Embed Size (px)
Citation preview

Pergamon
J Behuv. Thu. & Exp. P.qchia. Vol. 24, No. 3. pp. 219-225.1993. El,evier Saence Ltd
Printed I” Great Bnrain OOOS-7916193 $6 00 + 0.00
IDENTIFYING STAFF ADVOCATES OF BEHAVIORAL TREATMENT INNOVATIONS IN STATE PSYCHIATRIC HOSPITALS
PATRICK W. CORRIGAN, E. PAUL HOLMES and DANIEL LUCHINS
University of Chicago Center for Psychiatric Rehabilitation
Summary - Identification of advocates of behavioral innovation from the ranks of line-level clinical staff has been suggested as a means to implement these innovations in real-world settings. Peer nomination strategies that have been used in management research were adopted for this study so that nursing, professional, and administrative staff at a state hospital could nominate behavioral program advocates from their ranks. Subjects also completed measures that assessed knowledge of behavior therapy and perceptions of barriers to implementing interventions. Results showed that more than 90% of the sample nominated advocates. Tests that sought differences between advocates and nonadvocates showed the two groups to be similar demographically, but the former group was more likely to come from the ranks of professionals and administrators, was significantly more knowledgeable about behavior therapy, and perceived significantly fewer barriers to implementation. These results may help program administrators identify staff members who will
The symptoms, social functioning, and quality of life of severely mentally ill patients have been shown to improve significantly when these patients participate in behavioral programs. Social skills training (Bellack, Hersen, & Turner, 1976; Hogarty et al., 1991; Liberman, Wallace, & Mueser, 1986), token economies (Ayllon & Azrin, 1968; Paul & Lentz, 1977), and behavior family management (Anderson, Reiss, & Hogarty, 1985; Falloon, Boyd & McGill, 1984) have repeatedly been demonstrated to be effective with this population. Unfortunately, several barriers unrelated to the interventions themselves may impede their implementation in inpatient settings. Empowering advocates from the ranks of line- level staff to shepherd on-unit program development and implementation is one way in which these barriers can be overcome. The construct of advocates of behavioral programming will be examined in this study.
To identify barriers to behavioral programs, Emerson and Emerson (1987) surveyed 107 staff members at a large psychiatric hospital regarding
their perceptions of impediments to setting up innovative programs. A content analysis of their results uncovered 18 barriers which they organized into four groups: lack of sufficient human resources, competing contingencies operating on client’s responses, lack of collegial support, and environmental factors such as ward overcrowding that interfere with implementing specific contingencies. In an attempt to expand on these findings, Corrigan and colleagues (1992) surveyed 332 staff members at a state hospital in Southern California. A factor analysis of their responses uncovered five factors that reflected staff perceptions of barriers to implementing behavioral strategies: institutional constraints (administrators do not supply sufficient resources to support programs and bog down clinical work with bureaucratic tasks), insufficient collegial support (professional peers do not sustain innovations), philosophical opposition (behavioral interventions are called inappropriate or unethical with this population), patient dissatisfaction (patients do not like behavioral treatments and
Requests for reprints should be addressed to Patrick Corrigan, University of Chicago Center for Psychiatric Rehabilitation, 7230 Arbor Drive, Tinley Park, IL 60477, U.S.A.
219

220 PATRICK W. CORRIGAN, E. PAUL HOLMES and DANIEL LUCHINS
hence will not comply), and collateral interference (family and friends disrupt behavioral treatments). Endorsement of these factors was found to be associated with staff members’ knowledge of behavioral interventions and their level of job- related stress.
Several strategies may diminish these barriers, including education of administrative and clinical staff regarding behavioral treatments (Eckman et al., 1990; Rogers et al., 1986; Wallace et al., 1992), packaging behavioral innovations in user- friendly formats (Anthony, Cohen, & Pierce, 1980; Liberman & Corrigan, in press), and, of particular interest in this study, identifying advocates from the ranks of unit staff who will assume responsibility for maintaining clinical innovations on that unit (Blair & Wallace, 1989; Corrigan, MacKain, & Liberman, in press; MacKain & Wallace, 1989). Advocates tend to be knowledgeable clinicians who have the energy and abilities to manage colleagues in setting up treatment programs. These qualities may help diminish program barriers by improving staff satisfaction with work and knowledge about behavioral interventions.
advocates from the ranks of line-level staff working in a state hospital. Differences between advocates and nonadvocates will be investigated here in terms of their perceptions of behavioral innovations. Given the definition of technological leaders described by Howell and Higgins, advocates are expected to be more knowledgeable about behavioral treatments and less likely to perceive barriers to their implementation.
Methods
Subjects
Although the construct of advocate seems to make sense organizationally, little research has been completed on the issue in mental health. Advocates and leadership, however, have been the focus of extensive study in management and business (Achilladelis, Jervis, & Robertson, 1971; Burgelman, 1983; Gailbraith, 1982; Delbecq & Mills, 1985; Phillips & Lord, 1986). For example, personality characteristics and qualities of leadership that describe advocates of industrial innovations were examined in a recent study (Howell & Higgins, 1990). These investigators used a peer assessment method where employees were instructed to nominate colleagues from their ranks that had the qualities of advocates. Results showed that nominated advocates exhibited higher risk taking and a leadership style characterized as socially bold, inspiring, and charismatic.
All nursing, professional, and administrative staff of the Extended Care Units (ECU) at a 355 bed State of Illinois Hospital were invited to participate in this study. Fifty-one staff members completed test batteries, of which 47 were useable. The useable group represented 82.5% of the ECU day shift. The ECU sample had several qualities that commended it for this study. The ECU is a relatively closed organization in the larger state hospital; although part time replacements may float on the unit, staff, for the most part, fulfilled the majority of their responsibilities there. ECU staff members have worked at the hospital for some time; mean tenure was 15.3 years (SD = 7.3).
Measures
Subjects who agreed to participate in the study completed a battery of pencil-and-paper measures during one 90-minute test session. The battery included demographic questions, mean length of ECU employment, unit assignment, and job title. Subjects completed three additional measures during this period: Nominations for Clinical Leaders, Behavior Vignettes Test, and Barriers to Implementation of Behavioral Therapy.
Howell and Higgins’ study serves as a Nominations for Clinical Leaders (NCL). The prototype for investigation of advocates in other peer nomination strategy used in Howell and fields. Their peer nomination strategy was adopted Higgins (1990) was adopted for this study to for this study to identify a subgroup of behavioral produce the NCL. Peer nomination is not

