Upload
selley-kenanga
View
20
Download
0
Embed Size (px)
DESCRIPTION
INTERNATIONAL CLASSIFICATION OF CORNEAL DISTROPHY
Citation preview
SPECIAL ARTICLE
IC3D Classification of Corneal DystrophiesEdition 2
Jayne S. Weiss, MD,* Hans Ulrik Mller, MD, PhD, Anthony J. Aldave, MD, Berthold Seitz, MD,Cecilie Bredrup, MD, PhD, Tero Kivel, MD, FEBO,k Francis L. Munier, MD,**
Christopher J. Rapuano, MD, Kanwal K. Nischal, MD, FRCOphth, Eung Kweon Kim, MD, PhD,John Sutphin, MD, Massimo Busin, MD,kk Antoine Labb, MD,*** Kenneth R. Kenyon, MD,
Shigeru Kinoshita, MD, PhD, and Walter Lisch, MD
Purpose: To update the 2008 International Classication ofCorneal Dystrophies (IC3D) incorporating new clinical, histopath-ologic, and genetic information.
Methods: The IC3D reviewed worldwide peer-reviewed articlesfor new information on corneal dystrophies published between 2008and 2014. Using this information, corneal dystrophy templates andanatomic classication were updated. New clinical, histopathologic,and confocal photographs were added.
Results: On the basis of revisiting the cellular origin of cornealdystrophy, a modied anatomic classication is proposed consist-ing of (1) epithelial and subepithelial dystrophies, (2) epithelialstromal TGFBI dystrophies, (3) stromal dystrophies, and (4)endothelial dystrophies. Most of the dystrophy templates areupdated. The entity Epithelial recurrent erosion dystrophies
actually includes a number of potentially distinct epithelialdystrophies (Franceschetti corneal dystrophy, Dystrophia Smolan-diensis, and Dystrophia Helsinglandica) but must be differentiatedfrom dystrophies such as TGFBI-induced dystrophies, which arealso often associated with recurrent epithelial erosions. Thechromosome locus of Thiel-Behnke corneal dystrophy is onlylocated on 5q31. The entity previously designated as a variant ofThiel-Behnke corneal dystrophy on chromosome 10q24 mayrepresent a novel corneal dystrophy. Congenital hereditary endo-thelial dystrophy (CHED, formerly CHED2) is most likely only anautosomal recessive disorder. The so-called autosomal dominantinherited CHED (formerly CHED1) is insufciently distinct tocontinue to be considered a unique corneal dystrophy. On review ofalmost all of the published cases, the description appeared mostsimilar to a type of posterior polymorphous corneal dystrophylinked to the same chromosome 20 locus (PPCD1). Confocalmicroscopy also has emerged as a helpful tool to reveal in vivofeatures of several corneal dystrophies that previously requiredhistopathologic examination to denitively diagnose.
Conclusions: This revision of the IC3D classication includes anupdated anatomic classication of corneal dystrophies more accu-rately classifying TGFBI dystrophies that affect multiple layersrather than are conned to one corneal layer. Typical histopathologicand confocal images have been added to the corneal dystrophytemplates.
Key Words: cornea, cornea dystrophy, cornea pathology, cornea,genetics, genetic disease, hereditary disease, confocal microscopy,histopathology, epithelium, Bowman membrane, stroma, Descemetmembrane, endothelium, TGFBI, epithelial and subepithelial dys-trophies, epithelial-stromal TGFBI dystrophies, stromal dystrophies,endothelial dystrophies, keratoconus, epithelial basement membranedystrophy, epithelial recurrent erosion dystrophies, subepithelialmucinous corneal dystrophy, Meesmann dystrophy, gelatinousdrop-like corneal dystrophy, ReisBcklers corneal dystrophy,Thiel-Behnke corneal dystrophy, Lisch epithelial corneal dystrophy,lattice corneal dystrophy, granular corneal dystrophy type 1,granular corneal dystrophy type 2, macular corneal dystrophy,Schnyder corneal dystrophy, congenital stromal corneal dystrophy,eck corneal dystrophy, posterior amorphous corneal dystrophy, centralcloudy dystrophy of Franois, preDescemet corneal dystrophy, Fuchsendothelial corneal dystrophy, posteror polymorphous corneal dystro-phy, congenital corneal endothelial dystrophy and Xlinked endothelialdystrophy, histology, confocal microscopy
(Cornea 2015;34:117159)
Received for publication September 8, 2014; revision received October 2,2014; accepted October 3, 2014. Published online ahead of printDecember 14, 2014.
From the *Department of Ophthalmology, Pathology and Pharmacology,Louisiana State University Eye Center of Excellence, Louisiana StateUniversity Health Sciences Center, Louisiana State University, NewOrleans, LA; Department of Pediatric Ophthalmology, Viborg Hospitaland Aarhus University Hospital, Aarhus, Denmark; The Jules Stein EyeInstitute, University of California at Los Angeles, Los Angeles, CA;Department of Ophthalmology, Saarland University Medical Center,Homburg/Saar, Germany; Department of Ophthalmology, HaukelandUniversity Hospital, Bergen, Norway; kDepartment of Opthalmology,Helsinki University Central Hospital, Helsinki, Finland; **Jules-GoninEye Hospital, Lausanne, Switzerland; Cornea Service, Wills EyeHospital, Philadelphia, PA; University of Pittsburgh Medical CenterChildrens Eye Center, Pittsburgh, PA; Cornea Dystrophy ResearchInstitute, Department of Ophthalmology, College of Medicine, YonseiUniversity, Seoul, Korea; Department of Ophthalmology, University ofKansas Medical Center, Kansas City, KS; kkDepartment of Ophthalmol-ogy, Villa Igea Hospital, Matre de Confrences des Universits PraticienHospitalier, Forli, Italy; ***Centre Hospitalier National dOphtalmologiedes Quinze-Vingts, Institut de la Vision, Paris, France; Tufts UniversitySchool of Medicine, Harvard Medical School, Schepens Eye ResearchInstitute, New England Eye Center, Boston, MA; Department ofOphthalmology, Kyoto Prefectural University of Medicine, Kyoto, Japan;and Department of Ophthalmology, Johannes Gutenberg UniversityMainz, Mainz, Germany.
Supported by The Cornea Society, Louisiana Lions Eye Foundation, andResearch to Prevent Blindness.
The authors have no conicts of interest to disclose.Reprints: Jayne S. Weiss, MD, Department of Ophthalmology, Louisiana State
University Health Sciences Center, School of Medicine, 2020 Gravier St,Suite B, New Orleans, LA 70112. (e-mail: [email protected]).
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
Cornea Volume 34, Number 2, February 2015 www.corneajrnl.com | 117
INTRODUCTION
DedicationWe dedicate this work to the memory of Gordon
K. Klintworth, MD, PhD, a brilliant ophthalmic pathologist,and a highly esteemed member of the International Committeefor Classication of Corneal Dystrophies (IC3D), whose legacyof excellence in corneal research and teaching is legendary.
International Committee for the Classificationof Corneal Dystrophies
In 2008, the rst IC3D report sought to develop a newclassication system for corneal dystrophies through inte-gration of the then current information on phenotype,pathology, and especially genetics.1 This project was initiallyundertaken to correct the shortcomings of the century-oldphenotypic method of corneal dystrophy classication.
Cornea Dystrophy: History and DefinitionIn 1890, the term corneal dystrophy was introduced into
the literature by Groenouw2 and then by Biber.3 Groenouwreported 2 patients with noduli corneae, although he did notdistinguish between the one patient having granular cornealdystrophy (GCD) and the other having macular cornealdystrophy (MCD). Subsequently, Biber described a patientwith lattice corneal dystrophy (LCD). Thereafter, Fuchs,4
Uhthoff,5 and Yoshida6 continued to use the term cornealdystrophy.
The general term corneal dystrophy describes aninherited disorder that affects, singly or in combination, cells,tissues, and/or organs.1 In ophthalmology, corneal dystro-phies have typically referred to a group of inherited disordersthat are usually bilateral, symmetric, slowly progressive, andnot related to environmental or systemic factors.7 There areexceptions to each part of the dystrophy denition. Epithelialbasement membrane dystrophy (EBMD) and central cloudydystrophy of Franois (CCDF) are likely degenerative ratherthan hereditary conditions in the majority of patients. Cornealdystrophies can also be clinically unilateral, for example,posterior polymorphous corneal dystrophy (PPCD). Systemicchanges are occasionally seen as in Schnyder cornealdystrophy (SCD), where hypercholesterolemia is common.
Another challenge is that it is unclear where to draw thedividing line between hereditary bilateral essentially stationarycorneal diseases such as cornea plana (from mutations inkeratocan) and the hereditary bilateral diseases called cornealdystrophies. This is underscored by the entity, posterioramorphous corneal dystrophy (PACD) (from deletion ofkeratocan together with 3 other genes), which is typicallyminimally progressive and can be associated with iris abnor-malities. Consequently, many would agree that the termcorneal dystrophy may have more historic than practicalmeaning. However, we have chosen to follow custom, and inthis second edition of IC3D, we have continued to address onlyentities that have been traditionally included in cornealdystrophies.
KeratoconusIs It a Corneal Dystrophy?Do the corneal ectatic diseases, keratoconus and pellucid
marginal degeneration, meet the criteria for inclusion in cornealdystrophies? This is a complex and controversial discussion.
The choice to include keratoconus in a corneal dystrophyclassication could be supported by the emerging suggestion ofa genetic basis. There is a family history in 10% of cases,increased prevalence in rst-degree relatives of affectedindividuals, and markedly increased prevalence in trisomy21. Keratoconus is likely genetically heterogeneous and mayhave incomplete penetrance and variable expressivity.813
However, most cases of keratoconus are sporadic, andin contrast to established corneal dystrophies, potentialcausative associations such as eye rubbing and atopy arenoted. There is still insufcient evidence demonstrating a cleargenetic basis in the majority of patients with keratoconus. Forthis reason, the IC3D continues to support exclusion ofcorneal ectasias from the corneal dystrophy classication. Asinterest in molecular etiology of keratoconus continues, weanticipate future new insights into the true genetic basis ofthis highly prevalent corneal disease.
Shortcomings of the Historic CornealDystrophy Classification
There were numerous aws in the traditional and mostwidely used corneal dystrophy classication system.14,15 Someof the dystrophies were named before the advent of the slitlamp, whereas most were described before the development ofgenetic mapping. Introduction of genotyping revolutionizedour knowledge base of corneal dystrophies. Genotypingrevealed both genotypic heterogeneity, that is, a single dystro-phy such as Meesmann corneal dystrophy is associated withdifferent genes (KRT3 and KRT12) and with phenotypicheterogeneity, the TGFBI gene is associated with multipledistinct allelic dystrophy phenotypes, ReisBcklers cornealdystrophy (RBCD), Thiel-Behnke corneal dystrophy (TBCD),granular corneal dystrophy type 1 (GCD type 1), granularcorneal dystrophy type 2 (GCD type 2), and classic latticecorneal dystrophy (LCD).1 The IC3D classication systemattempts to address these critically important shortcomings.
