Embed Size (px)
Citation preview

Dow
nloadedfrom
https://journals.lww.com
/jtraumaby
BhDMf5ePH
Kav1zEoum1tQ
fN4a+kJLhEZgbsIH
o4XMi0hC
ywCX1AW
nYQp/IlQ
rHD3bhnalqTQ
iPuGRXx5KyPdFfH
/f+s9ooq0341a2oVqA8U=on
03/20/2019
Downloadedfromhttps://journals.lww.com/jtraumabyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3bhnalqTQiPuGRXx5KyPdFfH/f+s9ooq0341a2oVqA8U=on03/20/2019
Identifying patients with time-sensitive injuries: Association of mortality with
increasing prehospital time
Xilin Chen, MPH1
Francis X. Guyette, MD MPH2
Andrew B. Peitzman, MD1
Timothy R. Billiar, MD1
Jason L. Sperry, MD MPH1
Joshua B. Brown, MD MSc1 [email protected]
1 Division of General Surgery and Trauma, Department of Surgery, University of Pittsburgh
Medical Center, Pittsburgh, Pennsylvania 15213
2 Department of Emergency Medicine, University of Pittsburgh Medical Center, Pittsburgh,
Pennsylvania 15213
Correspondence and Reprints
Joshua B. Brown, MD, MSc
Division of General Surgery and Trauma, Department of Surgery
University of Pittsburgh Medical Center
Journal of Trauma and Acute Care Surgery, Publish Ahead of Print DOI: 10.1097/TA.0000000000002251
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

1
200 Lothrop Street, Pittsburgh, PA 15213
Phone: (716) 400-2471
Fax: (412) 647-1448
Email: [email protected]
No funding or support was directly received to perform the current study.
There are no conflicts of interest for the current study
These data were presented as a poster presentation at the 77th
Annual Meeting of the American
Association for the Surgery of Trauma, September 26-29th
, 2018 in San Diego, CA.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

2
Background: Trauma is a time-sensitive disease. However, recognizing which patients have
time-critical injuries in the field is challenging. Many studies failed to identify an association
between increasing prehospital time (PHT) and mortality due to evaluation of heterogenous
trauma patients, as well as inherent survival bias from missed deaths in patients with long PHT.
Our objective was to determine if a subset of existing trauma triage criteria can identify patients
in whom mortality is associated with PHT.
Methods: Trauma patients age ≥16years transported from the scene in the NTDB 2007-2015
were included. Cubic spline analysis used to identify an inflection where mortality increases to
identify a marginal population in which PHT is more likely associated with mortality and
exclude biased patients with long PHT. Logistic regression determined the association between
mortality and PHT, adjusting for demographics, transport mode, vital signs, operative
interventions, and complications. Interaction terms between existing trauma triage criteria and
PHT were tested, with model stratification across triage criteria with a significant interaction to
determine which criteria identify patients that have increased risk of mortality associated with
increasing PHT.
Results: Mortality risk increased in patients with total PHT≤30min, comprising a study
population of 517,863 patients. Median total PHT was 26min (IQR 22-28) with median ISS of 9
(IQR 4-14) and 7.4% mortality. Overall, PHT was not associated with mortality (AOR 0.984 per
5-min increase; 95%CI 0.960—1.009, p=0.20). Interaction analysis demonstrated increased
mortality associated with increasing PHT for patients with SBP<90mmHg (AOR 1.039; 95%CI
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

3
1.003—1.078, p=0.04), GCS≤ 8 (AOR 1.047; 95%CI 1.018—1.076, p<0.01), or non-extremity
firearm injury (AOR 1.049; 95%CI 1.010—1.089, p<0.01).
Conclusions: Patients with prehospital hypotension, GCS≤ 8, and non-extremity firearm injury
have higher mortality with increasing PHT. These patients may have time-sensitive injuries and
benefit from rapid transport to definitive care.
Level of Evidence: III, Prognostic
Key Words: Emergency medical services; Prehospital; Transport; Time; Triage
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

4
BACKGROUND
Trauma is a time-sensitive disease. This has been embodied by the "golden hour"
concept.1 The underlying theory is that minimizing the time from injury to definitive care at a
trauma center improves outcomes. This has led to the "scoop and run" approach to emergency
medical services (EMS) in which rapid transport is favored with few or no prehospital
interventions.2 However, many studies have not identified an association between increasing
prehospital time and mortality, calling into question this tenet of trauma care.3-8
This lack of relationship between prehospital time and outcome may have been seen in
prior studies for two reasons. First is the inherent survival bias in trauma registry data used in
prior studies. Registry data are collected from only patients brought to a participating trauma
center. Thus, patients farther from the trauma center with long prehospital times that survive long
enough to get to the trauma center are likely to survive their injuries. Patients far from the trauma
center who die in the field or at a closer non-trauma center are not captured. Only patients that
survive to arrive at the trauma center are included in registry data and bias the true relationship
between prehospital time and mortality for patients with longer prehospital times. This may
result in paradoxical findings in which longer prehospital time appears to be associated with
lower mortality.
Second, prior studies evaluate a heterogenous population of all trauma patients.
Ultimately, many patients do not have time-sensitive injuries. Absence of any selection criteria
produces a heterogenous population in which prehospital time is unlikely to be associated with
mortality. The key issue becomes recognizing which patients have time critical injuries in the
field. However, this remains challenging, as EMS providers have few resources to identify these
patients and act accordingly. To our knowledge, no prior studies have evaluated whether injured
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

