CASE PRESENTATIONSHOCK SEPSIS ON COMMUNITY-ACQUIRED
PNEUMONIA
Arranged by:Florence Low (0906550751)
Resource Person:dr. Dita Aditianingsih, Sp,An-KIC
Intensive Care Elective Practice Module Faculty of Medicine,
Universitas IndonesiaMay 2015
Case IllustrationPatients IdentityNama: Mr. RNo. Rekam Medis:
404-01-92Tanggal Lahir: 12 September 1962 (52 tahunJenis Kelamin:
Laki-lakiPekerjaan: Ketua RTPendidikan: SDStatus Perkawinan:
MenikahAgama: IslamAlamat: Kramat JatiTanggal masuk: 14 Mei
2015
AnanmnesisData didapat dari anamnesis dan rekam medis pada
tanggal 18 Mei 2015.
Keluhan UtamaPenurunan kesadaran sejak 7 jam sebelum masuk rumah
sakit.
Riwayat Penyakit SekarangPasien dirujuk ke RSCM dari RS daerah
karena pneurunan kesadaran yang membutuhkan perawatn ICU. 3 hari
SMRS, pasien mengeluhkan sesak yang memburuk. Sesak tidak
dipengaruhi posisi ataupun aktivitas. Mengi disangkal. Terdapat
demam namun suhu tidak diukur. Pasien sebelumnya hanya minum obat
warung untuk mengurangi demam. Satu hari SMRS, pasien tampak
mengantuk dan lemas. Pasien masih dapat diajak berbicara namun
lebih memilih untuk tidur terus. Nafsu makan pasien juga menurun. 7
jam SMRS, sesak bertambah parah, nafas bertambah cepat dan pasien
tidak dapat berbicara. Kesadaran pasien juga menurun dan pasien
tidak menjawab bila dipanggil. Sakit kepala disangkal, mulut
mencong dan kelemahan satu sisi juga disangkal, kejang disangkal.
Pasien lalu dibawa ke RS daerah.2 minggu SMRS, pasien mulai batuk
berdahak, batuk darah disangkal. Pada waktu itu, demam belum
muncul. Pasien tidak berobat dan hanya mengkonsumsi obat warung.
Riwayat batuk lama, keringat pada malam hari, dan penurunan berat
badan disangkal. Psien menyangkal riwayat sakit paru ataupun asma.
Pasien didiagnosis diabetes mellitus type II sejak 2,5 tahun yang
lalu. Pasien tidak rutin berobat. Pasien mengaku bahwa gula darah
rata-rata 300 mg/dL..
Riwayat Penyakit DahuluTerdapat riwayat darah tinggi, stroke dan
penyakit jantung sebelumnya. Pasien tidak memiliki pengobatan
apapun.
Riwayat Penyakit dalam KeluargaRiwayat DM, hypertensi, asma dan
penyakit jantung dalam keluarga disangkal.
Riwayat SosioekonomicPasien sudah menikah, memiliki 4 anak.
Pasien bekerja sebagai ketua RT. Untuk pembiayaan, pasien
menggunakan KJS.