Dystrophy Versus Degeneration andOther Questions
As noted previously, a number of entities formerlyconsidered as corneal dystrophies are more likely degener-ations rather than inherited diseases. For example, themajority of epithelial basement membrane dystrophy(EBMD) cases have no hereditary basis. Central cloudydystrophy of Franois (CCDF), although hereditary in a fewfamilies, is phenotypically identical to posterior crocodileshagreen. The only distinction is that CCDF is associated witha family history. There are only a few publications describingan entire family with CCDF.1618 Hence, in descriptionsof CCDF patients without a detailed family history, it isimpossible to exclude the diagnostic possibility of posteriorcrocodile shagreen degeneration.19
Fuchs endothelial corneal dystrophy (FECD) is a verycommon corneal dystrophy and has a familial basis.20,21 Stage
Weiss et al Cornea Volume 34, Number 2, February 2015
118 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
1 FECD consists of only cornea guttata without cornealdecompensation. Not all patients with stage 1 FECD progress.Are nonprogressive corneal guttae evidence of a cornealdegeneration rather than FECD? The answer is not knownbut has important clinical implications. Often, the patient withcornea guttata is informed of having a diagnosis of FECD. Ifthe individual consults the Internet or other sources, theirresearch will inevitably suggest that FECD is a disease thatoften progresses to corneal edema, visual loss, and surgicalintervention. Thus, a premature diagnosis of FECD in theabsence of a family history, genetic evidence, or corneal edemacan have important adverse psychological impact on the patientwho anticipates future visual loss and need for cornealtransplantation surgery.
Other dystrophies were described decades agowith minimal or unclear clinical information and no geneticinformation. In particular, such dystrophies as Grayson-Wilbrandt might be variants of other well-known dystrophiesor might not even exist.
Misleading dystrophy names have also contributed tomisdiagnosis. Among individuals with the disease formerlynamed Schnyder crystalline corneal dystrophy (SCCD), 50%actually have visible crystalline deposits.22 Correct diagnosisof those affected patients in the absence of crystals oftenconfounded even seasoned clinicians who depended on thisawed assumption coupled with erroneous literature, bothsupporting the notion that crystals were integral to thediagnosis.23,24 Indeed, the compounded errors of SCD werethe major impetus to create the IC3D nomenclature revisiongroup in 2005. Because the 2008 IC3D publication observedonce established in textbooks, it is exceedingly difcult topurge incorrect information about rare diseases. Many mythsare perpetuated because very few ophthalmologists have seena substantial number of the unusual corneal dystrophies.Even experienced corneal subspecialists often were unable tocorrectly diagnose those with acrystalline SCD24 and patientswent undiagnosed for decades.
Formation of the IC3D in 2005 Leading toPublication in 2008
Initially, the rst requirement for membership in theIC3D group was extensive rsthand knowledge and experi-ence in examining patients with one or more distinct cornealdystrophies. In this way, each dystrophy could be discussedand analyzed by those who had seen the disease rather thansolely being informed by published descriptions, which mightbe erroneous. The group was to critically assess the publishedliterature to purge errors. The members were also necessarilyinternational to assess geographically distinctive foundereffects on globally distinct population. Although SCD wasextremely common in central Massachusetts in the UnitedStates and the west coast of Finland, GCD type 2 wasextremely common in Korea. In some cases, the IC3D wasfortunate to include the individual who originally describedthe dystrophy, as in Lisch epithelial corneal dystrophy(LECD) and X-linked endothelial corneal dystrophy. Thesecond requirement for membership in the IC3D wasrepresentation from geneticists and ophthalmic pathologists.
The 2008 IC3D publication contained the traditionalanatomic classication that organized dystrophies accordingto the corneal layer that was chiey affected.14,15 Templatesfor each dystrophy were created in a standard format tosummarize clinical, pathological, and genetic information aswell as representative clinical photographs.
An evidence-based category system was suggested byProfessor Gordon K. Klintworth, MD, PhD, to indicate thelevel of evidence supporting existence of a given cornealdystrophy depending on how substantive was the knowledgeof its clinical, pathological, and genetic basis. He postulatedthat existence of a new corneal dystrophy must begin withidentication of a clinical phenotype and should progress tocharacterization of the causative gene mutation.
An example of a monogenic category 1 dystrophy isSCD, which is caused by mutations in 1 gene, UBIAD1.Another category 1 dystrophy PACD is caused by deletion ofmultiple genes, keratocan (KERA), lumican (LUM), decorin(DCN), and epiphycan (EPYC). The genetic basis of otherdystrophies, such as some types of FECD, may prove to becomplex and involve multiple genes.
These categories were specied as follows:
Category 1: A well-dened corneal dystrophy in whichthe gene has been mapped and identied and the specicmutations are known.Category 2: A well-dened corneal dystrophy that has been
mapped to one or more specic chromosomal loci, but thegene(s) remains to be identied.Category 3: A well-dened corneal dystrophy in which the
disorder has not yet been mapped to a chromosomal locus.Category 4: This category is reserved for a suspected, new,
or previously documented corneal dystrophy, although theevidence for it, being a distinct entity is not yet convincing.1
We postulated that with increased knowledge abouta dystrophy, its category should progress over time from 4 to3 to 2 to 1. Suspected dystrophies that remain category 4because no further information ever becomes available maybe eventually removed from the nomenclature. The group didnot further specify specic criteria for removal of a category 4dystrophy.
Corneal Dystrophy Purgatory and the Category 4DilemmaWhen Can a Category 4 DystrophyBe Eliminated?
In some cases, additional information might show thata category 4 dystrophy is not an independent entity. One suchexample is central discoid corneal dystrophy (CDCD).25,26
This category 4 dystrophy was phenotypically indistinguish-able from acrystalline SCD. When the causative gene forSCD was found to be UBIAD1,27,28 genetic testing of CDCDsimilarly demonstrated mutations in UBIAD1 indicating thatCDCD was not a unique dystrophy. CDCD was consequentlyremoved before publishing the rst IC3D classication, inwhich it was reclassied as SCD variant.26
Should elimination also be considered for a category 4corneal dystrophy in which no further information to prove ordisprove its unique existence is forthcoming? In such a case,there is no evidence to substantiate or to disprove the
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 119
existence of the dystrophy. We consider this the equivalent ofcorneal dystrophy purgatory.
A case in point is Grayson-Wilbrandt, a category 4dystrophy, which was described in 1 publication in 1966supported only by artists renditions of phenotype, withoutclinical photographs or genotyping.29 Over the ensuing 4decades, while no subsequent articles have disputed theoriginal publication, there also have been no articles sub-stantiating these ndings. Most members of the IC3D agreedthat this entity should be eliminated from the classication. Itis now being consigned to a category of Removed Dystro-phies (Table 1) so that in the event a future publicationseems to substantiate the existence of this entity, the referencepublication remains readily retrievable for future use.
Has the IC3D Been Accepted?The IC3D 2008 classication system successfully
integrated the then most currently accurate clinical, patho-logical, and genetic information regarding corneal dystro-phies. The nomenclature has been incorporated by theAmerican Academy of Ophthalmologys widely used Basicand Clinical Science Course Series,30 which instructs oph-thalmology residents in the United States and Europe and hasbeen referenced by the National Eye Institute. Nonetheless,
the recommendations of the IC3D have been incorporatedonly in a minority of new publications. They had been cited114 times by July 2014, according to Thomson Reuters Webof Science, as opposed to about 800 articles published oncorneal dystrophies since 2009. It is unclear whether theeditors and reviewers reject the new classication, think itunimportant, or remain creatures of habit. For example,despite the nomenclature revision to GCD type 2, the nameAvellino is still used, although its prevalence is seeminglydecreasing. Recognizing that change is an evolutionaryprocess, such incremental progress is encouraging.
Revising the IC3D NomenclatureThe nomenclature revision was congured to be user-
friendly and easily accessible to physicians and patients onwww.corneasociety.org and open access through the journalCornea. One stated requirement of the original nomenclaturerevision was that it be easily upgradeable. Six years afterthe original publication, sufcient new information hadbecome available to begin our rst revision of the IC3D.
Changes in the 2015 IC3D
Anatomic Classication ChangeThe traditionally accepted anatomic level corneal
dystrophy classication has limitations,14,15 as dystrophieswere solely assigned to the single layer most affected. YetRBCD and TBCD affect not only the subepithelial area withdestruction of the Bowman layer but also the anterior stromaand later the deeper stroma. Although categorized anatomi-cally as Bowman layer dystrophies, TGFBI dystrophiesaffect multiple layers. Other corneal dystrophies also affectmore than 1 layer. MCD affects both the stroma andendothelium, and SCD involves epithelium, stroma, andendothelium. As we understand the primary cell(s) of origin,it may be less important to categorize dystrophies as beingconned to 1 specic layer. In addition, histopathology,although affording improved resolution at the cellular level, isalso subject to individual case and disease stage variation.
In this revision of the original IC3D from 2008, weinclude a proposed alteration of the century-old anatomiclevel classication to more accurately reect involvement ofthe cellular layers. We now exclude the Bowman acellularlayer and Descemet acellular membrane. Dystrophies are nowdivided into epithelial and subepithelial dystrophies,epithelial-stromal TGFBI dystrophies, stromal dystrophies,and endothelial dystrophies (Table 1).
What We Have Removed and AddedThe IC3D elected to remove the extensive table of gene
loci and genes with specic mutations because this informa-tion is rapidly changing and can be more easily obtained onthe Internet. For similar reasons, a table of mutations is notincluded in this revision although templates still include thegene locus and gene.
The classic articles on corneal dystrophy classication byWaring, Rodrigues, and Laibson14,15 included clinical drawingsand histopathologic photographs. As clinicopathological
TABLE 1. The IC3D Classification (C = Category)
Epithelial and subepithelial dystrophies
1. Epithelial basement membrane dystrophy (EBMD) majoritydegenerative, rarely C1
2. Epithelial recurrent erosion dystrophies (EREDs)Franceschetti cornealdystrophy (FRCD) C3, Dystrophia Smolandiensis (DS) C3, andDystrophia Helsinglandica (DH) C3
3. Subepithelial mucinous corneal dystrophy (SMCD) C4
4. Meesmann corneal dystrophy (MECD) C1
5. Lisch epithelial corneal dystrophy (LECD) C2
6. Gelatinous drop-like corneal dystrophy (GDLD) C1
Epithelialstromal TGFBI dystrophies
1. ReisBcklers corneal dystrophy (RBCD) C1
2. Thiel-Behnke corneal dystrophy (TBCD) C1
3. Lattice corneal dystrophy, type 1 (LCD1) C1variants (III, IIIA, I/IIIA,IV) of lattice corneal dystrophy C1
4. Granular corneal dystrophy, type 1 (GCD1) C1
5. Granular corneal dystrophy, type 2 (GCD2) C1
Stromal dystrophies
1. Macular corneal dystrophy (MCD) C1
2. Schnyder corneal dystrophy (SCD) C1
3. Congenital stromal corneal dystrophy (CSCD) C1
4. Fleck corneal dystrophy (FCD) C1
5. Posterior amorphous corneal dystrophy (PACD) C1
6. Central cloudy dystrophy of Franois (CCDF) C4
7. Pre-Descemet corneal dystrophy (PDCD) C1 or C4
Endothelial dystrophies
1. Fuchs endothelial corneal dystrophy (FECD) C1, C2, or C3
2. Posterior polymorphous corneal dystrophy (PPCD) C1 or C2
3. Congenital hereditary endothelial dystrophy (CHED) C1
4. X-linked endothelial corneal dystrophy (XECD) C2
Removed dystrophies
Grayson-Wilbrandt corneal dystrophy (GWCD) C4
Weiss et al Cornea Volume 34, Number 2, February 2015
120 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
correlation remains a hallmark of corneal dystrophy diagnosis,we have included representative histopathology and electronmicroscopy, as well as confocal microscopy in some cases.
