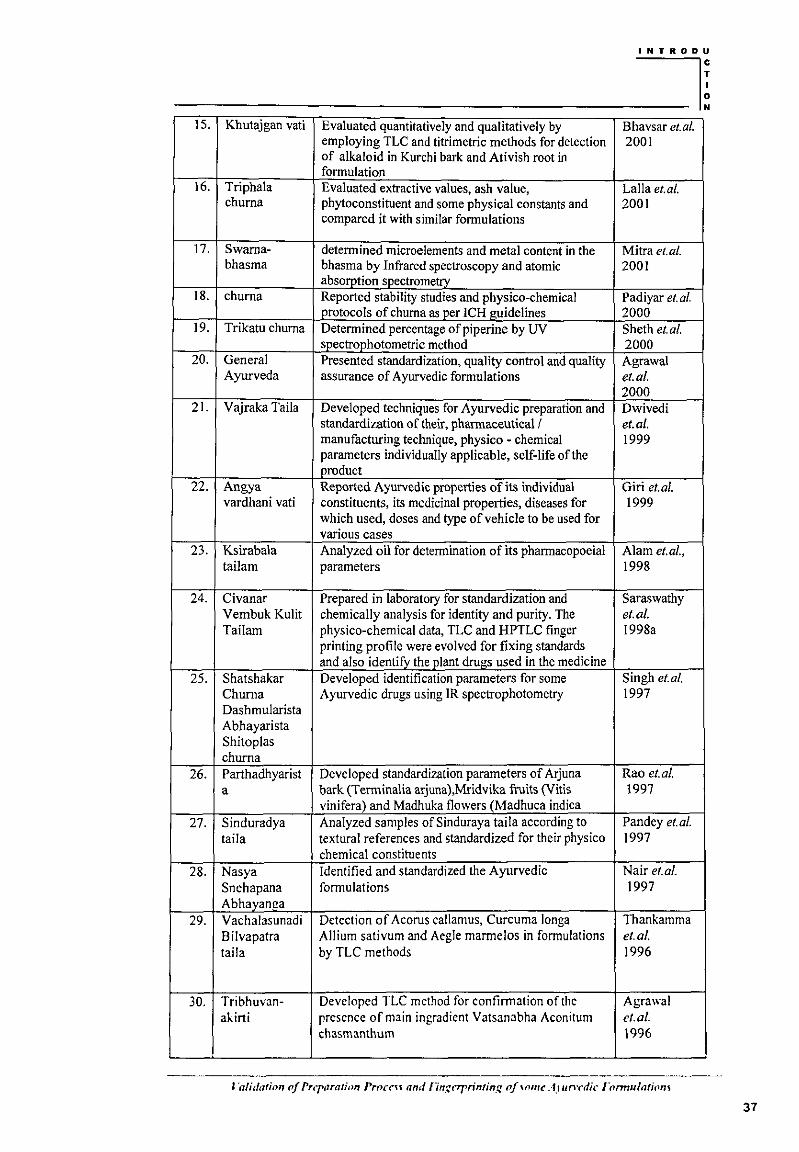
1 s. Khutajgan vati Evaluated quantitatively and qualitatively by Bhavsar et. a/. employing TLC and titrimetric methods for detection 2001 of alkaloid in Kurchi bark and Ativish root in formulation
16. Triphala Evaluated extractive values, ash value, Lalla et. a/. chum a phytoconstituent and some physical constants and 2001
compared it with similar formulations
17. Swama- determined microelements and metal content in the Mitra et. a/. bhasma bhasma by Infrared spectroscopy and atomic 2001
absorption spectrometry 18. chum a Reported stability studies and physico-chemical Padiyar et. a/.
protocols of chuma as ]JOr ICH guidelines 2000 19. Trikatu chuma Determined percentage of piperine by UV Sheth et.al.
spectrophotometric method 2000 20. General Presented standardization, quality control and quality Agrawal
Ayurveda assurance of Ayurvedic formulations et.a/. 2000
21. Vajraka Taila Developed techniques for Ayurvedic preparation and Dwivedi standardization of their, pharmaceutical/ et. al. manufacturing technique, physico - chemical 1999 parameters individually applicable, self-life of the product
22. Angya Reported Ayurvedic properties of its individual Giri et.al. vardhani vati constituents, its medicinal properties, diseases for 1999
which used, doses and type of vehicle to be used for various cases
23. Ksirabala Analyzed oil for determination of its pharmacopoeial Alam et.a/., tail am parameters 1998
24. Civanar Prepared in laboratory for standardization and Saraswathy Vembuk Kulit chemically analysis for identity and purity. The et.a/. Tailam physico-chemical data, TLC and HPTLC finger 1998a
printing profile were evolved for fixing standards and also identifY the plant drugs used in the medicine
25. Shatshakar Developed identification parameters for some Singh et. a/. Chuma Ayurvedic drugs using IR spectrophotometry 1997 Dashmularista Abhayarista Shitoplas chum a
26. Parthadhyarist Developed standardization parameters of Arjuna Rao et.al. a bark (Terminalia arjuna),Mridvika fruits (Vitis 1997
vinifera) and Madhuka flowers (Madhuca indica 27. Sinduradya Analyzed samples of Sinduraya taila according to Pandey et.al.
