Embed Size (px)
Citation preview
ICD Basics and BeyondICD Basics and Beyond
ICD Diagnostics: Making the most of it
Dulce Obias-Manno RN, BSN, MHSA, FHRS, CCDS, CEPSCardiac Arrhythmia Center, Device Clinic
Washington Hospital Center, Washington DC
Objectives
The participant will recognize the value f ICD di ti d tof ICD diagnostic data
The participant will learn how to use diagnostic data efficiently at follow-upg y p
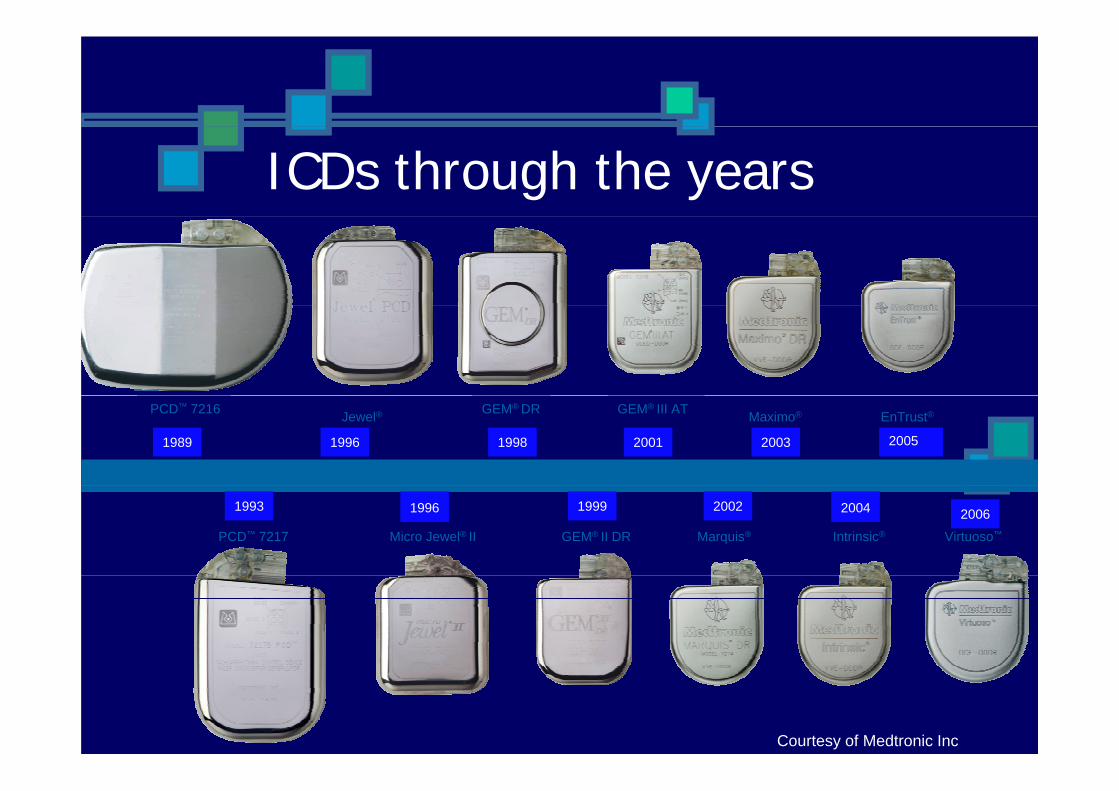
ICDs through the years
GEM® DR
1998
Jewel®
1996
PCD™ 7216
1989
GEM® III AT
2001
Maximo®
2003
EnTrust®
2005
GEM® II DR
1999
Micro Jewel® II
1996
PCD™ 7217
1993
Marquis®
2002
Intrinsic®
2004
Virtuoso™
2006
Courtesy of Medtronic Inc
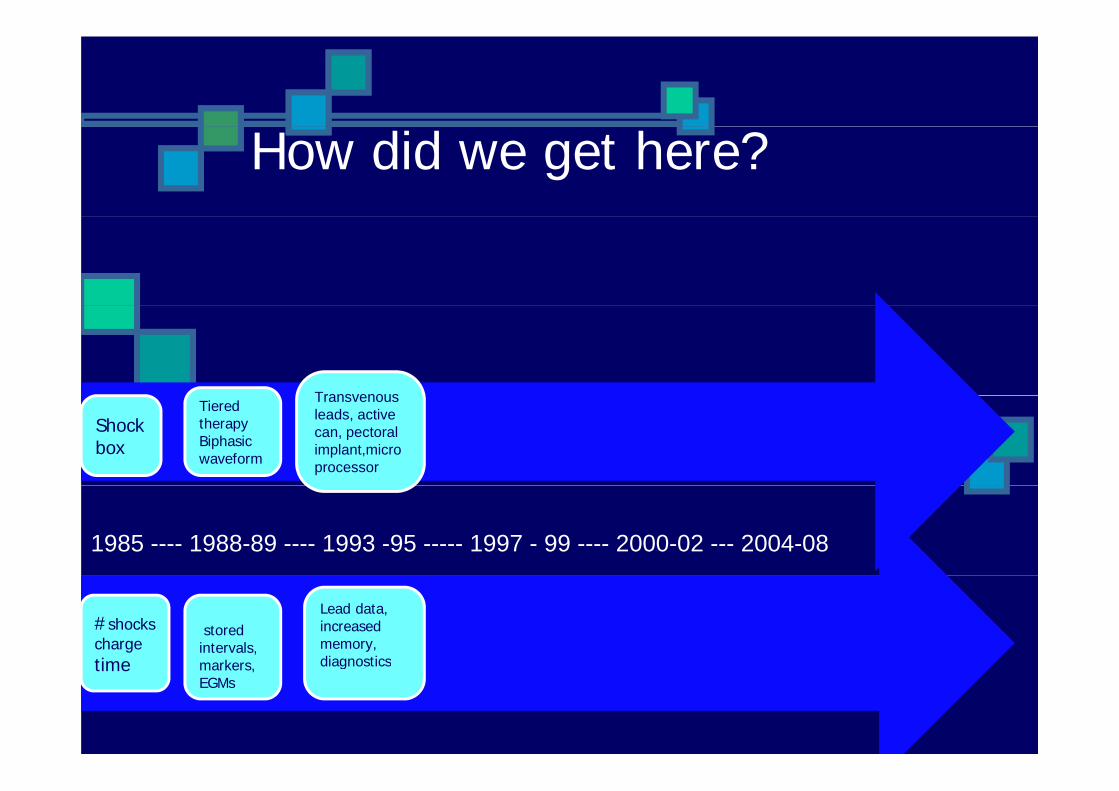
How did we get here?