Findings on the emerging technique of anteriorsegment optical coherence tomography (OCT) were addedto the templates when available. We expect that this methodwill rene clinical diagnostics of several dystrophies,especially the differential diagnosis between TBCD andRBCD by providing images that are highly similar tohistopathologic sections.
Reclassied Corneal DystrophiesCongenital Hereditary Endothelial Dystrophy
One challenge of the dystrophy nomenclature has beenthe tendency to emphasize a new or rare observation insteadof waiting for a complete analysis of a new disorder. In the2008 IC3D publication, we observed that inconsistencies inthe literature have confounded our understanding of precisendings in specic corneal dystrophies. Since then, we havelearned more about congenital hereditary endothelial dystro-phy (CHED). In 2008, we followed convention by including2 types of CHED: an autosomal dominant (AD) form withless severe ndings was called CHED1 and an autosomalrecessive (AR) form with more severe ndings was termedCHED2. Further review of the clinical and pathologicaldescriptions of the 5 families previously reported withCHED1 suggests that many and possibly all of these familieshave PPCD.3133 Consequently, AD CHED (CHED1) hasbeen eliminated. Autosomal recessive CHED, previouslycalled CHED2, is now called simply CHED.34
Is the 10q23-24 Dystrophy Distinct or a Variant of TGFBIThiel-Behnke Corneal Dystrophy?
In 1997, Yee et al35 reported a dystrophy affecting theBowman layer that mapped to 10q23-24, which they calledThiel-Behnke corneal dystrophy (TBCD). The article sug-gested that the affected individual had corneal ndingsconsistent with TBCD. The histological features of this patientwere subsequently reported by Lohse et al36; however, therewere different pedigrees in both articles. Clarication of the10q Thiel-Behnke phenotype37 presented other challenges.Nakamura et al38 described a mixture of honeycomb-like,geographic-like, and map-like opacity patterns of the presentedpatients in their legends, but these were not compatible with theaccompanying black and white photographs that did notdemonstrate a typical honeycomb-like pattern. Consequently,given the genetic heterogeneity, phenotypic heterogeneity andabsence of corroborating histopathology of the 10q23-24dystrophy, we believe that there is insufcient evidence toconsider this a variant of TBCD. Is it a distinct dystrophy?Because this is not presently known, we hope ongoinginvestigations will resolve this uncertainty before the nextIC3D revision. The 10q23-24 dystrophy is thus still listed asa footnote to TBCD and not promoted to a template.
Expanded TemplatesIn 2008, the epithelial recurrent erosion dystrophy
template included both Franceschetti39 hereditary recurrenterosion and Dystrophia Smolandiensis (DS),40 which shared
recurrent erosions as their major and often only clinicalnding. At that time, it was unclear whether these 2 entitieswere variants of the same condition or whether these weredistinct dystrophies. Lisch et al41 observed that the affectedmembers of the original Franceschettis family showedrecurrent erosions in the rst decades, as well as diffusesubepithelial opacities in the advanced age. The authorstermed this entity Franceschetti corneal dystrophy(FRCD). In 2009, another entity, Dystrophia Helsinglandica(DH)42 was published and has been added to the epithelialrecurrent erosion dystrophys template. Future information,especially future identication of the underlying gene(s) willreveal whether these 3 entities are unique entities or allelicvariants of one and the same disorder.
Diagnosis of a Corneal Dystrophy in thePediatric Patient
Diagnosing corneal dystrophies in the pediatric patientremains a challenge. Most publications contain photographsof the most classic advanced cases found in adults. Fewphotographs document the earliest and most subtle cornealchanges as would occur in children, and there is no atlas ofcorneal dystrophy ndings in children. This markedlyincreases the difculty of making the correct diagnosis inthe pediatric patient.43,44
Sporadic Corneal Dystrophy?It is important to be cautious before making the
diagnosis of a sporadic corneal dystrophy. It is mandatoryto obtain the family history and examine the parents and otherfamily members. For example, paraproteinemic immunotac-toid keratopathy can mimic SCD, lattice corneal dystrophy, orGCD type 1.45 Mucolipidosis IV can cause a cornea verti-cillata pattern similar to GCD type 1.
A PLEA TO REVIEWERS AND EDITORS
More Stringent Criteria for Publishing theNew Unique Corneal Dystrophy
An 8-year-old boy is examined and noted to have anunusual conguration of bilateral corneal ecks. Is thisa unique new corneal dystrophy? There is a systematicapproach to determining whether this is a corneal dystro-phy that has already been described or rather a unique newentity.
Do other family members have similar cornealndings? If so, the inheritance is likely AD or X-linked.Even if there is no family history, family members shouldstill be examined to detect subtle or previously unappre-ciated corneal changes. If no abnormalities are evident, theinheritance could be AR or there could be incompletepenetrance or poor expressivity. Although a classicalphenotypegenotype correlation facilitates diagnosis, thisdoes not always occur. Histopathology and genotyping canadd more information.
If geneticists discover a new mutation, a novel type ofcorneal dystrophy can be constructed phenotypically. Weadvise peer-reviewed journals to strengthen the criteria
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 121
required for publication of a new corneal dystrophy.A minimum of approximately 10 affected members in 3generations is reasonably convincing to demonstrate a dis-tinct dominant phenotype clinically and scientically. Sucha rigorous systematic approach also avoids creation of morecategory 4 dystrophies that may be destined only foreventual elimination. Corneal photographs with a dilatedpupil also facilitate diagnosis. When the gene or gene locushas been identied, it is preferable to include photographswith genetic conrmation. We have attempted to do bothwhen possible for this article.
As an example, a 27-year-old woman demonstratedrare bilateral lattice lines atypical for classic LCD. Genotyp-ing demonstrated the classical Arg124Cys TGFBI LCD1mutation conrming LCD. This was not a unique cornealdystrophy but rather an additional example of phenotypicvariation resulting from variable penetrance or expressivityof the gene.
Regarding mutations of TGFBI, a phenotype typicalenough to be clinically recognizable is generally limited toTBCD, RBCD, GCD1, GCD2, and classic LCD. When anyof these classic mutations is documented, correspondingterminology should be used without exception, despite anypossible individual variation in phenotype. Other TGFBImutations often produce variant, overlapping, or mixedphenotypes, often with amyloid, and these dystrophies canbe called variant LCD by IC3D conventions. Also, it is illappreciated that both Congo red and Masson trichromeoften co-label some deposits in GCD1 and LCD, suggest-ing a mixed phenotype or GCD2. Also in these cases, theterminology corresponding to the identied mutationshould simply be used.
There are frequent submissions to journals of suchnew dystrophies based on a small change in phenotype.More than a century away from the original description ofcorneal dystrophies, the eld has progressed from phenotypeto genotype. In the United States, support of the National EyeInstitute has made genotyping more accessible through eye-GENE.46 We implore authors and reviewers alike to requiregenotyping and phenotypic information before proposing thediscovery of any new genetic disease.
EPITHELIAL AND SUBEPITHELIAL DYSTROPHIES
Epithelial Basement MembraneDystrophy (EBMD)
Mendelian inheritance in man (MIM) #121820.
Former Alternative Names and EponymsMap-dot-ngerprint dystrophy.Cogan microcystic epithelial dystrophy.Anterior basement membrane dystrophy.
InheritanceIsolated familial cases have been reported. However,
because the majority of cases have no documentedinheritance, they are considered to be degenerative orsecondary to trauma.
Genetic Locus5q31.
GeneTransforming growth factor betainducedTGFBI in 2
families.
OnsetCommonly present in adult life. Rarely described in
children.
SignsPoor adhesion of basal epithelial cells to abnormal basal
laminar material is thought to predispose to recurrent erosions.
MapsIrregular islands of thickened, gray, hazy epithelium
with scalloped, circumscribed borders, particularly affectingthe central or paracentral cornea. Isolated or combined withother signs (Fig. 1A).
Dots (Cogan)Irregular round, oval, or comma-shaped, nonstaining,
putty-gray intraepithelial opacities, clustered like an archipelagoin the central cornea (Fig. 1B). Typically combined with othersigns, especially with maps.
Fingerprint LinesParallel, curvilinear lines, usually paracentral, best
visualized with retroillumination (Fig. 1C). Isolated or com-bined with other signs, especially maps.
Bleb Pattern (Bron)Subepithelial pattern like pebbled glass, best seen by
retroillumination (Fig. 1D). Isolated or combined with othersigns.
SymptomsEBMD can be asymptomatic, associated with painful
erosive episodes and/or may cause decreased vision byinducing mild irregular astigmatism (monocular diplopia,ghost images).
CourseLocation and degree of pathology can uctuate with
time.
Light MicroscopyMaps
Sheets of intraepithelial, multilamellar, basal laminarmaterial (Fig. 1F).
Fingerprint LinesRib-like intraepithelial extensions of basal laminar
material (Fig. 1E).
DotsIntraepithelial pseudocysts containing cytoplasmic debris.
Weiss et al Cornea Volume 34, Number 2, February 2015
122 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
Bleb PatternIrregular, subepithelial accumulation of brillogranular
material.
In contrast to some other supercial dystrophies, theBowman layer is normal.
Transmission Electron MicroscopyMaps
Thick, multilamellar sheets (26 nm thick) ofepithelial basement membrane that extend into theepithelium.
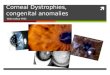
FIGURE 1. Epithelial basement mem-brane dystrophy. A, Map-like changes.B, Intraepithelial dot opacities (Cogancysts) underlying map-like figures. C,Fingerprint lines, best visualized withretroillumination. D, Multiple crow-ded blebs (Bron), only visible in ret-roillumination. E and F, Lightmicroscopy shows excessive base-ment membrane material (arrow-heads) intervening betweendistorted epithelium and the intactBowman layer) to form redundantsheets corresponding to maps (E)and fingerprint lines (F) (E, Massontrichrome; F, PAS, bar = 200 mm.) G,In vivo confocal microscopy demon-strates abnormal hyperreflective in-traepithelial basement membranematerial within suprabasal and basalepithelial cell layers (400 400 mm).
