Embed Size (px)
Citation preview

Identifying Schizophrenia and Bipolar Disorder from a Sea of Mimics
Michael Sean Stanley, MD
Assistant Professor
OHSU Department of Psychiatry

Identifying Schizophrenia and Bipolar Disorder from a Sea of Mimics
No Disclosures.

• Objectives:
– Understand the clinical presentation and approach to treatment of Schizophrenia and Bipolar Disorder
Psychotic disorders are:
• primarily problems of sensory processing and association, not emotion
• Exhibit profound disconnection from sensory reality
Mood Disorders are:
• Primarily problems of prolonged extreme emotional tone (mood).
• Exhibit excessive high or low mood/motivation from normal state

Psychosis
Schizophrenia

Schizophrenia
• a neurodevelopmental syndrome
• associated with functional impairments
• no single unifying cause
• emerges when environmental accelerants act upon genetic predisposition
• May be at the more severely impairing end of a spectrum of disorders.



+ -Positive Symptoms
New abnormal sx- Hallucinations
(auditory most commonly)
- Delusions- Significant
disorganization of thought/behavior
May come and go
May be responsive to antipsychotic meds
Negative Symptoms
Loss of normal fxn- Affective flattening- Anhedonia- Asociality- Alogia
A stable loss, do not fluctuate significantly once lost.
Minimally responsive to antipsychotic meds if at all.
For 6 mo or longer; Not due to medical or substance use cause.
Cognitive Symptoms
Accompany and likely precede +/- sx- Attentional problems- Slower processing- Difficulty with
planning/probsolving
- Memory problems
Prodromal sx?
May decrease to some degree with tx of pos sx, but rarely completely.
C

Positive Symptoms

Most commonly during teens-20s

Genetics:• Highly heritable – 30% of offspring• Many genes with small effect size• Some genetic overlap with other psych dx:
BPAD, MDD, Autism Spectrum DO• Genes point to multiple mechanisms
• Pathways implicated by Genes (a selection)• Synaptic function (DRD2, GlutR, voltage-
dependent calcium channels)• Synaptic plasticity• Cytoskeletal development• Immune response/modulation
Inflammatory EventsDamage Events
Inappropriate Pruning or Synaptic Changes: • Decr grey matter
• Prefrontal• Parahippoca
mpal• Temporal• thalamic
• Decr dendritic spines
Neuro-Cognitive Network Imbalance• Lack of coordination
of neural tasks• Lack of inhibition of
neural tasks
Inappropriate salience –hallucinations/delusions

Schizophrenia
Onset• One peak in men: generally adolescence to early 20s• Two peaks in women: similar as above + over 40sPrevalence• Lifetime likelihood of 0.7%Disability• 80-90% unemployed• Life-expectancy 10-20 years reduced
• Most likely due to cardiovascular and other health problems• High prev of smoking• High prev of dietary indiscretions• Low medical care use• Cardiometabolic effects of medication treatments

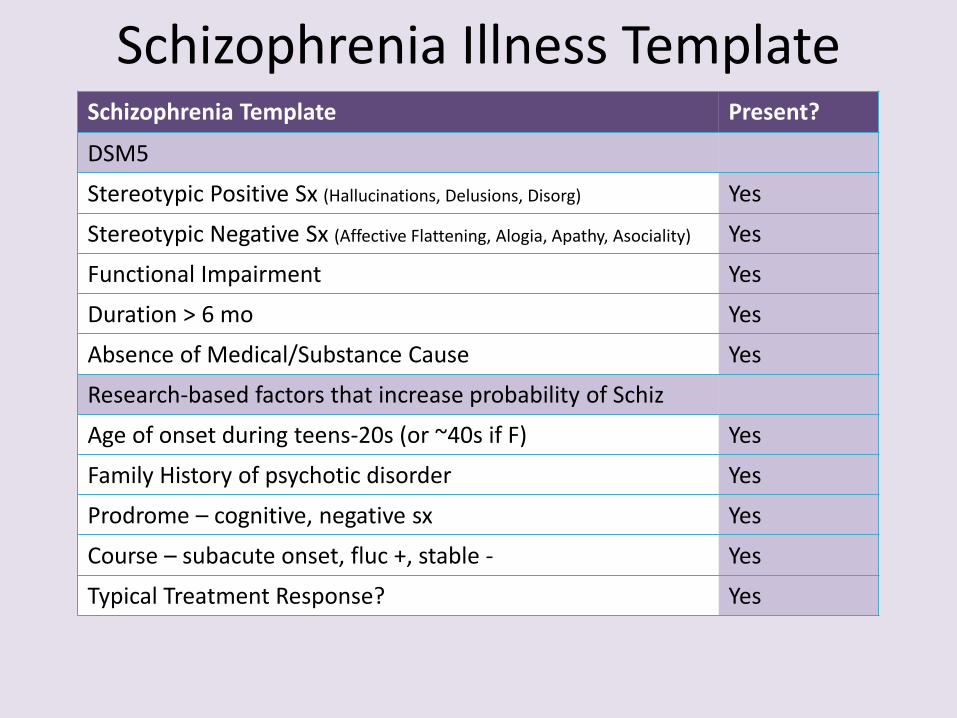
Schizophrenia Illness TemplateSchizophrenia Template Present?
DSM5
Stereotypic Positive Sx (Hallucinations, Delusions, Disorg)
Stereotypic Negative Sx (Affective Flattening, Alogia, Apathy, Asociality)
Functional Impairment
Duration > 6 mo
Absence of Medical/Substance Cause
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F)
Family History of psychotic disorder
Prodrome – cognitive, negative sx
Course – subacute onset, fluc +, stable -
Typical Treatment Response?

