-
NEUTRAL PEPTIDASE INHIBITORS
Indian Journal of Pharmacology 2003; 35: 139-145 EDUCATIONAL
FORUM
NEUTRAL PEPTIDASE INHIBITORS: NEW DRUGS FOR HEART FAILURE
I. BASURAY
Interventional Electrophysiology & Device Therapy,
Arrhythmia Service; Division of Cardiology,St Michael's Hospital,
University of Toronto, Toronto, Ontario, Canada.
Manuscript Received: 29.7.2002 Revised: 23.10.2002 Accepted:
26.1.2003
Once it sets in, the left ventricular dysfunction is a
continuous process ultimately leading to end stageheart disease.
End stage heart disease has a high mortality despite the presence
of a number of treatmentmodalities, as most of them are sub
optimal. Thus despite considerable advancement in therapy,
theoverall prognosis remains dismal. This has spurred the search
for newer agents that can effectivelyattenuate the aberrant
physiological changes evident in heart failure. Early research in
heart failuretreatment had made it evident that unloading the heart
should be a primary consideration if the progressof the aberrant
physiology is to be attenuated. Subsequently it became evident that
opposing the aberrantneurohormonal stimulation, to achieve
unloading is associated with a better outcome. Thus ACE(angiotensin
converting enzyme) inhibitors, which unload the heart by reducing
the formation ofangiotensin II; have a better effect on mortality
& morbidity, than the combination of nitrates andhydralazine.
This is despite the fact that both the latter mentioned drugs are
very potent venous andarteriolar dilator, respectively. Certain
recent studies, albeit small ones, conducted in the last few
yearshave shown natriuretic agents which promote diuresis by
augmenting body's defense against the abnormalneurohormonal milieu
evident in heart failure might have a better effect on long term
prognosis than thesymptomatically more effective diuretics. These
studies have lead to the development of novel agentsthat not only
block the over stimulated renin-angiotensin system but also augment
the natriuretic peptidesystem, the body's defence against the
abnormal neurohormonal milieu that is evident in heart failure.This
article reviews the clinical pharmacology of novel agents that
augments the natriuretic peptidesystem in the body and their
potential as new agents in the armamentarium of drugs for heart
failure.
Cardiac failure natriuretic peptides neutral endopeptidase
inhibitors
Introduction
Treatment of heart failure till date has at best
beensymptomatic, with very little effort being made toreverse the
pathology. The introduction of the ACEinhibitors in the treatment
of heart failure was thefirst successful attempt to achieve
symptomatic wellbeing along with attenuation of aberrant
biochemicalchanges that accompany failure. It has beenappreciated
that certain commonly used anti-failuremedications which induce
symptomatic relief quiteeffectively may either do not change (e.g.
digitalis1)or even worsen the biochemical anomalies of heartfailure
(e.g. loop diuretics) and thus provide thepatient with little or
even adverse mortality benefits.
An illustration in this context is the use of frusemide,a loop
diuretic, in heart failure. Although it causesdiuresis and reduces
the pulmonary capillary wedgepressure, it does so at the cost of
producing amanifold increase in renin. This chemical releasedfrom
the kidney amongst other places, is an adversebiochemical marker in
heart failure2. It has nowbecome evident that an increase in such
adversemarkers correlate with a poor mortal i ty andmorbidi ty.
Thus, in the hope of producing asymptomatic benefit and reversing
the pathology,there is a determined effort world over, to
generatedrugs that effectively alter the aberrations
ofneurohormonal milieu that accompany ventricularfailure. A group
of drugs presently undergoing
ABSTRACT
KEY WORDS
Correspondence: I. Basuraye-mail:
[email protected]
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]
-
I. BASURAY
clinical trials that effectively fit in such criteria are
theneutral peptidase inhibitors. These are a group ofchemicals that
inhibit the degradation of atrialnatriuretic peptide (ANP) and
related neuro-hormones which are released by the body as
acompensatory mechanism to reverse thepathophysiological state
present in heart failure thereby causing an increase in the levels
and activities ofthese hormones. This article intends to review
therecent evidences gathered from clinical trials thatpoint to the
possible role of these agents, as a groupwill play as future drugs
for heart failure. This reviewwill also discuss the role of novel
designer drugs;that combine ACE inhibition with peptide
inhibition,all as one molecule to treat heart failure.
