Embed Size (px)
Citation preview

ICD-10ICD-10 Initial Orientation

PRESENTED BY
Rhonda L. Anderson, RHIA
President
Anderson Health Information Systems, Inc.
940 W. 17th Street, Suite B
Santa Ana, CA 92706
Tel. 714-558-3887 Fax 714-558-1302
Email [email protected]
2

OBJECTIVES
• Participants will identify:– Dates for New ICD-10– Documentation support– New terms encounter principal diagnosis re-
defined– Some general coding guidelines– Will identify the Federal requirements re: ICD-9
changes for this year and coding accuracy.
3

ICD—10 “HAS TWO PARTS”
• ICD-10 CM = Clinical Modification• ICD-10 PCS = Procedural Code System
(used for procedures, operations within the hospital inpatient setting i.e., acute hospital)
4

FINAL REGULATION
• January 15, 2009 Final Regulation Released
• EXCHANGE the ICD-9 for the ICD-10 by October, 1, 2013
• ICD-10 for billing purposes as far as ability to accept the code known as “5010” is required by October 2011
5

HIPAA
• Assigning ICD-10 diagnosis codes is required under the Health Insurance Portability and Accountability Act (HIPAA)
• HIPAA had three parts HIPAA – 1996, HIPAA-II – HITECH we call it – relates to security and breaches
• HIPAA Transactions 5010 • ICD-10 Code Set
6

WHO IS AFFECTED??
• All inpatient and outpatient facility visits as well as freestanding providers and ancillary services “that means all of us really” who provide services and bill for them under Medicare, MediCal and private insurances. Current Procedural
• Terminology (CPT) is still used for the Physician and some services, but they must have a diagnosis that is ICD-10 Complaint
7

KEY HIGHLIGHTS -2
• Healthcare Common Procedural Coding system (HCPCS Level II) remains the same for outpatient reporting for procedures and services.
• ICD-10 code set, general acute care inpatient reimbursement for Medicare patients will be based on Medicare severity-based diagnosis related groups (MS-DRGs) using ICD-10 – CM – PCS (for those who have procedures).
8

WHAT DOES THIS MEAN??
• The guidelines in the ICD-10 manual developed for the provider and the coder….(person who may review the documentation and determine if code is accurate.
• Consistent, complete documentation in the medical record is a major emphasis.
9

KEY HIGHLIGHTS -3
• ICD-10 CM/PCS – Increased level of detail required for medicine advancements in technology, $$, improved data quality for clinical and financial decision making, to support value based purchasing and facilitate quality reporting.
• Mapping from ICD-9 to 10 tools are available and will be used by DCTSS.
• Called or “GEMS” – general equivalence mappings.
10
ICD-9-CM DIAGNOSIS CODES
• 3-5 characters in length• Approximately 14,000 codes• First digit may be alpha (E or V) or numeric• Digits 2-5 are numeric• Always at least three digits• Decimal placed after the first three
characters• Limited space for new codes
11

ICD-9-CM DIAGNOSIS CODES -2
• Lacks detail• Lacks laterality Difficult to analyze dated
due to non-specific and do not adequately define diagnoses needed for medical research
• Does not support interoperability because it is not used in other countries.
12
ICD-10 STRUCTURE
• Index and Tabular list similar to ICD-9• ICD-10 index larger, Categories,
subcategories and codes are contacted in the tabular list.
13

ICD-10 CM STRUCTURE -2
• Requires “use” of proper coding guidelines– Enter website here www._________.com (for
CMS codes for ICD 10)– Relies on the use of the guidelines and in our
case Skilled/ICF rules (more on this subject later during full training)
– ICD-10 CM Index – disease and injury and external causes of injury
14

ICD-10-CM DIAGNOSIS CODES – FORMAT & STRUCTURE
• 3-7 characters in length• Approximately 68,000 codes• Digit 1 is alpha, digit 2 and 3 are numeric;
digit 4-7 are alpha or numeric• Decimal placed after the first 3 characters• All letters used except “U”• Flexible for adding new codes• Very specific• Has laterality
15

