Embed Size (px)
Citation preview
Katie Davis
KNH 411
Mrs. Matuszak
Case Study 5 – Myocardial Infarction
Mr. Klosterman, a 61-year-old man, is admitted through the emergency department of
University Hospital after experiencing a sudden onset of severe precordial pain on the
way home from work. Mr. Klosterman is found to have suffered a myocardial
infarction and is treated with an emergency angioplasty of the infarct-related artery.
I. Understanding the Disease and Pathophysiology
1. Mr. Klosterman had a myocardial infarction. Explain what happened to his heart.
Myocardial infarction refers to the necrosis, or cell death, of the myocardial cells, which
are cells found in the muscle tissue of the heart, that happens as a result of oxygen
deprivation (Mahan, Excott-Stump, & Raymond, p. 743). Oxygen deprivation is most
likely caused by the development of an atherosclerotic plaque that caused restriction of
blood flow to the heart that was severe enough to cause the myocardial infarction
(Nelms, Sucher, Lacey, & Roth, p. 298). Simply put, this condition is also referred to as a
heart attack, which occurs as a result of a blockage of the blood flow to the heart that
damages portions of the heart muscle and can be fatal (“Heart Attack”). Myocardial
infarction in the coronary arteries is the most common form of heart disease that leads
to death (Mahan et al., p. 743).
2. Mr. Klosterman’s chest pain resolved after two sublingal NTG at 3-minute
intervals and 2 mgm of IV morphine. In the cath lab he was found to have a totally
occluded distal right coronary artery and a 70% occlusion in the left circumflex
coronary artery. The left anterior descending was patent. Angioplasty of the distal
right coronary artery resulted in a patent infarct-related artery with rear-normal flow.
A stent was left in place to stabilize the patient and limit infarct size. Left ventricular
fraction was normal at 42%, and a postero-basilar scar was present with hypokinesis.
Explain angioplasty and stent placement. When is the purpose of this medical
procedure?

Angioplasty is a procedure often used to open arteries of the heart that have been
blocked or clogged by temporarily inserting and inflating a small balloon-like item at
the location of the blockage inside the artery in order to cause widening. This
procedure is frequently combined with the permanent placement of a stent, which is a
small wire mesh tube, which aids in propping the artery open to decrease the chances
that it will narrow again. These procedures can improve the symptoms that accompany
blocked arteries (i.e. chest pain and shortness of breath) or they can be used during a
myocardial infarction to reduce the damage to the heart muscle (“Coronary
Angioplasty and Stents”).
3. Mr. Klosterman and his wife are concerned about the future of his heart health.
What role does the cardiac rehabilitation play in his return to normal activities and in
determining his future heart health?
Cardiac rehabilitation will help provide Mr. Klosterman and his wife with peace of
mind because it will help him recover from his myocardial infarction and surgery,
prevent future hospitalizations and heart complications, address the risk factors that he
has for heart disease, and help him create a healthy lifestyle that will allow him to
return to his normal activities with improved health. The cardiac rehabilitation will
help him be successful because of the support it offers. (“What is Cardiac
Rehabilitation?”).
II. Understanding the Nutrition Therapy
4. What risk factors indicated in his medical record can be addressed through
nutrition therapy?
Many of his risk factors for heart problems can be addressed through nutrition therapy.
These include his poor diet quality including excessive energy intake, slightly low
vitamin E and D intake, slightly low calcium intake, and his BMI of 26.6 (kg/m2) that
classifies him as overweight (Mahan, p. 750-751).

5. What are the current recommendations for nutritional intake during a
hospitalization following a myocardial infarction?
Immediately following the cardiac event, oral intake of food may need to be decreased
due to pain, anxiety, fatigue, and shortness of breath. Food may be limited to clear,
non-caffeinated liquids that later progresses toward the incorporation of soft, easily
chewed foods with small, frequent meals. When patients stabilize, nutrition intake
becomes individualized for the specific patient’s needs and risk factors for myocardial
infarction and should follow the Therapeutic Lifestyle Changes (TLC) Dietary
Recommendations (Nelms, p. 319). The Guide to TLC is basically a compilation of
changes that can be made in order to improve and reduce the risk of further heart
complications. The Guide to TLC includes food items to choose more often, food items
to choose less often, recommendations for weight reduction, recommendations for
increased physical activity, and recommended nutrition composition of a person’s diet
(Nelms, p.308-309).