Physiological role of natriuretic peptides in heartfai lure: A
review of the physiological role of thenatriuretic peptides would
be in order to understandthe pharmacodynamics of the neutral
peptidaseinhibitors. Three natriuretic peptides, the atrial
(ANP),the brain (BNP) and the C type natriuretic peptide (CNP)have
been identified in humans3. ANP is a 28 aminoacid peptide stored
predominantly in the right atriumand is believed to be coupled to
mechanoreceptors,and released upon atrial distension, as observed
incardiac failure. Accumulated evidence from the pastone decade
points to the crucial role played by thispeptide in inducing
vasodilatation, promoting natriuresisand miscellaneous other
functions including counter-acting the pathological role played by
catecholamines,the arginine-vasopressin,
renin-angiotensin-aldosterone system [RAAS]4. RAAS is known to
besignificantly augmented as part of body's mechanismto counter
fall in cardiac output in heart failure. Thisbecomes counter
productive as water & sodiumretention occurs, causing an overt
increase in theafterload to the failing ventricle. BNP is
structurallysimilar to ANP and is stored mainly in the
ventricles5.The ventricular filling pressure coordinates its
releaseand is functionally similar to ANP. CNP is a
potentvasodilator and is postulated to have a regulatory roleon the
RAAS. The natriuretic peptides are degraded inthe body by a
ubiquitous enzyme called neutralendopeptidase (NEP)6, found in many
organs andtissues. These include the kidneys, brain and
lungs7.Experimental evidence in lower mammals, initially8 andlater
in humans, have corroborated the finding thatinhibition of these
enzymes produce a sustainedincrease in plasma ANP level9.
A large body of accumulated data supports the factthat ANP
therapy in heart failure is accompanied byfavourable hemodynamic
responses. Prolongedinfusion of ANP in heart failure patients
belonging toclass III or IV is associated with a two fold
increasein urine flow rate and an almost four fold increase
insodium excretion10. In severe heart failure patients,similar
infusions have produced an increase incardiac output with a
concomitant decrease inpulmonary capillary wedge pressure
(PCWP),plasma renin levels and pulmonary vascularresistance11. BNP
has similar effects as ANP12; itreduces the pulmonary capillary
wedge pressure andsystemic vascular resistance and also initiates
asustained natriuresis producing up to a 10 foldincrease in sodium
excretion. Interestingly, thisbiochemical also fosters favourable
changes in theneurohormonal milieu. While suppressing
plasmaaldosterone levels, it increases ANP secretions.These
profiles of diuresis, vasodilatation andneurohormonal suppression
make the natriureticpeptides, a potentially attractive treatment
modalityfor heart failure patients.
However, it is obviously ostensible that the
therapeuticpotential of natriuretic peptides are
considerablyattenuated in chronic heart failure patients becauseof
the need to give them, as intravenous infusions.Thus, treatment of
chronic LV failure necessitates thedevelopment of orally active
long acting analoguesor agents that block the metabolism of
endogenouslygenerated natriuretic peptides. The development ofNEP
inhibitors, is thereby a step to meet the latterend.
Oral ly act ive natr iuret ic pept idase inhibi tors:Candoxatril
and ecadotril are the two highly specificinhibitors of NEP
presently undergoing trials as futuredrugs for heart failure. Both
these agents areprodrugs metabol ised in the body to act
ivecongeners. Candoxatril is activated in the liver
tocandoxatrilat, the active metabolite, while ecadotrilis converted
to its active congener, S-thiorphan.