ICD-10 CM STRUCTURE -3
• Former V=codes are now Z=codes and in Z=codes and in Chapter 21. Factors Influencing Health Chapter 21. Factors Influencing Health Status and Contact with Health Status and Contact with Health Services (NEW)…Services (NEW)…
16

CONVENTIONS FOR THE ICD-10-CM
• General rules for use of the classification independent of the guidelines– Alphabetic Index and Tabular List
• Alphabetic Index – List of terms and their corresponding code
• Tabular List – chronological list of codes divided into chapters based on body system/condition
17

CONVENTIONS FOR THE ICD-10-CM -2
• General rules for use of the classification independent of the guidelines– Format and Structure
• Three character category that has no further subdivision is equivalent to a code
• Subcategories are either 4 or 5 characters• Codes may be 3, 4, 5, 6 or 7 characters
18

CONVENTIONS FOR THE ICD-10-CM -3
• General rules for use of the classification independent of the guidelines– 7th Characters
• Certain ICD-10-Cm categories have applicable 7th characters
• Required for all codes within the category or as instructed by the notes in the Tabular List
• Must always be the 7th character in the data field• If a code that requires a7th character is not 6
characters, a placeholder X must be used to fill in the empty characters
19
ICD-10-CM DIAGNOSIS CODES-2
• Specificity improves coding accuracy and depth of data for analysis
• Detail improves the accuracy of data used in medical research
• Supports interoperability and the exchange of health care data between other countries and the U.S.
20

CODE STRUCTURE OF ICD-10
• ICD-10 Codes may consist of up to 7 digits, with the 7th digit extensions representing visit encounter or sequel for injuries or external causes.
21
CODE FORMAT
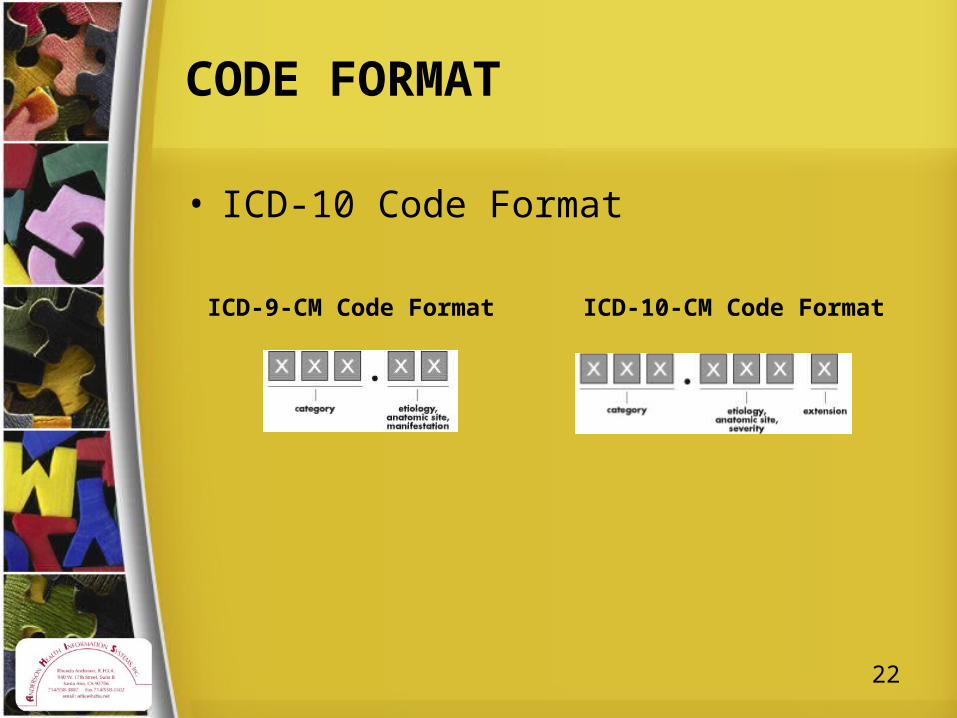
• ICD-10 Code Format
ICD-9-CM Code Format ICD-10-CM Code Format
22
GEM FILES
• Before we go further- do not despair…you vendor should prepare as much crosswalk as possible. There are “GEMS” files.
• General Equivalence Mappings (GEMS) – translation dictionary for diagnoses
• We will talk about those later and how to use them.. Key to early review!!!
• Your vendor will most likely provide
23