tail a textural references and standardized for their physico 1997 chemical constituents
28. Nasya Identified and standardized the Ayurvedic Nair et.al. Snehapana formulations 1997 Abhayanga
29. Vachalasunadi Detection of Acarus callamus, Curcuma longa Thankamma Bilvapatra Allium sativum and Aegle marmelos in formulations et.al. tail a by TLC methods 1996
30. Tribhuvan- Developed TLC method for confirmation of the Agrawal akini presence of main ingradicnt Vatsanabha Aconitum ct. a/.
chasmanthum 1996
l'a/idation nf Prrr(1rarion Procrn and lln.ccrprinting of,nmt A.1 urwdic romrulatiom
37
INTRODU
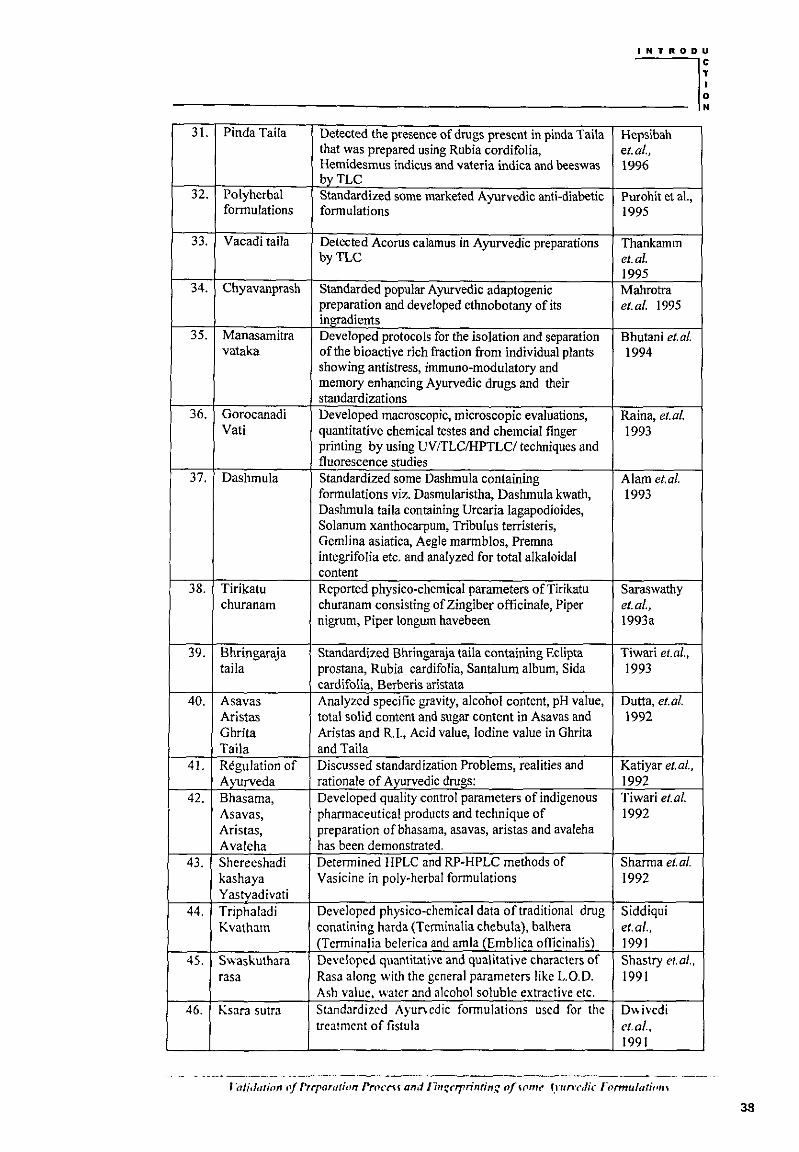
----~~ 31. Pinda Taila Detected the presence of drugs present in pinda Tai!a Hepsibah
that was prepared using Rubia cordifolia, et.a/., Hemidesmus indicus and vateria indica and beeswas 1996 byTLC