Schizophrenia Template Case• 19 yo male• CC: Presents for auditory hallucinations of his high school physics professor arguing
with his parents about implanting novel “microcircuits” in his body. Feels this might be true, and has shaved parts of his body to scan the “microcircuits”
• HPI (from collateral): sx began about 1 year ago, have fluctuated, and have been associated w/ performance decline at community college, last quarter his teachers expressed concern and he was on monitoring plan by student health center. Per family, throughout high school, patient displayed some thoughts of supernatural causes, but they had not caused functional problems. Gradually late in high school he became increasingly reclusive, stopped being interested in things that previously interested him, these sx have continued.
• Family Hx: Paternal uncle with schizophrenia• Exam: Medical exam benign, has never used drugs other than tobacco.• Mental Status Exam: + AH and delusions, thought blocking, appeared to attend to
internal stimuli, flat affect, paucity of spontaneous thought. • Course: saw psychiatrist who Rx’d Risperidone 2mg qhs, which significantly decreased
AH. Stopped medication after 6 mo, when noticed gynecomastia, and AH restarted.
Schizophrenia Illness TemplateSchizophrenia Template Present?
DSM5
Stereotypic Positive Sx (Hallucinations, Delusions, Disorg) Yes
Stereotypic Negative Sx (Affective Flattening, Alogia, Apathy, Asociality) Yes
Functional Impairment Yes
Duration > 6 mo Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) Yes
Family History of psychotic disorder Yes
Prodrome – cognitive, negative sx Yes
Course – subacute onset, fluc +, stable - Yes
Typical Treatment Response? Yes
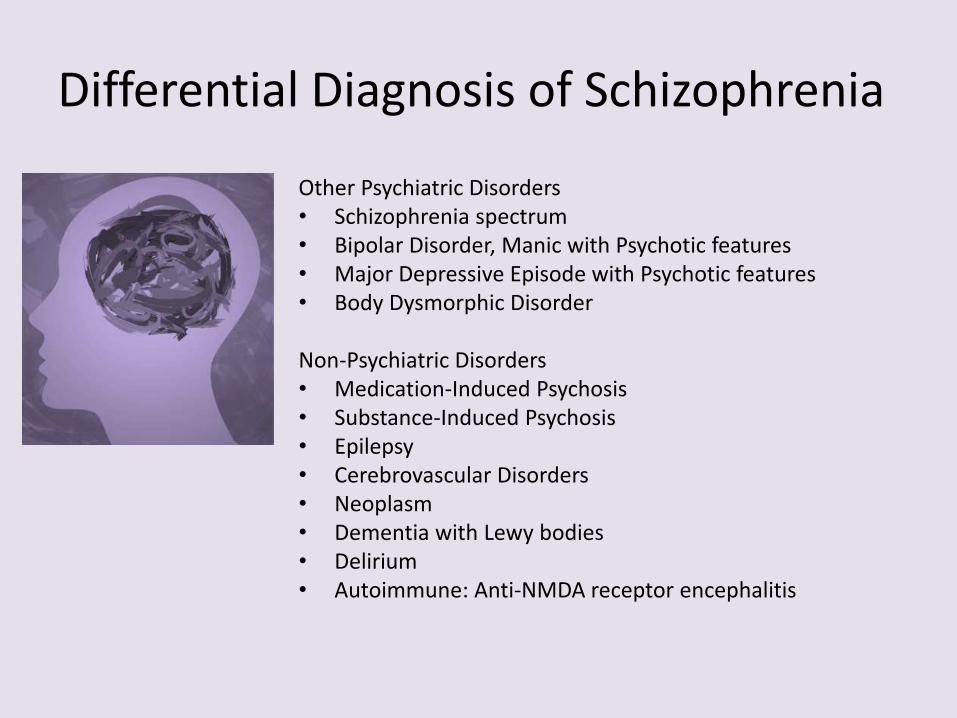
Differential Diagnosis of Schizophrenia
Other Psychiatric Disorders• Schizophrenia spectrum• Bipolar Disorder, Manic with Psychotic features• Major Depressive Episode with Psychotic features• Body Dysmorphic Disorder
Non-Psychiatric Disorders• Medication-Induced Psychosis• Substance-Induced Psychosis• Epilepsy• Cerebrovascular Disorders• Neoplasm• Dementia with Lewy bodies• Delirium• Autoimmune: Anti-NMDA receptor encephalitis

Psychotic symptoms, such as auditory hallucinations and paranoid thinking, occur in attenuated forms in 5–8% of the healthy population
Schizophrenia Spectrum
Normal
Schiz + prominent affective sx
Delusions only, function not grossly impaired
Cognitive or perceptual distortions or behavioral eccentricities that affect social connections, but not gross biological function
6 mo1 mo2+ sxDel only

Bipolar Disorder• a disorder of emotional tone
– Elevated = hypo/mania
– Low = major depressive episodes
• associated with functional impairments at peaks
• emerges when environmental accelerants act upon genetic predisposition
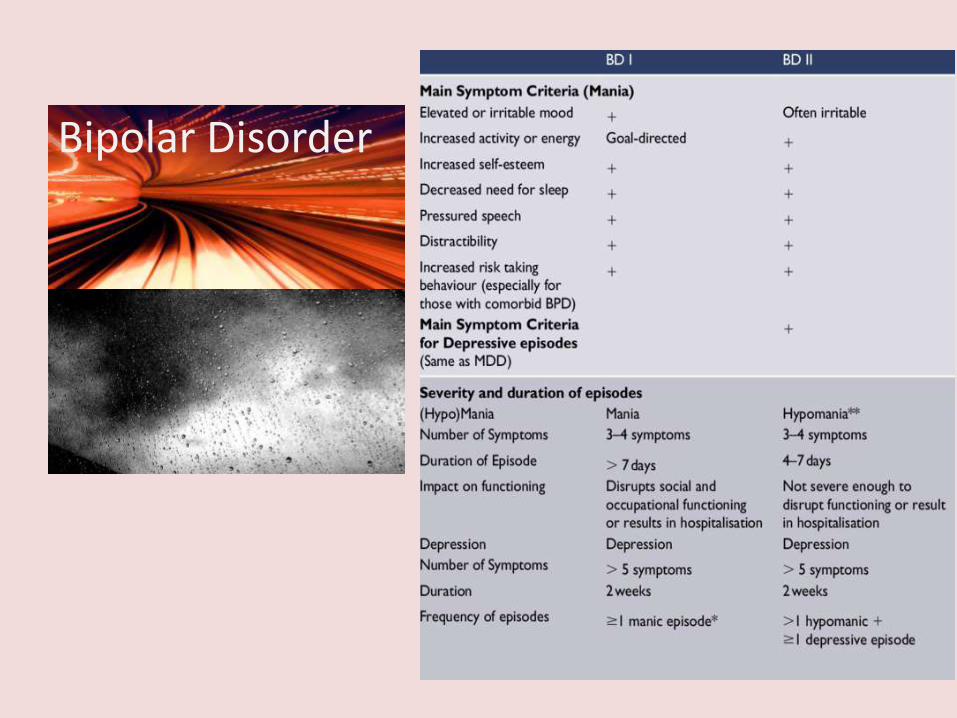
Bipolar Disorder

!!MANIC EPISODE!!
majordepressiveepisode
Bipolar DisorderEpidemiology of Bipolar Disorders:
• Lifetime prevalence of Bipolar Disorders is 1-3% worldwide
• Female:Male = 1:1
• Mean onset of Bipolar I DO is 18yo
• About 1/3 of patients with a parent with Bipolar Disorder will go on to have Bipolar Disorder
• Depressive Episodes are actually more common in Bipolar Disorder than are Manic/Hypomanic Episodes
• 10-15% of patients with Bipolar Disorder die by suicide, which is estimated at 12-15x greater rate than in the general population

