Embed Size (px)
Citation preview

Identification of Autism Spectrum Disorder in Young
ChildrenNancy Roizen, MD
Director, Division of Developmental/Behavioral Pediatrics and Psychology
Rainbow Child Development CenterProfessor of Pediatrics
Case Western Reserve University

Ages and areas of concern, consultations 1,2,3
Screening: false+ and false _
DSM criteria in < 3 year olds
Retrospective (1st yr videos) and prospective studies (Ausibs)
ADOS changes
EI data and recommendations
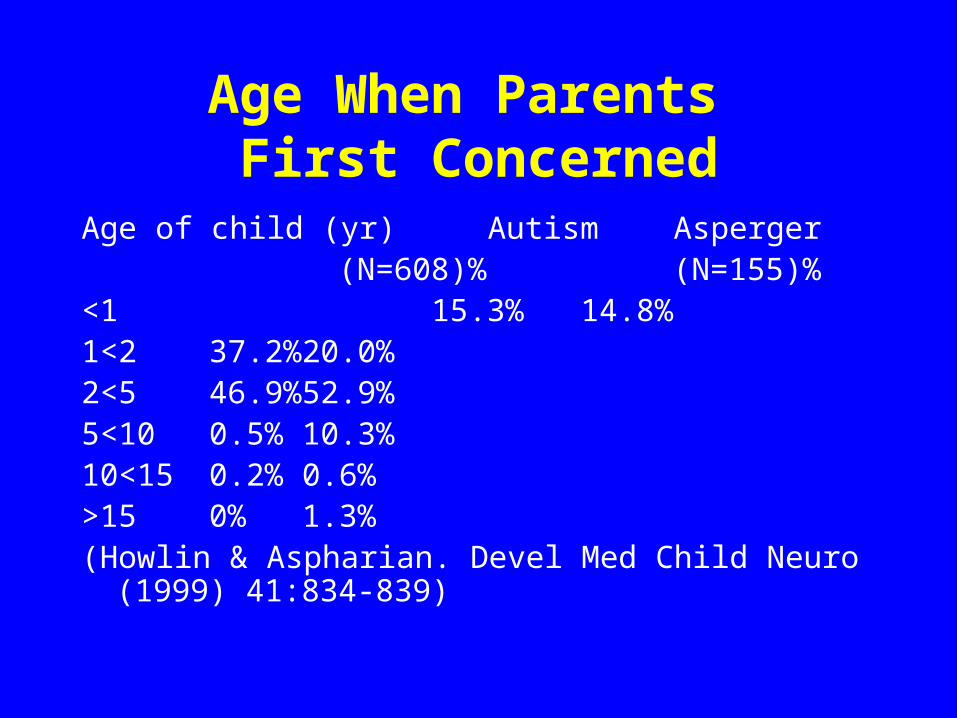
Age When Parents First Concerned
Age of child (yr) Autism Asperger (N=608)%
(N=155)%<1 15.3% 14.8%1<2 37.2% 20.0%2<5 46.9% 52.9%5<10 0.5% 10.3%10<15 0.2% 0.6%>15 0% 1.3%(Howlin & Aspharian. Devel Med Child Neuro (1999) 41:834-
839)
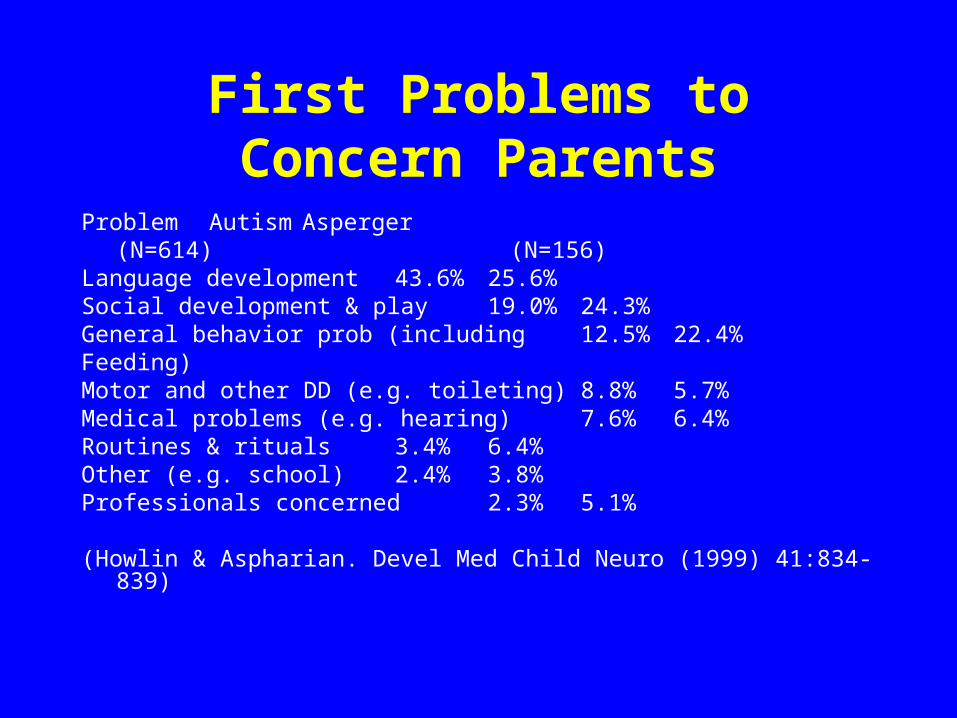
First Problems to Concern Parents