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 123
Fingerprint LinesFine brillar (17 nm diameter) and granular (8 nm)
substance in addition to undulating waves of the basementmembrane.
DotsIntraepithelial pseudocysts contain degenerating cells
with pyknotic nuclei and cytoplasmic debris.
BlebsDiscrete noncystic mounds of abnormal granular mate-
rial deposited between the epithelium and Bowman layer thatindents the overlying basal epithelial cells. May mimic cystsclinically, but no cysts present on histology.
Confocal MicroscopyMaps
Highly reective tissue in various congurationscorresponds to abnormal basement membrane extendinginto the intermediate and basal epithelial cell layers.Adjacent basal epithelial cells appear distorted. No abnor-malities in supercial epithelial cells or stroma.
Fingerprint LinesLinear hyperreective structures corresponding to abnor-
mal basement membrane projecting into the corneal epithelium(Fig. 1G).
DotsHyperreective structures with sharp border within the
intermediate cell layers.
BlebsCircular or oval hyporeective or hyperreective areas
at the level of the basal epithelium and Bowman layer.
CategoryMost cases are sporadic and may be degenerative.
Category 1 in rare cases.Note: Only 1 publication identies 2 families with EBMDwith TGFBI mutations.
BIBLIOGRAPHY Boutboul S, Black GC, Moore JE, et al. A subset of patientswith epithelial basement membrane corneal dystrophy havemutations in TGFBI/BIGH3. Hum Mutat. 2006;27:553557.
Bron AJ, Brown NA. Some supercial corneal disorders.Trans Ophthalmol Soc UK. 1971;91:1329.
Bron AJ, Tripathi RC. Cystic disorders of the cornealepithelium II. Pathogenesis. Br J Ophthalmol.1973;57:361375.
Cogan DG, Donaldson DD, Kuwabara T, et al. Microcysticdystrophy of the corneal epithelium. Trans Am OphthalmolSoc. 1964;62:213225.
Guerry D. Fingerprint-like lines in the cornea. Am JOphthalmol. 1950;33:724726.
Fogle JA, Kenyon KR, Stark WJ, et al. Defective epithelialadhesion in anterior corneal dystrophies. Am J OphthalmolSoc. 1964;62:213225.
Hau SC, Tuft SJ. In vivo confocal microscopy of bleb-likedisorder in epithelial basement membrane dystrophy.Cornea. 2011;30:14781480.
Labb A, De Nicola R, Dupas B, et al. Epithelial basementmembrane dystrophy: evaluation with the HRT II RostockCornea Module. Ophthalmology. 2006;113:13011308.
Laibson PR, Krachmer JH. Familial occurrence of dot(microcystic), map, ngerprint dystrophy of the cornea.Invest Ophthalmol Vis Sci. 1975;14:397399.
Laibson PR. Microcystic corneal dystrophy. Trans AmOphthalmol Soc. 1976;74:488531.
Lisch W, Lisch C. Die epitheliale Hornhautbasalmembran-dystrophie. Klin Monatsbl Augenheilkd. 1983;183:251255.
Munier FL, Korvatska E, Djema A, et al. Kerato-epithelinmutations in four 5q31-linked corneal dystrophies. NatGenet. 1997;15:247251.
Rodrigues MM, Fine BS, Laibson PR, et al. Disorders ofthe corneal epithelium. A clinicopathologic study of dot,geographic, and ngerprint patterns. Arch Ophthalmol.1974;92:475482.
Vogt A. Lehrbuch und Atlas der Spaltlampenmikroskopiedes lebenden Auges (1. Teil). Berlin, Germany: Springer;1930:119121.
Epithelial Recurrent ErosionDystrophies (EREDs)
MIM #122400.
VariantsFranceschetti corneal dystrophy (FRCD).Dystrophia Smolandiensis (DS).Dystrophia Helsinglandica (DH).
InheritanceAutosomal dominant.
Genetic LocusUnknown.
GeneUnknown.
OnsetEarly childhood.
SignsRecurrent epithelial corneal erosions presenting in the
rst decades of life lasting 1 to 7 days. During pain-freeintervals, no biomicroscopically evident changes are present(Fig. 2A). By mid-life, diffuse, central, subepithelial opacity,subepithelial brosis (Fig. 2B), or protruding keloid-likeformations develop.
SymptomsSevere epithelial erosive attacks commence in child-
hood and recur throughout life. The attacks often start atnight. Visual impairment from central corneal opacicationconsequent to erosions occurs in approximately 50% of cases.
Weiss et al Cornea Volume 34, Number 2, February 2015
124 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
By age 30 to 40 years, corneal erosions become less severeand less frequent.
CourseWith advancing age to 30 to 40 years, slow reduction in
frequency of painful erosive episodes. Slow progression ofcentral opacities impairs visual acuity.
Light MicroscopyFRCD
Based on supercial perilimbal biopsy, irregular basalepithelium with enlarged intercellular spaces. Alcian bluepositive deposits were present both intracellularly andintercellularly. Partial destruction and absence of the Bowmanlayer with intervening avascular connective tissue pannusbetween the basal epithelium and Bowman layer (Fig. 2C).Negative Congo red staining.
DSKeloid-like structure stains positive with Congo red
indicating secondary amyloidosis.
Transmission Electron MicroscopyFRCD
Irregularity in size and shape of the basal epithelial cellsand enlarged intercellular clefts corresponding to Alcianbluepositive deposits. Presumably dystrophic mitochon-dria in between basal epithelial cells. Pannus containsnumerous broblasts (Fig. 2D).
ImmunohistochemistryFRCD
Segmental reduced expression of the tight junctionproteins claudin and E-cadherin, desmosome components.Decorin expression seems to be enhanced in the basalepithelial layer compared with the normal postmortemcornea.
DSAbundant bronectin is present in the central subepi-
thelial stroma, localized in areas of subepithelial brosis.Keratocytes in these areas are immunoreactive for S100calcium-binding protein A4 (S100A4).
Confocal MicroscopyDS
Abnormal thinning of the corneal epithelium, absenceof the Bowman layer with accumulation of pathologicalmaterial at the level of the Bowman layer. Subepithelialcorneal nerves are sparse and tortuous.
Category3.
Note: The difference in severity of corneal opacication inFRCD, DS, and DH could be explained by the presence ofpolymorphism and difference in expressivity of a commongene. The term Familial recurrent corneal erosions isdescriptive and not diagnostic as recurrent erosions frequentlyoccur in other corneal dystrophies. Future DNA analyses willreveal more information about FRCD, DS, and DH and assistwith differential diagnosis.
FIGURE 2. Franceschetti cornealdystrophy. A, In first decades of life,the cornea appears normal withoutany dystrophy-specific signs afterrecurrent epithelial erosion. B, Withadvancing age, diffuse central haze ofthe epithelial/subepithelial layer de-velops. C, Light microscopy: inadvanced age, the Bowman layer(arrowhead) is partially destroyed andpannus (pan) develops between thebasal epithelium and Bowman layer(PAS, 200 mm). D, Electron micros-copy of pannus with numerous fibro-blasts. From Lisch W.41
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 125
BIBLIOGRAPHY Franceschetti A. Hereditre rezidivierende Erosion der
Hornhaut. Z Augenheilk. 1928;66:309316. Hammar B, Bjrck E, Lagerstedt K, et al. A new cornealdisease with recurrent erosive episodes and autosomal-dominant inheritance. Acta Ophthalmol. 2008;86:758763.
Hammar B, Bjrck E, Lind H, et al. Dystrophia Helsingland-ica: a new type of hereditary corneal recurrent erosions withlate subepithelial brosis. Acta Ophthalmol. 2009;87:659665.
Hammar B, Lagali N, Ek S, et al. Dystrophia Smolandien-sis: a novel morphological picture of recurrent cornealerosions. Acta Ophthalmol. 2010;88:394400.
Legrand J. Dystrophie pithliale cornenne rcidivantefamiliale. Bull Soc Ophtalmol. 1963;5:384387.
Lisch W, Bron AJ, Munier FL, et al. Franceschettihereditary recurrent corneal erosion. Am J Ophthalmol.2012;153:10731081.
Remler O. Beitrag zur hereditren rezidivierenden Horn-hauterosion. Klin Monatsbl Augenheilkd. 1983;183:59.
Shindo S. Familial recurrent corneal erosion. Nippon GankaGakkai Zasshi. 1968;72:9981004.
Wales HJ. A family history of corneal erosions. TransOphthalmol Soc NZ. 1955;8:7778.
Subepithelial Mucinous CornealDystrophy (SMCD)
MIM #612867.
Former Alternative Names and EponymsNone.
InheritanceAutosomal dominant inheritance most likely, but
X-linked inheritance not excluded.
Genetic LocusUnknown.
GeneUnknown.
OnsetFirst decade of life.
SignsDiffuse bilateral subepithelial opacities and haze, most
dense centrally (Fig. 3A).
SymptomsPainful episodes of recurrent corneal erosions, which
decrease during adolescence (only 1 publication of a singlefamily).
CourseProgressive loss of vision in adolescence.
Light MicroscopySubepithelial band of eosinophilic, periodic acidSchiff
(PAS)positive, Alcian bluepositive, hyaluronidase-sensitivematerial is present anterior to the Bowman layer (Fig. 3B).
Transmission Electron MicroscopySubepithelial deposits of ne brillar material.
ImmunohistochemistrySubepithelial deposits react for chondroitin-4-sulfate
and dermatan sulfate.
Confocal MicroscopyNot reported.
Category4.
BIBLIOGRAPHY Feder RS, Jay M, Yue BY, et al. Subepithelial mucinouscorneal dystrophy. Clinical and pathological correlations.Arch Ophthalmol. 1993;111:11061114.
Meesmann Corneal Dystrophy (MECD)MIM #122100.
Former Alternative Names and EponymsJuvenile hereditary epithelial dystrophy.
VariantStockerHolt variant.
InheritanceAutosomal dominant.
Genetic LociLocus 12q13 (KRT3)Locus 17q12 (KRT12) StockerHolt variant.
FIGURE 3. Subepithelial mucinouscorneal dystrophy. A, Slit-lamp bio-microscopy reveals that diffuse sub-epithelial opacities and haze aredensest centrally. B, Light micros-copy: a band of increased staining ispresent beneath the epithelium. TheBowman layer is thin (Alcian blue)(40). Photograph courtesy ofRobert Feder, MD.
Weiss et al Cornea Volume 34, Number 2, February 2015
126 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
GenesKeratin K3 (KRT3).Keratin K12 (KRT12) StockerHolt variant.
OnsetEarly childhood.