5
patients with time-sensitive injuries could be identified in the field. Triage criteria that identify
time-sensitive trauma patients represent actionable information for EMS providers, allowing
them to prioritize rapid transport with scoop and run or activating helicopter emergency medical
services (HEMS) to minimize prehospital time.
Thus, it was our objective was to determine if a subset of existing field trauma triage
criteria can identify patients in whom mortality is associated with increasing prehospital time
after accounting for potential survival bias.
METHODS
Study Population
All patients ≥16years transported by EMS from the scene in the National Trauma
Databank (NTDB) 2007-2015 were included. Patients with burn injury, missing total prehospital
time, or total prehospital time greater than 3 hours were excluded. Prehospital times longer than
3 hours were excluded as this is >90th
percentile of total prehospital time in the dataset and are
not representative of typical EMS transports across the United States. A subset of these patients
was studied in further detail using the Pennsylvania Trauma Outcomes Study (PTOS) 2007-
2015. The PTOS includes more detailed prehospital data to allow further exploratory analysis of
factors affecting prehospital time. The same inclusion/exclusion criteria and definitions were
applied to the PTOS subset.
Total prehospital time was defined as the time elapsed from dispatch of EMS by the 911-
system to arrival of EMS with the patient at the hospital. This incorporates three intervals of
prehospital time, including response (time from dispatch to arrival at the scene), scene (time
from arrival at the scene to leaving the scene), and transport time (time from leaving the scene to
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

6
hospital arrival). Total prehospital time was chosen as it accounts for the entire prehospital care
period and each time interval component may be modifiable through different strategies.
Missing Data
Multiple imputation was performed to account for the missing values. Imputed variables
included sex, race, insurance status, injury severity score (ISS), admission SBP, and mechanism
of injury. Multiple imputation using chained equations developed five imputed datasets.
Outcome models combined coefficients and standard errors from each imputed dataset while
adjusting for the variability between imputed datasets.9 Missing data for imputed variables
ranged from 0.1% (mechanism, PTOS) to 12.9% (insurance status, NTDB). Sensitivity analysis
with complete cases was performed and similar results were seen, thus results from imputed data
are presented below. Imputation was not used for variables affecting triage criteria (prehospital
Glasgow Coma Scale [GCS], systolic blood pressure [SBP], respiratory rate [RR]). These
variables were not imputed as different values could be imputed for the missing observations in
each of the five imputed datasets. Thus, a patient might have a positive triage criterion in some
but not all imputed datasets for criteria using these variables. This would make it impossible to
analyze a stratified sample based on interaction testing if the criterion was different within the
same patient across imputed datasets. Prehospital GCS, SBP, RR were missing in 5.1%, 7.0%,
and 5.2% of patients respectively.
Survival Bias
Since the databases utilized suffer from the survival bias noted above, we addressed this
by excluding patients with long prehospital times which represent a biased group where only
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED
7
patients surviving long enough to reach a trauma center were captured in the dataset. We sought
the prehospital timeframe where mortality drops off and remains relatively constant to identify
this biased group. To determine the prehospital time threshold to exclude this biased group, we
used restricted cubic spline analysis which evaluates the non-linear relationship between
mortality and prehospital time. This allowed us to empirically select the prehospital time
threshold to exclude patients with longer times based on data rather than using an arbitrary
threshold.
Restricted cubic splines were created for total prehospital time with 3 knots. Logistic
regression was then performed with mortality as the dependent variable and cubic splines as the
independent variables. The adjusted odds ratio (AOR) and 95% confidence interval (95%CI)
were estimated for each minute of total prehospital time relative to 180minutes. The AOR and
95%CI were plotted across prehospital time. This identified a marginal population with a shorter
prehospital timeframe that allowed patients to reach a trauma center regardless of injury severity
and would be less likely to suffer from survival bias. All further analyses were performed only
on patients within this prehospital timeframe.
Statistical Analysis
The primary outcome was in-hospital mortality. Logistic regression was used to
determine the association between in-hospital mortality and total prehospital time. Total
prehospital time was evaluated as a continuous variable. The model was adjusted for age, gender,
race, insurance status, transport mode, mechanism of injury, ISS, prehospital SBP, admission
SBP, need for urgent operation (emergency department disposition of operating room), need for
mechanical ventilation, in-hospital complications, and trauma center level. Models were also
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

8
adjusted for isolated severe (abbreviated injury scale [AIS]≥3) head, chest, or abdominal injury,
as well as combinations of severe head, chest, or abdominal injury to account for differing
anatomic patterns of injury. Interactions between prehospital time and anatomic injury pattern
were tested to determine if prehospital time had a different effect on mortality based on the
anatomic injury pattern. Robust variance estimators were used to account for clustering at the
center level.
Existing triage criteria were evaluated to identify patents with time-sensitive injuries,
including SBP<90mmHg, GCS≤13, GCS≤8, RR<10 or >29bpm, penetrating injury, unstable
chest wall, open skull fracture, ≥2 proximal long bone fractures, pelvic fracture, crush injury,
amputation, paralysis, hemothorax or pneumothorax, multisystem trauma (≥3 body regions
injured), and combination of physiologic plus anatomic triage criteria from the national field
triage guidelines.10
Penetrating injury was further classified as firearm versus non-firearm injury
based on external injury codes (e-codes), and non-extremity (head, face, neck, chest, abdomen,
or spine) versus extremity location of penetrating injury based on AIS body regions. Interaction
terms between these triage criteria and total prehospital time were tested.
A significant interaction indicates prehospital time has a different effect on mortality
based on the presence or absence of the criterion. Models were stratified across triage criteria
with significant interactions. This allowed determination of which criteria, when present, identify
patients with increased risk of mortality associated with increasing prehospital time.
Combinations of positive criteria were also tested. To account for multiple comparisons, false
discovery rate correction was used.11
Continuous data are presented as median (IQR) and compared using Mann-Whitney tests.
Proportions were compared using χ2 tests. A two-tailed p value of ≤0.05 was considered
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

