Embed Size (px)
Citation preview
EXPERIENCES OF INSTITUTIONAL RACISMIN THE HEALTH SECTOR:
PRELIMINARY FINDINGS FROM A MEMBER SURVEY BY THE NATIONAL
CONGRESS OF AUSTRALIA’SFIRST PEOPLES
SCOTT AVERY
AIATSIS NATIONAL INDIGENOUS STUDIES CONFERENCE
MARCH 2014
“I'd been walking and went running across the road and slipped and fell arse-over-head. When I went in there to have the x-rays and I told her what happened…She turned around and said to me, you weren't charged up were you? I just thought, well that's the last thing I expected to come out of your mouth.
Next time I see her, I'm going to sit her down and say, hey, just because I'm an Aboriginal person, doesn't mean I'm charged up. You're making them assumptions and generalisations you know. I thought it was disgusting coming from a health professional”
(Respondent to the Member Survey).
RACISM IS A DETERMINANT OF HEALTH AND WELLBEING
The prevalence of racism and its adverse impact on health and wellbeing is well documented (eg. Larson et al, 2007; Priest et al, 2012).
The ‘Experiences of Racism Survey’ in Victoria 2011-2012, funded by the Lowitja Institute, showed a relationship between mental health and reported episodes of racism (Ferdinand et al, 2013).
Critical race theory (eg. Moreton-Robinson) and critical discourse analysis (eg. Hardy, 1999; Phillips and Hardy, 2002) provide theoretical bases for understanding the perpetuation of racism through institutional practices.
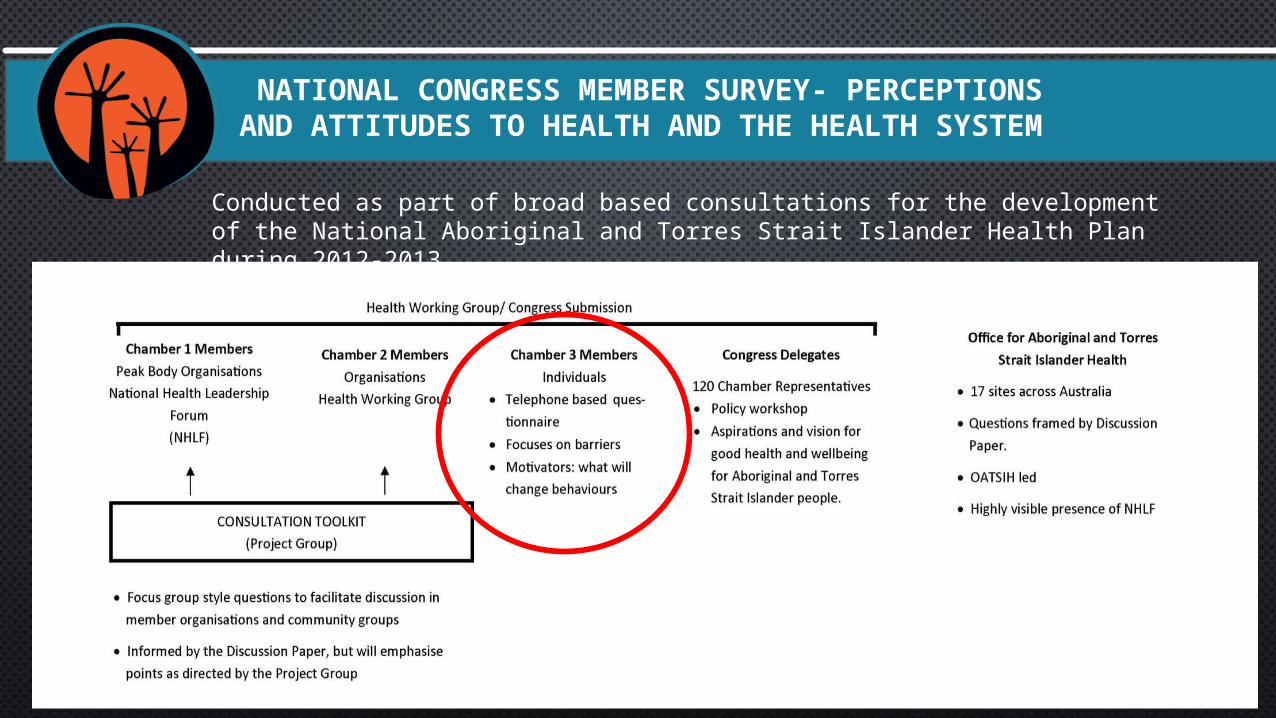
NATIONAL CONGRESS MEMBER SURVEY- PERCEPTIONS AND ATTITUDES TO HEALTH AND THE HEALTH SYSTEM
Conducted as part of broad based consultations for the development of the National Aboriginal and Torres Strait Islander Health Plan during 2012-2013.