While candoxatril has undergone the largest numberof trials
amongst drugs in this group, experience withecadotril is limited to
a few trials till date. Patientswith mild heart failure infused
with candoxatrilat, theactive molecule of candoxatril, have both
diuresisand natriuresis13. However, in severe heart failurepatients
these actions are considerably lessened,
140
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]
-
NEUTRAL PEPTIDASE INHIBITORS
probably due to decreased renal perfusion1 4 .Northridge et al.,
in a recent trial1 5 comparedcandoxatril in oral doses of 200-400
mg as mono-therapy in mild heart failure patients in a
double-blindclinical trial, with 20 mg frusemide. Severe
heartfailure patients could not be included in the trial sincea
diuretic free period of two weeks, as required inthe study design,
could not be enforced in them.Monotherapy with candoxatril induced
diuresis,natriuresis and kaluresis compared to frusemide.While a
greater decrease in systolic blood pressurewas documented with NEP
inhibitors, the heart rate,diastolic blood pressure and the
functional class ofthe patients remained similar to baseline
studies.Plasma renin activity, a negative prognostic factor
inchronic heart failure, showed a two fold increasefollowing the
first dose of frusemide, with a four-foldrise later on. Therapy
with candoxatril was notassociated at any stage with any
discernableincrements in plasma renin activity. Treadmillexercise
capacity, an important prognostic markerin heart failure,
registered an increase of 12+3.5 secafter 200 mg candoxatril twice
a day and a rise of35+3.1 sec after 400 mg of the drug twice daily
for9 days. However, frusemide treated patients in thesame period,
recorded a decreased exercisecapacity by 30+2.6 sec. The same group
in an earlierstudy also documented a 40% decrease inpulmonary capil
lary wedge pressure usingcandoxatril compared to a 15% reduction
withfrusemide2.
Experience with ecadotril as stated before is limited.In a
recent pilot safety study, though the drugcompared favorably with
placebo, as far as short-term safety and tolerance is concerned,
its clinicaleff icacy was shown to be disappointinglynegative 16,17
. Though this has been attributedprimarily to the study design,
which was not gearedto observe this parameter, other factors l
ikeinadequate dosing could have also played a role.However, in
earlier studies reported by Kahn et al.18
ecadotril administration to heart failure patientsresulted in a
rise in plasma ANP, decrease in bothplasma renin activity and
pulmonary capillary wedgepressure.
Role of NEP inhibitors in heart fai lure: The firstline
treatment for mild heart failure has been adiuretic, which is
usually combined with an ACEinhibitor. While ACE inhibitor use is
associated with
decreased hospitalization and death19, the long termeffects of
diuretics in heart failure, as far as mortalityand morbidity
statistics go, are yet ill-defined. Therehave been contradictory
findings with diuretic trialsin mild and severe heart failure.
Cowley et al.2 0
showed that moderately severe cardiac failurepatients put on
frusemide at high doses (120 mg),exhibited improved quality of life
and better exercisecapacity. Few other uncontrolled studies too
havecome to the same conclusion21. However, Northridgeand
colleagues, using low doses to treat mild heartfailure, have shown
a decrease rather than anincrease in exercise capacity. These
adverse effectsof diuretics on mild heart failure, with no evidence
offluid retention, can be explained by detrimentalchanges they
induce including stimulation of theRAAS mechanism, and a decrease
in cardiac outputby ventricular unloading15. Though both these
factorsexist even in severe heart failure patients treatedwith
diuretics, the decrease in congestion andreduction of fluid
overload achieved, producessymptomatic benefits. Thus the
pathophysiologicalaberrations instead of getting attenuated;
actuallyworsens over a time period, leading to more severeforms of
heart failure. The end point of this vortex ofincreasing failure
ultimately makes the disease drug-refractory. Accumulated evidence
for the past onedecade has confirmed the early elevation of NEP
inthe progression of left ventricular dysfunction, evenbefore the
onset of symptoms. There is considerableevidence that indicate the
fact that this increase isbeneficial; by preventing the activation
of RAAS andconsequent salt and water retention, thus delayingthe
initiation of pathological changes that continueunabated leading to
end stage cardiac failure22. Thusit is hypothesized, but not
actually proved thatinitiation of diuretics at this stage, as is
commonlydone nowadays, produces double harm; it not onlyreduces the
natriuretic peptide concentration but alsounleashes the RAAS from
the inhibitory effect ofthe endogenous NEP.