9
significant. Adjusted odds ratios (AOR) with 95%CI were obtained from regression models.
Regression coefficients were transformed to obtain the adjusted odds of mortality per 5-minute
increase in prehospital time. Model performance was assessed using the c-statistic and graphic
calibration. Data were analyzed using Stata v15MP (College Station, TX).
Subgroup Analysis
An exploratory subgroup analysis was conducted based on transport mode. Criteria
identified in the main analysis were evaluated separately in patients transported by ground EMS
(GEMS) and patients transported by HEMS, based on evidence that prehospital time may not be
the only important factor across transport modes.12
Subset Analysis
Analysis of the PTOS subset was aimed at evaluating the effect of transport distance,
time of day, and prehospital interventions on prehospital time. After excluding biased patients
with long prehospital times as above, similar models used in the NTDB were constructed. Given
the lower power of the subset analysis, all patients with criteria identified through the NTDB
analysis were included in each subset model.
To evaluate the effect of distance on prehospital time, transport distance was calculated
between patients' zip code centroid and the receiving trauma center address. Distance for patients
transported by HEMS was calculated using straight-line Euclidean distance. Distance for patients
transported by GEMS was calculated as the driving distance using geographic information
systems network analysis. (ArcGIS v10.5, ESRI, Redlands, CA). Transport distance and its
interaction with prehospital time were included in the model.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

10
To evaluate the effect of time of day on prehospital time, patient transports were
classified as peak or off-peak travel times based on recorded time of injury. Peak travel times
were defined as weekdays between 6:00am to 10:00am, and 3:00pm to 7:00pm to identify
periods of high traffic volume.13
Models were run separately on patients transported under peak
and off-peak traffic conditions.
To evaluate the effect of prehospital interventions on prehospital time, three prehospital
interventions available in PTOS were considered including intubation, crystalloid administration,
and blood transfusion. Models were run separately on patients receiving none of these
prehospital interventions and those receiving one or more of these interventions.
RESULTS
There were 2,508,215 patients eligible for inclusion (Fig. 1). Visual inspection of
mortality plotted against prehospital time demonstrated a higher mortality for prehospital times
≤30minutes (Fig. 2). Cubic spline analysis also demonstrated an inflection in the odds of
mortality over a similar prehospital time frame (AOR 1.17; 95%CI 1.26—1.36, Fig. 2). Thus,
prehospital time ≤30minutes is the empiric threshold at which longer prehospital times represent
a biased group based on the current data.
Further analysis was performed only on patients with total prehospital time ≤30minutes,
leaving 517,863 patients for analysis. The median prehospital time was 26minutes (IQR 22, 28),
with nearly a quarter of these patients sustaining penetrating injury, moderate injury by ISS
(median 9; IQR 4, 14), but significant mortality rate at 7.4% (Table 1).
In the overall study population, mortality was not associated with total prehospital time
(AOR 0.984; 95%CI 0.960—1.009, p=0.20). The model had excellent discrimination with a c-
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

11
statistic of 0.937. The model was also well calibrated when plotting predicted versus observed
mortality (Supplemental Digital Content 1, Figure 1, http://links.lww.com/TA/B313).
Interaction testing demonstrated significant interactions between prehospital time and
SBP (p=0.04), GCS (p=0.04), and mechanism of injury (p<0.001). Patients with SBP<90mmHg,
GCS≤ 8, or non-extremity firearm injury had increased odds of mortality associated with
increasing total prehospital time (Table 2), while patients without these criteria, including those
with extremity firearm injuries and non-firearm penetrating injuries, had no association between
mortality and prehospital time (p>0.05). Combinations of these criteria demonstrated higher odds
of mortality per 5-minute increase in prehospital time, with the exception of patients presenting
with all three criteria (Table 2). Patients presenting with all three criteria had 76.8% mortality
and this may mitigate the effect of increasing prehospital time in this moribund group. Among
these criteria, 24.7% of patients with SBP<90mmHg, 15.7% of patients with GCS≤8, and 42.7%
of patients with non-extremity firearm injury required urgent operation. Patients with one or
more of these criteria represented 21.1% of the study population and 81.6% of patients that died.
Interactions between prehospital time and anatomic injury pattern were non-significant (p>0.05).
Among the transport mode subgroups, there were too few HEMS transports with total
prehospital time ≤30minutes to allow meaningful analysis. Thus, to expand the number of
patients available in the HEMS subgroup, restricted cubic spline analysis was performed on
HEMS patients only, and an inflection with a decline in the odds of mortality was identified at
70minutes (Supplemental Digital Content 2, Figure 2, http://links.lww.com/TA/B314). Thus, we
included patients with prehospital time ≤70minutes for the HEMS subgroup analysis.
The same three criteria again identified patients with increased odds of mortality
associated with increasing prehospital time among those transported by GEMS (Table 3).
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