III. Nutrition Assessment
6. What is the healthy weight range for an individual of Mr. Klosterman’s height?
A healthy weight range for Mr. Klosterman’s height of 5’10” is between 60 and 76
kilograms (Mahan, p. 1067).
7. This patient is a Lutheran minister. He does exercise daily. He walks his dog
outside for about 15 minutes at a leisurely pace. Calculate his energy and protein
requirements.
Weight (kg) = (185 lbs) / (2.2) = 84.1 kg
Height (cm) = (70 in) x 2.54 = 177.8 cm
(10 x 84.1 kg) + (6.25 x 177.8 cm) – (5 x 61 yrs) + 5 = 1652.3 kcal
1652.3 kcal (PAL 1.6) = 2643.7 kcal per day = energy requirements
Males 50 years and older should consume 0.8 g protein per kg body weight every day.
(0.8 g) x (84.1 kg) = 67.3 g protein per day
8. Using Mr. Klosterman’s 24-hour recall, calculate the total number of calories he
consumed as well as the energy distribution of calories for protein, carbohydrate, and
fat using the exchange system.
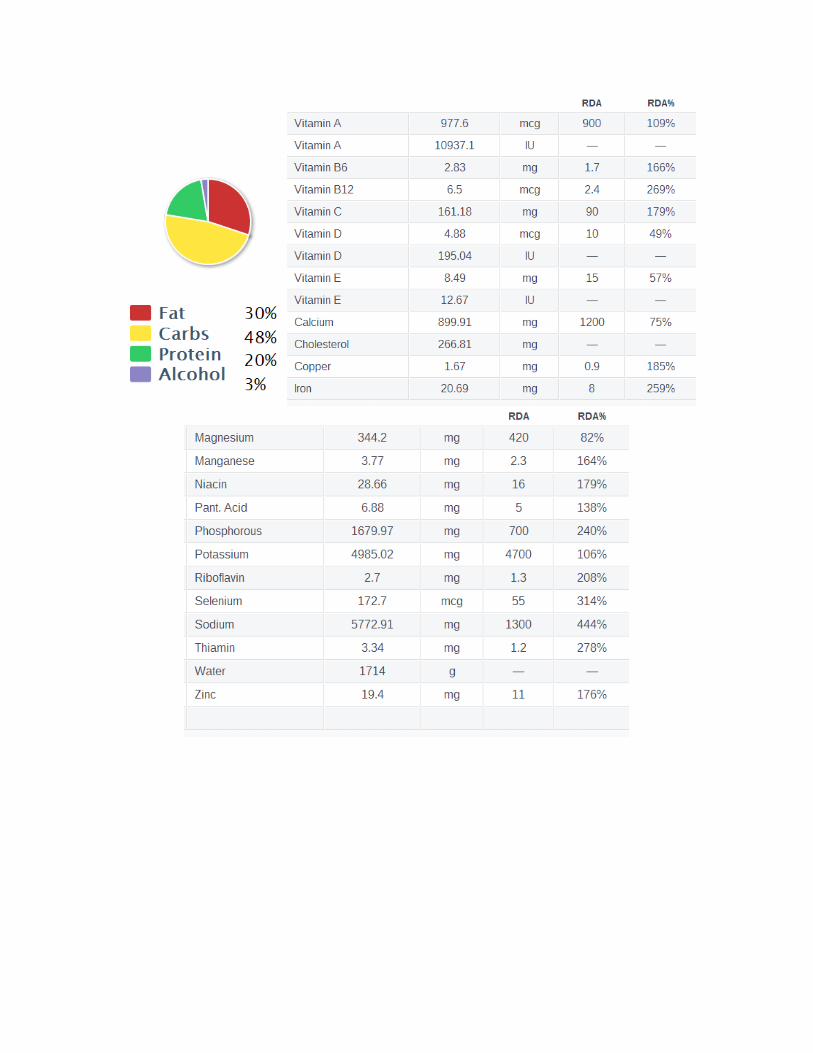
The following data on Mr. Klosterman’s calorie consumption based on his 24-hour
recall was gathered using www.fitday.com. However, the exchange system is also a
good way to calculate a client’s energy distribution from a 24-hour recall. The exchange
system states that 15 g carbohydrate is 1 serving, 7 g protein is 1 serving, and 5 g fat is 1
serving.