Problem Autism Asperger(N=614) (N=156)
Language development 43.6% 25.6%Social development & play 19.0% 24.3%General behavior prob (including 12.5% 22.4%Feeding)Motor and other DD (e.g. toileting) 8.8% 5.7%Medical problems (e.g. hearing) 7.6% 6.4%Routines & rituals 3.4% 6.4%Other (e.g. school) 2.4% 3.8%Professionals concerned 2.3% 5.1%
(Howlin & Aspharian. Devel Med Child Neuro (1999) 41:834-839)
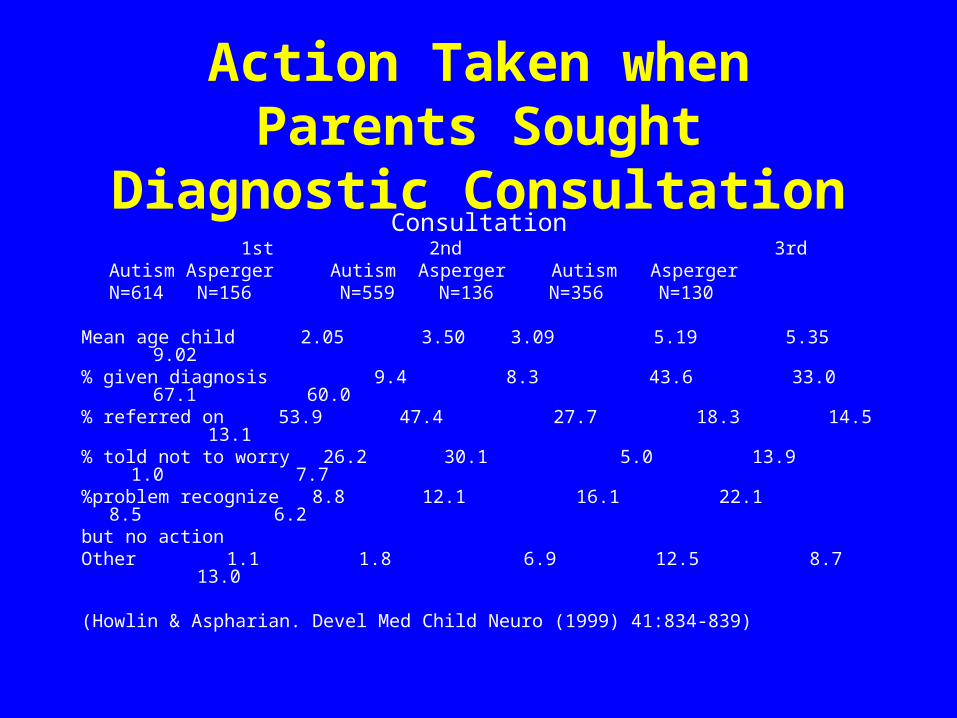
Action Taken when Parents Sought Diagnostic Consultation
Consultation 1st 2nd 3rd
Autism Asperger Autism Asperger Autism AspergerN=614 N=156 N=559 N=136 N=356 N=130
Mean age child 2.05 3.50 3.09 5.19 5.35 9.02% given diagnosis 9.4 8.3 43.6 33.0 67.1 60.0% referred on 53.9 47.4 27.7 18.3 14.5 13.1% told not to worry 26.2 30.1 5.0 13.9 1.0 7.7%problem recognize 8.8 12.1 16.1 22.1 8.5 6.2but no actionOther 1.1 1.8 6.9 12.5 8.7 13.0