12
Among HEMS transports, SBP<90mmHg and non-extremity firearm injury identified patients
with increased odds of mortality associated with increasing prehospital time, while patients with
GCS≤8 had lower odds of mortality associated with increasing time (Table 3).
Of patients with GCS≤8, 16.3% of GEMS patients were intubated, while 49.4% of
HEMS patients were intubated upon arrival to the emergency department. When further
exploring patients with GCS≤8 by intubation status, those transported with GEMS had increased
odds of mortality associated with increasing prehospital time whether intubated (AOR 1.087;
95%CI 1.025—1.153, p=0.01) or not intubated (AOR 1.035; 95%CI 1.010—1.065, p=0.02).
Patients with GCS≤8 transported by HEMS had no association between mortality and prehospital
time if not intubated (AOR 0.980; 95%CI 0.0942—1.011, p=0.17), but had lower odds of
mortality associated with increased prehospital time if intubated (AOR 0.95; 95%CI 0.917—
0.986, p=0.01).
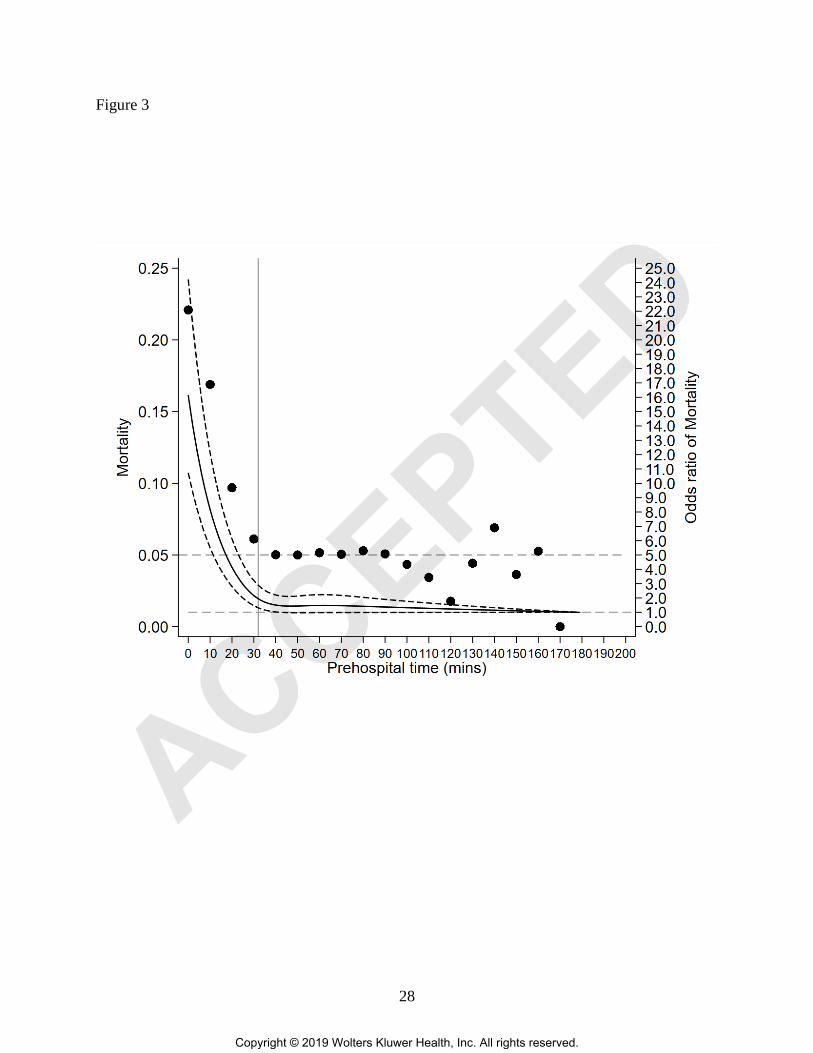
In PTOS, mortality also increased at a prehospital time ≤30minutes (Fig. 3), leaving
26,488 patients for subset analysis. This included 5,356 (20.2%) patients with SBP<90mmHg,
GCS≤ 8, or non-extremity firearm injury. Patients with at least one of these criteria had 17%
increase in odds of mortality per 5-minute increase in prehospital time (AOR 1.170; 95%CI
1.048—1.306, p<0.01).
When evaluating patients with at least one of these criteria, the interaction between
transport distance and prehospital time was not significant (p=0.59), nor was distance itself
(p=0.36) while prehospital time remained associated with mortality (p=0.01). An increase in
mortality for longer prehospital time was seen during off-peak traffic (AOR 1.142; 95%CI
1.023—1.274, p=0.02); however, this effect was magnified during peak traffic (AOR 1.419;
95%CI 1.026—1.963, p=0.03). Finally, longer prehospital time was associated with higher
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

13
mortality odds among patients receiving any prehospital intervention (AOR 1.260; 95%CI
1.120—1.417, p<0.01), while there was no association between prehospital time and mortality
among patients receiving no prehospital interventions (p=0.64). Patients with no prehospital
interventions had shorter prehospital time (22 [IQR 18, 26] versus 24 [IQR 20, 27], p<0.01).
DISCUSSION
The current study demonstrated a subset of existing trauma triage criteria can identify
patients in the field who have increased risk of mortality associated with increasing prehospital
time, including SBP<90mmHg, GCS≤8, and non-extremity firearm injury in a cohort with
prehospital time of ≤30minutes. These criteria may not be surprising, as they represent patients
in shock, with severe traumatic brain injury, and need for operative control of hemorrhage.
However, no study exists that has evaluated field criteria that can identify patients with time-
sensitive injuries and may benefit from minimizing prehospital time. These criteria also represent
current trauma triage criteria familiar to EMS providers, similar to the approach Champion and
colleagues used in developing the triage version of the Revised Trauma Score based on
categorized physiologic variables.14
Further, this data suggests these criteria represent 1 in 5
trauma patients with over 80% of deaths that may benefit from rapid transport to minimize
prehospital time. This may be particularly salient as Drake et al demonstrated a
preventable/potentially preventable death rate of 36% with hemorrhage the leading cause in
prehospital deaths.15
Results from prior work have been mixed regarding the relationship between mortality
and prehospital time, and it unclear that reducing prehospital time translates to better outcomes
after injury.16
Many recent studies in the US have not shown shorter prehospital times reduce
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

14
mortality. Newgard et al in a prospective cohort found no association between mortality and any
prehospital time interval in patients meeting physiologic field criteria.4 Several others also found
no association between outcome and prehospital time among undifferentiated trauma patients.3, 6,
8, 17, 18 Pepe found no association in hypotensive penetrating patients based on trauma score
stratification.5 Some groups have reported lower mortality in patients with longer prehospital
time, suggesting as noted above a survival bias.19, 20
Early data demonstrated mortality was associated with prehospital time, with up to a 5%
increase in mortality odds per 1-minute increase in prehospital time.21-23
More recent data has
suggested an association limited to specific subgroups of patients. Swaroop and colleagues
demonstrated a stepwise increase in mortality as prehospital time increased for hypotensive
patients with penetrating thoracic injury.24
Tien et al demonstrated a 3% increase in mortality
odds for each 1-minute increase in patients with subdural hematomas.25
Alarhayem and
colleagues also evaluated the NTDB and demonstrated increasing mortality with increasing
prehospital time among patients with torso injuries, particularly in the first 30minutes.26
Our
group previously reported prolonged scene time relative to other prehospital time intervals was
associated with increased mortality in patients with SBP<90mmHg, penetrating injury, and flail
chest even when accounting for prehospital interventions.27
Holcomb clearly demonstrated death
from severe truncal hemorrhage occurs before operative control is possible, highlighting the
importance of minimizing prehospital time as well as pushing critical interventions to mitigate
hemorrhage into the field for these patients.15
The military has shown over the recent conflicts
that prehospital time is a significant factor driving mortality in battlefield injuries. Policy change
that resulted in significant reductions in prehospital time was consistently associated with
improved mortality.28, 29
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