TransvenousTransvenous leads, active can, pectoral implant,microprocessor
Tiered therapy Biphasic waveform
Shockbox
1985 ---- 1988-89 ---- 1993 -95 ----- 1997 - 99 ---- 2000-02 --- 2004-08
stored intervals, markers
#shocks charge time
Lead data, increased memory, diagnosticsmarkers,
EGMstime diagnostics
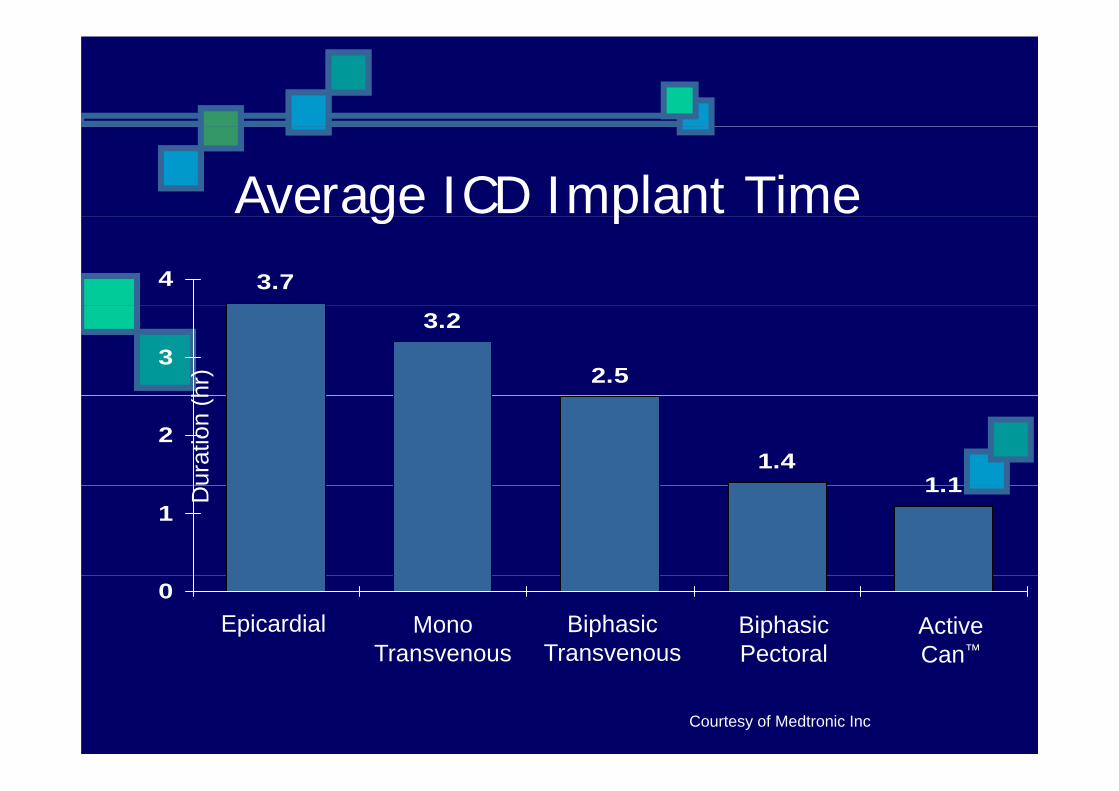
Average ICD Implant Timeg p3.74
3.2
2.53
hr)
1.41 1
2
urat
ion
(h
1.11
D
0Epicardial Mono
TransvenousBiphasic
TransvenousBiphasicPectoral
ActiveCan™
Courtesy of Medtronic Inc
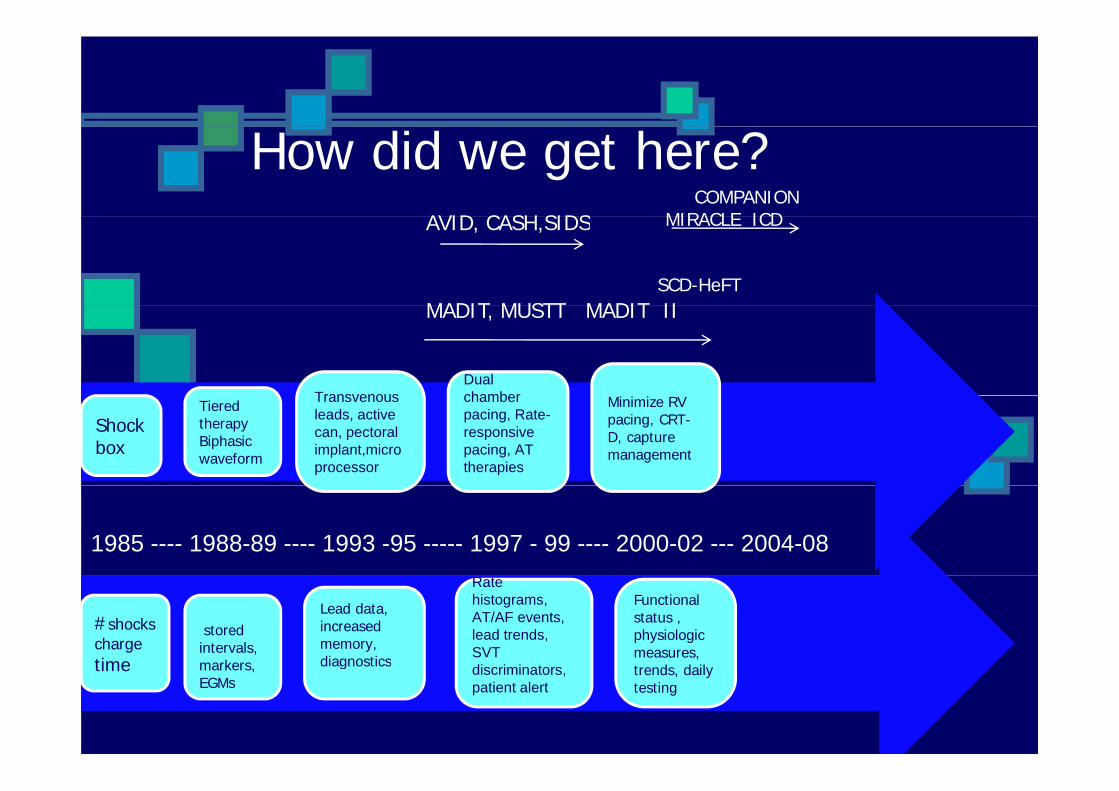
How did we get here?AVID CASH SIDS
COMPANION MIRACLE ICD
MADIT MUSTT MADIT IISCD-HeFT
AVID, CASH,SIDS MIRACLE ICD
TransvenousDual chamber
MADIT, MUSTT MADIT II
Transvenous leads, active can, pectoral implant,microprocessor
chamber pacing, Rate-responsive pacing, AT therapies
Minimize RV pacing, CRT-D, capture management
Tiered therapy Biphasic waveform
Shockbox
1985 ---- 1988-89 ---- 1993 -95 ----- 1997 - 99 ---- 2000-02 --- 2004-08
stored intervals, markers
Rate histograms, AT/AF events, lead trends, SVT di i i t
#shocks charge time