Genetic Risk
Gestational or Birth Stress
Early Life Stress
Head Injury
Substance Use
Life Stressors
Mood lability, subsyndromal
depression or mania symptoms
MDD with subsyndromal
mania, cylothymia, or psychosis
Elation, irritable mood, excess energy,
talkativeness, racing thoughts, decreased
need for sleep
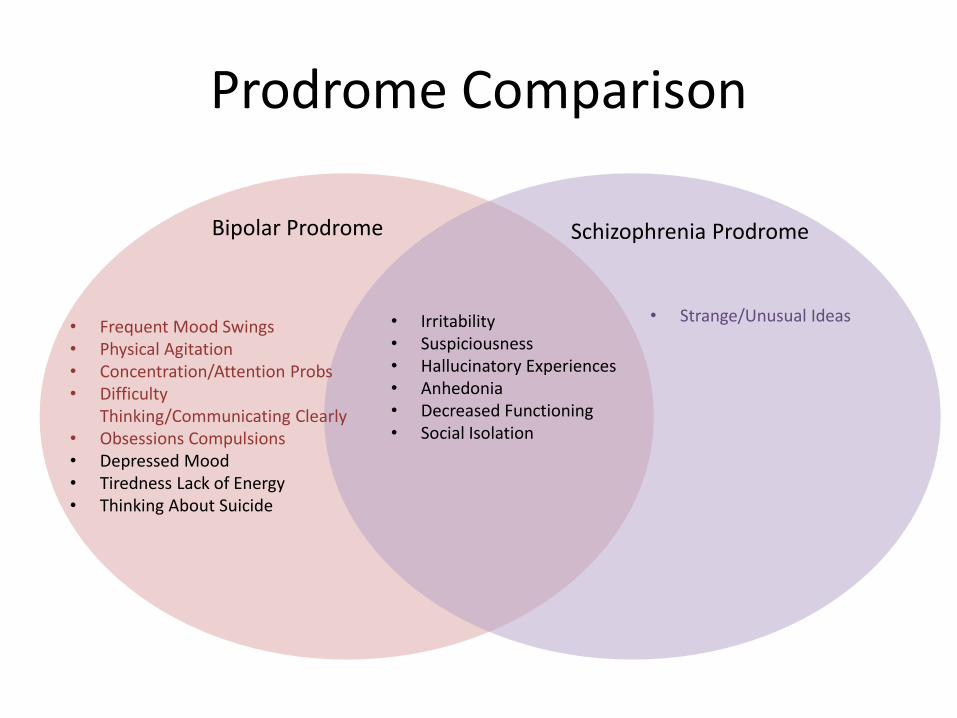
Prodrome Comparison
Bipolar Prodrome Schizophrenia Prodrome
• Frequent Mood Swings• Physical Agitation• Concentration/Attention Probs• Difficulty
Thinking/Communicating Clearly• Obsessions Compulsions• Depressed Mood• Tiredness Lack of Energy• Thinking About Suicide
• Strange/Unusual Ideas• Irritability• Suspiciousness• Hallucinatory Experiences• Anhedonia• Decreased Functioning• Social Isolation

Bipolar DO Illness TemplateBipolar Disorder Template Present?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
Major Depressive Episode (not needed if manic)
Functional Impairment
Absence of Medical/Substance Cause
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s
Family History of Bipolar Disorder
Prodrome – isolated manic sx
Course – episodic, relapsing/remitting
Typical Treatment Response?
Absence of other atypical features
Bipolar DO Template Case• 20 yo male• CC: Elevated mood, Increased energy, beliefs of God-given
mission to spread “heal broken street children” through “parkourscience”. Accompanied by agitation, decreased need for sleep, disorganized behaviors, rapid speech.
• HPI: sx started ~10 days ago, after returned from study abroad in Europe, increased gradually over 2-3 days.
• Collateral noted the following: • Cousin with Bipolar I Disorder on Lithium• Successfully recently completed 6 mo study abroad
program in global finance in Switzerland.• Has a girlfriend and 2 friends who accompanied him to ED,
and who are very worried about him, as this is very different behavior for him, as he has not been spiritual.
• Girlfriend noted that he had had sporadic periods of decreased need for sleep in past, but never like this.
• Med hx/Psych hx: no med probs, no psych dx, has never used drugs other than remote brief cannabis trial in high school
• Exam: agitation, talking mildly rapidly, focuses on spiritual mission, requires interruption, denies AH/VH, denies SI/HI.
• Course: Risperidone 2mg qhs, responded well, tapered off 12 molater, did not have recurrence of delusions immediately, although 2 years later had beginning of similar sx.

Bipolar DO Illness TemplateBipolar Disorder Template Present in this case?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
Yes
Major Depressive Episode (not needed if manic) N/A
Functional Impairment Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s Yes
Family History of Bipolar Disorder Yes
Prodrome – isolated manic sx Yes
Course – episodic, relapsing/remitting Yes
Typical Treatment Response? Yes
Absence of other atypical features Yes

Differential Diagnosis of Bipolar DOOther Psychiatric Disorders• Schizophrenia & spectrum• Major Depressive Disorder• Premenstrual Dysphoric Disorder• Borderline Personality Disorder• Attention-deficit Hyperactivity Disorder
Non-Psychiatric Disorders• Medication-Induced Mania
– Corticosteroids, Isoniazid, Levodopa
• Substance-Induced Mania– Cocaine, Stimulants, Cannabis
• Hyperthyroidism• Seizures/Strokes/Neoplasm• Multiple Sclerosis• Encephalitis
Bipolar Disorder

Identifying whether a primary psychiatric or secondary disorder:• there are no pathognomonic signs to differentiate primary from secondary disorders.
• Early differentiation is observational, based on• The known epidemiology and course of primary disorders• The known presentations of primary disorders:
• History• physical exam• mental status exam
• Any confounding features
• Follow-up over long-term watching for symptoms or signs that increase or decrease probability of primary psychiatric diagnosis

Cases
• 80 yo female• CC: New onset fixed false beliefs in the last few days that
she has caused the death of multiple friends, and the only way to atone is to starve herself. No hallucinations. Affect flattened.
• HPI: Adult daughter noted that her sx started 3 weeks ago, slowly becoming more encompassing; that she had stopped going to church, was isolating more over last month, staying in bedroom sleeping a lot, eating little.
• Past Med/Psych hx: mild vascular dz, a few episodes of major depression, but never tolerated medications long-term. Rare glass of red wine, no other substances.
• Fam Hx: depression, no psychosis. • Exam: psychomotor slowing, slowed responses, seems
distracted, flattened or sad affect, repeatedly comes back to thought that she must have caused deaths of friends.
• Course: Receives visits from members of church who have missed her leadership of their benevolent services committee. Referred to Electroconvulsive therapy (ECT) under daughter as POA, improves within a few weeks.
Case: “I’ve killed them all”
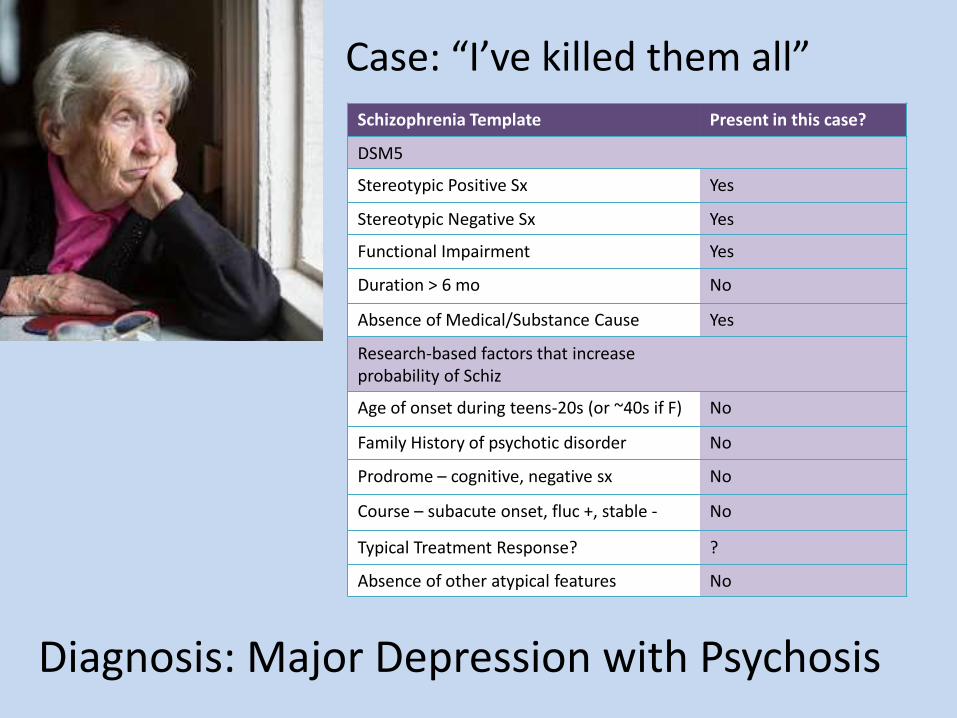
Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes
Stereotypic Negative Sx Yes
Functional Impairment Yes
Duration > 6 mo No
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) No
Family History of psychotic disorder No
Prodrome – cognitive, negative sx No
Course – subacute onset, fluc +, stable - No
Typical Treatment Response? ?
Absence of other atypical features No
Diagnosis: Major Depression with Psychosis
Case: “I’ve killed them all”