Pemeriksaan Fisik(Dilakukan tanggal 18 Mei 2015)Status
Generalis: tampak sakit beratKesadaran: coma (dalam pengaruh
obat)Tanda Vital Tekanan darah: 182/41 mmHg Nadi: 104x/minute,
Pernapasan: 20x/minute, on ventilator Suhu: 36.7C Berat badan: 60
kgPemeriksaan Kepala: normocephal, tidak ada tanda deformitas Mata:
konjuntiva pucat +/+, sklera ikterik -/-, pupil isokor 3mm, RCL
+/+, RCTL +/+ Hidung: on NGT Mulut: on ETT Leher: tidak teraba
pembesaran KGB, terpasang CVC Dada: simetris statis dinamis
Jantung: S1 S2 normal, murmur -/-, gallop -/- Paru: simetris,
perkusi kiri sama dengan perkusis kanan, vesikuler +/+, terdengar
rhonki basah halus pada kedua lapang paru Abdomen: buncit, kenyal,
tidak teraba massa, bising usus normal Ekstremitas: akral hangat,
CRT< 2, edema pada kedua lengan Kulit: pada region inguinal
bilateral hingga skrotim, tampak lasi plakat multiple diskret
ireguler, batas tegas denga lesi satelit
Pemeriksaan PenunjangPemeriksaan
Laboratorium14/4/1518/5/1518/5/15 (post
HD)19/5/1520/5/1521/5/1522/5/15
Hb (g/dL)7.7510,59,2728,79,928,4811,19.74
Ht (%)25,232,728,730,72433,430.4
Leukosit (/L)9970175002010021300124001220025200
Trombosit (L)4270001980001310001180001020005480071.900
MCV (fL)73,170,070,07273,674,4
MCH (Pg)23,722,622,625,424,423,8
PT12,4 (12,6)11,2 (11,8)11,9 (11,8)13,8 (11,2)13,0 (12,7)14,0
(10,8)
APTT69,9 (35,5)53,2 (32,5)65,2 (34,5)55,7 (36,3)>180
(35,1)
Na (mmol/dL)132135125135130127127
K (mmol/dL)4.55,04,24,33,84,84,4
Cl (mmol/dL)1061061031021009697
Ca7,98,48,389
Mg2,262,042,83,39
Ur (mg/dL)25,281,466,774,992,9117,294
Cr (mg/dL)1,3923,53,13,3473,8634,1043,316
AGD
pH7,2727,0767,2137,1906,864
pCO226,434,928,447,154,493,1
pO2206,5158,4149,5189,3188,4117,6
HCO312,310,311,517,215,917,7
BE-17,5-14,2-9,3-13,5-15,6
SaO295,996,198,997,997,492,5
Albumin (g/dL)2,052,272,16
Keton4
GDS
Prokalsitonin17,93
Laktat0,70,51,51,1
UrinalisisPada urinalisis ditemukan protein +2, keton +1, darah
+1 dan leukosit 1-2
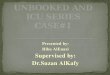
Pemeriksaan Radiologis Chest X-ray (18/5/15) 18/5/15: Tampak
inflitrat di parakardial kanan dan suprhiler kiri, sugestif
gambaran tanda awal bendungan paru 20/5/15: dibandingkan dengan
foto sebelunya, infiltrate di parakardial kanan berkurang
Daftar Masalah1. Penurunan Kesadaran ec sepsis dd metabolik2.
Shock sepsis ec CAP3. Ketoacidosis diabetikum pada DM type II tidak
terkontrol4. AKI dd Acute on CKD
Rencana Diagnosis1. Kultur sputum dan darah2. Tes resistensi and
sensitivitas antibiotic
Rencana Terapi1. Rawat ICU dengan ventilator pemantauan
hemodinamik2. IVFD RF 50cc/jam3. Diet per NGT nutriflex4. Atasi
sepsis dan CAPa. Stabilisasi hemodinamik: norepinephrine 0,1
mcg/kg/min IV, dobutamin 20mcg/kg IVb. Antibiotik: meropenem 3 x
1gr IV dikombinasikan dengan levofloxacin 1 x 750mg IVc.
Anti-fungal fluconazole 1 x 400mg IOd. Pengeluaran mucus: fluimucyl
3 x 1 sach, suction aktif / 4jam dan inhalasi B:V:N / 6jame. Atasi
demam: paracetamol 3 x 500mg5. Anti stress-ulcera. omeprazole 2 x
40mgb. Sucralfat 4 x 1 Corigc. Metoclopramid 3 x 1amp6. Atasi
hiperglikemia: Ringer Insulin 1Unit/jam, GDS per 6 jam7. Sedasi
midazolam 15 mg8. Anuria dengan fluid overload furosemide 20 mg IV,
balans diuresis negatif9. Jaga higienis mulut dan kulit
Follow up 16/5/2015S: perawatan hari ke-1; pasien masuk ICUO: BP
100-120/60-80; MAP 50-89 CVP +17,5 cmH2ORR 12-16x; Pola ventilator
PC 12, PEEP +5, RR 12, FiO2 40%, GDS 109, 85, 162, 325Input: 2221,2
ccOutput 420 cc Rate diuresis 0,29/kgBB/jamBalans/24 jam +1801,2
ccA: Shock sepsis ec CAP, KAD, AKI dd acute on CKDP: RDx: cek PCT,
kultur sputum dan darah, sputum BTA 3xRTh1. Lanjutkan terapi2.