32. Polyherbal Standardized some marketed Ayurvedic anti-diabetic Purohit et al., formulations formulations 1995
33. Vacadi taila Detected Acorus calamus in Ayurvedic preparations Thankamm byTLC et.a/.
1995 34. Chyavanprash Standarded popular Ayurvedic adaptogenic Mahrotra
preparation and developed ethnobotany of its et.al. 1995 ingradients
35. Manasamitra Developed protocols for the isolation and separation Bhutani et. a/. vataka of the bioactive rich fraction from individual plants 1994
showing antistress, immuno-modulatory and memory enhancing Ayurvedic drugs and their standardizations
36. Gorocanadi Developed macroscopic, microscopic evaluations, Raina, et. a/. Vati quantitative chemical testes and chemcial finger 1993
printing by using UV /TLCIHPTLC/ techniques and fluorescence studies
37. Dashmula Standardized some Dashmula containing Alam et.al. formulations viz. Dasmularistha, Dashmula kwath, 1993 Dashmula taila containing Urcaria lagapodioides, Solanum xanthocarpum, Tribulus terristeris, Gemlina asiatica, Aegle marmblos, Premna integrifolia etc. and analyzed for total alkaloidal content
38. Tirikatu Reported physico-chemical parameters ofTirikatu Saraswathy churanam churanam consisting of Zingiber officinale, Piper et.al.,
nigrum, Piper longum havebeen 1993a
39. Bhringaraja Standardized Bhringaraja taila containing Eclipta Tiwari et.al., tail a prostana, Rubia cardifolia, Santalum album, Sida 1993
cardifolia, Berberis aristata 40. A sa vas Analyzed specific gravity, alcohol content, pH value, Dutta, et.al.
Aristas total solid content and sugar content in Asavas and 1992 Ghrita Aristas and R.I., Acid value, Iodine value in Ghrita Taila and Taila
41. Regulation of Discussed standardization Problems, realities and Katiyar et.al., Avurveda rationale of A vurvedic drugs: 1992
42. Bhasama, Developed quality control parameters of indigenous Tiwari et. a/. As a vas, pharmaceutical products and technique of 1992 Aristas, preparation ofbhasama, asavas, aristas and avaleha Avaleha has been demonstrated.
43. Shereeshadi Determined HPLC and RP-HPLC methods of Sharma et. a/. kashaya Vasicine in poly-herbal formulations 1992 Yastvadivati
44. Triphaladi Developed physico-chemical data of traditional drug Siddiqui Kvatham conatining harda (Terminalia chebula), balhera et.a/.,
(Tcrminalia belerica and amla (Emblica omcinalis) 1991 45. Swaskuthara Developed quantitative and qualitative characters of Shastry et.al.,
rasa Rasa along with the general parameters like L.O.D. 1991 Ash value, water and alcohol soluble extractive etc.
46. Ksara sutra Standardized Ayuncdic formulations used for the D" ivcdi treatment of fistula ct. a/ ..
1991
-. ·- -- .. ---------------------------- -----------· J 'a/idatinn fJ/ rrrraration PrfJCt"H and f7rtr;cf'{'rintin.r: of Hlfrl~ fyun·cdic romru/atiom
INTRODU
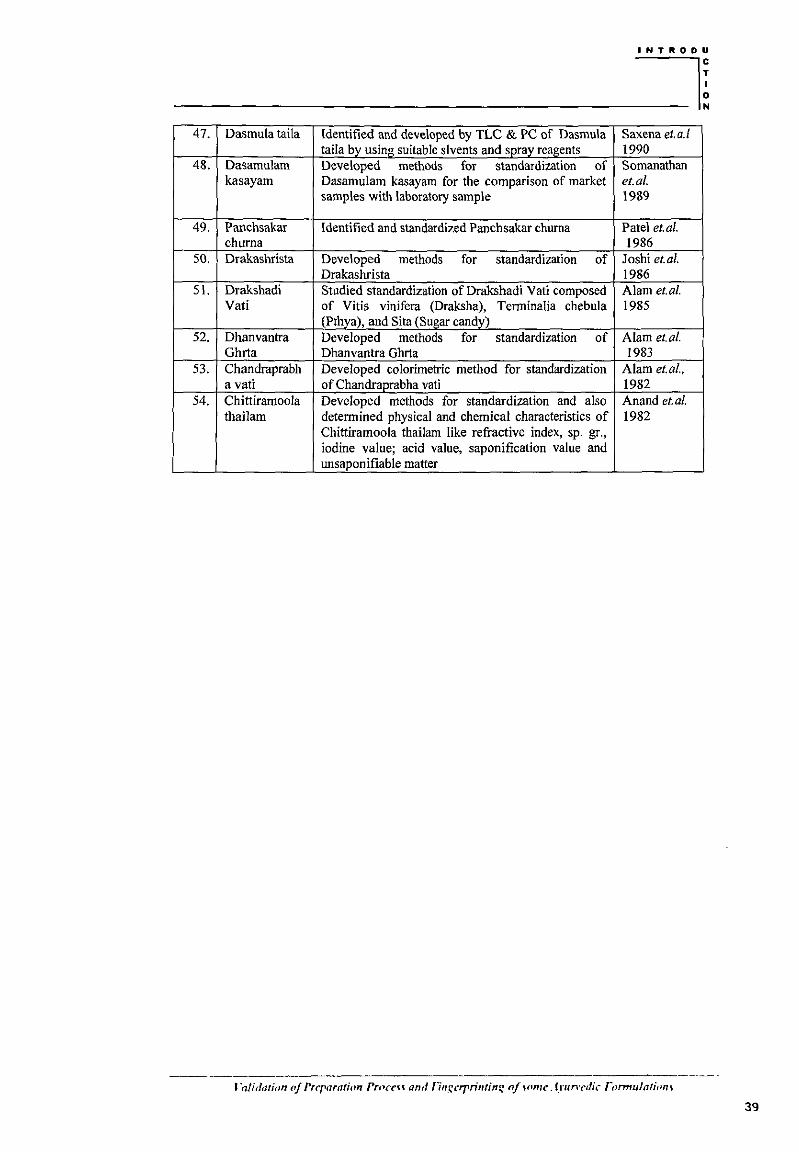
----~~ 47. Dasmula taila Identified and developed by TLC & PC of Dasmula Saxena et. a. I
taila by using suitable slvents and spray reagents 1990 48. Dasamulam Developed methods for standardization of Somanathan
kasayam Dasamulam kasayam for the comparison of market et.al. samples with laboratory sample 1989
49. Panchsakar Identified and standardized Panchsakar chuma Patel et.al. chuma 1986
50. Drakashrista Developed methods for standardization of Joshi et.al. Drakashrista 1986
51. Drakshadi Studied standardization ofDrakshadi Vati composed Alam et.al. Vati of Vitis vinifera (Draksha), Terminalia chebula 1985
(Pthya), and Sita (Sugar candy) 52. Dhanvantra Developed methods for standardization of Alam et.al.