• 16 yo female• CC: New onset auditory hallucinations telling her to end
her life, tactile hallucinations of worms under her skin. • HPI: Started 1 week ago per friend, one day she was good
the next hallucinating. Per community health case worker who brought her to the ED, pt was recently homeless, has hx of DV trauma and parents with significant substance use disorders. Case worker had never seen her like this.
• Med/Psych Hx: no known medical conditions, hx of substance use, but no prior psychosis known.
• Exam: somewhat cooperative with exam, scratching at skin, asked if ED staff could see the worms, disorganized speech at times, agitation, teary at times.
• Labs: UDS +methamphetamines, no other abnormalities. • Course: Started on quetiapine 50mg BID and 100mg QHS,
kept in ED obs, calms over 24 hours to cooperative with nursing staff, very congenial and thankful upon discharge.Sees outpatient psychiatrist who quickly tapers her quetiapine, offers hydroxyzine and trazodone PRN as she enters treatment program.
Case: “they’re telling me to kill myself”

Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes
Stereotypic Negative Sx No
Functional Impairment Yes
Duration > 6 mo No
Absence of Medical/Substance Cause No
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) Yes
Family History of psychotic disorder No
Prodrome – cognitive, negative sx No
Course – subacute onset, fluc +, stable - No
Typical Treatment Response? No
Absence of other atypical features? No
Diagnosis: Psychosis due to Methamphetamine Use
Case: “they’re telling me to kill myself”
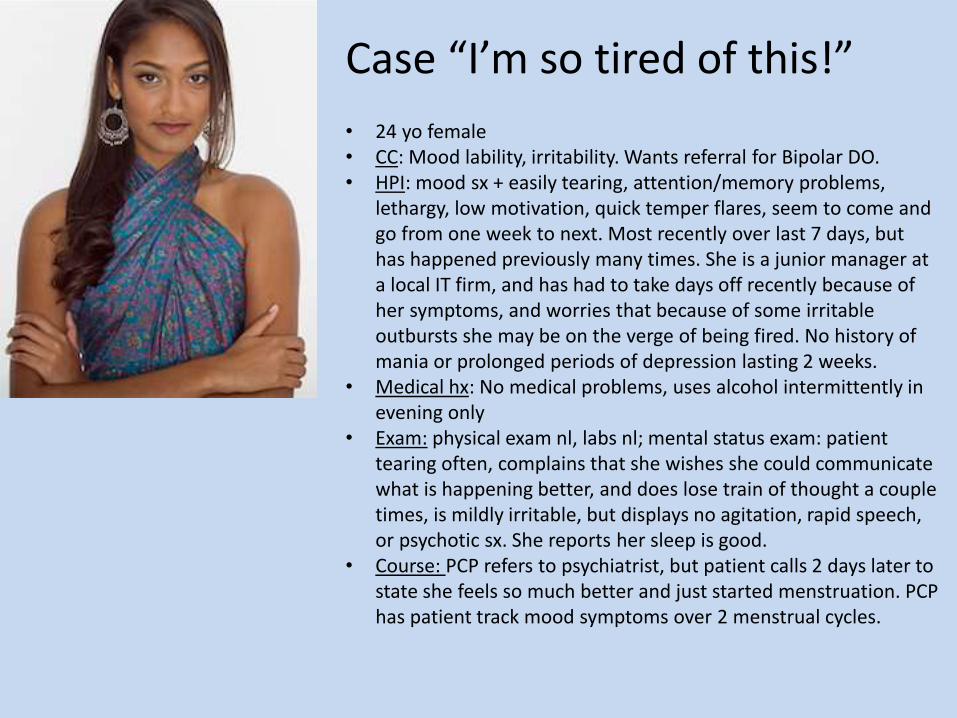
• 24 yo female• CC: Mood lability, irritability. Wants referral for Bipolar DO. • HPI: mood sx + easily tearing, attention/memory problems,
lethargy, low motivation, quick temper flares, seem to come and go from one week to next. Most recently over last 7 days, but has happened previously many times. She is a junior manager at a local IT firm, and has had to take days off recently because of her symptoms, and worries that because of some irritable outbursts she may be on the verge of being fired. No history of mania or prolonged periods of depression lasting 2 weeks.
• Medical hx: No medical problems, uses alcohol intermittently in evening only
• Exam: physical exam nl, labs nl; mental status exam: patient tearing often, complains that she wishes she could communicate what is happening better, and does lose train of thought a couple times, is mildly irritable, but displays no agitation, rapid speech, or psychotic sx. She reports her sleep is good.
• Course: PCP refers to psychiatrist, but patient calls 2 days later to state she feels so much better and just started menstruation. PCP has patient track mood symptoms over 2 menstrual cycles.
Case “I’m so tired of this!”
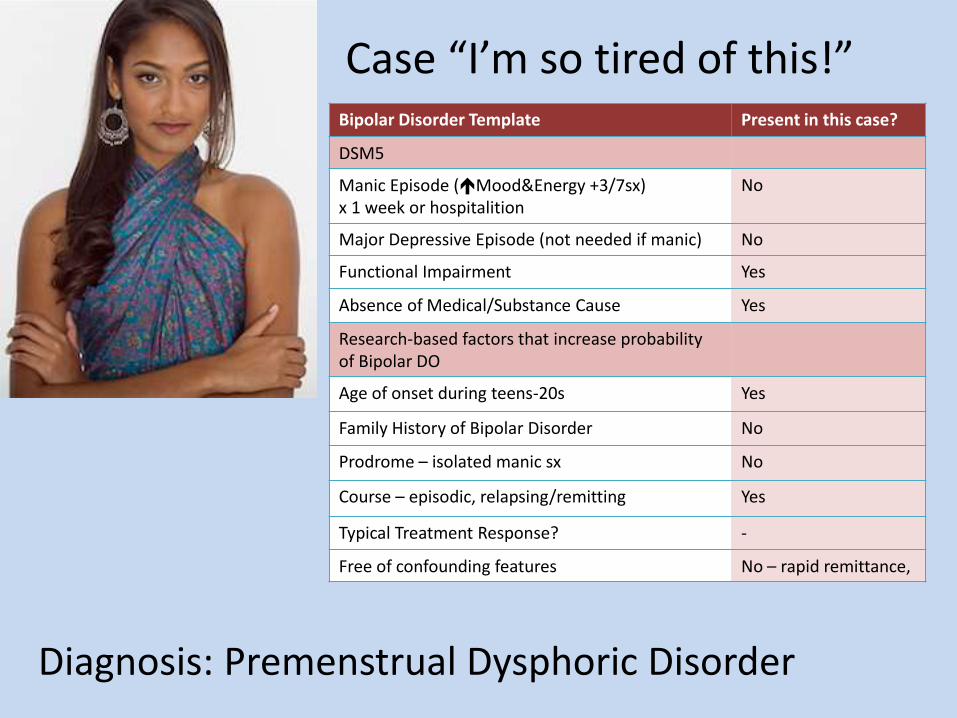
Diagnosis: Premenstrual Dysphoric Disorder
Bipolar Disorder Template Present in this case?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
No
Major Depressive Episode (not needed if manic) No
Functional Impairment Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s Yes
Family History of Bipolar Disorder No
Prodrome – isolated manic sx No
Course – episodic, relapsing/remitting Yes
Typical Treatment Response? -
Free of confounding features No – rapid remittance,
Case “I’m so tired of this!”