ICD-10 AND ICD-9 DIFFER
• Organization• Structure, • Code composition,• Level of detail• May consist of up to 7 digits with the
seventh digit extensions representing visit encounter or sequel as stated above.
24

ICD-10 AND ICD-9 DIFFER
• Includes full code titles and no reference back to common 4th and 5th digits)
• V and E codes are no longer supplemental
25

ABBREVIATIONS
• NEC – “Not elsewhere classifiable• Punctuation
– [ ] Brackets– ( ) Parentheses
• Use of “and”• “Other” or “other specified” • “Unspecified”• “Includes Notes”• “Inclusion Terms”
26

ABBREVIATIONS -2
• “Excludes Notes”• “Code first”, “Use additional code” and
“elsewhere notes”• “And”, “and” or “or”• “With”• “See”, “see also”• “Code also note”• “Default codes”• “Syndromes”
27

GENERAL CODING GUIDELINES
• Locating a code in the ICD-10-CM• Level of detail coding• Code/codes from A00.0 through T88.9,
Z00-Z99.8• Signs and symptoms
28

GENERAL CODING GUIDELINES
• Multiple coding for a single condition– “Use additional code”
• Sequencing rule is the same as the etiology/manifestation pair
29

GENERAL CODING GUIDELINES
• Acute and Chronic Conditions• Combination Code• Late Effects (Sequela)
– Residual effect (condition produced) after the acute phase of an illness/injury terminated
– Condition/nature of the late effect is sequenced; late effect code is second
– Acute phase of an illness/injury• Sequelae of complication of pregnancy• See Section 1.C.19. Code extensions
30

GENERAL CODING GUIDELINES
• Documentation for BMI and Pressure Ulcer Stages– Assignment may be based on medical record
documentation from clinicians who are not the patient’s provider
– Physician / qualified healthcare practitioner legally accountable for establishing the patient’s diagnosis
– Dietitian often documents the BMI and nurses often documents the pressure ulcer stages
31

GENERAL CODING GUIDELINES
• Documentation for BMI and Pressure Ulcer Stages– Associated diagnosis such as overweight,
obesity, pressure ulcer must be documented by the patient’s provider
– Conflicting medical record documentation queried for clarification
– BMI codes should only be reported as secondary diagnoses
32

ICD-10 NEW FEATURES
• Combination Codes for Condition s and Common Symptom or Manifestations
• I25.110 - Arteriosclerotic heart disease of native coronary artery with unstable angina pectoris
33

ICD-10 NEW FEATURES -2
• Added Laterality– C50.212 Malignant neoplasm of upper-inner
quadrant of left female breast– H02.835, Dermatochalasis of left lower eyelid– I80>01, Phlebitis and thrombophlebitis of
superficial vessels of right lower extremity– L80.213, Pressure Ulcer of right hip, Stage III
34

A FEW CODES YOU WILL LEARN
• Pg 479 of the ICD-10 manual• A41.9 Sepsis without cause organism –
Sepsis, unspecified• Severe Sepsis – A41.9 Sepsis unspecified
for the infection. Additional code for organ must be identified.
• UROSEPSIS is not allowed as a dx.
35

A FEW CODES YOU WILL LEARN-2
• Septic Shock– Circulatory failure associated with severe
sepsis; represents a type of acute organ dysfunction. Underlying infection sequenced first, followed by code R65.21 Severe sepsis with septic shock. Add additional codes for other acute organ dysfunction
• New guidelines for sequencing Severe Sepsis
• Must be clear if it is present on admission
36

ICD-10 NEW FEATURES
• Expanded Codes (injury, diabetes alcohol/substance abuse, postoperative complications)
• E08.22 Diabetes due to underlying condition with diabetic chronic kidney disease
37