15
Interestingly, in subset analysis distance was not associated with mortality, but
prehospital time remained important. This suggests that strategies to limit prehospital time even
at long distances such as HEMS transport may be a successful strategy to reduce mortality in
these patients. Additionally, peak traffic time magnified the effect of prehospital time on
mortality likely due to delays in response and transport. Thus, again use of HEMS at shorter
distances during peak traffic may reduce prehospital time.30
When evaluating the effect of prehospital interventions on prehospital time and mortality
in subset analysis, patients that underwent any prehospital intervention had higher odds of
mortality associated with longer prehospital time, while those that underwent no prehospital
intervention had lower prehospital times which were no longer significantly associated with
mortality. This suggests for patients meeting one of the time-sensitive criteria, a scoop and run
approach may be favored as the time to perform field interventions results in an increase in
mortality as prehospital time increases.
These findings have several potential implications. At the individual patient level, these
criteria may help EMS providers make decisions about if and when to provide prehospital
interventions based on the presence or absence of the criteria demonstrated here. These criteria
allow EMS providers to take a more tailored approach to their patients, applying a scoop and run
approach in patients who may truly benefit from it. This also may allow mitigation of risk to
EMS providers and the public by informing appropriate utilization strategies for HEMS or use of
lights and sirens transport.31, 32
At the system level, these criteria may be considered in triage
protocols to encourage minimization of scene time. They may facilitate performance
improvement review to identify opportunities to reduce delays in patients meeting these criteria.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

16
These potential clinical and policy implications require further targeted study prior to
consideration of wide-spread application.
In our transport mode subgroup analysis, patients transported by GEMS had increasing
mortality associated with increasing prehospital time across all three criteria, while HEMS
patients only had this relationship if they had SBP<90mmHg or non-extremity firearm injury.
However, HEMS patients had lower mortality associated with increasing prehospital time if they
had GCS≤8. When investigating the potential role of prehospital intubation in patients with
GCS≤8, lower mortality was associated with longer prehospital time in patients intubated by
HEMS crews, while increased mortality was associated with increasing prehospital time in
GEMS patients regardless of intubation status. The point estimate for mortality odds was more
than double for patients who were intubated compared with those not intubated by GEMS crews.
These finding suggest prehospital intubation significantly affects outcomes for injured
patients with GCS≤8. Further, that effect is different across transport modes, and the additional
time to perform intubation in the field may improve outcome in the hands of HEMS but not
GEMS providers, which has been supported by prior reports as well.12, 33-35
GEMS and HEMS
differ with respect to training, experience, and regulatory requirements. Additionally, there may
be some selection bias as GEMS in some locations cannot perform medication assisted
intubation. Mounting evidence suggests the speed of HEMS transport is not the only important
factor, and the care received by HEMS crews influences outcome.12, 36, 37
These findings may
also have implications for air medical triage policies in which HEMS may be considered if it
would ultimately reduce prehospital time for patients with these criteria, or prehospital intubation
is indicated for GCS≤8.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

17
Taking the subset and transport subgroup data together, our results suggest patients with
SBP<90mmHg and non-extremity firearm injury should undergo few if any prehospital
interventions with priority placed on rapid transport to minimize prehospital time, while patients
with GCS≤8 benefit from undergoing prehospital intubation by HEMS providers when available
even if this may not result in the shortest prehospital time possible.
There are several limitations for consideration. First are those inherent to a retrospective
observational design. Second are those documented for the NTDB.38
The advantage of the
NTDB is a large national sample of patients; however, there are limited outcomes and variables
for analysis. We supplemented this limitation by performing a subset analysis using the PTOS
dataset which included more granular prehospital data. Missing data is always a limitation of
registry studies; however, we used multiple imputation to mitigate this. Despite our large sample
in the NTDB, cohorting based on triage criteria resulted in some small groups that limited our
power to evaluate the relationship of mortality and prehospital time. This is a particular
limitation in the PTOS subset analysis, requiring evaluation of patients with any one of the three
criteria identified in NTDB to maintain adequate power for regression modeling.
As noted above, we restricted analysis to prehospital times ≤30minutes to address the
survival bias inherent to long prehospital times in registry data based on empirical analysis of the
datasets utilized. This represents a trade-off in which we did not evaluate longer prehospital
times where there may be even more opportunity to minimize prehospital time, and limits our
generalizability. Our data likely are more representative of urban/suburban environments
relatively close to trauma centers. This is particularly important in potential urban-rural
differences of the prehospital time and outcome relationship, where different criteria may be
useful across different geographies. We also do not have the time from injury to 911-system
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED
18
notification which may be significant in some patients. A number of patients were missing
prehospital time and excluded; however, this represented only 9% of eligible patients.
Our primary outcome was in-hospital mortality; however, longer-term outcomes and
morbidity not available in the NTDB or PTOS are important outcomes for injured patients. Our
subgroup and subset analyses are exploratory and should be viewed to motivate future research.
We included HEMS patients with prehospital time ≥70minutes in subgroup analysis for power
reasons; however, this cutoff was based on data from similar cubic spline analysis used for the
main analysis. We investigated prehospital intubation as a potential mechanism of the
differences seen between HEMS and GEMS among patients with GCS≤8; however, there was
limited data available regarding timing or other prehospital interventions and again is
exploratory.
CONCLUSION
In patients with short total prehospital time, prehospital hypotension, GCS≤ 8, and non-
extremity firearm injury identify patients with increased risk of mortality associated with
increasing prehospital time. These patients may have truly time-sensitive injuries and benefit
from rapid transport to definitive care with few or no prehospital interventions. An exception is
patients with GCS≤ 8 that may benefit from intubation by HEMS providers. Further prospective
research is necessary to refine the identification of patients with time-sensitive injuries in the
field and overcome the survival bias for patients with longer prehospital times.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