Lead data, increased memory, diagnostics
Functional status , physiologic measures, t d d ilmarkers,
EGMsdiscriminators, patient alert
time diagnostics trends, daily testing
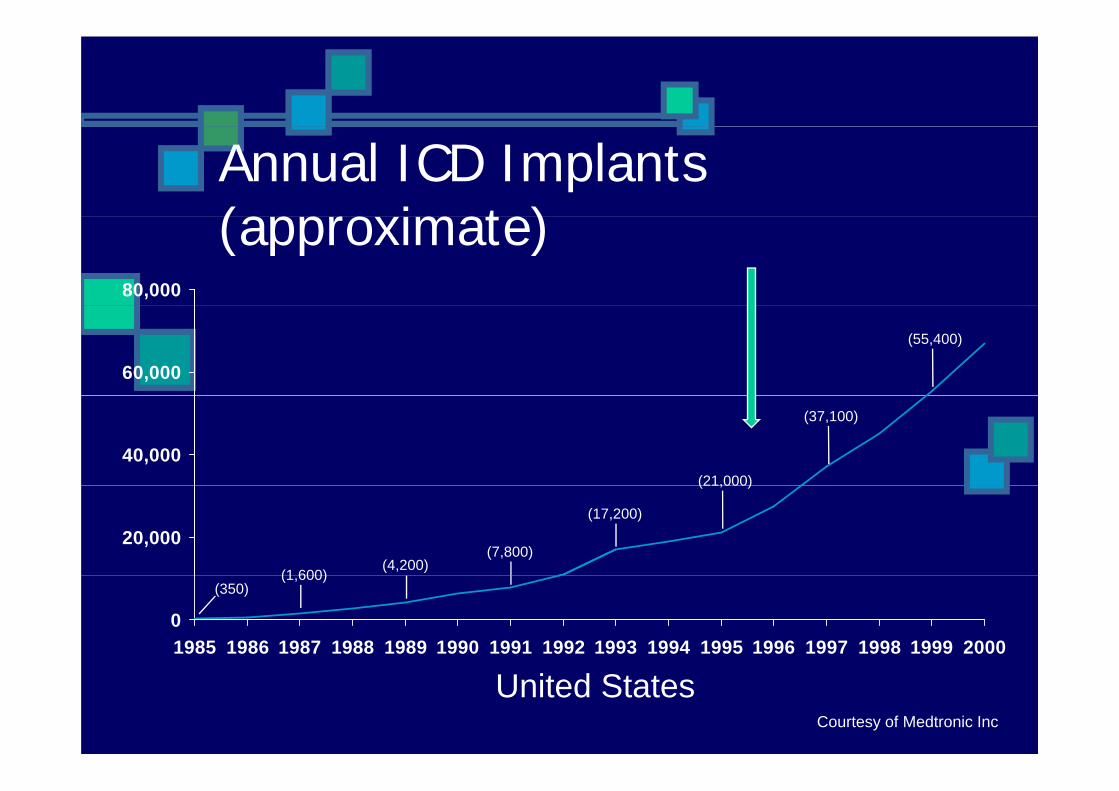
Annual ICD Implants (approximate)(approximate)
80,000
60,000
(55,400)
40,000(21,000)
(37,100)
20,000
(1 600)(4,200)
(7,800)
(17,200)
(21,000)
01985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
(350)(1,600)
United StatesCourtesy of Medtronic Inc
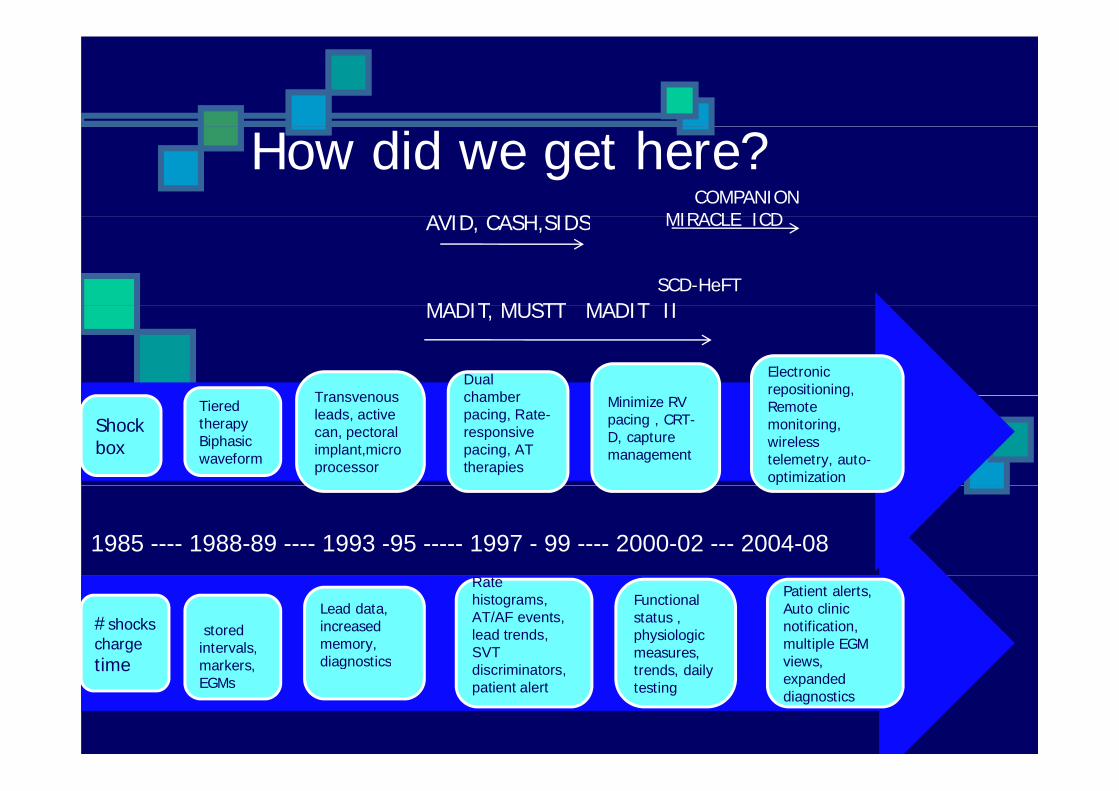
How did we get here?AVID CASH SIDS
COMPANION MIRACLE ICD
MADIT MUSTT MADIT IISCD-HeFT
AVID, CASH,SIDS MIRACLE ICD
TransvenousDual chamber
Electronic repositioning,
MADIT, MUSTT MADIT II
Transvenous leads, active can, pectoral implant,microprocessor
chamber pacing, Rate-responsive pacing, AT therapies
Minimize RV pacing , CRT-D, capture management
p g,Remote monitoring, wireless telemetry, auto-optimization
Tiered therapy Biphasic waveform
Shockbox
1985 ---- 1988-89 ---- 1993 -95 ----- 1997 - 99 ---- 2000-02 --- 2004-08
stored intervals, markers
Rate histograms, AT/AF events, lead trends, SVT di i i t