kcal from fat = (93.2 g) x (9 kcal/g) = 838.8 kcal
( (838.8 kcal from fat) / (2757 kcal total) ) x 100 = 30.4% kcal from fat
kcal from carbohydrates = (330.7 g) x (4 kcal/g) = 1322.8 kcal
( (1322.8 kcal from carbohydrates) / (2757 kcal total) ) x 100 =
48.0% kcal from carbohydrate
kcal from protein = (135.3 g) x (4 kcal/g) = 541.2 kcal
( (541.2 kcal from protein) / (2757 kcal total) ) x 100 = 18.6% kcal from protein
( (87 kcal from alcohol) / (2757 kcal total) ) x 100 = 3.2% kcal from alcohol

9. Examine the chemistry results for Mr. Klosterman. Which labs are consistent with
the MI diagnosis? Explain. Why were the levels higher on day 2?
One of the World Health Organization’s criteria for diagnosis of myocardial infarction
is the rise and fall of a series of serum cardiac enzymes that are released from damaged
or dying cells during necrosis. These enzymes are normally found within myocardial
cells in the heart; however, a myocardial injury such as a heart attack that destroys the
cells will cause large amounts of these enzymes to be released in the patient’s blood.
The enzymes that serve as biomarkers of a myocardial injury include MB isoenzyme of
creatine kinase (CK-MB), CK-MB isoforms, lactate dehydrogenase isoenzyme (LD-I),
cardiac troponin I (cTnI), cardiac troponin T (cTnT), and myoglobin (Nelms, p.319).
Below are Mr. Klosterman’s laboratory results for these select enzymes.
Ref. Range Dec. 1 Dec. 2 Dec. 3
Biomarker
CK-MB (U/L) 55-170 75 500 335
CK-MB
isoforms (U/L)
0 0 75 55
LD-I (U/L) 208-378 325 685 365
cTnI (ng/dL) <0.2 2.4 2.8
cTnT (ng/dL) <0.03 2.1 2.7
Although there are no lab results for myoglobin, all other select biomarkers for
myocardial infarction are consistent with Mr. Klosterman’s myocardial infarction
diagnosis. The levels of enzymes in his blood are highest on day 2 (Dec. 2) due to the
fact that it takes time for the enzymes to reach a peak elevation in the blood stream after
the myocardial injury. For instance, peak elevation occurs after 12 to 24 hours for CK-
MB after a MI, 18 hours for CK-MB isoforms after a MI, 48 to 72 hours for LD-I after a
MI, 12 hours for cTnI after a MI, and 12 to 48 hours for cTnT after a MI (Nelms, p.318).
10. What is abnormal about his lipid profile? Indicate the abnormal values.
Mr. Klosterman’s cholesterol is well above the desirable level of 120 to 199 mg/dL
that would put him at a lower risk for heart disease and future heart
complications. His total cholesterol was 235 mg/dL on 12/1, 226 mg/dL on 12/2,
and 214 mg/dL on 12/3.

His HDL cholesterol level is less than 40 mg/dL, which is a major risk for heart
disease and future heart complications. His HDL cholesterol should at least be
above 40 mg/dL and preferably above 60 mg/dL. His HDL cholesterol was 30
mg/dL on 12/1, 32 mg/dL on 12/2, and 33 mg/dL on 12/3.