Ghrta Dhanvantra Ghrta 1983 53. Chandraprabh Developed colorimetric method for standardization Alam et.al.,
a vati of Chandraprabha vati 1982 54. Chittiramoola Developed methods for standardization and also Anand el. a/.
thailarn determined physical and chemical characteristics of 1982 Chittiramoola thailam like refractive index, sp. gr., iodine value; acid value, saponification value and unsapouifiable matter
··a/idarion of Preparation rrr'CCH and fl~t.r:crrrintinr: nf Hlmt". fyun·cdic Tormulatiom
39
INTRODU
----~~ 1. 7 Research envisages and plan of work
In the last few decades there has been an exponential growth in the field of
herbal medicine. It is getting popularized in developing as well as in developed
countries owing to its natural origin and lesser side effect.Traditionalfherbal
medicines, which formed the basis of health care throughout the world since the
earliest days of mankind are still widely used, and have considerable importance
in international trade.
Ayurveda is an ancient and popular form of holistic medicine system originated
in India and now spreading worldwide. In Ancient time when the ayurvedic
medicines were developed, preparation, standardization and quality control of
ayurvedic formulation maintained by fully committed professionals. The
traditional ayurvedic text claims that ayurvedic formulation prepared according
to the method given in ayurvedic text will superior in quality, safety, and
efficacy. Process of preparation hold significant role in effectiveness and quality
of ayurvedic formulations. Process validation is "a documented program which
provides a high degree of assurance that a specific process will consistently
produce a product meeting its predetermined specification and quality
attributes". The quality of pharmaceuticals has been a concern of the World
Health Organization (WHO) since its inception. Many international authorities
and agencies including the European Agencies for the evaluation of medicinal
product and European Scientific Co-operation of phyto-medicine, U.S. Agencies
for Health Care Policy and Research, European Pharmacopoeia Commission,
Department of Indian System of Medicine and such have started creating a new
mechanism to induce a quality control and standardization of botanical and
ayurvcdic medicine. It is absolutely necessary to develop reliable analytical
J ·alidttlimr ''~ frcparatirm rr,.CC\t and ringcrpn·nring ll/ .~flm,; Ayun·cdic r ()nttulation~
40
INTRODU
---:;--;----;--~~~~~ methods in order to control the quality of herbal medicines. Fingerpnnt
technique was introduced and accepted by WHO as a powerful tool for
identification and quality evaluation of multi -component herbal/traditional
medicines. Ayurvedic formulations cover wide range of product from solid to
semisolid to liquid dosage forms. There fore the formulations were selected from
each dosage forms. The selected formulation for present research work has taken
by discursive attempts of studying various classical literatures. The identified
formulations are enlisted in the essential drug list declared by Central Council of
Ayurveda. The formulation was selected in the list are available in each
ayurvedic dispensaries from metro to micro interiors. The present work is an
approach to develop preparation process validation and fmgerprinting for some
formulations viz Arjunaristha (AJR), Vasavleha (VSL), Bhaskar Iavan chuma
(BLC), and Chyavanprash (CHY), which are official in Ayurvedic Formulary of
India.