19
ACKNOWLEDGEMENTS
Committee on Trauma, American College of Surgeons. NTDB 2007-2015, Chicago, IL. The
content reproduced from the NTDB remains the full and exclusive copyrighted property of the
American College of Surgeons. The American College of Surgeons is not responsible for any
claims arising from works based on the original data, text, tables, or figures.
AUTHOR CONTRIBUTIONS: X.C., F.X.G., and J.B.B. designed the study and performed the
literature search. X.C and J.B.B. performed the data collection. X.C. and J.B.B performed the
data analysis. X.C., F.X.G, and J.B.B. participated in initial manuscript preparation. All authors
contributed to data interpretation and critical revision of the manuscript.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

20
REFERENCES
1. Lerner EB, Moscati RM. The golden hour: scientific fact or medical "urban legend"?
Acad Emerg Med. 2001;8:758-760.
2. Seamon MJ, Fisher CA, Gaughan J, Lloyd M, Bradley KM, Santora TA, Pathak AS,
Goldberg AJ. Prehospital procedures before emergency department thoracotomy: "scoop
and run" saves lives. J Trauma. 2007;63:113-120.
3. Lerner EB, Billittier AJ, Dorn JM, YB W. Is Total Out-of-hospital Time a Significant
Predictor of Trauma Patient Mortality? Acad Emerg Med. 2003;10:949-954.
4. Newgard CD, Schmicker RH, Hedges JR, Trickett JP, Davis DP, Bulger EM,
Aufderheide TP, Minei JP, Hata JS, Gubler KD, et al. Emergency medical services
intervals and survival in trauma: assessment of the "golden hour" in a North American
prospective cohort. Ann Emerg Med. 2010;55:235-246 e234.
5. Pepe PE, Wyatt CH, Bickell WH, Bailey ML, Mattox KL. The relationship between total
prehospital time and outcome in hypotensive victims of penetrating injuries. Ann Emerg
Med. 1987;16:293-297.
6. Petri RW, Dyer A, Lumpkin J. The effect of prehospital transport time on the mortality
from traumatic injury. Prehosp Disaster Med. 1995;10:24-29.
7. Pons PT, Markovchick VJ. Eight minutes or less: does the ambulance response time
guideline impact trauma patient outcome? J Emerg Med. 2002;23:43-48.
8. Stiell IG, Nesbitt LP, Pickett W, Munkley D, Spaite DW, Banek J, Field B, Luinstra-
Toohey L, Maloney J, Dreyer J, et al. The OPALS Major Trauma Study: impact of
advanced life-support on survival and morbidity. CMAJ. 2008;178:1141-1152.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

21
9. Rubin DB. Multiple Imputation for Nonresponse in Surveys. Hoboken, NJ: John Wiley &
Sons; 1987.
10. Sasser SM, Hunt RC, Faul M, Sugerman D, Pearson WS, Dulski T, Wald MM, Jurkovich
GJ, Newgard CD, Lerner EB, et al. Guidelines for Field Triage of Injured Patients.
MMWR. 2012;61:1-20.
11. Benjamini Y, Hochberg Y. Controlling the False Discovery Rate: A Practical and
Powerful Approach to Multiple Testing. J R Statist Soc B. 1995;57:289-300.
12. Chen X, Gestring ML, Rosengart MR, Billiar TR, Peitzman AB, Sperry JL, Brown JB.
Speed is not everything: Identifying patients who may benefit from helicopter transport
despite faster ground transport. J Trauma Acute Care Surg. 2018;84:549-557.
13. Schrank D, Eisele B, Lomax T, Bak J. 2015 Urban Mobility Score Card. In. College
Station, Tx: Texas A&M Transportation Institute, 2015.
14. Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA, Flanagan ME. A
Revision of the Trauma Score. J Trauma Acute Care Surg. 1989;29:623-629.
15. Drake SA, Holcomb JB, Yang Y, Thetford C, Myers L, Brock M, Wolf DA, Cron S,
Persse D, McCarthy J, et al. Establishing a Regional Trauma Preventable/Potentially
Preventable Death Rate. Ann Surg. 2018.
16. Harmsen AM, Giannakopoulos GF, Moerbeek PR, Jansma EP, Bonjer HJ, Bloemers FW.
The influence of prehospital time on trauma patients outcome: a systematic review.
Injury. 2015;46:602-609.
17. Baez AA, Lane PL, Sorondo B, Giraldez EM. Predictive effect of out-of-hospital time in
outcomes of severely injured young adult and elderly patients. Prehosp Disaster Med.
2006;21:427-430.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