His LDL cholesterol levels range from borderline high to high values that
contribute to his risk of heart disease and future complications. His LDL
cholesterol levels should be below 100 mg/dL for optimum health; however, his
levels were 160 mg/dL on 21/1, 150 mg/dL on 12/2, and 141 mg/dL on 12/3.
His triglyceride levels were normal.
11. Mr. Klosterman was prescribed the following medications on discharge. What
are the food-medication interactions for this list of medications?
Medication Possible Food-Medication Interactions
Lopressor 50 mg daily This medication competes for
metabolizing enzymes in the liver, so if a
food is competing with this drug, more of
the drug could reach systemic circulation
and lead to a toxic effect (Mahan, p.214).
Calcium interferes with absorption.
Lisinopril 10 mg daily He should avoid natural licorice and salt
substitutes.
Nitro-Bid 9.0 mg twice daily No significant food-medication
interactions, but side effects may be n/v,
abdominal pain, or dry mouth.
NTG 0.4 mg sl prn chest pain No significant food-medication
interactions, but side effects may be n/v,
abdominal pain, or dry mouth.
ASA 81 mg daily He should avoid alcoholic beverages and
medications. Side effects may be stomach
irritation if this medication is not
consumed with food.
12. You talk with Mr. Klosterman and his wife, a math teacher at the local high
school. They are friendly and seem cooperative. They are both anxious to learn what
they can do to prevent another heart attack. What questions will you ask them to
assess how to best help them?

Are you willing to make changes to your diet?
Are you willing to try a wide variety of new foods?
Are you willing to eat some of your favorite foods in moderation?
Would you be able to make more room in your schedule to incorporate
additional exercise or recreational activities?
Would you be willing to make an extra effort to incorporate more physical
activity into your daily routine?
Would you like to learn about which foods will lower your total and LDL
cholesterol and raise your HDL cholesterol? Would you, Mrs. Klosterman, like
to learn how to incorporate these foods into new recipes that the both of you can
eat together?
Would you be interested in learning about your options for reducing the amount
of cigarettes you smoke?
13. What other issues might you consider to support successful lifestyle changes for
Mr. Klosterman?
I would emphasize his family history of heart disease in order to encourage him
and help him see the importance of making lifestyle changes.
I would consider the fact that he works a full time job and will have limited time
and energy to incorporate changes and may have increased stress in his
everyday life.
I would consider the fact that he has a college education and will be able to
understand the information that I provide at a higher level than other
individuals.
I would consider the fact that his wife cooks for him and that she needs to be
informed just as much as him so that he has a supporter and someone who will
cook healthy meals for him.
I would consider his smoking habits because tobacco use significantly increases
his risk for future heart complications. However, it will be important to also
consider that he has smoked one pack of cigarettes each day for the past 40 years
and this may be a sensitive subject or a habit not easily broken.

14. From the information gathered within the assessment, list possible nutrition
problems using the correct diagnostic terms.
Excessive energy intake (NI-1.5)
Excessive tobacco intake (NI-4.2)
Inappropriate intake of saturated and trans fats (NI-5.6.3)
Altered lipid profile (NC-2.2)
Food-medication interaction (NC-2.3)
Overweight/obesity (NC-3.3)
(“IDNT Reference Manual”, p.203-212)
IV. Nutrition Diagnosis
15. Select two of the identified nutrition problems and complete the PES statement
for each.
1. Patient is overweight related to excess energy intake and decreased energy needs
as evidenced by 24-hour recall of food and beverage intake and BMI of 26.6.
2. Patient has a diet high in fat and cholesterol related to inappropriate intake
dietary lipids as evidenced by abnormal anthropometric blood lipid
measurements.
16. For each of the PES statements you have written, establish an ideal goal (based on
the signs and symptoms) and an appropriate intervention (based on the etiology).
1. Goal: Patient will reduce daily energy intake to by 500 kcal per day (in order to
lose at least one pound each week) and increase amount of daily physical
activity.