Sedasi morfin 1mg/jam dan midazolam 1mg/jam3. IVFD NS 500cc/24jam4.
MC 30cc/jam5. Nutriflex 1 /24jam6. RI 1 unit/jam7. NE
0,05mcg/kgBB/min
Follow up 17/5/2015S: perawatan hari ke-2; pasien arrest dan
di-RJP, re-intubasi karena mucus plugO: BP 120-140/60-80; MAP
66-103 CVP +15 cmH2ORR 12-16x; Pola ventilator SIMV 14, PC 12, PEEP
+7, RR 16, FiO2 40%, GDS 324, 304, 311, 219, 150, 118Input: 3183,3
ccOutput 781 cc Rate diuresis 0,54cc/kgBB/jamBalans/24 jam +2402,3
ccA: Shock sepsis ec CAP, KAD, AKI dd acute on CKDP: RDx: DPL,
Ur/Cr, P/APTT, AGD, elektrolit, GDSRTh1. MC 50cc/jam2. Nutriflex
1/24jam3. RF 50cc/jam4. RI 1 unit/jam titrasi5. Midazolam 2mg/jam6.
MAP 50 NE dinaikkan darri 0,15mcg ke 0.75mcg7. Arrest bradicardi
36x; BP 36/29 Dilakukan RJP 2 siklus, mendapat SA 6 ampul,
Adrenalin 1 amp NE 1,1 mcg, dobutamin start dosis 5-10mcg
Reintubasi ETT ditemukan sekret kental putih (mucus plug)
Follow up 18/5/2015S: perawatan hari ke-3, pasien HD, ditarik
cairan sebanyak 1500ccO: BP 182/82; MAP 90-124; CVP +22cmH2ORR
16-20x; Pola ventilator PC 14, PEEP +7, RR 16 FiO2 50%, GDS 188,
207, 306, 203Input: 3984,4 ccOutput 2520cc Rate diuresis
0,63/kgBB/jamBalans/24 jam +1464,4ccA: Shock sepsis ec CAP, KAD,
AKI dd acute on CKD, riwayat cardiac arrestP: RDx: cek ulang
PT/APTT, konsul nefrologiRTh:1. lanjutkan terapi2. Peptamen
30cc/jam per NGT3. Nutriflex 1/24jam4. RF 50cc/jam5. RI 1 unit/jam
titrasi6. NE 0,3mcg/kgBB7. Lasix 2mg/jam8. MAP >100 Titrasi
Norepinephrine 0,1mcg
Follow up 19/5/2015S: perawatan hari ke-4, residu makanan keluar
dari NGTO: BP 140-120/80-90; MAP 92-100; CVP +12cmH2ORR 16-20x;
Pola ventilator PC 12, PEEP +7, RR 12, FiO2 50%, GDS 146, 104, 157,
38, 75Input: 2358,6 ccOutput 550cc Rate diuresis
0,38/kgBB/jamBalans/24 jam +1808,6 ccA: Shock sepsis ec CAP, KAD,
AKI dd acute on CKD, riwayat cardiac arrestP: RDx: GDS berkala,
rencana echocardiographyRTh: RI 1U/jam titrasi NE 0,4mcg/kgBB RF
20cc/jam Lasix drip 2mg/jam miloz 1mg/jam GDS menurun, stop RI
pasien dipuasakan GDS menurun, stop RI; pasien dipuasakan
Follow up 20/5/15S: perawatan hari ke-5; GDS menurun, residu
makanan keluar dari NGTO: BP 140-110/80-90; MAP 50-89 CVP +17,5
cmH2ORR 12-16x; Pola ventilator PC 12, PEEP +7, RR 12, FiO2 60%,
GDS 75, 68, 121, 112,Input: 2412 ccOutput 830 cc Rate diuresis
0,26/kgBB/jamBalans/24 jam +1582,2 ccBalans kumulatif +9058,7A:
Shock sepsis ec CAP, KAD, AKI dd acute on CKD, riwayat cardiac
arrestP: RDx: cek PCT, konsul radiologi untuk USG abdomenRTh: GDS
menurun stop RI, bolus D40%, cek GDS berkala Peptamen stop, ganti
CF 30cc/jam, konsul IPD Rencana HD Koreksi albumin untuk persiapan
HD Hb 8,48 Transfusi PRC 1 bag Ganti ETT MAP 50 dosis NE 0,8mcg,
dobutamin 15mcg Rencana HD menjadi CVVH karena hemodinamik tidak
stabil start epinephrine 0,1 mcg
Follow up 21/5/15S: Perawatan hari ke-6, pasien mulai CVVHO: BP
96-105/58-66; MAP 50-70; CVP +12cmH2ORR 16-20x; Pola ventilator PC
12, PEEP +7, RR 15, FiO2 60%, Input: 2579,4 ccOutput 400cc Rate
diuresis 0,27/kgBB/jamBalans/24 jam +2179,4 ccA: Shock sepsis ec
CAP, KAD, AKI dd acute on CKD, riwayat cardiac arrestP: RDx:
rencana USG abdomenRTh: MAP 70 titrasi epinephrine hingga 0,5mcg,
bila tercapai mulai titrasi NE
Literature ReviewCommunity-Acquired PneumoniaPneumonia is
defined as infection of lung parenchyma. Clasically, pneumonia can
be classified to 3 type: community-acquired (CAP),