(Howlin & Aspharian. Devel Med Child Neuro (1999) 41:834-839)
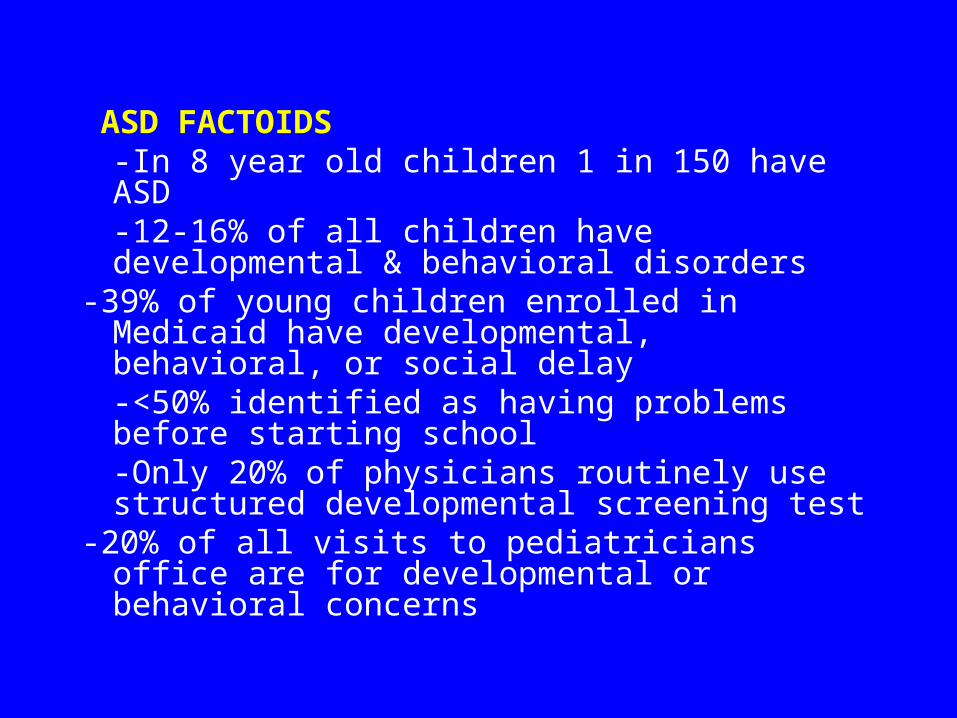
ASD FACTOIDS-In 8 year old children 1 in 150 have ASD-12-16% of all children have developmental & behavioral disorders
-39% of young children enrolled in Medicaid have developmental, behavioral, or social delay-<50% identified as having problems before starting school-Only 20% of physicians routinely use structured developmental screening test
-20% of all visits to pediatricians office are for developmental or behavioral concerns
Suzie is four years old and referred by her pediatrician for language delays and concerns about her lack of eye contact and possible autism. In the last 2 years she has been evaluated by a pediatric neurologist and another developmental pediatrician. By history, she says nothing when she is outside her home.