l·a!idt1timr nf Prrraratirm Prnccu and 1/m:rrprintinr: ofwm<' Arun·<·dic rnrmu/atinm
41
INTRODU
----~~ 1.7.1 Candidate formulation
Arjunaristha
Arjunaristha is a well known ayurvedic formulation described in ayurvedic text
Charak-Samhita, Bhaisajyaratnawali and Ayurvedic formulary of India. It is a
potent ayurvedic medicine containing self-generated alcohol used as general
tonic for heart disease, lung diseases, loss of strength, immunomodulator and in
azoospermia. Aristhas are classical ayurvedic liquid dosage form made by
soaking the drugs (powder or decoction) in a solution of jaggery for a specified
period of time, which undergoes a fermentation process to generating alcohol,
thus facilitating the extraction of active principles contained in the drug(s). The
alcohol generated, also serves as a preservative.
Vasavleha
Vasavleha is a well known ayurvedic formulation prescribed in Ayurvedic
formulary of India and in classical ayurvedic texts Bhaisajyaratnawali, and
Charak Samhita. It is used for Asthma, cough, fever, angina pectoris and for
abdominal pain. Vasavleha falls under the category of Avaleha-paka group of
ayurvedic formulations. The main components are Piper longum and Adhatoda
zeylenica. Method of preparation for avaleha-paka group of ayurvedic
formulations is very tedious and plays a vital role in quality, and efficacy of any
formulations.
Bhaskar Iavan churna
The Bhaskar Iavan churna, a well known formulation described in Ayurvedic
formulary of India, traditionally used for digestive impairment, rheumatism,
dyspepsia, malabsorption syndrome, angina pectoris, disease of skin, splenic
disorder, oedema, asthma and constipation. Among all the ayurvedie medicine
J 'alit!ation nf Preparation rrnccu and llngc·rrrimim: nf \Onlt*. trunwlic rnrmulatiotl\
42
INTRODU
fO< tho ga<ro '""-""'' dl""'b'"" Bh""'M Ia- chama;, llia mo.t relabc&ol 11 by the ayurvedic practitioners of India. It falls under the category of Churna in
ayurvedic formulation.
Chyavanprash
Chyavanprash is a very commonly used ayurvedic medicine and health
supplement since centuries. It is reputed as antioxidant, nervine tonic, anxiolytic
having adaptogenic activity. In modern time it acts as immunomodulator,
memory enhancer, growth promoter in children's and digestive fire improver.
Administration of this r~uvenation therapy promotes intellect, memory, luster,
immunity to diseases, longevity, strength of sense organs, sexual excitement,
great stimulation of digestive and clarity of complexion. Chyavanprash falls
under the category of avaleha-paka group of ayurvedic formulations. Method of
preparation for avaleha-paka group of ayurvedic formulations is very tedious
and plays a vital role in quality, and efficacy of any formulations. The entire
Indian market for Chyavanprash stands about 50-60 tones, even though very few
quality control methods for its evaluation has been attempt. Till date no work
were carried out in the field of validation of preparation process for assuring the
quality and consistency with methods for fingerprinting of the most popular
ayurvedic formulation.
43
INTRODU
----~~ 1.7.2 Plan ofwork
The present study is an approach to develop, preparation process validation and
fingerprinting methods for some identified ayurvedic formulations that are
official in Ayurvedic Formulary of India. In order to achieve this objective
following studies have been undertaken:
>- Preparation of selected formulations and bifurcation of process m
different stages.
>- Validation of preparation process of different stage samples and finished
formulations.
>- Development of quality control parameter of formulation and their
validation.
>- Development of finger print method of formulation using sophisticated
instrument.
>- Evaluation of marketed formulation and comparison with the laboratorv
formulation.
>- Stability studies of laboratory formulation.
------------------------ ---·-----------' ·alidarimt fl[ Prrraratimt ProccH and riTt::crrrimin.~ of wmc Ayunwlic r flrmulatinn"i
44
INTRODU
_R_E_F_E_R_E_N_C_E_S _____ ~~ + Agarwal BL, Agarwal AK. Modem Text Book of Analytical chemistry. 3rd
ed. Agra: Universal book depot; 1979:213-28.
+ Agrawal RG, Joshi PC, Pandey MJ, Pandey G. Ancient Science of Life
I 996; I 5(3): 169-71.