hospital-acquired (HAP), and ventilator-associated (VAP). Each
types have different pathogens causing the infection. Streptococcus
pneumonia, Mycoplasma pneumonia, Haemophilus pneumonia are the most
common typical bacteria associated with CAP. Less common typical
bacteria include Staphylococcus aureus and Pseudomonas aeruginosa.
Pneumonia results from combination of pathogens activity at alveoli
and hosts response to these activities. Normally, when pathogens
are inhaled, mechanical factors of respiratory system will act to
capture the particles. Then mucociliary clearance and local
antibacterial factor will response to either clear or kill the
pathogens. If the pathogens managed to reach the alveolar level,
local alveolar macrophages then act to eliminate it. However, if
macrophages are overwhelmed by thse pathogens, colonization of
pathogens occurs. Inflammation response are triggered causing
release of inflammatory mediators causing the clinical
manifestation of pneumonia. Interleukin (IL)-1 and tumour necrosis
factors (TNF) wresults in fever while chemokines stimulates the
release of neutrophils, resulting in increase of leukocytes and
production of purulent and mucus. These mediators also caused
capillary leakage which can be seen in radiographic examination as
infiltrate and rales which are detectable on auscultation. The
leakage will cause alveolar filling which in turn caused hypoxemia.
All this contributes to dyspnoea. Clinical manifestations of CAP
are fever with tachycardia, productive or non-productive cough, and
shortness of breath. Pleuritic chest pain and haemoptysis may also
occurs. In cases of atypical pneumonia, low-grade fever and
non-productive cough may be seen. American Thoracic Society (ATS)
recommend laboratory testing such as sputum and blood culture to
identify the aetiology accompanied by chest radiographic to
appropriately diagnose pneumonia. Initial assessment of severity is
important in determining whether patient can be managed as
outpatients or in the hospital. British Thoracic Society (BTS)
recommends the CURB-65 score for this assessment while ATS used
Pneumonia Severity Index (PSI) to assess the severity of CAP. Below
are the scoring system of CURB-65 and PSI.
The decision of ICU treatment for CAP patients is performed on
second-level admission. Based on ATS guidelines, patients with
septic shock requiring vasopressor or those with acute respiratory
failure requiring intubation and mechanical ventilation fulfilled
the criteria for ICU. Patients with severe CAP are also recommended
for ICU admission.
Determining the severity of CAP is also important for the
antibiotic selection. Empirical antibiotic therapies are given
before responsible pathogens are identified by culture. For
inpatient in non-ICU settings, respiratory fluroquinolone are
-lactam plus macrolide can be used for hospitalized patients
without complication. In ICU settings, antibiotic of choice are
-lactam (cefotaxime, ceftriazone, ampicillin-sulbactam) plus either
azithromycin or fluoroquinolone. In the suspicion of pseudomonas
infection, anti-pseudomonas -lactam such as carbapenem plus
fluoroquinolones can be given. As soon as specific pathogen
responsible for CAP are identified, therapy should be switch to
antimicrobial therapy directly targeted for the specific
pathogens.