Intervention: Patient will keep a food journal and/or use fitday.com to count
calories and will incorporate physical activity into his daily routine (i.e. take a
walk during his hour lunch break at work and take the stairs instead of the
elevator at work and other locations)
2. Goal: Patient will increase the consumption of dietary polyunsaturated and
monounsaturated fats and decrease consumption of dietary saturated/total fat
and cholesterol.
Intervention: Patient and spouse will be educated on the importance of the
incorporation of monounsaturated fats, polyunsaturated fats, and omega-3 fatty
acids and reduction of saturated fats, trans fats, and dietary cholesterol into
patient’s diet. Patient’s spouse will prepare recipes high in “healthy” fats and
low in “unhealthy” fats.
17. Mr. Klosterman and his wife ask about supplements. “My roommate here in the
hospital told me I should be taking fish oil pills.” What does the research say about
omega-3-fatty acid supplementation for this patient?
The research says that fish oil pills would be a good way to incorporate healthy fats
(especially omega-3 fatty acids) in his diet. However, obtaining omega-3 fatty acids
from fish or other foods rich in omega-3 fatty acids like oils, nuts, and plants is
advisable in addition to fish-oil supplements or as an alternative to fish oil supplements
because they contain other beneficial nutrients such as proteins, vitamins, and minerals.
Also, the research on omega-3 fatty acids shows that it can raise HDL cholesterol and
lower total cholesterol, which would lower Mr. Klosterman’s risk of future heart
complications and risk of heart disease. Research has also shown that they have other
health benefits like reducing inflammation and lower the risk of other chronic diseases
like cancer and arthritis, which would benefit Mr. Klosterman’s overall health.
Therefore, fish oil supplementation would be appropriate for Mr. Klosterman.
However, if he is eventually able to incorporate enough foods that are rich in omega-3
fatty acids into his diet, it may not be necessary for him to take a fish oil supplement
any longer (“Omega-3 fatty acids”).
18. What would you want to assess in three to four weeks when he and his wife
return for additional counseling?
I would want to assess his laboratory blood data to mark his progress toward
making changes in his lipid profile and check that his enzyme levels have
returned to normal (i.e. CK-MB, CK-MB isoforms, LD-I, cTnI, and cTnT).
I would want to assess Mr. and Mrs. Klosterman’s progress toward making
changes in their cooking and eating habits.
I would want to assess Mr. Klosterman’s progress toward incorporating physical
activity into his daily life.
I would want to assess Mr. Klosterman’s progress toward lowering his calorie
intake by having him once again do a 24-hour recall and look over his food
journal with him.
I would assess whether Mr. Klosterman is able to incorporate additional changes
or whether he needs to set different goals or have different intervention
strategies implemented.
References
American Dietetic Association. (2009). International Dietetics& Nutrition Terminology
(IDNT) Reference Manual: Standardized Language for the Nutrition Care Process,
Second Edition. Chicago, IL: American Dietetic Association.
Coronary Angioplasty and Stents. (2010). Mayo Clinic. Retrieved from
http://www.mayoclinic.com/health/angioplasty/MY00352
Ehrlich, S. D. (2011). Omega-3 fatty acids. University of Maryland Medical System.
Retrieved from http://umm.edu/health/medical/altmed/supplement/omega3-
fatty-acids
Heart Attack. Mayo Clinic. (2013). Retrieved from
http://www.mayoclinic.com/health/heart-attack/DS00094
Mahan, L.K., Escott-Stump, S., and Raymond, J.L. (2012). Krause’s Food & The Nutrition
Care Process, Thirteenth Edition. St. Louis, MO: Elsevier Saunders.
Nelms, M., Sucher, K. P., Lacey, K., and Roth, S. L. (2011). Nutrition Therapy &
Pathophysiology, Second Edition. Belmont, CA: Brooks/Cole Cengage Learning.
What is Cardiac Rehabilitation? (2012). National Heart, Lung, and Blood Institute (NIH).
http://www.nhlbi.nih.gov/health/health-topics/topics/rehab/





