SignsMultiple, tiny intraepithelial vesicles extend to the
limbus and are most numerous in the interpalpebral areawith clear surrounding epithelium. Direct illuminationshows varying diffuse gray opacities in different patterns,which may have a distinct border (Fig. 4A). Areas of thecentral or peripheral cornea may be unaffected. Whorled andwedge-shaped epithelial patterns have been reported. Thegray opacities appear as solitary transparent cysts on indirectillumination (Figs. 4B, C). Approximately 85% of eyesshow microcysts affecting the entire epithelium, while theremainder are localized in the upper, lower, central, and/or
peripheral cornea. Coalescence of several cysts may result inrefractile linear opacities with an intervening clear cornea.The cornea may be slightly thinned and corneal sensationmay be reduced.
StockerHolt VariantThe entire cornea demonstrates ne grayish punctate
epithelial opacities that stain with uorescein and ne linearopacities that may appear in a whorl pattern.
SymptomsPatients are typically asymptomatic or may have
mild visual reduction, although some patients complain ofglare and light sensitivity. Foreign body sensation ortearing may escalate to painful recurrent epithelial ero-sions. Rarely, blurred vision results from corneal irregu-larity and scarring.
FIGURE 4. Meesmann corneal dys-trophy. A, In direct illumination,diffuse gray, superior opacity witha distinct border is apparent. B, Withretroillumination, the same eyedemonstrates that the opacity pat-tern is composed of multiple solitarytransparent microcysts. C, Multiplesolitary transparent microcysts inretroillumination. D, Light micros-copy: intraepithelial cysts sometimesextruding onto the corneal surface,contain amorphous material probablycomprised of degenerated epithelialcells. The basement membrane isthickened (Alcian blue and hematox-ylin and eosin stain, 400). E, Electronmicroscopy: intracytoplasmic fibrillarpeculiar substance, surrounding tan-gles of filaments. F, In vivo confocalmicroscopy shows hyporeflectiveareas corresponding to microcysts inthe basal epithelial layer and roundhyperreflective structures (400 400 mm). Figures 4A, B, and C fromFigures 4A and B: Weiss JS, Mller HU,Lisch W, et al. The IC3D classificationof the corneal dystrophies. Cornea.2008;27(suppl 2):S1S42.
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 127
StockerHolt VariantPatients demonstrate more severe signs and symptoms
with earlier onset compared with classic Meesmann cornealdystrophy.
CourseStationary or slowly progressive.
Light MicroscopyThe thickened and disorganized epithelium always
demonstrates intraepithelial cysts (Fig. 4D) lled with PAS-positive cellular debris, which uoresces. The cells alsocontain of PAS-positive and diastase-sensitive material(glycogen). A thickened multilaminar basement membraneprojects into the basal epithelium.
StockerHolt VariantVariably thickened epithelium with vacuolated and
degenerating cells. Variably thickened basement membraneextends into the epithelium. The Bowman layer and stromaremain normal.
Transmission Electron MicroscopyIntracytoplasmic peculiar substance represents a focal
collection of brogranular material surrounded by tangles ofcytoplasmic laments (Fig. 4E). These cysts are round anduniform (1050 mm). Some lesions with reective points inthe cytoplasm probably correspond to cell nuclei.
StockerHolt VariantNot reported.
Confocal MicroscopyHyporeective areas in the basal epithelium ranging
from 40 to 150 mm in diameter, some with reective spotsinside (Fig. 4F).
Numerous corneal intraepithelial microcysts and hyper-reective material thought to represent degenerative cellshave been detected closer to the basal layer of the cornealepithelium in older patients. Compared with the basalepithelial layer, the supercial layer contains larger micro-cysts with atrophic changes of the hyperreective material.Clearly visualized demarcation lines between the microcystsand normal epithelial cells correspond to the biomicroscopi-cally visible demarcation between clear and affected areas.
StockerHolt VariantNot reported.
Category1 including StockerHolt variant.
BIBLIOGRAPHY Allen EH, Atkinson SD, Liao H, et al. Allele-specicsiRNA silencing for the common keratin 12 foundermutation in Meesmann epithelial corneal dystrophy. InvestOphthalmol Vis Sci. 2013;54:494502.
Behnke H, Thiel HJ. On hereditary epithelial dystrophy ofthe cornea (type Meesmann-Wilke) in SchleswigHolstein.Klin Monatsbl Augenheilkd. 1965;147:662672.
Burns RP. Meesmanns corneal dystrophy. Trans AmOphthalmol Soc. 1968;66:530635.
Cao W, Yan M, Hao Q, et al. Autosomal-dominantMeesmann epithelial corneal dystrophy without an exonmutation in the keratin-3 or keratin-12 gene in a Chinesefamily. J Int Med Res. 2013;41:511518.
Clausen I, Duncker GI, Grnauer-Kloevekorn C. Identi-cation of a novel mutation in the cornea specic keratin 12gene causing Meesmanns corneal dystrophy in a Germanfamily. Mol Vis. 2010;16:954960.
Cremona FA, Ghosheh FR, Laibson PR, et al. Meesmanncorneal dystrophy associated with epithelial basementmembrane and posterior polymorphous corneal dystro-phies. Cornea. 2008;27:374377.
Ehlers N, Hjortdal J, Nielsen K, et al. Phenotypic variabilityin Meesmanns dystrophy: clinical review of the literatureand presentation of a family genetically identical to theoriginal family. Acta Ophthalmol. 2008;86:4044.
Fine BS, Yanoff M, Pitts E, et al. Meesmanns epithelialdystrophy of the cornea. Am J Ophthalmol. 1977;83:633642.
Hassan H, Thaung C, Ebenezer ND, et al. SevereMeesmanns epithelial corneal dystrophy phenotype dueto a missense mutation in the helix-initiation motif ofkeratin 12. Eye (Lond). 2013;27:367373.
Javadi MA, Rezaei-Kanavi M, Javadi A, et al. Meesmanncorneal dystrophy; a clinico-pathologic, ultrastructural andconfocal scan report. J Ophthalmic Vis Res. 2010;5:122126.
Meesmann A. ber eine bisher nicht beschriebene domi-nant vererbte Dystrophia epithelialis corneae. Ber Zusam-menkunft Dtsch Ophthalmol Ges. 1938;52:154158.
Nielsen K, Orntoft T, Hjortdal J, et al. A novel mutation asthe basis for asymptomatic Meesmann dystrophy in a Dan-ish family. Cornea. 2008;27:100102.
Ogasawara M, Matsumoto Y, Hayashi T, et al. KRT12mutations and in vivo confocal microscopy in two Japanesefamilies with Meesmann corneal dystrophy. Am J Oph-thalmol. 2014;157:93102.
Seto T, Fujiki K, Kishishita H, et al. A novel mutation inthe cornea-specic Keratin 12 gene in Meesmann cornealdystrophy. Jpn J Ophthalmol. 2008;52:224226.
Stocker FW, Holt LB. A rare form of hereditary epithelialdystrophy of the cornea: a genetic, clinical and pathologicstudy. Trans Am Ophthalmol Soc. 1954;52:133144.
Sullivan LS, Baylin EB, Font R, et al. A novel mutation ofthe Keratin 12 gene responsible for a severe phenotype ofMeesmanns corneal dystrophy. Mol Vis. 2007;13:975980.
Szaik JP, O1dak M, Maksym RB, et al. Genetics ofMeesmann corneal dystrophy: a novel mutation in thekeratin 3 gene in an asymptomatic family suggestsgenotype-phenotype correlation. Mol Vis. 2008;14:17131718.
Thiel HJ, Behnke H. On the extent of variation of hereditaryepithelial corneal dystrophy (Meesmann-Wilke type). Oph-thalmologica. 1968;155:8186.
Weiss et al Cornea Volume 34, Number 2, February 2015
128 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
Tuft S, Bron AJ. Imaging the microstructural abnormalitiesof Meesmann corneal dystrophy by in vivo confocalmicroscopy. Cornea. 2006;25:868870.
Wittebol-Post D, van Bijsterveld OP, Delleman JW.Meesmanns epithelial dystrophy of the cornea. Biometricsand a hypothesis. Ophthalmologica. 1987;194:4449.
Yeung JY, Hodge WG. Recurrent Meesmanns cornealdystrophy: treatment with keratectomy and mitomycinC. Can J Ophthalmol. 2009;44:103104.
Lisch Epithelial Corneal Dystrophy (LECD)MIM #300778.
Former alternative names and eponymsBand-shaped and whorled microcystic dystrophy of the
corneal epithelium.
InheritanceX-chromosomal dominant.
Genetic LocusXp22.3.
GeneUnknown.
OnsetChildhood.
SignsDirect illumination shows localized gray opacities in
different patterns: whorl-like, radial, band-shaped ame/feathery, and club shaped (Figs. 5A, B). Indirect illuminationdemonstrates multiple densely crowded clear cysts (Fig. 5C).Opacities can be minimal or asymmetric with clear surround-ing epithelium. Similar appearance in males and females.
SymptomsAsymptomatic or blurred vision if the pupillary axis is
involved.
FIGURE 5. Lisch epithelial cornealdystrophy. A and B, Diffuse grayishepithelial opacities form radial,feathery or club-shaped patterns.C, Opacification consists of crow-ded, transparent microcysts in ret-roillumination. D, Light microscopy:pronounced vacuolization of theepithelial cells, particularly in outerlayers (hematoxylin and eosin stain,250). E, Electron microscopy: dis-closes coalescent intracellular va-cuolization of the wing cells. Someof these vacuoles coalesce to formempty spaces within the cytoplasmof the epithelial cells, 4000. F, Invivo confocal microscopy shows in-traepithelial hyperreflective dystro-phic areas containing hyporeflectiveround structures, sharply demar-cated from normal epithelial areas(400 400 mm). Figure 5C fromFigure 5C in Weiss JS, Mller HU,Lisch W, et al. The IC3D classificationof the corneal dystrophies. Cornea.2008;27(suppl 2):S1S42.
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 129
CourseSlow progression of opacities with possible visual
deterioration.
Light MicroscopyEpithelial basal cells are cuboidal with low nuclear to
cytoplasmic ratio. In the suprabasal and parabasal layers,vacuolated cells (Fig. 5D) progress to the epithelial surface,where they adopt elongated at squamous shapes. Thesevacuoles are PAS positive, diastase labile, Luxol fast blue andSudan black negative, consistent with glycogen. Intercellularcysts, parakeratosis, orthokeratosis, and hyperkeratosis arenot identied.
Transmission Electron MicroscopyBasal epithelial cells with intact basement membrane
and hemidesmosomes are unremarkable. In the midlevel andsupercial epithelium, there are cells with myriad vacuolesand inclusions (Fig. 5E) of 2 forms; vaguely occulent orlamellar material with or without a circumscribing membrane,and more electron-dense whorled or membranous structures.
Confocal MicroscopyThere are 4 characteristic features of the abnormal
epithelial cells: highly hyperreective cytoplasm andhyporeective nuclei (Fig. 5F); uniform involvement ofall epithelial layers within the affected areas; well-demarcated borders with adjacent normal epithelium;involvement of the limbal area. No distinct intracellulardeposits are present, although the cytoplasm has granularhyperreectivity.