The differential diagnosis of a child with language delay:
Intellectual disability
Autism spectrum disorder
Selective mutism
Mental retardation
Expressive language delay
Environmental deprivation
Verbal dyspraxia/apraxia
The parents report that she speaks with her siblings and somewhat less so with her parents at home. With much cajoling and a slow moving presentation of questions with assistance from the parents, she answered several but not all questions at age level. Questionnaires indicated anxiety
A diagnosis of selective mutism is made because she does she speaks only in specific situations and by history and observation exhibits significant anxiety. She is referred to Dr. Cunningham our clinical psychologist who has a special interest in anxiety. Dr. Cunningham begins counseling and suggests that medication be added to the treatment regimen as progress is going slowly with counseling.
What will happen with our child? She is young. Hopefully, through counseling and medication, she will get on a better trajectory. She needs to be more confident and comfortable to speak at school and other out-of-home situations. She might have problems with repeated issues of anxiety. Dr. Cunningham might be working with her intermittently for years.
Emphasis on Early Diagnosis
-Mounting evidence that developmental disruption is present before 3 yrs of age in children subsequently diagnosed with ASD
-Research on neuroplasticity and intervention for ASDs indicates that early intervention is likely to optimize the outcome for children with ASDs
-Intervention may minimize or possibly prevent some handicapping symptoms such as sequelae of self-imposed social deprivation.
Important and Exciting Happenings in the Nation, State, and County
Studies on Early Identification
Studies on Improving Sensitivity and Specificity
Funds to Increase the Screening, Identification, and Intervention for ASD
Nationally : Combating Autism Act is infusing monies into LEND, MCHB D-B Fellows Developmental-Behavioral FellowshipsState of Ohio: AAP John Duby, MD Autism Education Pilot ProjectRainbow Child Development CenterRainbow: Pediatric Neurology, Developmental-Behavioral Peds, Child PsychiatryUMAC (University of Michigan Autism Center)Autism Treatment Network
SCREENING CHAT screening twice (if positive) of 16,235 infants at 18
months of age-12 failed all key items measuring proto-declarative pointing,
gaze monitoring, and pretend play-At 7 yr of age: 9 autism, 1 PDD, 1 language disorder, and 1
normal-22 children were medium risk as missed proto-declarative
pointing-At 7 yr of age: 1 autism, 9 PDD, 7 language disorders, 2
developmental delay, 1 CP, 1 nl-50 cases with autism in screening population only 10
identified as medium or high risk.-44 with PDD only 10 in medium or high risk group
(Baird et al., J Am Acad Child Adoles Psychiatry. (2000)39:694-702.)
PROBLEMS: FALSE POSITIVES AND NEGATIVES

DSM-IV Diagnostic Criteria for Autistic Disorder
A. A total of six (or more) items from (1), (2), and (3), with at least two from (1) and one each from (2) and (3):
(1) qualitative impairment in social interaction, as manifested by at least two of the following:
(a) marked impairment in the use of multiple non-verbal behaviors, such as, eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction
(b) failure to develop peer relationships appropriate to developmental level
(c) a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest)
(d) lack of social or emotional reciprocity
DSM-IV Diagnostic Criteria for Autistic Disorder (cont)
(2) qualitative impairments in communication as manifested by at least one of the following:
(a) delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication, such as, gesture or mime)
(b) in individuals with adequate speech, marked impairment in the ability to initiate of sustain a conversation with others
(c) stereotyped and repetitive use of language or idiosyncratic language
(d) lack of varied, spontaneous, make-believe play or social imitative play appropriate to developmental level
DSM-IV Diagnostic Criteria for Autistic Disorder (cont)
(3) restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
(a) encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
(b) apparently inflexible adherence to specific, nonfunctional routines or rituals
(c) stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements)
(d) persistent preoccupation with parts of objects