#shocks charge time
Lead data, increased memory, diagnostics
Functional status , physiologic measures, t d d il
Patient alerts, Auto clinic notification, multiple EGM views,markers,
EGMsdiscriminators, patient alert
time diagnostics trends, daily testing
views, expanded diagnostics
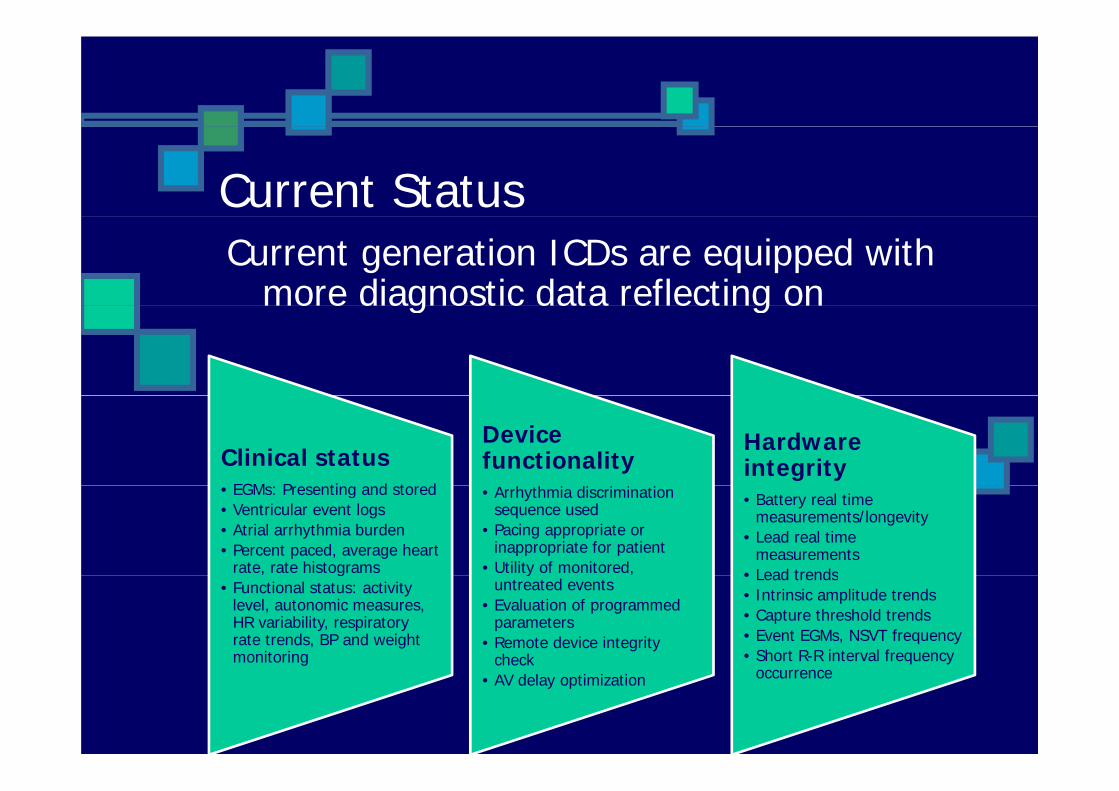
Current Status Current generation ICDs are equipped with
more diagnostic data reflecting ono e d ag ost c data e ect g o
Clinical statusEGM P ti d t d
Device functionality
Hardware integrity
• EGMs: Presenting and stored• Ventricular event logs• Atrial arrhythmia burden• Percent paced, average heart
rate, rate histograms
• Arrhythmia discrimination sequence used
• Pacing appropriate or inappropriate for patient
• Utility of monitored,
• Battery real time measurements/longevity
• Lead real time measurements
• Lead trends, g• Functional status: activity
level, autonomic measures, HR variability, respiratory rate trends, BP and weight monitoring
y ,untreated events
• Evaluation of programmed parameters
• Remote device integrity check