Category2.
BIBLIOGRAPHY Butros S, Lang GK, Alvarez de Toledo J, et al. Die
verschiedenen Trbungsmuster der Lisch-Hornhautdystrophie.Klin Monatsbl Augenheilkd. 2006;223:837840.
Charles NC, Young JA, Kunar A, et al. Band-shaped andwhorled microcystic dystrophy of the corneal epithelium.Ophthalmology. 2000;107:17611764.
FIGURE 6. Gelatinous drop-like cor-neal dystrophy. A, Band keratopathytype. B, Mulberry type. C, Fluoresceinstaining shows an extremely hyper-permeable corneal epithelium, herewithout superficial punctate keratop-athy or erosion. D, Kumquat-likediffuse stromal opacity. E, Lightmicroscopy: massive amyloid ina subepithelial lesion (arrowheads)extending to the midstromal cornea.Bar = 400 mm (direct fast scarlet[DFS], 10). Figures 6A, B, andD from Figures 6A, B, and C in WeissJS, Mller HU, Lisch W, et al. TheIC3D classification of the cornealdystrophies. Cornea. 2008;27(suppl2):S1S42.
Weiss et al Cornea Volume 34, Number 2, February 2015
130 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
Kurbanyan K, Sejpal KD, Aldave AJ, et al. In vivo confocalmicroscopic ndings in Lisch corneal dystrophy. Cornea.2012;31:437441.
Lisch W, Bttner A, Offner F, et al. Lisch corneal dystrophyis genetically distinct from Meesmann corneal dystrophyand maps to Xp22.3. Am J Ophthalmol. 2000;130:461468.
Lisch W, Steuhl KP, Lisch C, et al. A new, band-shapedand whorled microcystic dystrophy of the corneal epithe-lium. Am J Ophthalmol. 1992;114:3544.
Robin SB, Epstein RJ, Kornmehl EW. Band-shaped,whorled microcystic corneal dystrophy. Am J Ophthalmol.1994;117:543544.
Wessel MM, Sarkar JS, Jakobiec FA, et al. Treatment ofLisch corneal dystrophy with photorefractive keratectomyand Mitomycin C. Cornea. 2011;30:481485.
Gelatinous Drop-like Corneal Dystrophy (GDLD)MIM #204870.
Former Alternative Names and EponymsSubepithelial amyloidosis.Primary familial amyloidosis (Grayson).
InheritanceAutosomal recessive.
Genetic Locus1p32.
GeneTumor-associated calcium signal transducer 2 (TACSTD2,
previously M1S1).
OnsetFirst to second decade.
SignsInitially, subepithelial lesions may appear similar to band-
shaped keratopathy (Fig. 6A) or there may be groups of smallmultiple nodules, that is, mulberry conguration (Fig. 6B).They stain with uorescein (Fig. 6C), indicating epithelialhyperpermeability. Supercial vascularization is frequentlyseen. In later life, patients may also develop stromal opacica-tion or develop larger nodular, kumquat-like lesions (Fig. 6D)although it is uncertain whether there is a transition of the 4different phenotypes from one to the other with time.
SymptomsSignicant decrease in vision, photophobia, irritation,
redness, and tearing.
CourseProgression of protruding subepithelial deposits and
stromal opacity. Most patients develop recurrence aftersupercial keratectomy, lamellar keratoplasty, or penetratingkeratoplasty, typically within a few years.
Light MicroscopySubepithelial and stromal amyloid deposits (Fig. 6E).
Transmission Electron MicroscopyDisruption of epithelial tight junctions in the supercial
epithelium. Amyloid evident in the basal epithelial layer.
ImmunohistochemistryDeposits stain with antibodies to lactoferrin.
Confocal MicroscopyEpithelial cells are irregular in shape and often
elongated. There is a mild disorganization of the overallepithelial architecture. Large accumulations of brightly reec-tive material are noted within or beneath the epithelium andwithin the anterior stroma. No evident abnormalities can bedetected in the posterior cornea.
Category1.
BIBLIOGRAPHY Fujiki K, Nakayasu K, Kanai A. Corneal dystrophies inJapan. J Hum Genet. 2011;46:431435.
Ide T, Nishida K, Maeda N, et al. A spectrum of clinicalmanifestations of gelatinous drop-like corneal dystrophy inJapan. Am J Ophthalmol. 2004;137:10811084.
Kaji Y, Oshika T, Takazawa Y, et al. Co-localization ofadvanced glycation end products and D-beta-aspartic acid-containing proteins in gelatinous drop-like corneal dystro-phy. Br J Ophthalmol. 2012;96:11271131.
Kinoshita S, Nishida K, Dota A, et al. Epithelial barrierfunction and ultrastructure of gelatinous drop-like cornealdystrophy. Cornea. 2000;19:551555.
Kitazawa K, Kawasaki S, Shinomiya K, et al. Establish-ment of a human corneal epithelial line lacking thefunctional TACSTD2 gene as an in vitro model forgelatinous drop-like dystrophy. Invest Ophthalmol VisSci. 2013;57015711.
Klintworth GK, Valnickova Z, Kielar RA, et al. Familialsubepithelial corneal amyloidosisa lactoferrin-relatedamyloidosis. Invest Ophthalmol Vis Sci. 1997;38:27562763.
Nakaizumi GA. A rare case of corneal dystrophy. Acta SocOphthalmol Jpn. 1914;18:949950.
Nakatsukasa M, Kawasaki S, Yamasaki K, et al. Tumor-associated calcium signal transducer 2 is required for theproper subcellular localization of claudin 1 and 7: impli-cations in the pathogenesis of gelatinous drop-like cornealdystrophy. Am J Pathol. 2010;177:13441355.
Nakatsukasa M, Kawasaki S, Yamasaki K, et al. Two novelmutations of TACSTD2 found in three Japanese gelatinousdrop-like corneal dystrophy families with their aberrantsubcellular localization. Mol Vis. 2011;19:965970.
Paliwal P, Gupta J, Tandon R, et al. Identication andcharacterization of a novel TACSTD2 mutation in gelati-nous drop-like corneal dystrophy. Mol Vis. 2010;16:729739.
Ren Z, Lin PY, Klintworth GK, et al. Allelic and locusheterogeneity in autosomal recessive gelatinous drop-likecorneal dystrophy. Hum Genet. 2002;110:568577.
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 131
Tsujikawa M, Kurahashi H, Tanaka T, et al. Identicationof the gene responsible for gelatinous drop-like cornealdystrophy. Nat Genet. 1999;21:420423.
Tsujikawa M. Gelatinous drop-like corneal dystrophy.Cornea. 2012;31(suppl 1):S37S40.
Yoshida S, Kumano Y, Yoshida A, et al. Two brotherswith gelatinous drop-like dystrophy at different stages ofthe disease: role of mutational analysis. Ophthalmol.2002;133:830832.
EPITHELIALSTROMAL TGFBI DYSTROPHIES
ReisBucklers Corneal DystrophyMIM #608470.
Former Alternative Names and EponymsCorneal dystrophy of Bowman layer, type I (CDB I).Geographic corneal dystrophy (Weidle).Atypical Granular Corneal Dystrophy.Granular Corneal Dystrophy, type 3.Anterior limiting membrane dystrophy, type 1.Supercial Granular Corneal Dystrophy.
InheritanceAutosomal dominant.
Genetic Locus5q31.
GeneTransforming growth factor beta-inducedTGFBI.
OnsetChildhood.
SignsConuent early irregular geographic-like opacities with
varying densities develop at the level of the Bowman layer
and supercial stroma, initially discrete (Fig. 7A) andsubsequently extending to the limbus and deeper stroma(Fig. 7B). Can be confused with TBCD especially in the rst2 decades. In this early stage, RBCD shows more irregulardiffuse opacities with clear interruptions, whereas TBCDexhibits multiple ecks with reticular formation.
SymptomsVision is impaired from childhood. Painful recurrent
corneal erosions.
CourseSlowly progressive deterioration of vision. Recurrent
corneal erosions tend to abate with time. Similar butfrequently more aggressive course than TBCD but may notbe able to distinguish in an individual case.
Light MicroscopyThe Bowman layer is replaced by a sheet-like layer of
granular Masson trichromered deposits (Fig. 7C), which canextend to the subepithelial stroma and, in advanced cases,sparse round deposits appear in the middle and posterior stroma.
Transmission Electron MicroscopySubepithelial electron-dense, rod- or trapezoidal-shaped
bodies identical to those in GCD1 (Fig. 7D) replace theBowman layer and extend from the basal epithelial cell level toanterior stroma and, sparsely, to deeper stroma. Basal epithelialcells may contain vesicles with similar rods. Electron micros-copy is necessary for denitive histopathologic diagnosis todistinguish from TBCD, which demonstrates curly bers notrod-shaped bodies.
ImmunohistochemistryRod-shaped bodies are immunopositive for transform-
ing growth factor betainduced protein (keratoepithelin).
FIGURE 7. ReisBucklers cornealdystrophy. A, Confluent irregular,geographic-like opacities. B, Geo-graphic opacities extend to the lim-bus and deeper stroma in a moreadvanced case. C, Light microscopy:Masson trichrome stains keratohyalinintensely red beneath the epitheliumand between superficial stromallamellae. Note characteristic destruc-tion of the Bowman layer. Deeper redspots (asterisk) are artifact of lamellarkeratoplasty (Arg124Leu TGFBImutation), bar = 200 mm. D, Electronmicroscopy: broad band of irregularlyarranged, subepithelial rod-shapedbodies (3000). E, In vivo confocalmicroscopy shows a granular highlyreflective material without anyshadow within the basal epithelium(Arg124Leu mutation) (400 400mm).
Weiss et al Cornea Volume 34, Number 2, February 2015
132 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
Optical Coherence TomographyA homogenous conuent layer of hyperreective depos-
its often with serrated anterior border is apparent at the level ofthe Bowman layer and anterior stroma. It is thickest in thecenter (72132 mm), becomes thinner in midperiphery, anddisappears toward the limbus.
Confocal MicroscopyDistinct deposits are found in the epithelium and
Bowman layer. The deposits in the suprabasal and basalepithelial cell layer show extremely high reectivity from smallgranular or amorphous material without shadows (Fig. 7E).The Bowman layer is replaced by highly reective irregularmaterial, even more reective than in TBCD. Fine diffuseround or spindle-shaped deposits may be noted in the anteriorand sparsely even in the posterior stroma.
Category1.
BIBLIOGRAPHY Bcklers M. ber eine weitere familire Hornhaut-
dystrophie (Reis). Klin Monatsbl Augenkeilkd.1949;114:386397.
Kobayashi A, Sugiyama K. In vivo laser confocalmicroscopy ndings for Bowmans layer dystrophies(Thiel-Behnke and ReisBcklers corneal dystrophies).Ophthalmology. 2007;114:6975.