CHAPTER 4 – E00-E89
• Endocrine, nutritional and metabolic diseases– Diabetes Mellitus
• Combination codes• Includes the body system affected and complications
affecting the body system• Many codes particular category as are necessary to
describe all of the complications of the disease may be used
• Sequenced base on the reason for a particular encounter
38

CHAPTER 4 – ENDOCRINE, NUTRITIONAL…(E00-E89)
• Endocrine, nutritional and metabolic diseases– Secondary Diabetes Mellitus
• Category E08 due to underlying condition• Category E09 for drug/chemical induced• Use code Z79.4 for patients who routinely use insulin;
also assigned for long-term (current) use
39

CHAPTERS 5 – 8
• Chapter 5 – Mental (F01-F99)– See Section 1.C.6. Pain
• Chapter 6 – Diseases of Nervous System (G00-G99)
• Chapter 7 – Disease s of Eye and Adnexa (F00-F59)
• Chapter 8 – Disease of Ear and Mastoid (H60-H95)
40

CHAPTER 9 – DISEASES OF CIRCULATORY SYS. (I00-I99)
• Hypertension with Heart Disease– Heart conditions classified to I50 or I51.4-I51.9
are assigned to, a code from category I11 when a causal relationship is stated (due to hypertension) or implied (hypertensive)
– Use an additional code from category I50– Heart failure, to identify the type of heart failure
41

CHAPTER 9 – DISEASES OF CIRCULATORY SYS. (I00-I99)
• Hypertensive Cerebrovascular Disease– Assign the appropriate code from categories
I60-I69, followed by the appropriate hypertension code
42

CHAPTER 10 – DISEASES OF RESPIRATORY SYS. (J00-J99)
• Chronic Obstructive Pulmonary Disease (COPD) and Asthma– Acute exacerbation of chronic obstructive
bronchitis and asthma– J44 and J45 distinguish between uncomplicated
cases and those in acute exacerbation
• Acute Respiratory Failure– Principle diagnosis when it is the condition
established after study to be chiefly responsible
43

CHAPTER 10 – DISEASES OF RESPIRATORY SYS. (J00-J99)
• Influenza due to certain identified influenza viruses– Only on confirmed cases (J09.0)– Avian influenza or novel H1N1 or swine flu,
code J09.1
44

CHAPTERs 11 & 12
• Chapter 11 – Diseases of Digestive System (K00-k94)
• Chapter 12 – Diseases Of Skin
45

CHAPTER 13 – DISEASE OF MUSCULOSKELETAL (M00-M99)
• Site and laterality– Designations– Represents the bone, joint or the muscle– Where more than one bone, joint or muscle is
involved, such as osteoarthritis, use the assigned “multiple sites” code; if not available, use multiple codes to indicate the sites
– Bone vs. Joint – Certain conditions where the bone may be affected at the upper & lower end; site designation will be the bone, not the joint
46

ICD-10 NEW FEATURES-4
• Laceration with foreign body of the abdominal wall, right lower quadrant w/penetration—an extension used with a laceration code. (all the description is written out) S31.623A
47

CHAPTER 14 – DISEASES OF GENITOURINARY (N00-N99)
48

ICD-10 NEW FEATURES -2
• Laceration with foreign body of the abdominal wall, right lower quadrant with penetration, an extension used with a laceration code. (All the description is written out – S31.623A.)
• Fracture Codes require a seventh character that identified if the fracture is open or closed for an initial encounter or if a subsequent encounter is for routine healing, delayed healing, nonunion, malunion or sequelae.
49

LET’S SEE SOME CODES
• Hypertensive Cerebrovascular Disease• First assign the code from I60-169
followed by hypertension Code• Cerebral atherosclerosis• I69.34 Monoplegia of lower limb following
cerebral infarction • I11.9, Hypertensive heart disease without
heart failure or W/heart failure I11.0
50

LET’S SEE SOME CODES
• Sequencing of codes is determined by the reason for admission/encounter - Hypertensive Retinopathy– H35.03 Hypertensive Retinopathy– 031-Right eye, 032, left eye, 033, bilateral,– 039 unspecified (and this would be a ?? For
billing most likely)!!– I10, Essential Primary Hypertension
51