Sepsis and Septic ShockSepsis is defined as systemic
inflammation in response to infection. The diagnosis of sepsis can
be established when systemic inflammation response syndrome (SIRS)
are documented along with the presence of infection. Severe sepsis
occurs when one or more signs of organ dysfunction is found. Organ
dysfunction occurs due to lack of tissue perfusion induced by
sepsis. When sepsis-indeuced hypotension cannot be manage despite
adequate fluid resuscitation, septic shock occurs.Inflammation
ConditionCriteria
Systemic Inflammation Response Syndrome (SIRS)1. Fever more than
38.3oC or hyperthermia 90x/min)3. Tachypnoea (RR> 24x/min)4.
Leukocytosis >12000/L, leukopenia 1mmol/L)2. Oliguria (output
< 0.5ml/kgBW/h)3. ALI with hypoxemia (PaO2< 300)4.
Creatinine> 2mg/dL5. Bilirubin >2mg/dL6. Thrombocytopenia
1.5)
In patient with severe sepsis, initial resuscitation is
important in preventing further organ dysfunction. The target for
resuscitation includes CVP 8-12mmHg, MAP >65mmHg, urine output
>0.5mL/kgBW/h, central venous or mixed vein oxygen saturation
70% or 65% respectively and normalized lactate. Further management
should be identification of microbes by culture along with initial
empirical anti-infective therapy. Anti-microbes recommended in
cases of respiratory failure and septic shock is combination of
broad-spectrum beta-lactam and aminoglycoside or
fluoroquinolone.
Diabetic KetoacidosisDiabetic ketoacidosis (DKA) is an acute
complication of diabetes mellitus (DM). Although it is usually
found in DM type I patients, it can also be seen several DM type II
patients. Clinical manifestation of DKA includes nausea-vomiting,
thirst, decrease of consciousness, Kussmaul breathing, abdominal
tenderness, lethargy, tachycardia and signs of dehydration. DKA is
usually precipitated by certain condition in the patient such acute
myocardial infarction, stroke or acute infection. Laboratory
findings of DKA includes hyperglycemia with blood glucose of
>250mg/dL, metabolic acidosis and ketosis in the form of
ketonemia or ketonuria. Pathophysiology of DKA can be seen from
hormonal onbalance betwenn regulatory hormones of blood glucose.
Deficit in insulin hormone, coupled with excess in its
counterregulatory hormones such as glucagon cause increase in
gluconeogenesis, glycogenolysis causing increase in glucose
synthesis. Reduced insulin level and elevation of catecholamine
promoted release of free fatty acids from adypocutes, which is
metabolized in the liver, forming ketone body due to
hyperglucagonemia, causing ketosis.In the management of DKA,
monitoring of electrolytes, acid-base status and renal functions
are important. Fluid therapy at the first 6 hours of hospital
admission is important along with management of hyperglycemia with
insulin. Based on guidelines by Indonesian Society of Endocrinology
(PERKENI), 2-3 L of NaCl 0.9% must be given in the first 3 hours,
then on the second hour, insulin must be administered with dosage
of 280mU/kgBW bolus, continued with drip of dosage 90mU/kgBW/hours
in NaCl0.9%. Dosage can be lowered based on the level of blood
glucose. Correction of potassium and bicarbonate can be given of
necessary. Since potassium stores are depleted in DKA, hypokalemia
commonly occurred. 50 mEq/6 hours can be given then after
administration, addition of potassium can be added if hypokalemia
still occurring. Vital signs and blood glucose level must be
monitored every hour while blood gas analysis and electrolyte level
can be measured every 6 hours until patient is stable. Acute Kidney
InjuryBased on Kidney Disease Inmproving Global Outcome (KDIGO)
guidelines, acute kidney injury (AKI) is defined as increase in
serum creatinine of more than 0.3 mg/dL within 48 hours or increase
of more than 1.5x baseline or decrease urine output of less than
0.5 ml/kg/hour for 6 hours. Based on serum creatinine level and
urine output, AKI can be divided to 3 stages. Other criteria which
can be used is the RIFLE, stages includes risk, injury, failure,
loss, and end-stage renal disease (ESRD). These stages determined
types of treatment AKI patients should receive. Determination of
cause of AKI is important to prevent worsening of condition,
decrease kidney perfusion, glomerulonephritis, urinary tract
obstruction are among the common cause of AKI. Among the cause,
persistent hypotension in patient with shock who are not responsive
towards fluid resuscitation increase the risk of development of
AKI. Vassopressor are recommended in septic shock patients for
prevention and even treatment of patient with AKI.. Noreponephrine,
dopamine and vasopressin are the drugs of choice used. Vasopressin
are quite effective increasing blood pressure and enhance diuresis.