• 48 yo male• CC: new onset auditory hallucinations of people outside
house, paranoid – checking locks, agitation, insomnia• HPI: Started rapidly 3 days ago; brought to ED by brother,
wife and teenage daughter who note he has never had sxlike this; was recently working as middle school science teacher for last 22 years, assistant coaches school basketball team; recently treated for severe asthma for first time with high-dose prednisone
• Medical hx: severe asthma from childhood, moderate alcohol use, but no hx of use disorder or withdrawal. No prior psychiatric hx.
• Family Hx: cousin with schizophrenia• Exam: Well-groomed male with mild agitation,
restlessness, tremor, exhibiting paranoid thoughts, appears distracted at time, but accepts reassurance from brother, no SI/HI, accepting of help.
• Course: Started on olanzapine 2.5mg for duration of prednisone treatment, then decreased slowly 1 week after prednisone treatment completed, psychotic sx do not recur.
Case: “we’re surrounded”

Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes
Stereotypic Negative Sx No
Functional Impairment Yes
Duration > 6 mo No
Absence of Medical/Substance Cause No
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) No
Family History of psychotic disorder Yes
Prodrome – cognitive, negative sx No
Course – subacute onset, fluc +, stable - No
Typical Treatment Response? No
Absence of other atypical features No
Diagnosis: Psychosis due to Steroid Treatment
Case: “we’re surrounded”
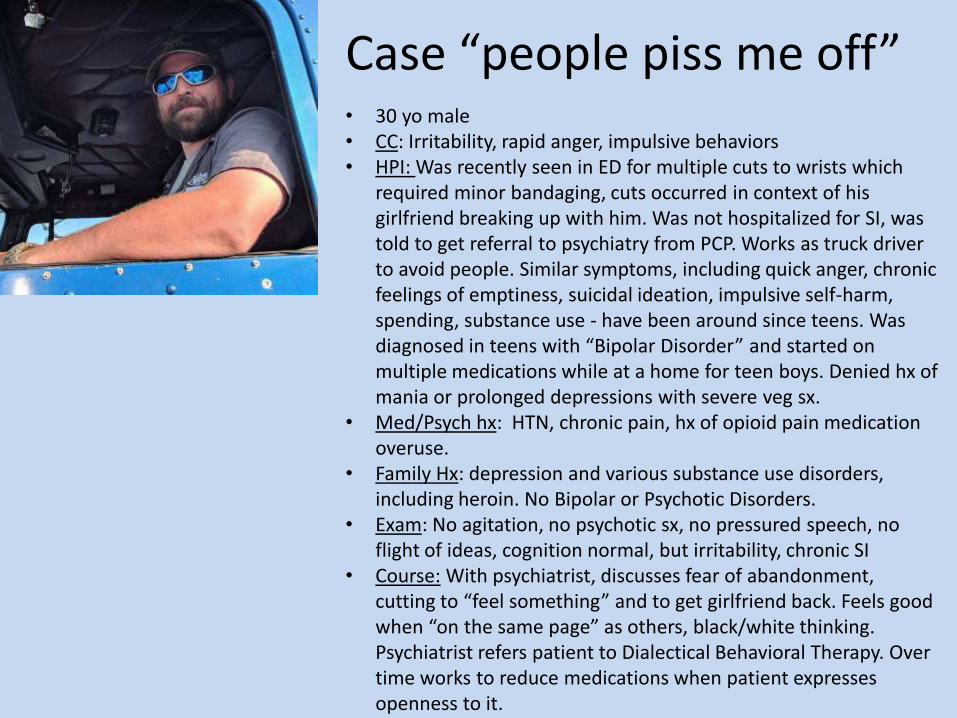
• 30 yo male• CC: Irritability, rapid anger, impulsive behaviors• HPI: Was recently seen in ED for multiple cuts to wrists which
required minor bandaging, cuts occurred in context of his girlfriend breaking up with him. Was not hospitalized for SI, was told to get referral to psychiatry from PCP. Works as truck driver to avoid people. Similar symptoms, including quick anger, chronic feelings of emptiness, suicidal ideation, impulsive self-harm, spending, substance use - have been around since teens. Was diagnosed in teens with “Bipolar Disorder” and started on multiple medications while at a home for teen boys. Denied hx of mania or prolonged depressions with severe veg sx.
• Med/Psych hx: HTN, chronic pain, hx of opioid pain medication overuse.
• Family Hx: depression and various substance use disorders, including heroin. No Bipolar or Psychotic Disorders.
• Exam: No agitation, no psychotic sx, no pressured speech, no flight of ideas, cognition normal, but irritability, chronic SI
• Course: With psychiatrist, discusses fear of abandonment, cutting to “feel something” and to get girlfriend back. Feels good when “on the same page” as others, black/white thinking. Psychiatrist refers patient to Dialectical Behavioral Therapy. Over time works to reduce medications when patient expresses openness to it.
Case “people piss me off”

Diagnosis: Borderline Personality Disorder
Bipolar Disorder Template Present in this case?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
No
Major Depressive Episode (not needed if manic) Yes
Functional Impairment Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s Yes
Family History of Bipolar Disorder No
Prodrome – isolated manic sx No
Course – episodic, relapsing/remitting Yes
Typical Treatment Response? Yes/No
Free of confounding features No: fears of abandonment, sx peak in interpersonal situations, cutting
Case “people piss me off”

• 75 yo female• CC: New onset visual hallucinations, tactile hallucinations,
paranoia that staff are poisoning her; • HPI: Brought to ED by assisted living care staff, for rapid
onset over last 1 week of hallucinations/paranoid delusions; found searching halls for lost dog which she doesn’t have, then locking herself in her room. Is former executive assistant, mother of 3, grandmo of 6, was cooperative 1 week prior
• Med/Psych Hx: osteoporosis, osteoarthritis on low-dose nortriptyline for chronic pain, hypothyroidism, mild neurocognitive disorder. No prior Psych hx.
• Family Psych Hx: none• Exam: fluctuating sensorium and disorientation - she
thought date was 1985 and that the ED physician was her son. At times she would lose track of the conversation or become upset and hit out at staff. Bladder distention, tachycardia.
• Labs: hyponatremia• Course: Was given 0.25mg haldol, and she calmed and
cleared for 6 h, but then disorientation, VH came back.
Case: “they’re putting it in my food.”

Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes
Stereotypic Negative Sx No
Functional Impairment Yes
Duration > 6 mo No
Absence of Medical/Substance Cause No
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) No
Family History of psychotic disorder No
Prodrome – cognitive, negative sx No
Course – subacute onset, fluc +, stable - No
Typical Treatment Response? Yes
Absence of other atypical features No – fluctuating consciousness, VH, disorientation
Diagnosis: Delirium from multiple potential causes
Case: “they’re putting it in my food.”

• 79 yo male• CC: New onset visual hallucinations of children outside
room at assisted living facility where lives with wife• HPI: last 3 weeks has had VH, are distracting, but don’t
strike fear, and have led him to wander outside to look for the children. Also has had severe sleep probs, mild cognitive problems. Worked in healthcare for 40 years, with ~20 years as hospital administrator for single local children’s hospital. Was seen in ED 1 weeks ago where UA showed equivocal UTI, and superimposed delirium was considered, was given haldol once – had severe medication-induced parkinsonism, and flattening.
• Medical hx: Hx hip replacement, no prior psych hx, no alcohol or substance use.
• Fam hx: grandson with Autism, father had Parkinsons, no other mental health disorders.
• Exam: fluctuating vitals, parkinsonism (now off haldol), mild cognitive impairments, fleeting VH.
Case: “can you see them?”

Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes/No
Stereotypic Negative Sx No
Functional Impairment Yes
Duration > 6 mo No
Absence of Medical/Substance Cause ??
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) No
Family History of psychotic disorder No
Prodrome – cognitive, negative sx No
Course – subacute onset, fluc +, stable - No
Typical Treatment Response? No
Absence of other atypical features No - VH only, fluct vitals, sleep probs, Parkinsonism
Diagnosis: Lewy-Body Dementia
Case: “can you see them?”

• 15 yo male• CC: Anger, Agitation, Poor Sleep, Impulsive behaviors. Brought to
PCP by parents for worry about risky behaviors.• HPI: Recently got caught for stealing a neighbors car and going
for a joyride with a friend in the middle of the night on a weeknight. Has court date coming up. Father notes he is “up at all hours”, “can’t finish anything at school or home” and “won’t listen to anything we say”. With father in room, sulks with arms folded, doesn’t speak. With father gone talks about hating school, not knowing if its worth continuing to go, he doesn’t feel good about himself there, just wishing he could leave home or die, but doesn’t have active SI. He says he gets to sleep at 1-2am most nights because it is hard to shut his body down, barely wakes in time for school at 7am feeling exhausted, and on weekends sleeps until noon. Chronically impulsive, attention problems, no grandiosity, likes to sleep, no psychosis.
• Med/Psych Hx: ADHD since age 8, multiple broken bones; Has tried many substances, but nothing repeatedly.
• Social hx: High school sophomore in IEP for ADHD, performing poorly, and missing classes. Enjoys skateboarding and rock climbing. Has girlfriend and multiple friends.
• Family Hx: ADHD• Exam: phys exam normal, mental status exam: exhibits mild
hyperactivity, overtalks at times, but shows no severe agitation, no flight of ideas or loose associations, no psychosis sx. UDS neg.
Case “I get bored”

Diagnosis: ADHD +/- Oppositional Defiant/conduct DO and Substance Use Disorder
Bipolar Disorder Template Present in this case?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
No
Major Depressive Episode (not needed if manic) No
Functional Impairment Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s No - before
Family History of Bipolar Disorder No
Prodrome – isolated manic sx No
Course – episodic, relapsing/remitting No
Typical Treatment Response? -
Free of confounding features No: chronic hyperactivity, impulsivity, not decreased need for sleep
Case “I get bored”

• 17 yo female• CC: Auditory hallucinations, paranoia, possible seizure, mutism• HPI: last 2 weeks experienced fairly fast onset of above sx.
Brought to parents who are very concerned because this was a very sudden change for her, and she has never had such symptoms prior, has had to stay home from school. She is an A student and vice president of her class at high school, who recently helped lead organization of the high school dance.
• Past Medical Hx: No medical problems, had tried cannabis once in last month
• Family Hx: Schizoaffective Disorder and Borderline Personality Disorder
• Exam: patient had some insight to abnormality of thinking, some attention-problems, headache, autonomic instability, odd posturing, periods of mutism, fluctuating paranoia and hallucinations. Mother sat with her to calm her.
• Course: Low dose olanzapine given, but did not help much. Head MRI showed mesiotemporal hyperintensities, EEG showed generalized slowing, LP showed oligoclonal bands, and ovarian teratoma discovered. Removal of ovarian teratoma and immunosuppression led to symptom remission.
Case: “tell them to stop shouting at me”

Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes
Stereotypic Negative Sx No
Functional Impairment Yes
Duration > 6 mo No
Absence of Medical/Substance Cause No
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) Yes
Family History of psychotic disorder Yes
Prodrome – cognitive, negative sx No
Course – subacute onset, fluc +, stable - No
Typical Treatment Response? No
Absence of other atypical features No – some insight, headache, autonomic instability, MRI findings
Diagnosis: Anti-NMDA receptor encephalitis
Case: “tell them to stop shouting at me”

• 37 yo female• CC: Rapid onset over a week of agitation, mood irritability and
lability, increased energy, decreased ability to sleep, “because I can’t stop my brain”, rapid speech, agitation.
• HPI: Had some recent viral infection, was just getting over it, when she began to feel less herself, have harder time sleeping, more moody, difficulty controlling thoughts and attention, lost track of what she was doing several times during the day.
• Med/Psych Hx: Depression stable on escitalopram for many years. No other problems. Not pregnant.
• Social hx: Works in mayor’s office on regional planning team. • Family Hx: Depression• Physical exam: double vision, mild ataxia• Mental Status Exam: well-groomed female appearing stated age,
mild agitation, but not requiring redirection, no tremor, speech mildly pressured, some challenges with attention, seems to lose track of course of conversation, memory poor for short term, but can remember things from a few weeks ago, problem finding words at times, mood/affect labile and irritable, insight fair to “something being wrong”, judgment fair.
• Course: Received Olanzapine 2.5mg which helped her sleep and improved mood. Referred for urgent MRI brain, which showed a few scattered T2 white matter hyperintensities. Referred to neurology.
Case “I don’t know what’s happening to me”

Diagnosis: Bipolar Disorder due to Multiple Sclerosis
Bipolar Disorder Template Present in this case?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
Yes
Major Depressive Episode (not needed if manic) Yes
Functional Impairment Yes
Absence of Medical/Substance Cause ??
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s No
Family History of Bipolar Disorder No
Prodrome – isolated manic sx No
Course – episodic, relapsing/remitting No
Typical Treatment Response? Yes
Free of confounding features? No: Sudden onset outside typical years, with MRI hyperintensities
Case “I don’t know what’s happening to me”