“I had my second child at another hospital... He was above birth weight, a healthy baby. The baby had no problems attaching, breast feeding, weight, everything. I've got no issues whatsoever, I'm in a stable marriage, got a previous healthy child. I know how to look after my child
I'm ready to go home - as I'm leaving with my bag she said, “what nationality are you?” I said, “I'm Aboriginal” and she went, oh. She goes, “oh, we're allowed to keep you in here”. I said, “for what reason?” She goes, “because you're at risk”.
How am I at risk? How's my child at risk; please do tell me. Without knowing my race, everything's fine, and all of a sudden..."
(Respondent to Member Health Survey)
METHOD
Siggins Miller were commissioned to conduct a 47 question telephone-based survey over a three week period October-November 2012.
Part quantitative, part qualitative, covering topics including:- Self reported perceptions of health and wellbeing;- Barriers and motivators for health behaviour change;- Access to services and health information;- Racism and other forms of discrimination and its impacts;
and- Culture and traditional healing.
169 respondents drawn from a sample of 559 Members which was a stratified random sample by states/territories, age and gender (response rate 30.2%).

METHOD
Semi-structured interview:
- Have you experienced discrimination?- If so what type?- Where did this happen?- Explain in your own words what happened?- Did you complain about it? If so, how was this resolved?- What impact has your experience had on the likelihood of you
using health or wellbeing services in the future?- What needs to change for you to use healthcare or wellbeing
services more regularly?
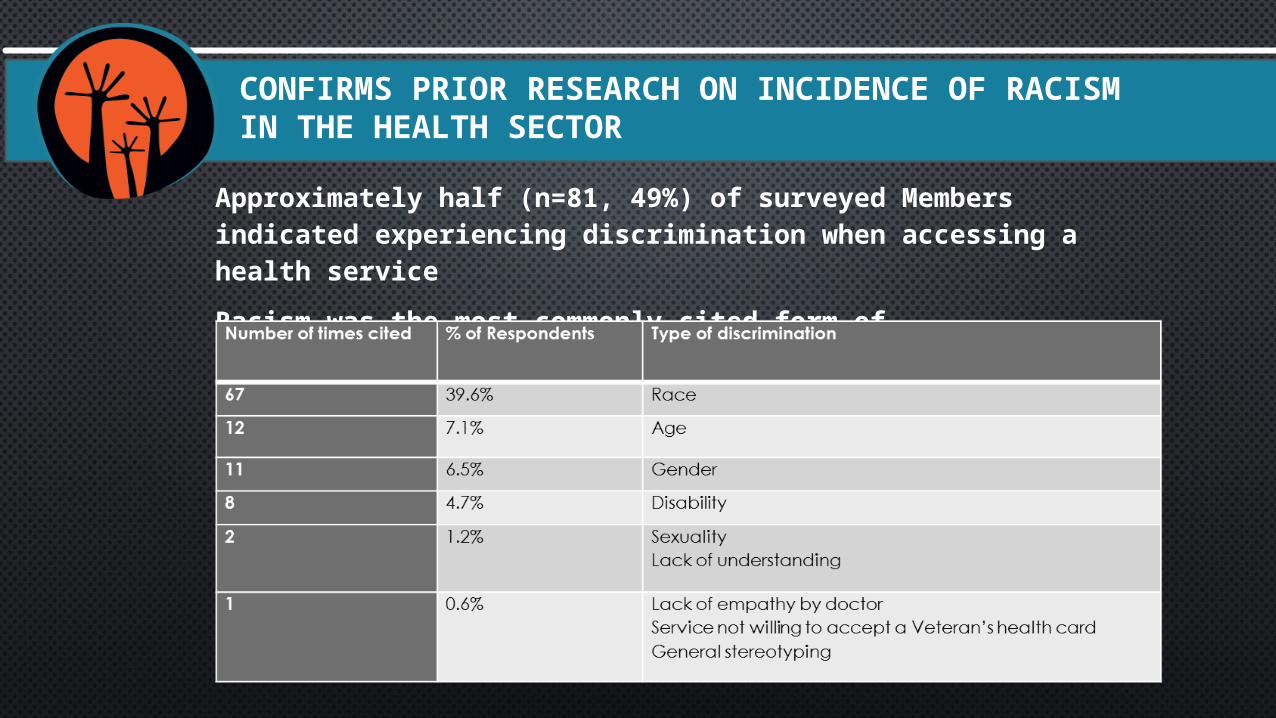
CONFIRMS PRIOR RESEARCH ON INCIDENCE OF RACISM IN THE HEALTH SECTOR
Approximately half (n=81, 49%) of surveyed Members indicated experiencing discrimination when accessing a health service
Racism was the most commonly cited form of discrimination