NEP inhibitors have a number of potential advantagesover
conventional diuretics in the treatment of patientswith chronic
heart failure since they do not activateRAAS system. Ample evidence
also suggests thathemodynamic changes attained using these drugsare
decidedly better at least in cases of mild heartfailure when
compared to diuretics. Extrapolation ofthese results to more severe
cases of cardiac failure
141
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]
-
I. BASURAY
is not undesirable; as presently we have some, thoughnot
extensive data advocating their efficacy in suchstates. More
extensive studies are warranted withsubjects in New York Heart
Association class III orIV to collect supporting data. It is also
important torealise that these group of patients are really in
needof more effective pharmacological agents to controlheart
failure. Failure of appropriate pharmacologicalmeasures to treat
such patients makes it inevitablein clinical practice to go for
invasive alternatives likebiventricular pacing.
An additional unique property present in these drugscould be of
clinical importance. The effects of NEPinhibitors are caused by
potentiation of endogenousnatriuretic peptides, so their action
depends on thesecretion of such peptides. It has thus
beenhypothesised but not proved that NEP inhibitors wouldbe most
effective in patients with high peptidesecretion. As the peptide
secretion is related to high
left ventricular preload, such patients are in most needof
diuresis. Thus there is a built-in self regulation; anyevent like
dehydration or diuresis that decreasespreload would automatically
decrease natriureticpeptide secretion and their diuretic effect, so
that thedehydration is not exacerbated. Dehydration is animportant
adverse effect of diuretics that restrict theiruse in heart failure
patients. However there is a flipside to this phenomenon; this may
be also the causeof the rather nonsustained action of these drugs,
whengiven to heart failure patients.
To summarise, the use of NEP inhibitors at variousstages of
heart failure, results in an equitable or evenbetter hemodynamic
changes but not at the cost ofadverse neurohormonal stimulation.
The role of thesedrugs in more severe form of heart failure alone
orin combination, though appears to be promising, isyet to be
tested by clinical trials.
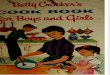
Figure 1. Pathways showing the sites of drug action in heart
failure.
Angiotensinogen Kininogen
Natriuretic peptidase
Kininogenase
ACE
Angiotensinogen I
Angiotensinogen II Bradykinin
Inactivemetabolite
NEP
Inactivemetabolite
ACE inhibitors
Vasoactivepeptidase inhibitors
Facilitates:
Renin
142
NEP inhibitors
Inhibits:
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]
-
NEUTRAL PEPTIDASE INHIBITORS
Future directions: While the salutary effect of ACEinhibitors in
heart failure, in general, and NEPinhibitors in particular, in
changing adverseneurohormonal milieu per se remains
unquestioned,efforts are in progress to develop a chimericmolecule;
called vasopeptidase inhibitors, combiningboth these properties23.
Figure 1 depicts the site ofaction of such drugs. Such molecules
(Table 1),would have both the advantage of antagonising theRAAS and
added natriuresis and diuresis of NEPinhibitors. In principle it is
also expected to haveboth the tremendous mortality and morbidity
benefitsas ACE inhibitors with potent anticongestive powersof loop
diuretics, but devoid of their adverse effects.
Clinical trials with omapatrilat, the combined ACE andNEP
inhibitor has indeed shown it to have betternatriuretic and humoral
(decrease in renin) effectsthan the ACE inhibitor lisinopril24. If
the mortalityamong two recently concluded trials are
comparedomapatrilat exhibited a significant decrease inmortality
when compared to 20 mg/d of lisinopril25.In the just concluded
joint International Society andEuropean Society of Hypertension
meet; the resultsof the massive OCTAVE trial, that
comparedOmapatrilat to Enalapril, another ACE inhibitor
wasannounced. This trial tested; omapatrilat Vs enalaprilin25-27
hypertensive patients recruited from 3298 sitesin 12 countries26.