• 17 yo female• CC: Referred to Psychiatry for bizarre thoughts• HPI: Over course of last year has begun to voice that she feels
she is directing the actions of a K-pop band from afar, and they communicate to each other through a special “radio-force-channel” that others do not experience.
• Collateral: parents note she has become more isolative, spends much of her time drawing pictures of K-pop stars and collating memorabilia, and school engagement and performance has declined over last year, does not complete much school work. Denies significant mood sx or clear hallucinations. Reported delusion does not go away, but intensity fluctuates.
• Past Med Hx/Psych Hx: no medical conditions, has been diagnosed with cognitive processing disorder, on IEP in school for last 3 years.
• Family Hx: unknown, patient adopted at age 12 months• Exam/Labs: normal• Mental Status Exam: Speech normal, thought content
+delusions, thought process mildly slowed, cognition mild attention probs, orientation good, memory fair, affect is flat, insight poor to delusional process, judgment fair to care.
• Course: Referred to Early Assessment and Support Alliance, started in activities, and started on Asenapine 5mg twice daily, responds well.
Case “We’re connected”

Diagnosis: Schizophrenia
Schizophrenia Template Present in this case?
DSM5
Stereotypic Positive Sx Yes
Stereotypic Negative Sx Yes
Functional Impairment Yes
Duration > 6 mo Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Schiz
Age of onset during teens-20s (or ~40s if F) Yes
Family History of psychotic disorder unknown
Prodrome – cognitive, negative sx Yes
Course – subacute onset, fluc +, stable - Yes
Typical Treatment Response? Yes
Absence of other atypical features Yes
Case “We’re connected”

• 23 yo female• CC: Brought to ED by police• HPI: Very little history, she is speaking rapidly, has difficulty
sitting down at times, writes copious notes on every piece of paper she is given, disrobes and lays on the ground of her room repeating “Om” on repeat for over an hour, is irritable when others try to ask her to stop. While in ED, does not sleep.
• Police match to missing persons report, calls point of contact, mother, who notes: • Patient went missing a week prior after displaying some
bizarre behaviors at her academic lab job. • Police had contacted her lab PI who noted increasingly
pressured speech, some bizarre associations and ideas about the research, and attending work disheveled, and a few times in the same clothes she wore the previous day. He said this was very uncharacteristic of her, and denied any known in-lab toxic exposures.
• Exam: phys exam and labs are normal, UDS negative. • Family Hx: father has Bipolar Disorder w/ mult hospitalizations.• Course: She is admitted and started on olanzapine 20mg at
bedtime, eventually started on lithium. Her mood normalizes over 10 days. Transfers to intensive outpatient program for 3 weeks. Back to work part time after 2 montha.
Case “Ommmmm”
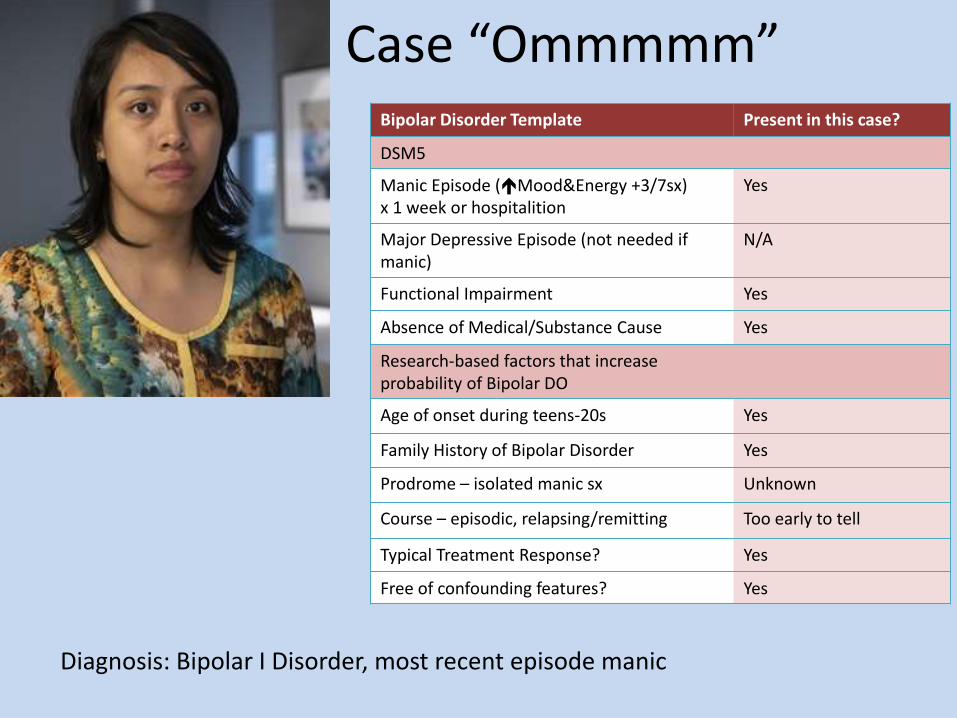
Diagnosis: Bipolar I Disorder, most recent episode manic
Bipolar Disorder Template Present in this case?
DSM5
Manic Episode (Mood&Energy +3/7sx) x 1 week or hospitalition
Yes
Major Depressive Episode (not needed if manic)
N/A
Functional Impairment Yes
Absence of Medical/Substance Cause Yes
Research-based factors that increase probability of Bipolar DO
Age of onset during teens-20s Yes
Family History of Bipolar Disorder Yes
Prodrome – isolated manic sx Unknown
Course – episodic, relapsing/remitting Too early to tell
Typical Treatment Response? Yes
Free of confounding features? Yes
Case “Ommmmm”