• Lead trends• Intrinsic amplitude trends• Capture threshold trends• Event EGMs, NSVT frequency• Short R-R interval frequency g check
• AV delay optimization occurrence
Increased diagnostic data: B l i th d d thBalancing the good and the badbad
TimeSupplementary data source
Increased battery drain
Time consuming
Overwhelming
Increased diagnostic data: Balancing the good and theBalancing the good and the bad
TimeSupplementary data source
Increased battery drain
Improved battery technology Time consuming
Overwhelming
Improved battery technology
Effici
O ti i
ienc
Optimize
Customizey
Tips for optimizing diagnostic data
•Start with the fundamentals
Summary of events andSummary of events and parameters, presenting EGM, measured values, capture and
i d bsensing data, battery status
•Enhance clinical diagnostics with patient reported symptoms
h th i di i i tiarrhythmia discrimination, arrhythmia burden, lead and
event trends
Summary of events andSummary of events and parameters, presenting EGM, measured values, capture and
i d bsensing data, battery status
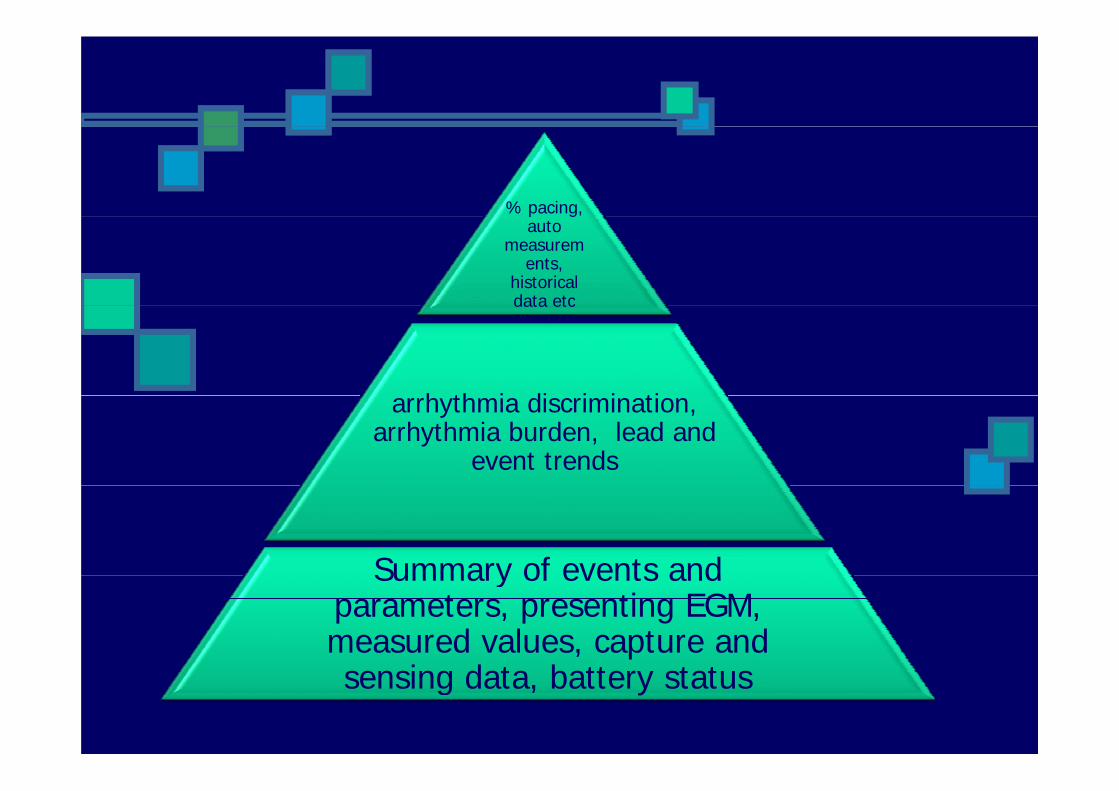
% pacing, p g,auto
measurements,