+ Alam M, Sarawathy VN, Venugopalan lN, Jaya N, Namboodiri PKN,
Ramarao B. Aryavidyan 1998;11(3):164-67.
+ Alam M, Dasan KKS, Rukmani B, Purshothaman KK. Bull. Med. Ethnobot.
Res. I 985;6(2-4):133-40.
+ Alam M, Dasan KKS, Sathiavasan K, Purshothaman KK. Bull. Med.
Ethnobot. Res. I983;4(3-4):I58-61.
+ Alam M, Rukmani B, Meenakshi N, Dasan KKS, Bhima Rao R. J. Res.
Ayur. Siddha I993;I4(1-2):68-73.
+ Alam M, Sathiavasan K, Varadarajan TV, Shanmugadhasan KK,
Purshothaman KKA. J.Res.Ayur.Siddha I 982;3(3-4):216-20.
+ Anand KA, Thirugunana sambanatham P, Rajendran V, Muralidharan, R,
Balasubramanian M. J. Res. Ayur. Siddha I982;3(3-4):200-04.
+ Ayurveda Sarsangrah. 20th ed. Nagpur: Shri Baidhnath Ayurveda Bhawan ltd.;
2000: I -131.
+ Bagul M S, Rajani M. Indian drugs 2005;42(1):15-19.
+ Bah! BS, Bah! A. Advanced Organic Chemistry. 3rd ed. New Delhi: S.
chand and company ltd.; 200 I: 1316-20.
+ Beckett AH, Stenlake JB. Practical Pharmaceutical Chemistry. Part I, 4th ed.
New Delhi: CBS publishers and distributors; 2000:176-97.
+ Bhagwat M, Kashalkar RV, Bhavc AS , Vaidya SS, Ramaswami V. Indian
drugs 2004; 14(4):207-13.
J ·a/idation r{ Prrpnrathm Proccn and Tingcrrrinting nf !>nme. frun cdic TlJrmulation'l
45
INTRODU
~~~~~~ + Bhagwat M, Kashalkar RV, Bhave AS, Vaidya SS, Ramaswami V. Indian
drugs 2003;41(1):12-18.
+ Bhavsar GC, Pundrikakshudu K, Kudalkar VP, Patel RK. Indian J. Nat.
Prod. 2001;20(1):33-35.
+ Bhutani KK, Gupta DK, Kapil RS. Update Ayurveda 1994; 52-62.
+ Blumenthal M. HerbalGram 1991;24: 41-43.
+ Bodekar G, Kronenberg F. Am. J. Public Health 2002;92:1582-91.
+ Braun RD. Introduction to Instrumental Analysis. Internal ed. Singapore:
McGraw-Hill book company; 1987:136-70.
+ Brinckmann J, Mcintyre M. HerbalGrarn 2006;70:62-66.
+ British Pharmacopoeia. vol. II, United Kindgom: The stationary office ltd;
1998: AppendixXIEA 181.
+ Cardellina JH. J. Nat. Prod. 2002;65:1073-084.
+ Chaudhari RD. Herbal Drug Injuries. 1st ed. New Delhi: Eastern publisher;
1996:491-509.
+ Dharmananda S. The Ayurvedic Medicine Industry in India. 2004. Available
from: URL www.itmonline.com
+ Dutta SK. International Seminar on Traditional Medicine. 1992;69-70;
Calcutta.
+ Dwivedi AK, Chaudhary M, Kulshreshtha DK, Sarin JPS. J. Res. Ayur.
Siddha 1991; 12(1-2):85-92.
+ Dwivedi PK, Pandey S, Jha CB. Sachitra Ayurveda 1999;51(7):541-43.
+ Eapen Saumy MS, Grampurohit ND. Indian drugs 2002;39(2):101-05.
+ Edwards EJ, Cobb AH. Journal of Agricultural and Food Chemistry 1996;44
(9):2705-09.
~~~-- --------~-----------------· --- ---~---
l·alidatinn fl/ Prt"r11ration PrflCC\~ atr.f !lngaprinrin.r: of \nnu• A runw/ic rnrmulatwm
46
INTRODU
------~~ + Kasar R, Laddha KS, Chaudhary J, Shukla A. Nat Prod Radience 2006;
5(1 ):33-41.
+ Katiyar CK, Bittal Babu A, Narayana DBA. International Seminar on
Traditional Medicine. 1992; 69; Calcutta.
+ Keller K. Pflanzliche Arzneimittel - rechtlicher Status und offene
Forschungsfragen. Forschungsmagazin der Johannes Gutenberg UniversiUit
Mainz, Sonderausgabe Naturheilkunde 1992:59-68.
+ Lalla JK, Hamrapurkar PD, Mamania HM. Indian drugs 2001;38(2):87-94.