“She asked what nationality [my children] were and I said Aboriginal…I said their father's from Northern Territory and I'm from Tasmania. She said - she made reference to them not being what she determined a real Aboriginal person.
So to me she was saying well they're not black enough to be real Aboriginal kids.”
(Respondent to Member Health Survey)
RACISM PRESENTED ITSELF IN MANY FORMS
Racially based stereo-typing.
Prejudicial assumptions of health risk and status based on race, rather than the presenting clinical factors.
Challenging a person’s Aboriginality on the basis of skin-colour:
THE KEY FINDINGS
1. There is still a high and unacceptable prevalence of racism in Aboriginal and Torres Strait Islander peoples’ interactions with the health system.
2. Institutional forms of racism (including well-intentioned or paternalistic clinical pathways) compromises the quality of care provided to the individual, undermining their trust in the health system and acting as a barrier to people seeking health care at the time when they need it.
3. Inappropriate and unnecessary care undermines the performance of the health system as a whole, diverting resources away from clinical need.
POLICY OUTCOMES
Narrative evidence on the experiences of racism by Aboriginal and Torres Strait Islander people provided an important educative role on its impact at the national health policy level.
This shifted discourse from defensive and avoidance (“non-discrimination”) to constructive and direct (“free from racism”).
Vision for the National Aboriginal Torres Strait Islander Health Plan:
“ The Australian health system is free of racism and inequity and all Aboriginal and Torres Strait Islander peoples have access to health services that are effective, high quality and affordable…: (p.7)

WHERE TO NEXT? POSSIBLE DIRECTIONS FOR RESEARCH, POLICY AND PRACTICE
Shift the focus to de-instutionalising racism:
- This is more than just talking about cultural competency – its about system competency.
- Gaps in the governance frameworks of health systems (ie. how decisions are made)
- The curricula of health and medical training institutions (ie. what health care providers are taught).
The voices of Aboriginal and Torres Strait Islander people are the means to address the semiotic void between their experiences of health care and an under-performing health system.

GENERAL EMAIL: [email protected]
MEMBERSHIP: [email protected]
PH (02) 8070 3100
NATIONAL CONGRESS OF AUSTRALIA’S FIRST PEOPLES