historical data etc
h th i di i i ti
data etc
arrhythmia discrimination, arrhythmia burden, lead and
event trends
Summary of events andSummary of events and parameters, presenting EGM, measured values, capture and
i d bsensing data, battery status
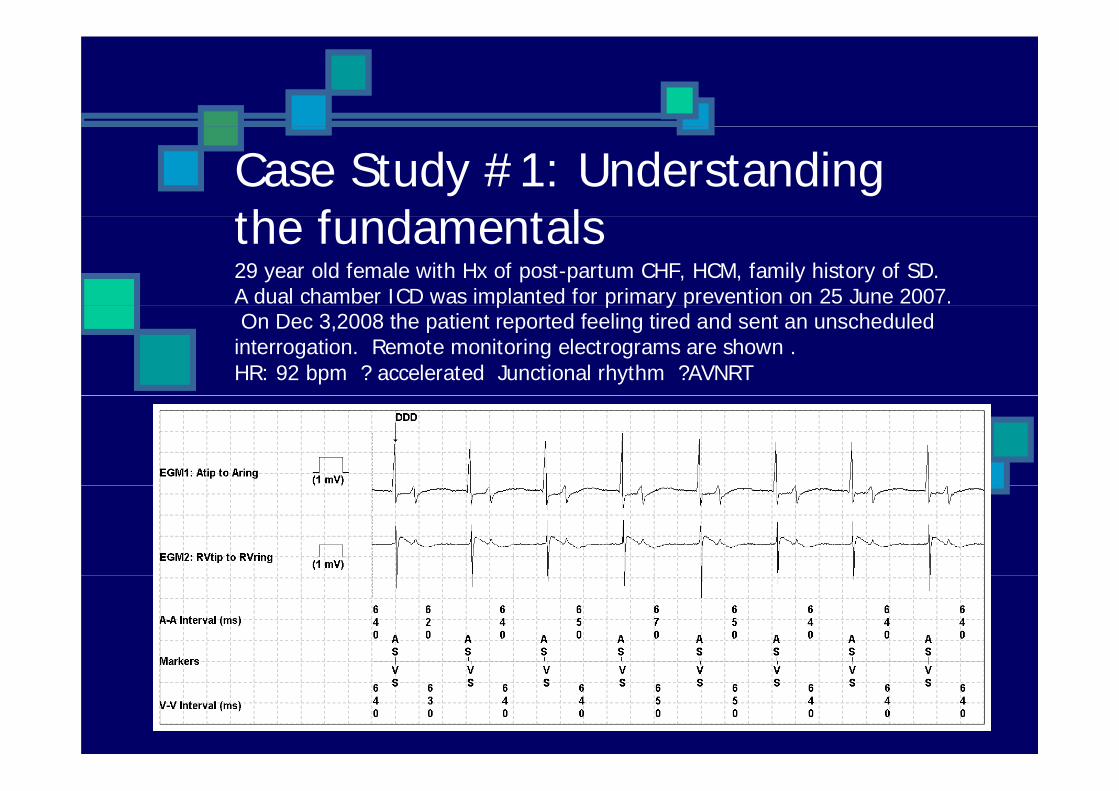
Case Study #1: Understanding th f d t lthe fundamentals29 year old female with Hx of post-partum CHF, HCM, family history of SD. A dual chamber ICD was implanted for primary prevention on 25 June 2007.p p y pOn Dec 3,2008 the patient reported feeling tired and sent an unscheduled
interrogation. Remote monitoring electrograms are shown . HR: 92 bpm ? accelerated Junctional rhythm ?AVNRT
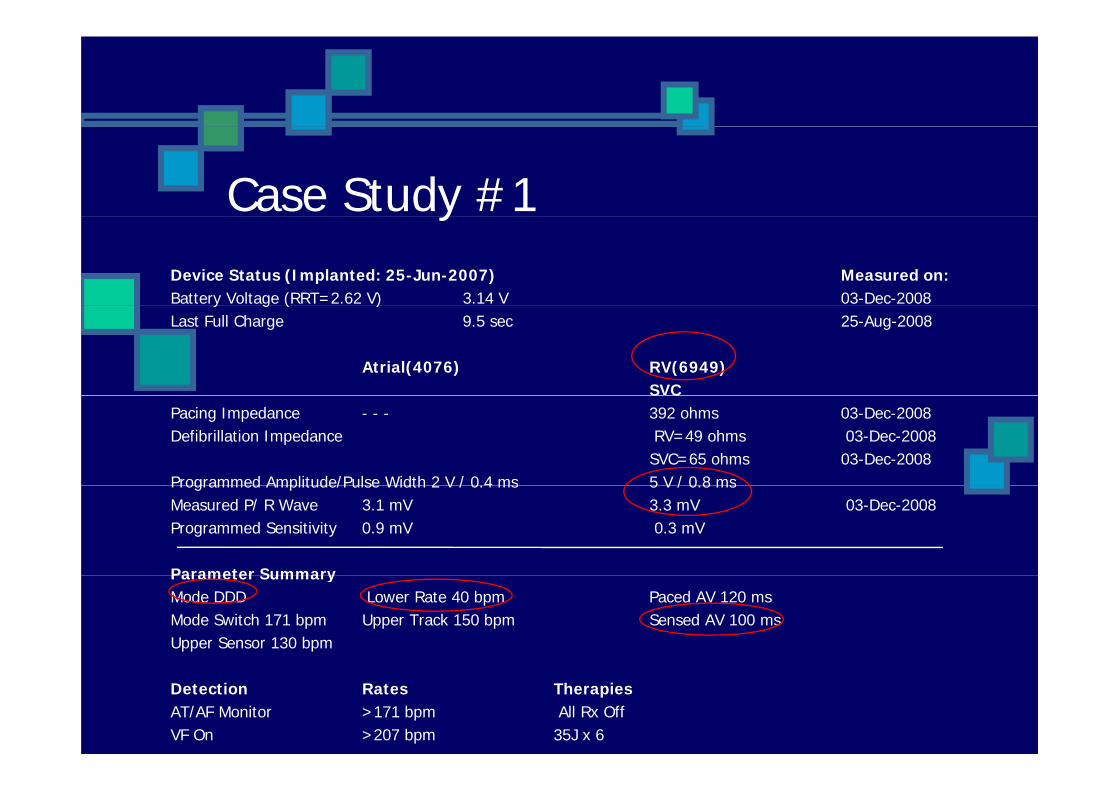
Case Study #1yDevice Status (Implanted: 25-Jun-2007) Measured on:Battery Voltage (RRT=2.62 V) 3.14 V 03-Dec-2008y g ( )Last Full Charge 9.5 sec 25-Aug-2008
Atrial(4076) RV(6949)SVCS C
Pacing Impedance - - - 392 ohms 03-Dec-2008Defibrillation Impedance RV=49 ohms 03-Dec-2008
SVC=65 ohms 03-Dec-2008Programmed Amplitude/Pulse Width 2 V / 0.4 ms 5 V / 0.8 msProgrammed Amplitude/Pulse Width 2 V / 0.4 ms 5 V / 0.8 msMeasured P/ R Wave 3.1 mV 3.3 mV 03-Dec-2008Programmed Sensitivity 0.9 mV 0.3 mV