22
18. McCoy CE, Menchine M, Sampson S, Anderson C, Kahn C. Emergency medical services
out-of-hospital scene and transport times and their association with mortality in trauma
patients presenting to an urban Level I trauma center. Ann Emerg Med. 2013;61:167-174.
19. Osterwalder JJ. Can the "golden hour of shock" safely be extended in blunt polytrauma
patients? Prospective cohort study at a level I hospital in eastern Switzerland. Prehosp
Disaster Med. 2002;17:75-80.
20. Ryb GE, Dischinger P, Cooper C, Kufera JA. Does helicopter transport improve
outcomes independently of emergency medical system time? J Trauma Acute Care Surg.
2013;74:149-154; discussion 154-146.
21. Sampalis JS, Denis R, Lavoie A, Frechette P, Boukas S, Nikolis A, Benoit D, Fleiszer D,
Brown R, Churchill-Smith M, et al. Trauma Care Regionalization: A Process-Outcome
Evaluation. J Trauma Acute Care Surg. 1999;46:565-581.
22. Sampalis JS, Lavoie A, Williams JI, Mulder DS, Kalina M. Impact of on-site care,
prehospital time, and level of in-hospital care on survival in severely injured patients. J
Trauma. 1993;34:252-261.
23. Feero S, Hedges JR, Simmons E, Irwin L. Does out-of-hospital EMS time affect trauma
survival? Am J Emerg Med. 1995;13:133-135.
24. Swaroop M, Straus DC, Agubuzu O, Esposito TJ, Schermer CR, Crandall ML. Pre-
hospital transport times and survival for Hypotensive patients with penetrating thoracic
trauma. J Emerg Trauma Shock. 2013;6:16-20.
25. Tien HC, Jung V, Pinto R, Mainprize T, Scales DC, Rizoli SB. Reducing time-to-
treatment decreases mortality of trauma patients with acute subdural hematoma. Ann
Surg. 2011;253:1178-1183.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED
23
26. Alarhayem AQ, Myers JG, Dent D, Liao L, Muir M, Mueller D, Nicholson S, Cestero R,
Johnson MC, Stewart R, et al. Time is the enemy: Mortality in trauma patients with
hemorrhage from torso injury occurs long before the "golden hour". Am J Surg.
2016;212:1101-1105.
27. Brown JB, Rosengart MR, Forsythe RM, Reynolds BR, Gestring ML, Hallinan WM,
Peitzman AB, Billiar TR, Sperry JL. Not all prehospital time is equal: Influence of scene
time on mortality. J Trauma Acute Care Surg. 2016;81:93-100.
28. Howard JT, Kotwal RS, Santos-Lazada AR, Martin MJ, Stockinger ZT. Reexamination
of a Battlefield Trauma Golden Hour Policy. Journal of Trauma and Acute Care Surgery.
2018;84:11-18.
29. Kotwal RS, Howard JT, Orman JA, Tarpey BW, Bailey JA, Champion HR, Mabry RL,
Holcomb JB, Gross KR. The Effect of a Golden Hour Policy on the Morbidity and
Mortality of Combat Casualties. JAMA Surg. 2016;151:15-24.
30. Bledsoe BE, Smith MG. Medical Helicopter Accidents in the United States: A 10-Year
Review. J Trauma Acute Care Surg. 2004;56:1325-1329.
31. Kahn CA, Pirrallo RG, Kuhn EM. Characteristics of fatal ambulance crashes in the
United States: an 11-year retrospective analysis. Prehosp Emerg Care. 2001;5:261-269.
32. Cudnik MT, Newgard CD, Wang H, Bangs C, Herrington Rt. Distance impacts mortality
in trauma patients with an intubation attempt. Prehosp Emerg Care. 2008;12:459-466.
33. Davis DP, Stern J, Sise MJ, Hoyt DB. A follow-up analysis of factors associated with
head-injury mortality after paramedic rapid sequence intubation. J Trauma. 2005;59:486-
490.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

24
34. Wang HE, Peitzman AB, Cassidy LD, Adelson PD, Yealy DM. Out-of-hospital
endotracheal intubation and outcome after traumatic brain injury. Ann Emerg Med.
2004;44:439-450.
35. Brown JB, Gestring ML, Guyette FX, Rosengart MR, Stassen NA, Forsythe RM, Billiar
TR, Peitzman AB, Sperry JL. Helicopter transport improves survival following injury in
the absence of a time-saving advantage. Surgery. 2016;159:947-959.
36. Holcomb JB, Donathan DP, Cotton BA, Del Junco DJ, Brown G, Wenckstern TV,
Podbielski JM, Camp EA, Hobbs R, Bai Y, et al. Prehospital Transfusion of Plasma and
Red Blood Cells in Trauma Patients. Prehosp Emerg Care. 2014;19:1-9.
37. Chen X, Gestring ML, Rosengart MR, Peitzman AB, Billiar TR, Sperry JL, Brown JB.
Logistics of air medical transport: When and where does helicopter transport reduce
prehospital time for trauma? J Trauma Acute Care Surg. 2018;85:174-181.
38. American College of Surgeons. NTDB Research Data Set User Manual and Variable
Description List. American College of Surgeons. 2017
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

25
FIGURE LEGEND
Figure 1. Patient selection from the National Trauma Databank (NTDB) from 2007 to 2015.
Figure 2. Mortality rate (left axis) and odds of mortality (right axis) from cubic spline regression
plotted against total prehospital time in the NTDB. Top horizontal dashed line represents 5%
mortality rate. Bottom horizontal dashed line represents odds of mortality of 1.0. The odds of
mortality increase above 1.0 at prehospital times of ≤30minutes (vertical gray line).
Figure 3. Mortality rate (left axis) and odds of mortality (right axis) from cubic spline regression
plotted against total prehospital time in PTOS. Top horizontal dashed line represents 5%
mortality rate. Bottom horizontal dashed line represents odds of mortality of 1.0. The odds of
mortality increase above 1.0 at prehospital times of ≤30minutes (vertical gray line).
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

26
Figure 1
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

27
Figure 2
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED
28
Figure 3
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

29
Table 1. Analysis population characteristics and triage criteria.
N 517,863
Age, years median (IQR) 40 (26, 58)
Gender, n (%)
Female 150,324 (29.0%)
Male 367,539 (71.0%)
Race, n (%)
White 300,642 (58.1%)
Non-white 217,221 (41.9%)
Insurance status, n (%)
None/Subsidized 332,554 (64.2%)
Commercial 185,309 (35.8%)
Transport mode, n (%)
Ground 511,612 (98.8%)
Helicopter 6,251 (1.2%)
Total prehospital time, mins median (IQR) 26 (22, 28)
ISS, median (IQR) 9 (4, 14)
ICU admission, n (%) 156,239 (30.2%)
Prehospital SBP, mmHg median (IQR) 133 (116, 150)
Admission SBP, mmHg median (IQR) 136 (119, 153)
Urgent operation, n (%) 12,647 (2.4%)
Any complication, n (%) 108,512 (21.0%)
In-hospital mortality, n (%) 38,167 (7.4%)
Triage Criteria
Prehospital SBP<90mmHg, n (%) 37,642 (7.8%)
Prehospital RR<10 or >29, n (%) 39,642 (8.1%)
Prehospital GCS≤13, n (%) 108,081 (22.0%)
Prehospital GCS≤8, n (%) 62,348 (12.7%)
Penetrating injury mechanism, n (%) 121,335 (23.4%)
Non-extremity firearm injury, n (%) 43,308 (8.36%)
Unstable chest wall fractures, n (%) 20,688 (4.0%)
Open skull fracture, n (%) 10,431 (2.0%)
≥2 proximal long bone fractures, n (%) 6,905 (1.3%)
Pelvic fracture, n (%) 36,676 (7.1%)
Amputation, n (%) 1,335 (0.3%)
Crush injury, n (%) 1,640 (0.3%)
Paralysis, n (%) 2,280 (0.4%)
Hemothorax/Pneumothorax, n (%) 59,186 (11.4%)
Multisystem injury, n (%) 5,763 (1.1%)
Physiologic and anatomic criterion, n (%) 53,428 (10.3%)
IQR, interquartile range; ISS, injury severity score; ICU, intensive
care unit; SBP, systolic blood pressure; RR, respiratory rate; GCS,
Glasgow Coma Scale
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