Though the trial did not have any
Table 1. Combined NEP and ACE inhibitors (vasoactivepeptidase
inhibitors) and their inhibitory activity in various phases of
studies.
Agent Study phase ACE Ki (nmol/L) NEP Ki (nmol/L)
Omapatrilat (BMS186716) III 6 9
Sampatrilat (UK81252) II 1.2 8
Fasidotril (BP1.137) II 9.8 5.1
MDL 100,240 (active metabolite MDL 100,173) I 0.08 0.11
Z13752A I 3.2 1.8
BMS189921 II 12 63
Mixanpril (active metabolite RB105) Preclinical 4.2 1.7
ACE = angiotensin-converting enzyme; Ki = inhibitory constant;
NEP = neutral endopeptidase.
Table 2. Clinical trials showing efficacy of omapatrilat in
varying severity of heart failure.
Heart failure No of patients Treatment Findings(NYHA Class)
II-IV27 369 Omapatrilat 2.5, 5, 10, 20, Dose-dependent reduction
in PCWP,and 40 mg/day SBP/DBP, and SVR, and improvement in
NYHA class
II and III2 8 48 Omapatrilat 2.5, 5-10, 20-40 Dose-dependent
improvement in functionalmg/day status and LVEF
Dose-dependent reduction in SBP/DBPSignificant reduction in
predose serum BNP,epinephrine, and aldosterone.
II-IV29 573 Omapatrilat 10 mg/day Significant benefit of
composite end pointstitrated to 40 mg/day Vs of death,
hospitalization, discontinuation oflisinopril 5 mg/day titrated
study treatment for worsening heart failureto 20 mg/day
SBP=systolic blood pressure; DBP=diastolic blood pressure;
SVR=systemic vascular resistance; LVEF-left ventricular ejection
fraction
143
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]
-
I. BASURAY
heart failure patient as such but the fact thatomapatrilat was a
more effective antihypertensivethan enalapril clearly positions the
drugs to be moreeffective in attenuating changes that lead to
frankheart failure than enalapril. Omapatrilat was foundto have the
same side effect profile as Enalapril,other than the incidence of
Angioedema wasdecidedly more (3.1 times more). This has raisedsome
concern, with FDA withholding its approval forthis particular
agent. There has however been anumber of other trials that has
compared the efficacyof omapatrilat in heart failure. These are
summarizedin Table 2 27-29.
Conclusion
With the elucidation of the neurohumoral mechanismof heart
failure, the realization has dawned thateffective therapy, against
these hormonal changesappropriately modifies the course of heart
failure withapparent decrease in both mortality and morbidity.The
RAAS has been decidedly one of the mostimportant culprits, in the
progressive down hill courseof an untreated heart failure.
Similarly secretion ofNEP is one of the few positive responses of
the bodyagainst the self destructive neurohormonalstimulation that
is active in heart failure. Thus atreatment modality that
effectively attenuates theformer and potentiates the latter would
indeed be amajor pharmacological progress. Preliminary resultswith
such drugs like NEP inhibitors and Omapatrilatconform to the above
expectation. However, giventhe fact that medical practice at the
present time isexclusively evidence based, larger studies with
thesedrugs are warranted to confirm or negate our
positiveexperience with these agents30.
REFERENCES
1. Digitalis Investigation Group. The effect of digoxin
onmortality and morbidity in patients with heart failure. N EngJ
Med 1997;336:525-33.
2. Northridge DB, Jackson NC, Metcalfe MJ, MacFarlane N,Dargie
HJ. Effects of candoxatril, a novel endopeptidaseinhibitor,
compared with frusemide in mild chronic heartfailure. Proceedings
of the British Pharmacological Society,University of Glasgow, July
10-12, 1991. Br J Clin Phar-macol 1991;32:645.
3. Struthers AD. Ten years of natriuretic peptide research: Anew
dawn for their diagnostic and therapeutic use. Br MedJ 1994;308
:1615.