DSM-IV Diagnostic Criteria for Autistic Disorder (cont)
B. Delays or abnormal functioning in at least one of the following areas, with onset prior to age 3 years:
(1) social interaction (2) language as used in social communication (3) symbolic or imaginative play
C. The disturbance is not better accounted for by Rett’s Disorder or Childhood Disintegrative Disorder
Autism Spectrum Disorder (ASD)=autistic disorder , Asperger disorder, and pervasive developmental disorder-not otherwise specified
Children Younger Than 3 Years of Age: Apply 4 of DSM-IV Criteria
-Lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. by lack of showing, bringing, or pointing out objects of interest)
-Lack of social and emotional reciprocity-Marked impairment in the use of multiple nonverbal
behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction
-Delay in or total lack of the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime)
(Stone et al. J Child Psychol Psychiatry. (1999) 40:219-226)
EARLY SOCIAL SKILL DEFICITS
Typical: Social development usually parallels overall general function (motor+adaptive+language+cognitive domains) in typically developing children and in those with developmental delays
ASD: social skills and language more delayed or “out of sync” with motor, adaptive, and cognitive function
(Johnson. Pediatrics in Review (2008) 29:86-96)
JOINT ATTENTION (JA): lack or delay specific to autism
Definition: normal, spontaneously developing behavior that demonstrates child’s joy in sharing an object or event with another personSpontaneous: child looks back and forth between interesting object and caregiver to share interest Responding: child looks in direction indicated by the pointing of a caregiver and connects. Typically at 10-12 months
Initiating: child points to object to establish a connection with another person. Typically at 14-16 months.Show: “show” or bring an object to parent as if to say, “Look at this.” Typically at 14 to 16 months
SOCIAL ORIENTING: ability to orient to verbal stimuli specifically one’s own name
Typically at 8-10 months consistently turn toward the speaker when their name is called.
ASD: fail to orient to name but may respond to environmental sounds

PRETEND (SYMBOLIC) PLAY: using pretend actions with objectsTypically, simple pretend play at 16-18 months with use of miniature representative items talk on phone, feed doll. ASD: often have little interest in toys, frequently preferring everyday items such as string, sticks, books or videos for carrying. May be content to play alone for hours. Play usually sensory-motor, ritualistic or constructive. May enjoy “roughhouse play” and show fleeting moment of social relatedness.
PRELANGUAGE ABNORMALITIES
Typical: cooing or babbling by 6 months. Inflection by 10-12 months
ASD: quiet and make few vocalizations. Atypical vocalization with hum or grunt. May be irritable and cry for long periods of time. May not wave bye or extend arms to be picked up. Do not have back and forth babbling conversations. Do not add inflection at 10-12 months.
ABSENT OR DELAYED SPEECH
Differential diagnosis:Hearing lossGlobal developmental delays due to intellectual disabilityLack of stimulating environmentExpressive language delayDyspraxiaSelective mutismAutism
LANGUAGE REGRESSION: 25% to 30% with ASD appear to develop normally and
regress
ASD: regression usually between 15 to 24 months most frequently 18 to 21 months
Differential diagnosis of loss of language skills:Rett syndromeNeurodegenerative disordersLandau-Kleffner syndrome with seizures is usually>3 yr.
ATYPICAL LANGUAGE
-false impression of “advanced speech” but is echolalic, ritualistic, and not functional-immediate in ASD and typical but delayed in ASD and can be pervasive, enduring, and larger chunks of verbal material-ASD: obsessed with labeling colors, shapes, and numbers but unable to use in conversation-recite jungles and ABCs but unable to ask for a drink or follow a command-can have giant words (e.g. Whatisit?) and “pop-up” words that seem out of context and to have no communicative intent and then disappear.
RESTRICTIVE INTERESTS, STEREOTYPIES, AND REPETITIVE
BEHAVIORS
-Typical, form attachments to stuffed animal but ASD prefers hard items like pens or ropes with more robust attachment needing to hold during dinner, etc
-Stereotypies with hand flapping, twirling, finger movements, toe walking, licking, and sniffing.