Konishi M, Yamada M, Nakamura Y, et al. Immunohistol-ogy of keratoepithelin in corneal stromal dystrophiesassociated with R124 mutations of the BIGH3 gene. CurrEye Res. 2000;21:891896.
Kchle M, Green WR, Vlcker HE, et al. Reevaluation ofcorneal dystrophies of Bowmans layer and the anteriorstroma (ReisBcklers and Thiel-Behnke types): a light andelectron microscopic study of eight corneas and a review ofthe literature. Cornea. 1995;14:333354.
Liang Q, Pan Z, Sun X, Baudouin C, et al. ReisBcklerscorneal dystrophy: a reappraisal using in vivo and ex vivoimaging techniques. Ophthalmic Res. 2014;51:187195.
Munier FL, Korvatska E, Djema A, et al. Keratoepithelinmutations in four 5q31-linked corneal dystrophies. NatGenet. 1997;15:247251.
Reis W. Familire, eckige Hornhautentartung. Dtsch MedWochenschr. 1917;43:575.
Ridgway AE, Akhtar S, Munier FL, et al. Ultrastructuraland molecular analysis of Bowmans layer corneal dystro-phies: an epithelial origin? Invest Ophthalmol Vis Sci.2000;41:32863292.
Small KW, Mullen L, Barletta J, et al. Mapping of ReisBcklers corneal dystrophy to chromosome 5q. Am JOphthalmol. 1996;121:384390.
Stone EM, Mathers WD, Rosenwasser GO, et al. Threeautosomal dominant corneal dystrophies map to chromo-some 5q. Nat Genet. 1994;6:4751.
Streeten BW, Qi Y, Klintworth GK, et al. Immunolocaliza-tion of beta ig-h3 protein in 5q31-linked corneal dystrophiesand normal corneas. Arch Ophthalmol. 1999;117:6775.
Weidle EG. Klinische und feingewebliche Abgrenzung derReis-Bcklersschen Hornhautdystrophie. Klin MonatsblAugenheilkd. 1989;194:217226.
Wittbol-Post D, Pels E. The dystrophy described by Reisand Bcklers. Ophthalmologica. 1989;199:19.
ThielBehnke Corneal Dystrophy (TBCD)MIM #602082.
Former Alternative Names and EponymsCorneal dystrophy of Bowman layer, type II (CDB2).Honeycomb-shaped corneal dystrophy.Anterior limiting membrane dystrophy, type II.Curly bers corneal dystrophy.WaardenburgJonkers corneal dystrophy.
InheritanceAutosomal dominant.
Genetic Loci5q31.
GeneTransforming growth factor betainducedTGFBI.
OnsetEarly childhood.
SignsInitial signs are solitary ecks or irregularly shaped
scattered opacities at the level of the Bowman layer, followedby symmetrical subepithelial honeycomb opacities (Figs. 8A,B, Ci) with peripheral cornea typically uninvolved. In olderpatients, opacities can progress to deeper stromal layers andthe corneal periphery. It is difcult to distinguish from ReisBcklers corneal dystrophy (RBCD) in early or individualcases.
Rare alleles that combine Arg555Gln with other TGFBImutations lead to variants of TBCD with atypical opacities.
SymptomsRecurrent corneal erosions may be painful in the rst
and second decades. Gradual visual impairment developslater. Erosions are less frequent, and the onset of visualimpairment is later than in RBCD.
CourseSlowly progressive deterioration of vision results from
increasing corneal scarring. Recurrent corneal erosionsdiminish with time. Similar but frequently less aggressivecourse than RBCD but difcult to distinguish individualcases.
Light MicroscopyAlternating irregular thickening and thinning of the
epithelial layer to compensate for ridges and furrows ofunderlying stroma, with focal absence of the epithelialbasement membrane (Fig. 8D). The Bowman layer is replaced
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 133
by a supercial brocellular pannus with a pathognomonicwavy sawtoothed pattern.
Transmission Electron MicroscopyPresence of curly collagen bers 9 to 15 nm in
diameter (Fig. 8E), importantly distinguishes TBCD fromRBCD.
ImmunohistochemistryCurly bers are immunopositive for transforming
growth factor betainduced protein (keratoepithelin).
Confocal MicroscopyDistinct deposits are found in the epithelium and
Bowman layer. The deposits in the basal epithelial cell layershow homogeneous reectivity with round edges accompa-nying dark shadows (Fig. 8F). The Bowman layer is replacedwith reective irregular material that is less reective than inRBCD.
Optical Coherence TomographyProminent hyperreective material at the level of the
Bowman layer extending into the epithelium in a characteristic
FIGURE 8. Lattice Corneal Dystro-phy, type 1 (LCD). A, Initial signs ofmild honeycomb appearance. B,Intensive honeycomb opacity pat-tern in advanced disease(Arg555Gln mutation). C, In a 42-year-old with genetically confirmedTBCD: (i) the cornea displays hon-eycomb opacity while (ii) confocalmicroscopy demonstrates the saw-tooth pattern of hyperreflectivematerial in the Bowman layer. D,Light microscopy: varying thicknessof the epithelium due to a thickenedabnormal subepithelial fibrous layer(arrowheads) that replaces theBowman layer and has a characteris-tic sawtooth-like surface. Massontrichrome, bar = 200 mm. E, Trans-mission electron microscopy: sub-epithelial curly filaments witha thickness of 10 nm (50,000). F, Invivo confocal microscopy imageshows abnormal hyperreflectivematerial with homogeneous re-flectivity, round edges, and darkshadows within the basal epithelium(400 400 mm).
Weiss et al Cornea Volume 34, Number 2, February 2015
134 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
sawtooth pattern (Fig. 8Cii), a major feature in distinguishingTBCD from RBCD.
Category1.
Note: Linkage to 10q24 has been reported in 1 family. Theinitial and later descriptions of the phenotype are incompleteand variable, and light microscopic, immunohistochemical,and anterior segment optical coherence tomographic evidenceof subepithelial scarring similar to and consistent with TBCDhas not been published.
BIBLIOGRAPHY Chen YJ, Chen JT, Lu DW, et al. In vivo corneal confocalmicroscopic ndings and gene analysis of three patientswith Thiel-Behnke corneal dystrophy. Br J Ophthalmol.2010;94:262264.
Cho KJ, Mok JW, Na KS, et al. TGFBI gene mutations ina Korean population with corneal dystrophy. Mol Vis.2012;18:20122021.
Kobayashi A, Sugiyama K. In vivo laser confocal microscopyndings for Bowmans layer dystrophies (Thiel-Behnke andReisBcklers corneal dystrophies). Ophthalmology.2007;114:6975.
Kchle M, Green WR, Vlcker HE, et al. Reevaluation ofcorneal dystrophies of Bowmans layer and the anteriorstroma (ReisBcklers and Thiel-Behnke types): a light andelectron microscopic study of eight corneas and a review ofthe literature. Cornea. 1995;14:333354.
Lohse E, Stock EL, Jones JC, et al. ReisBcklers cornealdystrophy. Immunouorescent and electron microscopicstudies. Cornea. 1989;8:200209.
Munier FL, Korvatska E, Djema A, et al. Keratoepithelinmutations in four 5q31-linked corneal dystrophies. NatGenet. 1997;15:247251.
Niel-Butschi F, Kantelip B, Iwaszkiewicz J, et al.Genotype-phenotype correlations of TGFBI p.Leu509Pro,p.Leu509Arg, p.Val613Gly, and the allelic association ofp.Met502Val-p.Arg555Gln mutations. Mol Vis.2011;17:11921202.
Nowinska AK, Wylegala E, Janiszewska DA, et al.Genotype-phenotype correlation of TGFBI corneal dystro-phies in Polish patients. Mol Vis. 2011;17:23332342.
Ridgway AE, Akhtar S, Munier FL, et al. Ultrastructural andmolecular analysis of Bowmans layer corneal dystrophies: anepithelial origin? Invest Ophthalmol Vis Sci. 2000;41:32863292.
Streeten BW, Qi Y, Klintworth GK, et al. Immunolocaliza-tion of beta ig-h3 protein in 5q31-linked corneal dystrophiesand normal corneas. Arch Ophthalmol. 1999;117:6775.
Thiel HJ, Behnke H. Eine bisher unbekannte subepithelialehereditre Hornhautdystrophie. Klin Monatsbl Augenheilkd.1967;150:862874.
Vajzovic LM, Karp CL, Haft P, et al. Ultra high-resolutionanterior segment optical coherence tomography in theevaluation of anterior corneal dystrophies and degenera-tions. Ophthalmology. 2011;118:12911296.
Weidle EG. Die wabenfrmige Hornhautdystrophie (Thiel-Behnke) Neubewertung und Abgrenzung gegenber der
Reis-Bcklerschen Hornhautdystrophie. Klin Monatsbl Au-genheilkd. 1999;214:125135.
Wittebol-Post D, Van Schooneveld MJ, Pels E. The cornealdystrophy of Waardenburg and Jonkers. Ophthalmic Pae-diatr Genet. 1989;10:249255.
Lattice Corneal Dystrophy, type 1 (Classic)(LCD1) and Variants
MIM #122200.
Former Alternative Names and EponymsLCD, type 1.Biber-Haab-Dimmer.
InheritanceAutosomal dominant.
Genetic Locus5q31.
GeneTransforming growth factor betainducedTGFBI.
OnsetFirst to second decade.
SignsThe rst signs are central supercial eck-like opacities
that usually develop by the end of the rst decade (Fig. 9A).In retroillumination, isolated peripheral, few, and subtlelattice lines in deeper layers are visible initially in thesupercial stroma of the same patient (Fig. 9B). Thinbranching refractile lines and/or subepithelial, whitish, ovoiddots also develop by the end of the rst decade. These linesstart centrally and more supercially, spreading centrifugallyand deeply, but leaving the far peripheral stroma, Descemetmembrane and the endothelium uninvolved (Figs. 9C, D).Diffuse subepithelial ground-glass haze of the central andparacentral cornea develops concurrently with the lattice linesin the central and paracentral cornea and subsequentlyprogresses (Fig. 9C), accompanied by recurrent erosions.Development of diffuse central haze in the second to thirddecade may reduce vision sufciently to necessitate surgicalintervention. The number of lattice lines may differ betweenthe 2 eyes (unilateral cases are described). Variant LCD, typeIIIA also shows central thicker lattice lines (Fig. 10A),whereas LCD, type IV is characterized more by deeperdeposits without epithelial erosion (Fig. 10B).
SymptomsOcular discomfort, pain, and visual impairment, some-
times start as early as the rst decade as consequent tofrequent recurrent erosive attacks. Visual impairment withinthe fourth decade.
CourseProgressive, often with marked visual decrease by the
fourth decade.