4. Wei CM, Heublein DM, Perella MA, Lerman A, RodehefferRJ,
McGregor CG, et al. Natriuretic peptide system inhuman heart
failure. Circulation 1993;88:1004-9.
5. Yasue H, Yoshimura M, Sumida H, Kilkuta K, Kugiyama
K,Jougasaki M, et al. Localization and mechanism ofsecretion of
B-type natriuretic peptide in comparison withthose of A-type
natriuretic peptide in normal subjects andpatients with heart
failire. Circulation 1994;90:195-203.
6. Stephenson SL, Kenny AJ. The hydrolysis of alpha-humanatrial
natriuretic peptide by pig kidney microvillarmembranes is initiated
by endopeptidase-24.11. BiochemJ 1987; 243:183-7.
7. Ronco P, Pollard H, Galceran M, Delauche M, SchwartzJC,
Verroust P. Distribution of enkephalinase
(membranemetalloendopeptidase, E.C.3.4.24.11) in rat
organs.Detection using a monoclonal antibody. Lab
Invest1988;58:210-7.
8. Shepperson NB, Barclay PL, Bennett JA, Samuels GM.Inhibition
of neutral endopeptidase (E.C.3.4.24.11) leadsto an atrial
natriuretic factor - mediated natriuretic, diureticand hypertensive
response in rodents. Clin Sci 1991;80:265-9.
9. Richards M, Espiner E, Frampton C, Ikram H, Yandle T,Sopwith
M, et al. Inhibition of endopeptidase EC 24.11 inhumans: Renal and
endocrine effects. Hypertension 1990;16:269-76.
10. Elsner D, Muders F, Muntze A, Kromer EP, Forssmann
WG,Riegger GA. Efficacy of prolonged infusion of
urodilatin[ANP-(95-126)] in patients with congestive heart
failure.Am Heart J 1995;129:766-73.
11. Molina CR, Fowler MB, McCrory S, Peterson C, Myers
BD,Schroeder JS, et al. Hemodynamic, renal and endocrineeffects of
atrial natriuretic peptide infusion in severe heartfailure. J Am
Coll Cardiol 1988:12:175-86.
12. Yoshimura M, Yasue H, Morita E, Sakaino M, JougasakiM,
Kurose M, et al. Hemodynamic, renal and hormonalresponses to brain
natriuretic peptide infusion in patientswith congestive heart
failure. Circulation 1991;84:1581-8.
13. Northridge DB, Jardine AG, Alabaster CT, Barcly PL,Connell
JMC, Dargie HJ, et al. Effects of UK 69,578: Anovel atriopeptidase
inhibitor. Lancet 1989;2:591-3.
14. Munzel T, Kurz S, Holtz J, Busse R, Just H, Drexler H, etal.
Neurohormonal inhibition and hemodynamic unloadingduring prolonged
inhibition of ANF degradation in patientswith severe chronic heart
failure. Circulation 1992;86:1089-98.
15. Northridge DB, Newby DE, Rooney E, Norrie J, Dargie
HJ.Comparison of the short-term effects of candoxatril, anorally
active neutral endopeptidase inhibitor, and frusemide
144
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]
-
NEUTRAL PEPTIDASE INHIBITORS
in the treatment of patients with chronic heart failure. AmHeart
J 1999;138:1149-57.
16. Christopher MO, Wendy AG, Christopher BG. A randomizedtrial
of ecadotril versus placebo in patients with mild tomoderate heart
failure: The U.S. Ecadotril Pilot SafetyStudy. Am Heart J
1999;138:1140-8.
17. Francis GS. Is there still a future for neutral
endopeptidaseinhibitors? Am Heart J 1999;138:1007-8.
18. Kahn JC, Patey M, Dubois-Rande JL, Merlet P, CastaigneA,
Lim-Alexandre C, et al. Effect of sinorphan on plasmaatrial
natriuretic factor in congestive heart failure.
Lancet1990;335:118-9.