Treatments – Schizophrenia Am Fam Physician. 2014;90(11):775-782

AntipsychoticMedications
• Most of effect comes from effect at Dopamine Receptor 2 (D2)– Some medications very potent – haldol
– Some less potent – quetiapine
– A few have very minimal effects at D2 – clozapine
• effective when the levels occupy approximately 70% of D2 receptors.
• Persons with schizophrenia vary in response to antipsychotics:– 10-30% of pts with schiz get no benefit
– up to 30% may get partial benefit
– 50%+ get strong positive response
• In patients with schizophrenia recommendation is to continue antipsychotic treatment life long. – 4-30% of patients with schizophrenia will have another during their
lifetime – and no way to predict who will or won’t.
– In studies of continuation, 64% of patients randomized to placebo had relapse within 1 year, 23% of patients randomized to continuation of antipsychotic had relapse with 1 year.
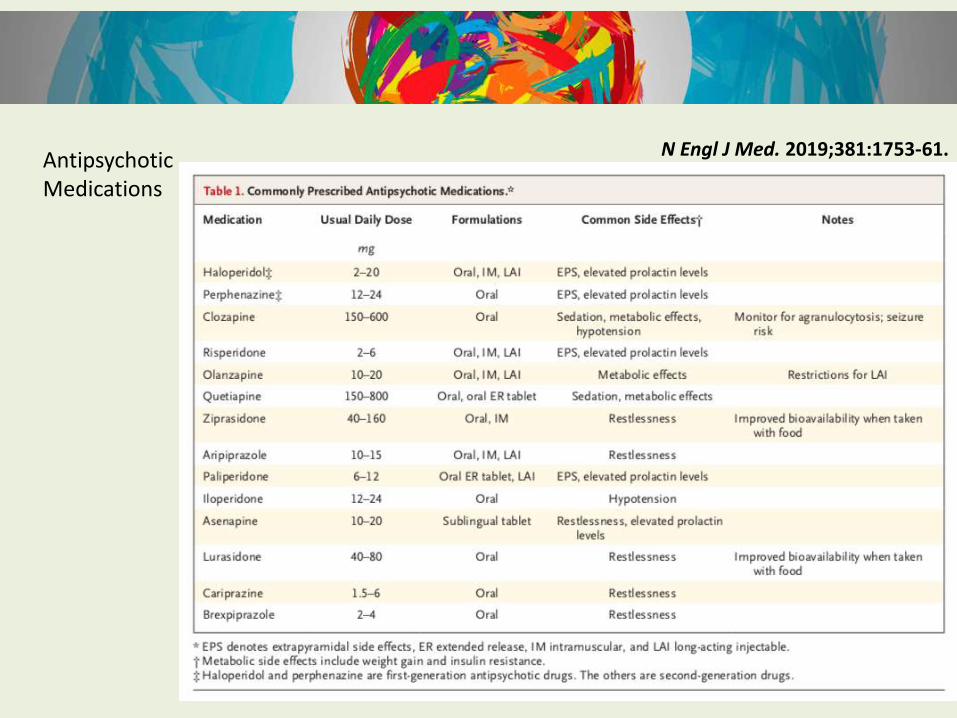
AntipsychoticMedications
N Engl J Med. 2019;381:1753-61.
AntipsychoticMedications
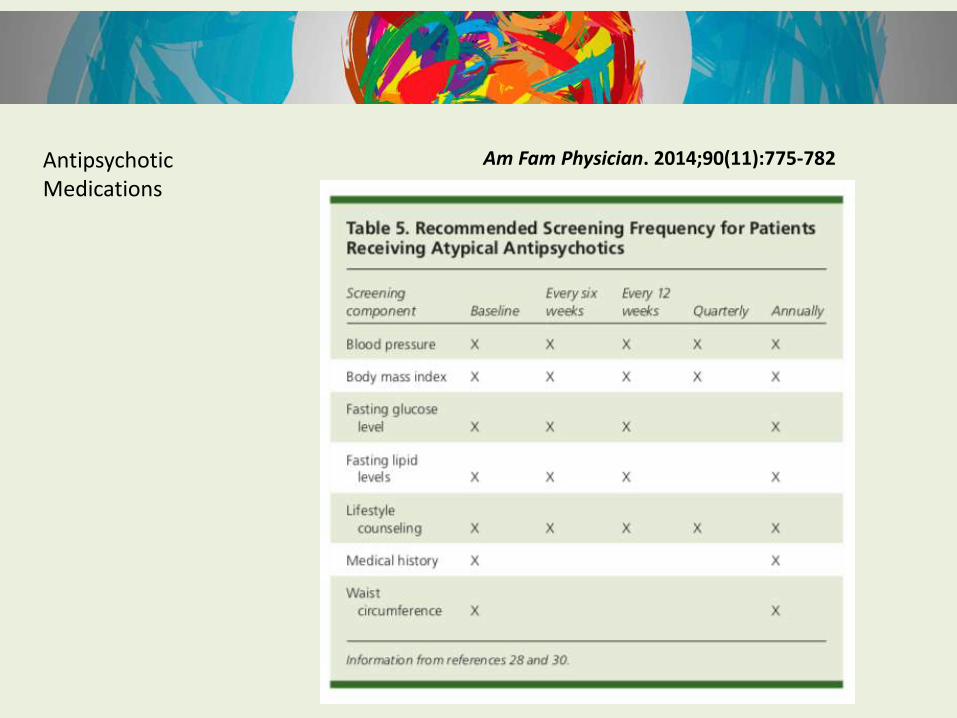
Am Fam Physician. 2014;90(11):775-782

Treatments – Bipolar Disorder Am Fam Physician. 2014;90(11):775-782

Medications to treat Bipolar Disorder Lancet 2016; 387: 1561–72

ExtrasMedical Causes of psychosis

ExtrasMedical Causes of psychosis
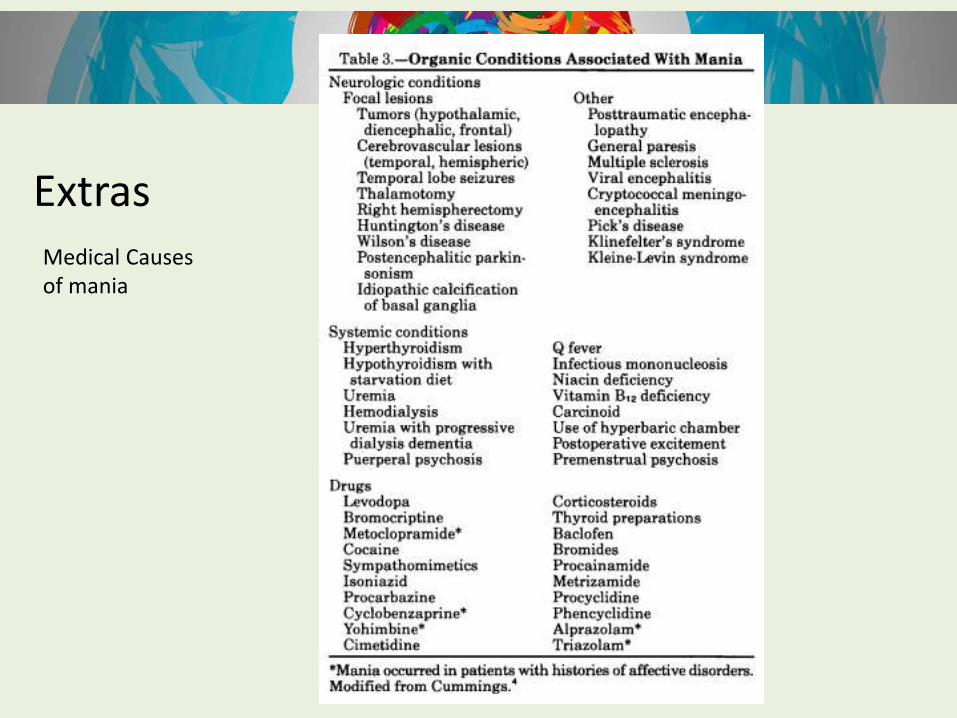
Medical Causes of mania
Extras

N Engl J Med. 2019;381:1753-61.
Am Fam Physician. 2014;90(11):775-782
Lancet. 2016; 388: 86–97
Am Fam Physician. 2014;90(11):775-782
Lancet 2016; 387: 1561–72
N Engl J Med. 2004; 351:476-486.

Bipolar Disorders.
2018; 20 (2):97-170.
Schizophrenia Bulletin. 2010; 36 (1) pp 94-103





