Parameter SummaryParameter SummaryMode DDD Lower Rate 40 bpm Paced AV 120 msMode Switch 171 bpm Upper Track 150 bpm Sensed AV 100 msUpper Sensor 130 bpm
Detection Rates TherapiesAT/AF Monitor >171 bpm All Rx OffVF On >207 bpm 35J x 6
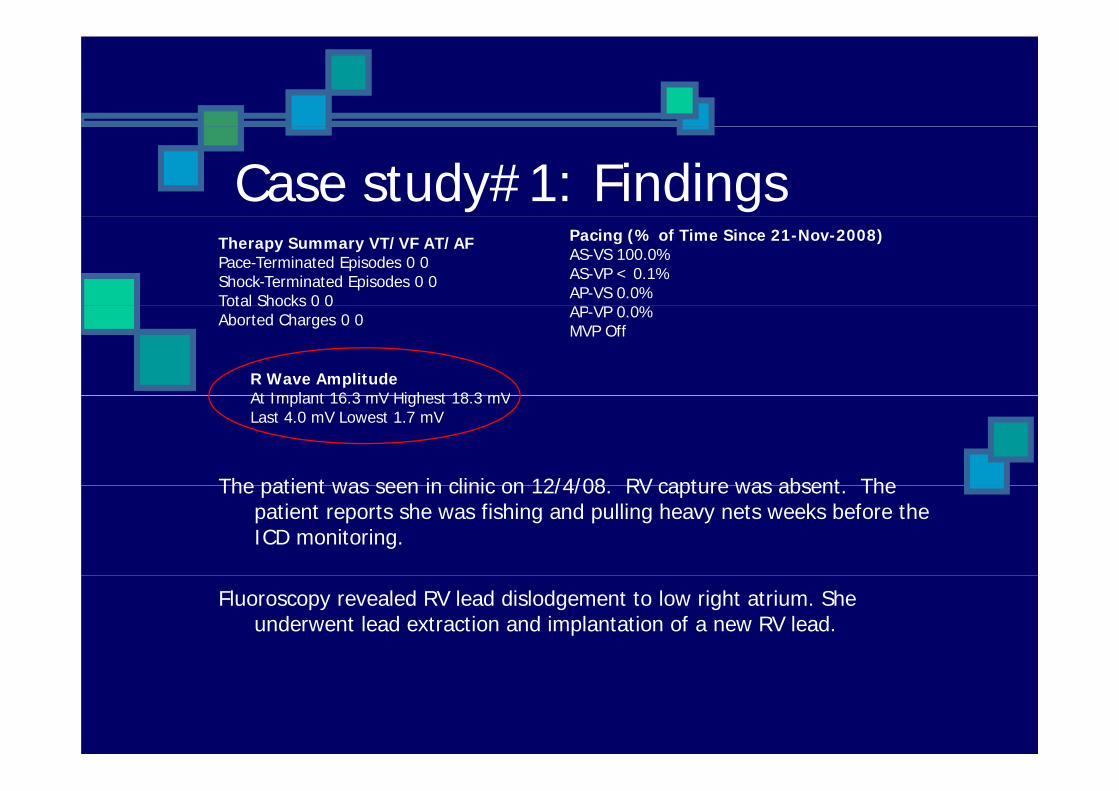
Case study#1: FindingsTherapy Summary VT/VF AT/AFPace-Terminated Episodes 0 0Shock-Terminated Episodes 0 0Total Shocks 0 0
Pacing (% of Time Since 21-Nov-2008)AS-VS 100.0%AS-VP < 0.1%AP-VS 0.0%AP VP 0 0%
Total Shocks 0 0Aborted Charges 0 0 AP-VP 0.0%
MVP Off
R Wave AmplitudeAt Implant 16 3 mV Highest 18 3 mV
The patient was seen in clinic on 12/4/08 RV capture was absent The
At Implant 16.3 mV Highest 18.3 mVLast 4.0 mV Lowest 1.7 mV
The patient was seen in clinic on 12/4/08. RV capture was absent. The patient reports she was fishing and pulling heavy nets weeks before the ICD monitoring.
Fluoroscopy revealed RV lead dislodgement to low right atrium. She underwent lead extraction and implantation of a new RV lead.