-Repetitive behavioral such as lining things up and protesting violently when directed to a new activity
Retrospective Studies Involving Home Videos
-Home videos of first birthdays comparing children later diagnosed with ASDs compared to typically developing children and non-ASD-related developmental delays
-Children with ASDs exhibited:Less frequently responding to their nameLess frequently looking at the faces of other individualsLess often using a pointing gesture to request or to share interest
(Landa. Nature Clinical Practice Neurology. (2008) 4:138-147)
Prospective Studies Involving Infant Siblings of Children with ASDs
-Diagnostic Classifications made at 2-3 years of age
-6 months olds later dx with ASD:
WNL visual perception and language
ABN motor w/fine & gross motor delays
Hypotonia
Atypical motor behaviors
(Landa. Nature Clinical Practice Neurology. (2008) 4:138-147).
Development in Infants with ASD in Infant Siblings of Children with ASDs
-87 Infants tested at 6, 14, and 24 months from high risk (sibs) and low risk groups
-6 months: no stat diff between siblings and unaffected group-14 months: ASD group signif worse on all scales except visual
reception-24 months: ASD performed signif worse in all domains and
worse than language delayed group in Gross Motor, Fine Motor, and Receptive Language
-developmental trajectory of ASD group had unusual slowing in performance between 14 and 24 months of age in ASD
(Landa & Garett-Mayer. J Child Psychol and Psychiatry
(2006) 47:629-638)
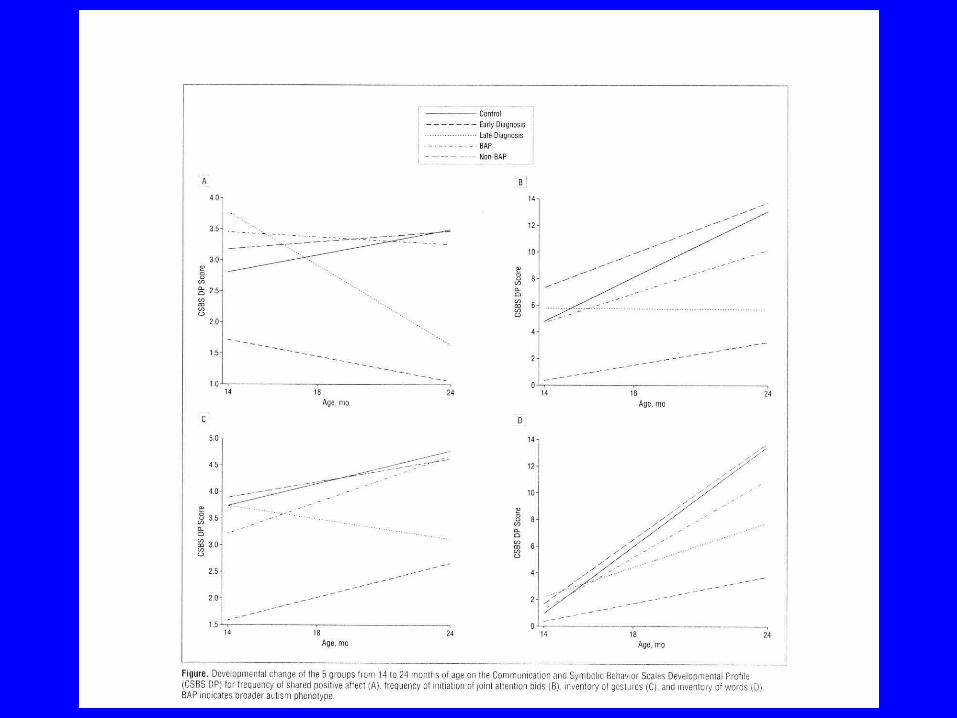
Social & Communication Development in Infant/Toddler Siblings of Children with
ASDs-N=107 AUsibs (59 boys and 48 girls); N=18
low-risk controls-used Communication and Symbolic Behavior
Scales Developmental Profile (CSBS DP), Mullen Scales of Early Learning or Preschool Language Scale, and other measures
-Dx on clinical judgment and ADOS

X-Early Diagnosis Group=diagnosis at 14 month visit (n=16;14 boys and 2 girls )
-Late Diagnosis Group= diagnosis after 14 months visit (n=14; 11 boys and 3 girls)
-expected 5-8% but 26%. Possible sampling bias as parents (44% at 6 mo & 76% at 14 mo) reported concerns
-AUsibs had group (n=19; 13 boys & 6 girls) exhibited language and/or social delays (broader autism phenotype or BAP) but not ASD
(Land et al. Arch Gen Psychiatry. (2007) 64:853-864)
X-Early Diagnosed Group produced less frequent shared positive affect, initiation of behavior regulatory bids, initiation of joint attention bids, and smaller inventory of gestures and consonants
-Early Diagnosed Group sign worse that BAP on all variables (P<.01)
-Late Diagnosed Group at 14 mo differed from non-BAP groups only on fewer gaze shifts
-ASD children tended to show decreases, or arrest or make very slow gains compared with other groups
(Land et al. Arch Gen Psychiatry. (2007) 64:853-864)
Autism Diagnostic Observation Scale (ADOS)
Standardized semi-structured observational play and activity assessment of the child
Module chosen depending on the developmental and language level of the child