30
Table 2. Adjusted odds ratio of in-hospital mortality per 5-minute increase in total prehospital time.
Triage Criterion AOR 95%CI p value
SBP<90mmHg 1.039 1.003—1.078 0.045
GCS≤8 1.047 1.018—1.076 0.001
Non-extremity firearm injury 1.049 1.010—1.089 0.011
Combination of criteria
SBP<90mmHg + non-extremity firearm injury 1.079 1.015—1.147 0.015
SBP<90mmHg + GCS≤8 1.069 1.027—1.112 0.001
GCS≤8 + non-extremity firearm injury 1.061 1.001—1.126 0.048
SBP<90mmHg + GCS≤8 + non-extremity firearm injury 1.047 0.967—1.132 0.259
AOR, adjusted odds ratio; 95%CI, 95% confidence interval; SBP, systolic blood pressure; GCS, Glasgow
Coma Scale
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

31
Table 3. Adjusted odds ratio of in-hospital mortality per 5-minute increase in total
prehospital time by transport mode subgroup
Triage Criterion AOR 95%CI p value
GEMS
SBP<90mmHg 1.042 1.004—1.082 0.030
GCS≤8 1.050 1.022—1.079 <0.001
Non-extremity firearm injury 1.090 1.040—1.142 <0.001
HEMS*
SBP<90mmHg 1.042 1.005—1.081 0.020
GCS≤8 0.967 0.942—0.992 0.010
Non-extremity firearm injury 1.065 1.009—1.125 0.022
* Includes patients with total prehospital time ≤70 minutes
AOR, adjusted odds ratio; 95%CI, 95% confidence interval; GEMS, ground emergency
medical services; HEMS, helicopter emergency medical services; SBP, systolic blood
pressure; GCS, Glasgow Coma Scale
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED

32
SUPPLEMENTAL DIGITAL CONTENT
eFigure 1. Calibration curve of predicted versus observed mortality across predicted mortality
risk deciles from the multivariable risk-adjustment logistic regression model.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED
33
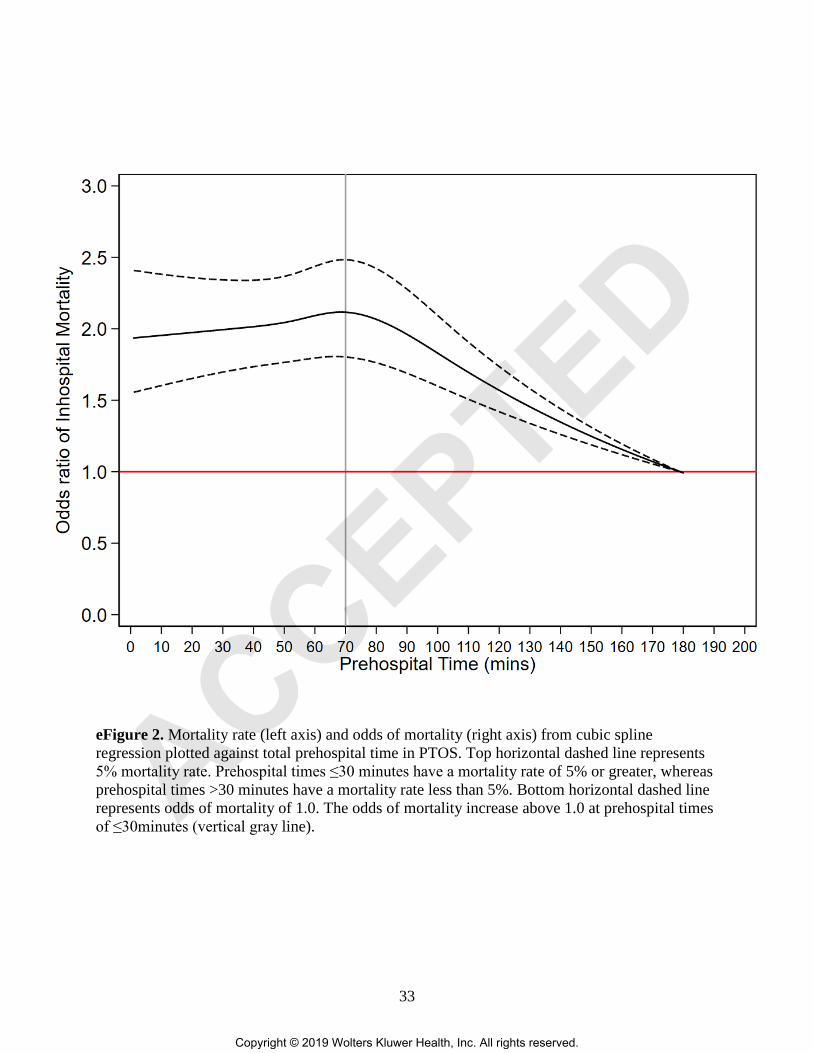
eFigure 2. Mortality rate (left axis) and odds of mortality (right axis) from cubic spline
regression plotted against total prehospital time in PTOS. Top horizontal dashed line represents
5% mortality rate. Prehospital times ≤30 minutes have a mortality rate of 5% or greater, whereas
prehospital times >30 minutes have a mortality rate less than 5%. Bottom horizontal dashed line
represents odds of mortality of 1.0. The odds of mortality increase above 1.0 at prehospital times
of ≤30minutes (vertical gray line).
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
ACCEPTED





