19. The SOLVD Investigators. Effect of enalapril on mortalityand
the development of heart failure in asymptomaticpatients with
reduced left ventricular ejection fractions. NEng J Med
1992;327:685-91.
20. Cowley AJ, Stainer K, Wynne RD, Rowly JM.
Symptomaticassessment of patients with heart failure:
Double-blindcomparison of increasing doses of diuretics and
captoprilin moderate heart failure. Lancet 1986;2:770-2.
21 Bayliss J, Norell M, Canepa-Anson R, Sutton G, Poole-Wilson
P. Untreated heart failure: Clinical and neuroen-docrine effects of
introducing diuretics. Br Heart J 1987;57:17-22.
22. Francis GS, Benedict C, Johnstone DE, Kirlin PC, NicklasJ,
Liang CS, et al. Related articles, links comparison
ofneuroendocrine activation in patients with left
ventriculardysfunction with and without congestive heart failure.
Asubstudy of the studies of left ventricular dysfunction(SOLVD).
Circulation 1990;82:1724-9.
23. Gros C, Noel N, Souque A. Mixed inhibitors of
angiotensin-converting enzyme (EC 3.4.15.1) and
enkephalinase(E.C.3.4.24.22): Rational design, properties, and
potential
cardiovascular applications of glycopril and alatriopril.
ProcNatl Acad Sci USA 1991;88:4210-4.
24. Kostis JB, Rouleau JL, Pfeffer MA. Beneficial effects
ofvasopeptidase inhibition on mortality and morbidity in
heartfailure: Evidence from the omapatrilat heart failure program.J
Am Coll Cardiol 2000;35:240.
25. Chen HH, Lainchbury JG, Harty G, Burnett JC. Thesuperior,
renal and humoral actions of acute dual NEP/ACE inhibition by
vasopeptidase inhibitor versus ACEinhibition alone in experimental
mild heart failure: Propertiesmediated via potentiation of
endogenous cardiac natriureticpeptides. J Am Coll Cardiol
2000;35:270.
26. Kostis JB. Omapatrilat Cardiovascular TreatmentAssessment
Versus Enalapril (OCTAVE). Abstracts ofHypertension Prague 2002 -
Joint 19th Scientific Meetingof the International Society of
Hypertension and 12thEuropean Meeting on Hypertension, June 23-27,
2002,Prague, Czech Republic. Abstract O018a.
27. Ikram H, McClean DR, Mehta S. Long-term
beneficialhemodynamic and neurohormonal effects of
vasopeptidaseinhibition with omapatrilat in heart failure
[abstract]. J AmColl Cardiol 1999;33:A185.
28. McClean DR, Ikram H, Garlick AH, Richards AM, NichollsMG,
Crozier IG. The clinical, cardiac, renal, arterial andneurohormonal
effects of omapatrilat, a vasopeptidaseinhibitor, in patients with
chronic heart failure. J Am CollCardiol 2000;36:479-86.
29. Rouleau JL, Pfeffer MA, Stewart DJ, Isaac D, Sestier F,Kerut
EK, et al. Comparison of vasopeptidase inhibitor,omapatrilat and
lisinopril on exercise tolerance andmorbidity in patients with
heart failure: IMPRESSrandomised trial.Lancet. 2000;356:615-20.
30. Basu Ray I, Reddy KN. Neutral peptidase inhibitors.
HeartDrug 2001;1:236-40.
145
ATTENTION PLEASE!!!
Abstracts of papers presented at 35th annual conference of IPS,
Gwalior will bepublished in the IJP. Those who wish to publish
their abstract(s) should send a copy ofthe same in MS-Word format
by email (as an attached file). Abstracts should conformto the IJP
format i.e. structured abstract with subheadings (Objective,
Methods, Resultsand Conclusion).
Abstracts should be mailed to [email protected]
[Downloaded free from http://www.ijp-online.com on Saturday,
August 01, 2009]









![Peptido c _citrulin[1]](https://img.pdfslide.net/doc/110x75/556e217cd8b42a6a2c8b505e/peptido-c-citrulin1.jpg)