Scoring includes cut-offs for autism and autism spectrum disorder (ASD)
Module 1 for children with no speech of single word has several itemsResponse to nameResponse to smileResponse to joint attentionAnticipation of social routineBirthday party and snack
Coded for social interaction and communication domains.
ADOS:Revised algorithm for improved
diagnostic validity
Coded for Social affect and restricted, repetitive behavioral (RRB)
Research demonstrated that repetitive behaviors observed during administration were of diagnostic significance (La Couteru. (2008). J Autism Dev Disord;38:362-372.)
Autism Diagnostic Interview-Revised (ADI-R)
Investigator-based semi-structured diagnostic interview designed to provide a developmental history framework for a lifetime differential diagnosis of Pervasive Developmental Disorders.
Takes 2-3 hours and asks questions about function over the previous 3 months
Scoring based on algorithms relating to social interaction, communication, and repetitive behaviors with scoring cut-off for Autism.
For older children, questions are asked about behavior for the year that the child was 4.
IMPROVING SENSITIVITY AND SPECIFICITY

AUTISM OBSERVATION SCALE FOR INFANTS (AOSI)
Infants 6-18 months; 18-item direct observational measureVisual tracking; Coordination of eye gaze and actionDisengagement of attentionOrientation to name; Eye contact; Reciprocal social smileDifferential response to facial emotionAnticipatory social response; Social interest and shared
affectImitation; Social babblingCuddliness; Soothability Transitions; Motor controlAtypical motor behavior; Atypical sensory behaviorBryson et al. J Autism Dev Disord (2008) 38:731-38.
Early Intervention Preschool-aged Children with ASDs
-positive responses to >20 hours/week -interventions that target wide range of skills-average IQ gain of 20 points with ABA based on
operant conditioning with discrete skills taught by use masses trail conducted outside the natural context
-more-naturalistic applications of ABA (Pivotal Response Training) have been shown effective for teaching important social and communication skills
-similar improvements in developmentally based interventions in which teaching often occurs within the natural context.
-number of hours of speech-language therapy received between 2 and 4 years by children with ASDs is related to their development of spoken language
-National Research Council recommended 25 h/wk of therapy-based engagement which can be delivered by therapists, family members and other caregivers
(Landa. Nature Clinical Practice Neurology. (2008) 4:138-147.)
SUMMARY
Need early identification: screening and diagnosis
Better standardized tools and clinical diagnosis
Increased EI services and data














![Enduring Wellness, L.L.C. v. Roizen · [Cite as Enduring Wellness, L.L.C. v. Roizen, 2020-Ohio-3180.] COURT OF APPEALS OF OHIO EIGHTH APPELLATE DISTRICT COUNTY OF CUYAHOGA ENDURING](https://img.pdfslide.net/doc/110x75/5f235988aea53a366a24058b/enduring-wellness-llc-v-cite-as-enduring-wellness-llc-v-roizen-2020-ohio-3180.jpg)