+ Lalla JK, Harnrapurkar PD, Patil PG, Mamania HM. Indian drugs
2002;39(3): 152-56.
+ Leung A Y. Encyclopedia of Common Natural Ingredients Used in Food,
Drugs and Cosmetics. 2nd ed. New York-Chichester: Wiley; 1980.
+ Mabey R. The Complete New Herbal. 4th ed. London: Elm Tree Books;
1988:182-95.
+ Mahrotra S, Rawat AKS, Singh HK, Shome U. Ethanobotony
1995;7(1&2): 1-15.
+ Martindale. The Complete Drug Reference, 32nd ed. London: The
Pharmaceutical Press; 1999.
+ McGhie TK. J. Chromatogr. 1993; 634:107-13.
+ Mendham J, Denney RC, Barnes JD, Thomas M. Vagal's Textbook of
Quantitative Chemical Analysis. 6th ed. New Delhi: Pearson education pvt.
ltd.; 2002:251-720.
+ Mitra A, Chakraboty S, Auddy B, Triphati P, Sen S, Saha AV, Mukherjee B.
Journal of Ethnopharmacognosy 2002;80: 14 7-53.
• Mukherjee PK. Quality control of Herbal Drugs. 1st ed. New Delhi:
Horizons Pham1aceutica! Publishers; 2002:1-8 I 6.
J 'a/idatiolt flj Preparation Proccu ami /'in.r.:crprintin~ of.,omc Ayunt•dic r nnnu/atiom
48
INTRODU
N KV . . ~j + mr , Nair AR, Nair CPR. Bull. Med. Ethnobot. Res. 1997;18(3-4):151-
56.
+ Padiyar A, Ali J, Khar RK. Pharma times 2000;30(8):35-38.
+ Pandey NN, Yadav RS, Sharma GK. Sachitra Ayurved 1997;49(12):937-40.
+ Patel BR, Patel KG, Thomas PJ. Abstracts of Papers Presented at 38th !PC;
1986; Ahmedabad, India.
+ Patwardhan B. Indian drugs 2000; 37(5):213-26.
+ Purohit AP, Bosale PH. International Seminar on Recent Trends in Pharm.
Sci. 1995; Ootacmnund; A44.
+ Raina MK. Indian J. Nat. Prod. 1993; 9:18-22.
+ Rao VN, Jha CB, Maheswar T, Sahai M. Sachitra Ayured 1997;49(11):855-
57.
• Rastogi S, Bala S, Govindrajan R, Shukla M, Mehrotra S. Indian J. Pharm.
Sci. 2004;66(6):753-57.
+ Ravishankara MN, Shrivastava N, Padh H, Rajani M. Planta medica
2001;67:294-96
+ Remington's Pharmaceutical Sciences. 19th ed. Pennsylvania: Mack
publishing company; 1980:82-89.
+ Robert M, Silverstein FX. Spectrophotometric Identification of Organic
Comounds. 6th ed. New York: John Wiley & Sons; 2002:217-49.
+ Saleem AM, Gopal V, Rafiullah MRM, Bharathidasan P. Afr. J Traditional,
complementary and Alternative medicines 2006;3(2):27-36.
+ Samanta MK, Wagh VD, Prduhviraju D, Suresh B. Indian J. Pharm. Educ.
2004;38( I ):16-18.
+ Sane RT. Indian drugs 2002;39(3): 184-90.
J fl!idmiml nf Prt'rflration Proccu and nm:aprinring of WNif!' tyun·c·dic ronrmlatiom
49
INTRODU
----::----:-------~~ + Sanyal U, Bhattacharyy S, Patra A, Hazra B. J. Chromatogr. A 2003;
1017:225.
+ Saraswathy A, Girija RM, Shankari R. J. Res. Ayur. Siddha 1993;14(3-
4):174-78.
+ Saraswathy A, Girijarani M, Suganthan J. Bull. Med. Ethnobot. Res. 1998a;
19(3-4):165-75.
+ Saxena RB, Dholikia MV. Bull. Med. Ethnobot. Res. 1990;11(4):84-95.
+ Scartezzinia P, Antognonia F, Raggib MA, Polia F, Sabbionib C. J.
Ethnopharmacology 2006;104(1-2):113-18.
+ Sharma A, La! K, Handa SS. Int. J. Pharmacognosy 1992; 30(3):205-08.
+ Shastry MS, Dave KK, De S. J. research & education in Indian medicine
1991; 1 0(1 ):31-34.
+ Sheth A, La! K, Handa SS. Phytochem. Anal. 2000; 3:129.
+ Shihabi ZK, Kute T, Garcia LL, Hinsdale M. J. Chromatogr. A
1994;680: 181-87.
+ Siddiqui SH, Zaidi SJH, Khan G, Sharma HD. Ind. J. Unani Med.