ICD-10 NEW FEATURES -3
• An example S42.321A. Displaced transverse fracture of shaft of humerus, right arm, initial encounter for closed fracture.
• This means more specific documentation from the physician (the initial encounter may not have been in your setting).
52

CHAPTER 18
• Symptoms, Signs and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (R00-R99)
53

REPEATED FALLS
• Code R29.6 Repeated falls for use for encounters when a patient has recently fallen and the reason for the fall is being investigated. Code Z91.81, History of falling, is for use when a patient has fallen in the past is at risk for future falls. Both codes may be assigned
54

CODING OF TRAUMATIC FRACTURES
• Fractures of specified sites are coded individually by site..S-codes…need to pay attention to level of detail furnished by medical record content.
• Fracture not indicated as open or closed, displaced, initial vs. subsequent encounter for fractures. (use 7th character extension for initial encounter (A.B.C) There are specific instructions related to this area. (#18)
55

FRACTURES
• Multiple fractures are sequenced based on the severity of the fracture.
56

AFTERCARE
• Visit codes cover situations when the initial treatment of a disease has been performed and the patient requires continued care during the healing or recovery phase or the long term consequences of the disease
• Z code should not be used if treatment is directed at a current acute disease
57

AFTERCARE
• Exceptions– First listed, followed by the diagnosis code
when a patient’s encounter is solely to receive radiation therapy
58
PRINCIPAL DIAGNOSIS
• Hospital Discharge Data Set (UHDDS) defines as that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care
59

PRINCIPAL DIAGNOSIS -2
• Codes for symptoms, signs, and ill-defined conditions – NOT to be used as a principal diagnosis when definitive diagnosis has been established.
60

PRINCIPAL DIAGNOSIS -3
• Two or more interrelated conditions with either one meeting the definition– Such as diseases in the same ICD-10-CM or
manifestations characteristically associated with a certain disease) potentially meeting the definition of principal diagnosis, either condition may be sequenced first, unless the circumstances of the admission, the therapy provided, the Tabular List, or the Alphabetic Index indicate otherwise
61

PRINCIPAL DIAGNOSIS -4
• Two or more interrelated conditions equally meeting the definition– Determined by the circumstances of
admission, diagnostic workup and/or therapy provided, and the Alphabetic Index, Tabular List, or another coding guidelines does not provide sequencing direction, any one of the diagnoses may be sequenced first
62

PRINCIPAL DIAGNOSIS -5
• Two or more comparative or contrasting condition– Coded as if the diagnoses were confirmed and
the diagnoses are sequenced according to the circumstances of the admission
– Either diagnosis may be sequenced first
• Symptom(s) followed by contrasting/comparative diagnoses– Code is sequenced first
63

PRINCIPAL DIAGNOSIS -6
• Complications of surgery and other medical care– Is sequenced as the principal diagnosis
• Uncertain Diagnosis– “probable”, “suspected”, “likely”, “questionable”,
“possible”, or “still to be ruled out”, or other similar terms indicating uncertainty, code the condition as if it existed/established
– Applicable only to inpatient admissions to short-term, acute, long-term care & psychiatric hospitals
64

CHAPTER 21 –Z CODES
• Factors Influencing Health Status and Contact With Health Services
• Vaccinations
65

IN FOCUS FOR ACCURACY OF CODING
66

ICD-9 CODE CHANGES AND MORE ON CODING ACCURACY
• Contact AHIS for a specialized Webinar on ICD09 Coding Accuracy and Updates
67

REQUIREMENTS
• Official coding guidelines require the use of V codes for aftercare and specify that applicable aftercare V-codes are to be used for conditions requiring continued / long term care or healing phase of a condition/disease.
68
REQUIREMENTS -2
• The official coding guidelines are developed by CMS (Centers for Medicare and Medicaid Services) & NCHS (National Center for Health Statistics) and updated in October and April of every year. http://www.cdc.gov/nchs/data/icd9/icdguide10.pdf
69