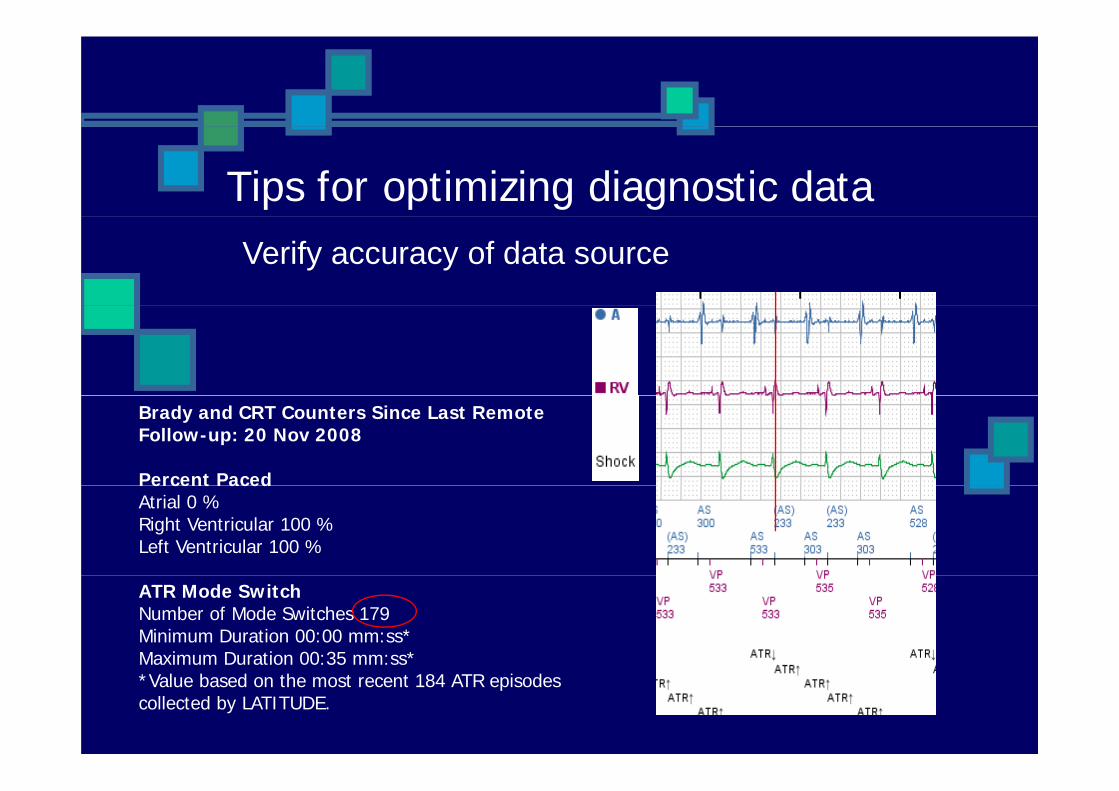
Tips for optimizing diagnostic dataVerify accuracy of data source
Brady and CRT Counters Since Last Remote Follow-up: 20 Nov 2008
Percent PacedPercent PacedAtrial 0 %Right Ventricular 100 %Left Ventricular 100 %
ATR Mode SwitchNumber of Mode Switches 179Minimum Duration 00:00 mm:ss*Maximum Duration 00:35 mm:ss*a u u a o 00 35 ss*Value based on the most recent 184 ATR episodes collected by LATITUDE.
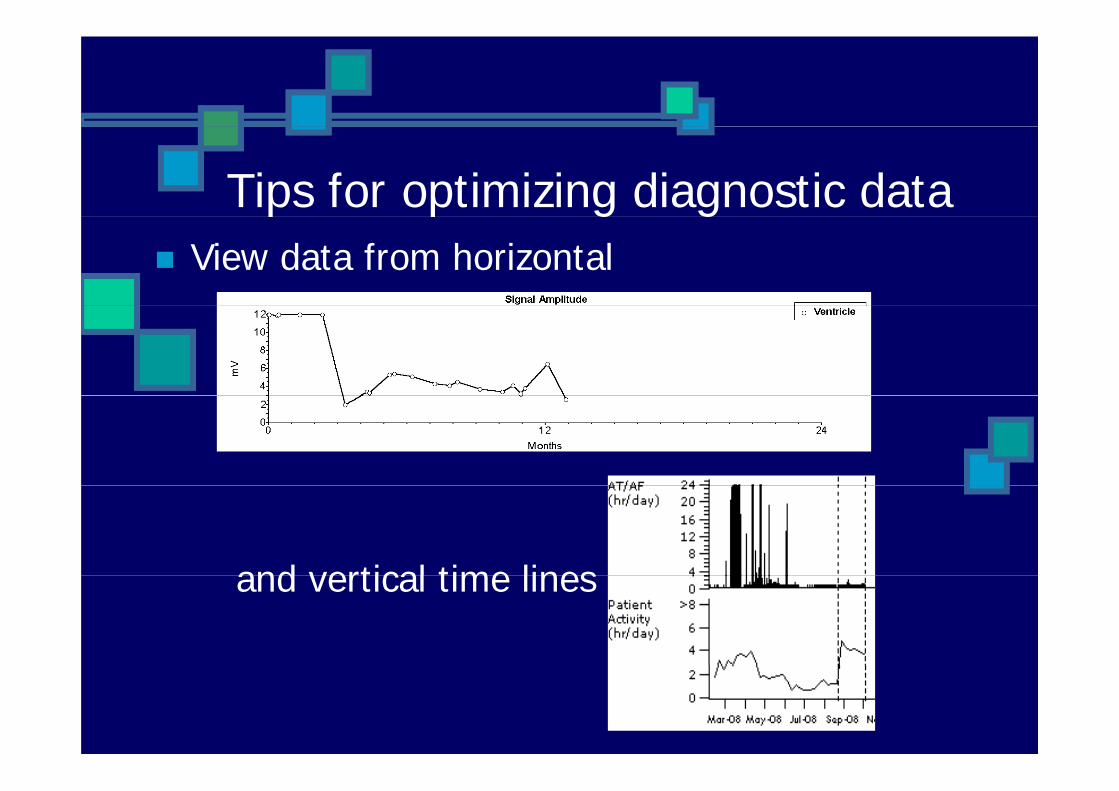
Tips for optimizing diagnostic datap p g gView data from horizontal
and vertical time linesand vertical time lines
Tips for optimizing diagnostic dataTips for optimizing diagnostic data
Do not obsess over irrelevant details during routine follow-up
“One cannot manage too many affairs:One cannot manage too many affairs: like pumpkins in the water, one pops up while you try to hold down the other “while you try to hold down the other
Chi P bChinese Proverb
Make the most of it !Organize and archive patient data in electronic data storageelectronic data storage
Accessible, confidential
Adjust parameters and automatic alerts parameters tailored to patient’s needs
When troubleshooting, use all data available do manual lead tests obtainavailable, do manual lead tests, obtain patient history then connect the dots
One final pointOne final point
When you don’t understand, seek help f th t (t h i l tfrom the experts (technical support, Electrophysiologist, peers )
“Experience is what you get when you p y g ydidn’t get what you wanted “
Randy Pausch in The Last LectureRandy Pausch in The Last Lecture