Diuretics are not recommended in the management of AKI except
volume overload is present in the patient. DiscussionSince patient
was admitted to ICU, the antibiotics of choices are -lactam plus
fluoroquinolone or azithromycin. However, patient has history of
hospitalization for 2 days prior to this admission. P. aeruginosa
infection should be considered in this patient. Hence,
anti-pseudomonas is considered in this patient. Therapy given in
this patient, which is levofloxacin and meropenem is appropriate
for the settings. Anti-fungal such as fluconazole can be considered
in patient suspected with Candida sp. infection. Length of
treatment should be 3-5 days and can be extended to 7-10 days in
patient with slow clinical response. Procalcitonin can be use as
biomarkers for the effectivity of empiric antibiotics.In case of
life-threatening hypotension, vasopressor therapy should be
initialized with target MAP of 65mmHg. The drug of choice used is
norepinephrine. Norepinephrine was used to increase atrial blood
pressure, increase myocardial contractility and cardiac output. It
was given in continuous infusion in the range of 1-20 g/min.
Vasopressin can be added to norepinephrine to increase the target
MAP while epinephrine can be used as potential substitute for
norepinephrine or as addition to increase cardiac output rather
than to increase MAP.Managemeent of AKI in patient with fluid
overload and increasing creatinine level is according to the RIFLE
criteria. In this patient, the creatinine level is already above
4mg/dL with decrease urine output less than 0.3cc/kgBW/hour. Based
on this criteria, patient is already classified in AKI stage 3 or
RIFLE criteria of failure. Moreover, patient also had acid-base
imbalance from the DKA condition with unstable haemodynamic
condition. hence patient is indicated for hemodialysis therapy. On
the day-7, patient has low pH with a high PCO2 and near normal
HCO3. This shown that patient develop respiratory acidosis due to
poor oxygenation despite breathing on ventilator. The ventilator
mode in this patient was pressure control with PEEP. Patient was
shown to be struggling a bit with the ventilator and still have
several spontaneous breathing. Pressure-control is still
appropriate in this patient since he showed a poor lung compliance,
hence PC mode can reduce the risk of barotrauma on this patient.
SIMV can also be applied since patient sometimes still has
spontaneous breathing and SIMV mode can make sure that ventilation
given does not collide with patients own breathing. It can be given
with lower tidal volume might be more appropriate since in ensures
patient to have minimum ventilation but still protect the lung from
further injury due to mechanical ventilation.
References1. Dellinger RP et al. Surviving sepsis campaign:
international guidelines for management of severe sepsis and septic
shock 2012. Crit Care Med 2013;41:580-637. 2. Mandell LA, Wunderink
RG, Anzueto A, et al. Infectious diseases society of America/
American thoracic society consensus guidelines on the management of
community-acquired pneumonia in adults. Clinical Infectious
Diseases. 2007; 44:S2772.3. KDIGO. KDIGO Clinical practice
guidelines for acute kidney injury. KDIGO Kidney International
Supplements. 2012;2:1; doi:10.1038/kisup.2012.24. Miller RD, Pardo
MC. Basics of anesthesia. 6th edition. Philadelphia (PA): Elsevier
Saunders; 2011.5. Longo DL, Kasper DL, Fauci AS, et al. Harrisons
principle of internal medicine. 18th edition. New York (NY):
McGraw-Hill; 2012. 6. PERKENI. Petunkuk praktis pengelolaan
diabetes mellitus tipe II. Jakarta: PB PERKENI; 2002.