CMS MANUAL SYSTEM TRANSMITTAL 437
• Principal Diagnosis Code - SNFs enter the ICD-9-CM code for the principal diagnosis in FL 67. The code must be reported according to Official ICD-9-CM Guidelines for Coding and Reporting, as required by the Health Insurance Portability and Accountability Act (HIPAA), including any applicable guidelines regarding the use of V codes. The code must be the full ICD-9-CM diagnosis code, including all five digits where applicable.
70

CMS MANUAL SYSTEM TRANSMITTAL 437 -2
• Other Diagnosis Codes Required – The SNF enters the full ICD-9-CM codes for up to eight additional conditions in FLs 68-75. Medicare does not have any additional requirements regarding the reporting or sequence of the codes beyond those contained in the ICD-9-CM guidelines.
71

30 – BILLING SNF PPS SERVICES
• (REV. 2011, ISSUED: 07-30-10, EFFECTIVE: 01-01-11, IMPLEMENTATION: 01-03-11)
• Principal Diagnosis Code - SNFs enter the ICD-CM code for the principal diagnosis in the appropriate form locator. The code must be reported according to Official ICD-CM Guidelines for Coding and Reporting, as required by the Health Insurance Portability and Accountability Act (HIPAA), including any applicable guidelines regarding the use of V codes. The code must be the full ICD-CM diagnosis code, including all five digits where applicable.
72

30 – BILLING SNF PPS SERVICES -2
• Other Diagnosis Codes Required – The SNF enters the full ICD-CM codes for up to eight additional conditions in the appropriate form locator. Medicare does not have any additional requirements regarding the reporting or sequence of the codes beyond those contained in the ICD-CM guidelines.
73

WHAT THIS MEANS TO YOU
• The Principal diagnosis can no longer be an acute diagnosis and it may be a V-CODE
• 800.XX codes for fractures are NO LONGER used
74
DEFINITION OF PRINCIPAL DIAGNOSIS
• “FIRST LISTED DIAGNOSES” is the diagnosis that is chiefly responsible for the admissions to, continued residence in the nursing facility and the diagnosis that support the reimbursement and should be sequenced first.”
• Medicare – To be covered the extended services must be for the treatment of a condition for which the resident received inpatient hospital services during the 3-day qualifying stay
75

TYPE OF CODES USED IN LTC
• Aftercare – used when the initial treatment of a disease or injury has been performed and the patients still requires continued care to heal or recover.
• Late Effects – a late effect is a residual condition that remains and requires medical evaluation, rehab treatments and/or nursing care after the initial illness or injury.
76

WHAT TO CODE?
ALL CONDITIONS THAT EXIST AT THE TIME OF ADMISSION, THAT EFFECT
TREATMENT RECEIVED
77

LOCATING THE PRINCIPAL DIAGNOSIS
78

ADMISSIONS/ENCOUNTERS FOR REHABILITATION
• When the purpose for the admission/encounter is rehabilitation, sequence the appropriate V code from category V57, Care involving use of rehabilitation procedures, as the principal/first-listed diagnosis. The code for the condition for which the service is being performed should be reported as an additional diagnosis.
79

V57 – CARE INVOLVING REHAB
• Category V57 does not indicate that rehab services were provided, only that the resident was admitted for this purpose
80

AFTERCARE
• Aftercare are used when the initial treatment has been performed but the patient continues to need care during the healing / recovery phase
• Examples: – Aftercare following surgery – Physical and/or occupational therapy – Aftercare for healing traumatic fracture
81

POP QUIZ
82
25
43
6
1

POP QUIZ ANSWERS
83
25
43
6
1
Phalanges
Optical Nerve
Tibial Distal
Nares
Sternum
Left Upper Humerus

CERTIFICATE & EVALUATION
• Certificate will be sent upon receipt of evaluation
• Email to [email protected]
84

Rhonda Anderson, RHIA
President, AHIS
Email: [email protected]
Mobile: 714-299-0573
Office: 714-558-3887
YOUR ATTENDANCE IS APPRECIATED!!!
85