1991; I (l ):37-42.
+ Singh J, Rarnprakash L, Indian drugs 1997; 34(6):360-61.
+ Stockigt J, Sheludko Y, Unger M, Gerasimenko I, Warzecha H, Stockigt D.
J. Chromatogr. A 2002; 967:85-89.
+ Strum S, Stuppne H. Electrophoresis 1998; 19:3026.
• Thanawiroon C, Linhardt RJ. J. Chromatogr. A 2003; 1014:215-17.
• Thankamma A, Radhika LG, Saudamini C. Ancient science of Life 1995;
14(4):276-80.
J 'a/idation fl/ rrcpt1rafion ProC<'H and lln.r:crpn'ntim: of wm(. tyun•t•dic r ormufarinn'l
50
INTRODU
~---~~ + Thankamma A, Radhika LG, Saudamini C. J. Res. Ayurveda Siddha 1996;
17(1-2):98-1 04.
+ The Ayurvedic Formulary of India. Part I, 1st ed. Delhi: Govt. of India,
Ministry of Health and Family Planning, Dept. of Health; 2003:381-398.
+ The Ayurvedic Formulary of India. Part II, 1st ed. Delhi: Govt. of India,
Ministry of Health and Family Planning, Dept. of Health; 2000:385-413.
+ The Pharmacopoeia of India. 2nd ed. Delhi: Manager of publications Govt.
oflndia; 1966: Appendix XXXI, XXXII: 971-85.
+ Tiwari SK, Pattanshetty JK, Pushpalatha H. J. Res. Ayur. Siddha 1993; 14(1-
2):83-87.
+ Unger M, Stockigt D, Belder D, Stockigt J. J. Chromatogr. A 1997;767:263-
68.
+ Yoga! HG. J. Ethnopharmacology 1991;35(2):179-90.
+ Wadekar MP, Rode CV, Bendale YN, Patil KR, Gaikwad AB, Prabhune AA.
J. Pharrn. Biomed. Anal. 2006:1473-78.
+ WHO Guidelines for formulation of national policy on herbal medicines -<A~ .. 4:. --. ~
I. <ti /' ' ' e. r . Alexandria, Eastern Mediterranean 1994:45-47. ' ;
.,,; I
' ~ "(TII~.(IJ.If.) + WHO Guidelines, Quality control methods for medicinal plant mate~S-\
·.~I.. _/ ' ~>l> .._,_,~ ,..,.
Geneva, 2004: 3-70. · .. ~ \11''!01 ~, ' - /. ----~"""
+ WHO, Expert committee on specifications for pharmaceutical
preparations, Thirty-fourth report. Geneva, 1996: 863:178-84.
+ WHO, Guidelines for formulation of national policy on herbal medicines.
Alexandria, 1994:16-36.
+ WHO, Guidelines for the assessment of herbal medicines. Geneva, 1991: 33-
"T ?..2 q'!(' 39. ll!]l!ll]I[D:[U I
T 22470
J ·a!idatinn nf Prt'paration Prncrn and rin_r:t'rpn"ntin_r: of some Ayun-(•dic Tnnnulatiom
INTRODU
~---~~ + WHO, Legal status of traditional medicine, complementary/alternative
medicine: a worldwide review. Geneva, 2001:12-17.
+ WHO, Quality control methods for medicinal plant materials. Geneva
1998a: 1-25.
+ WHO, Regulatory situation of herbal medicines a worldwide review Geneva
1998b: 64-96.
+ WHO, Research guidelines for evaluating the safety and efficacy of herbal
medicines. Manila, 1994a: 17-24.
+ WHO, Traditional medicine programme 2000:18-32.
+ WHO, Traditional medicine strategy 2002-2005:6-86.
+ WHO, Traditional medicines and modem health care 1990:12-18.
+ Willard HH, Merritt LL, Dean JA, Settle FA. Instrumental Methods of
Analysis. 7th ed. New Delhi: CBS publishers and distributors;
1986:290,425,499.
+ Zhang X, Yu MJC. J. Chromatogr. Sci. 2003;41 :241-45.
J ·alidmion lif Preparation Proc(H and rim;crpn'ntim; o[Hm,,• AJIInt•dic Tflrmulatiom
52
![t'.t,'t,u, '|/ i 20., ')',,'!,'i,!' file"i]''- -.. - "r,W8:Form ro :z s Ir fllB.t'f ittjrli rii I,t ii#tr :it#-$ffi h I [t ff lpfl]], {l;,",+i(',"'''tlY-',Jj/I"'t t'.t,'t,u, '|/ i](https://img.pdfslide.net/doc/110x75/5cd1d09a88c993a34d8b6674/tttu-i-20-i-quoti-rw8form-ro-z-s-ir-fllbtf.jpg)