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 135
Light MicroscopyEpithelial atrophy and disruption with degeneration of
basal epithelial cells, focal thinning, or absence of theBowman layer, progress with age. Eosinophilic amyloidmaterial accumulates between the epithelial basement mem-brane and Bowman layer. Stromal deposition of amyloid
distorts the architecture of corneal lamellae. Amyloid depositscharacteristically stain positive with Congo red (Fig. 9E), anddisplay birefringence and red-green di rhos under polarizedlight (Fig. 9F). Also, deposits exhibit metachromasia withcrystal violet and uorescence with the use of thioavin Tstaining.
FIGURE 9. Lattice corneal dystro-phy, type 1 (classic lattice). Direct(A) and retroillumination (B) of earlylattice corneal dystrophy (LCD) withdots and fine lattice lines withgenetic confirmation of Arg124Cysin TGFBI. C, Subepithelial ground-glass haze of the central and inferiorcornea, and diffuse lattice lines inadvanced LCD with genetic confir-mation of Arg124Cys in TGFBI. D,Dots and paracentral lattice lines inretroillumination with genetic con-firmation of Arg124Cys in TGFBI. E,Light microscopy: Congo red (E)prominently stains a continuouslayer of amyloid (asterisk) that un-derlies and partially destroys theBowman layer and intrastromalamyloid deposits corresponding tolattice lines (arrowheads). F, Thissame section viewed with polarizedlight confirms deposits are birefrin-gent and red-green dichroic, thusamyloid. Arg124Cys TGFBI muta-tion, bars = 200 mm. G, In vivoconfocal microscopy image showsfilaments corresponding to latticelines within the stroma (400 400mm). Figure 9D from Figure 10A, inWeiss JS, Mller HU, Lisch W, et al.The IC3D classification of the cornealdystrophies. Cornea. 2008;27(suppl2):S1S42.
Weiss et al Cornea Volume 34, Number 2, February 2015
136 | www.corneajrnl.com Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved.
Transmission Electron MicroscopyExtracellular masses of ne, electron-dense randomly
aligned brils of uniform 8 to 10 nm diameter are character-istic of amyloid protein. There are fewer keratocytes in theareas of amyloid deposition: some are degenerated withcytoplasmic vacuolization, whereas others appear metaboli-cally active. Descemet membrane and the endothelium arenormal.
Confocal MicroscopyLinear and branching structures (Fig. 9G) in stroma
with changing reectivity and poorly demarcated margins.Such lines must be differentiated from other similar images(ie, fungi).
Category1.
Note: The LCD variants (Figs. 10A, B) are caused by morethan 2 dozen distinct heterozygous amyloidogenic mutations,nearly all of which are located in the fourth FAS1 domain ofTGFBI. LCD variants (previously designated type IIIA, I/IIIA,IV, and polymorphic amyloidosis) have a delayed onsetcompared with classic LCD. The lattice lines may be larger,with a limbus to limbus ropy appearance (type IIIA), thinner(type I/IIIA), smaller (type IV) or even absent (polymorphicamyloidosis), although one has to keep in mind that the latticepattern is very much dependent on age and mutation. Somepatients do not have clinically evident lattice lines. Corneal
epithelial erosions are a typical presenting sign of LCD, typesIIIA and I/IIIA, but are virtually absent in others (type IV andpolymorphic corneal amyloidosis). The frequency of recurrenterosions is more common in subtypes that progress fromanterior to posterior (types IIIA and I/IIIA) compared withthose progress from posterior to anterior (type IV). Althoughclassic LCD has been found in numerous countries, LCDvariants are mostly geographically restricted. For example,LCD type IIIA and LCD type IV were reported predominantlyin Japan and Italy, and the 2 LCD type IV variants werereported to be derived from solitary founder mutations in Japanand Italy.
Historically, multiple subtypes of lattice were createdon the basis of phenotypic and genotypic variations. Theso-called lattice corneal dystrophy type 2 (LCD2) is a mis-nomer, in fact comprising systemic amyloidosis plus corneallattice lines and should be termed familial amyloidosis,Finnish type, or gelsolin type. Eponymously, it is known asMeretoja syndrome (Figs. 11A, B).
BIBLIOGRAPHY Biber H. Ueber einige seltene Hornhautkrankungen: die
oberaechliche gittrige Keratitis [Inaugural dissertation].Zurich;1890.
Chiou AG, Beuermann RW, Kaufman SC, et al. Confocalmicroscopy in lattice corneal dystrophy. Graefes Arch ClinExp Ophthalmol. 1999;237:697701.
FIGURE 10. Lattice dystrophy var-iants. A, Type IIIA with centralthicker ropy-appearing lattice linesextending to the limbus. B, Type IVwith minimal findings of centralfleck-like opacities in deeper corneaand few small lattice lines. Epithelialerosions are typically absent becausethere is posterior-to-anterior cornealprogression.
FIGURE 11. Familial amyloidosis(Meretoja syndrome). A, Lax, mask-like facies consequent to cranialnerve VII palsy. B, Lattice lines areless numerous than in classic andvariant LCD, start peripherally, andspread centrally (Images providedfor differential diagnostic purposes).
Cornea Volume 34, Number 2, February 2015 IC3D Classification of Corneal Dystrophies
Copyright 2014 Wolters Kluwer Health, Inc. All rights reserved. www.corneajrnl.com | 137
Dighiero P, Drunat S, Ellies P, et al. A new mutation(A546T) of the big-h3 gene responsible for a French latticecorneal dystrophy type IIIA. Am J Ophthalmol.2000;129:248251.
Dighiero P, Niel F, Ellies P, et al. Histologic phenotype-genotype correlation of corneal dystrophies associated witheight distinct mutations in the TGFBI gene. Ophthalmol-ogy. 2001;108:818823.
Ellies P, Renard G, Valleix S, et al. Clinical outcome ofeight BIGH3-linked corneal dystrophies. Ophthalmology.2002;109:793797.
Fujiki K, Hotta Y, Nakayasu K, et al. A new L527Rmutation of the beta IGH3 gene in patients with latticecorneal dystrophy with deep stromal opacities. Hum Genet.1998;103:286289.
Fukuoka H, Kawasaki S, Yamasaki K, et al. Lattice cornealdystrophy type IV (p.Leu527Arg) is caused by a foundermutation of the TGFBI gene in a single Japanese ancestor.Invest Ophthalmol Vis Sci. 2010;51:45234530.
Funayama T, Mashima Y, Kawashima M, et al. Latticecorneal dystrophy type III in patients with a homozygousL527R mutation in the TGFBI gene. Jpn J Ophthalmol.2006;50:6264.
Hida T, Proia AD, Kigasawa K, et al. Histopathologic andimmunochemical features of lattice corneal dystrophy typeIII. Am J Ophthalmol. 1987;104:249254.
Hotta Y, Fujiki K, Ono K, et al. Arg124Cys mutation of thebetaig-h3 gene in a Japanese family with lattice cornealdystrophy type I. Jpn J Ophthalmol. 1998;42:450455.
Kannabiran C, Klintworth GK. TGFBI gene mutations incorneal dystrophies. Hum Mutat. 2006;27:615625.
Kawamoto K, Morishige N, Yamada N, et al. Delayedcorneal epithelial wound healing after penetrating kerato-plasty in individuals with lattice corneal dystrophy. Am JOphthalmol. 2006;142:173174.
Klintworth GK, Bao W, Afshari NA, et al. Two mutationsin the TGFBI (BIGH3) gene associated with lattice cornealdystrophy in an extensively studied family. Invest Oph-thalmol Vis Sci. 2004;45:13821388.
Munier FL, Frueh BE, Othenin-Girard P, et al. BIGH3mutation spectrum in corneal dystrophies. Invest Ophthal-mol Vis Sci. 2002;43:949954.
Munier FL, Korvatska E, Djema A, et al. Keratoepithelinmutations in four 5q31-linked corneal dystrophies. NatGenet. 1997;15:247251.
Nakagawa AS, Fujiki K, Enomoto Y, et al. Case of lateonset and isolated lattice corneal dystrophy with Asn544S-er (N544S) mutation of transforming growth factor beta-induced (TGFBI, BIGH3) gene. Nippon Ganka GakkaiZasshi. 2004;108:618620.
Schmitt-Bernard CF, Guittard C, Arnaud B, et al. BIGH3 exon14 mutations lead to intermediate type I/IIIA of lattice cornealdystrophies. Invest Ophthalmol Vis Sci. 2000;41:13021308.
Seitz B, Weidle E, Naumann GOH. Einseitige gittrigestromale Hornhautdystrophie Typ III (Hida). Klin Mon-atsbl Augenheilkd. 1993;203:279285.
Snead DR, Mathews BN. Differences in amyloid depositionin primary and recurrent corneal lattice dystrophy type 1.Cornea. 2002;21:308311.
Stewart H, Black GCM, Donnai D, et al. A mutation withinexon 14 of the TGFBI (BIGH3) gene on chromosome 5q31causes an asymmetric, late-onset form of lattice cornealdystrophy. Ophthalmology. 1999;106:964970.
Stix B, Leber M, Bingemer P, et al. Hereditary latticecorneal dystrophy is associated with corneal amyloiddeposits enclosing C-terminal fragments of keratoepithelin.Invest Ophthalmol Vis Sci. 2005;46:11331139.
Stock EL, Feder RS, OGrady RB, et al. Lattice cornealdystrophy type IIIA. Clinical and histopathologic correla-tions. Arch Ophthalmol. 1991;109:354358.
Suesskind D, Auw-Haedrich C, Schorderet DF, et al.Keratoepithelin in secondary corneal amyloidosis. GraefesArch Clin Exp Ophthalmol. 2006;244:725731.
Tian X, Fujiki K, Wang W, et al. Novel mutation (V505D) ofthe TGFBI gene found in a Chinese family with latticecorneal dystrophy, type I. Jpn J Ophthalmol. 2005;49:8488.
Tsujikawa K, Tsujikawa M, Yamamoto S, et al. Allelichomogeneity due to a founder mutation in Japanesepatients with lattice corneal dystrophy type IIIA. Am JMed Genet. 2002;113:2022.
Yamada N, Chikama TI, Morishige N, et al. Homozygousmutation (L527R) of TGFBI in an individual with latticecorneal dystrophy. Br J Ophthalmol. 2005;89:771773.
Yamamoto S, Okada M, Tsujikawa M, et al. A kerato-epithelin (big-h3) mutation in lattice corneal dystrophytype IIIA. Am J Hum Genet. 1998;62:719722.
Yamamoto S, Okada M, Tsujikawa M, et al. The spectrumof beta ig-h3 gene mutations in Japanese patients withcorneal dystrophy. Cornea. 2000;19(3 suppl):S21S23.
Granular Corneal Dystrophy, type 1(Classic) (GCD1)
MIM #121900.
Former Alternative Names and EponymsCorneal dystrophy Groenouw type I.
InheritanceAutosomal dominant.
Genetic Locus5q31.
GeneTransforming growth factor betainducedTGFBI.
OnsetChildhood, as early as 2 years of age.
SignsIn children, a vortex pattern (Fig. 12A) of brownish
granules develops supercial to the Bowman lay