Advocates of Behavioral Innovation 221
confounded by self-halo effects common to self- report measures (Phillips & Lord, 1986). Rather, peer nomination strategies are particularly useful because they represent collegial opinions about the leadership merit of fellow line-level staff, an important quality in actual leaders. The NCL comprised eight open-ended items; four that reflected behaviors characteristic of unit leaders (e.g., “Who on your unit would you say is most likely to inspire other staff to learn new treatment ideas?‘) and four that reflected spoiler qualities, behaviors that tend to undermine program development and implementation (e.g., “Who on your unit would you say has few clinical skills. This person is frequently overwhelmed by patients and has few ideas for good treatment?“). Items were taken from a larger pool of behaviors and qualities independently generated by two experts in psychiatric rehabilitation. Subjects completing the NCL were instructed to write down names of staff members from their unit who met leadership qualities described in each NCL item.
Despite their benefits, peer nominations methods may be confounded by subtle organizational pressures that result in under- reporting advocates (Kane & Lawler, 1978; Love, 1981). Several strategies were employed to diminish these pressures. The measure was administered by a research assistant not affiliated with the state hospital who assured subjects that all information would be confidential and not available to state administrators. Subjects were explicitly told not to restrict choices to unit supervisors or shift leads. Subjects were encouraged not to leave any item blank; if they believed no peer met the item description, they were supposed to write “no one”. The impact of these pressures was assessed by determining the percent of staff members who completed the NCL.
Behavior Vignettes Test (BVT). Subjects read 20 clinical problems and chose the correct intervention from four multiple choice options (Heifetz et al., 1981). This test has been used extensively to assess staff familiarity with clinical strategies related to operant conditioning and has
been shown to have good internal consistency and test-retest reliability.
Barriers to the Implementation of Behavior Therapy (BZBT). The BIBT comprises 18 statements about barriers to introducing behavioral innovations at the subject’s mental health setting (Corrigan, Kwartarini, & Pramana, 1992). The statements are rated on a six point Likert scale of agreement from 1 (strongly agree) to 6 (strongly disagree). Factor analysis identified five factors - institutional constraints, insufficient collegial support, philosophical opposition, patient dissatisfaction, and collateral interference - which have good internal consistency and test-retest reliability.
Results
The sample was 50% female with an average age of 45.2 years (SD = 8.6). Thirty percent of the sample was single, 51.3% was married, and 17.9% was widowed or separated. On average, subjects had completed 15.7 years of education (SD = 2.7). The staff was 41.7% African-American, 33.3% Caucasian, 16.7% Latino, and 8.3% Asian. Jobs were grouped into three categories for analyses in this paper: (1) nursing, which included psychological technicians and licensed/registered nurses; (2) professional staff including psychiatrists, other physicians, psychologists, social workers, and activity therapists; and (3) administrators or unit chiefs. The sample comprised 41.5% nurses, 49.0% professionals, and 9.5% administrators.
Staff Participation in the NCL
To determine whether subtle pressures affected subject responses on the NCL, staff participation on this measure was examined. Ninety-one percent of the sample either nominated someone from the hospital staff as advocate (N = 39) or explicitly stated that none of their peers would be good advocates (N = 4). The remaining 9% did not respond to the measure. We hypothesized that

222 PATRICK W. CORRIGAN, E. PAUL HOLMES and DANIEL LUCHINS
fewer NCL nominations might result from organizational pressures perceived by line-level staff. This was supported by a significant correlation between perceived institutional constraints on the BIBT and number of advocates reported on the peer nomination measure (r = 0.40, p < .01). In addition, results of tests discriminating staff members who made nominations from those who did not found the former group was better educated (I = 2.10, p < .05) and more likely to be professionals or administrators (x? = 6.05, p < .05); these staff members are likely to experience organizational pressures less forcefully. No other significant differences in age, gender, marital status, or ethnicity were found across groups.
Internal consistency of the NCL was determined in terms of number of advocates or spoilers nominated for each item. Cronbach’s alpha for advocates or spoilers was 0.82 and 0.83, respectively.
Churucteristics of Advocates und Nonadvocates
Identification of differences between advocate and nonadvocate groups may depend on the number of nominations set as criterion for defining each group. If a liberal criterion is used (e.g., the subject is an advocate if he or she received two or more leadership nominations from peers and no nominations as spoiler), then size of the nomination sample is relatively large (which increases the power of statistical tests), but the likelihood of false positives is also increased. Conversely, if a more conservative criterion is adopted (e.g., advocate nominations 2 4 and spoiler nominations = 0). a group of “super” advocates with few false positives is identified, but the power of the analyses is diminished. To address this difficulty, both criteria were used in the study with findings from the two analyses reported here. Seventeen staff members were nominated as advocates using the less conservative criterion; this represented 3 1.5% of staff members working the day time shift. Five individuals were nominated as super advocates (9% of the day shift).
The demographic profile of advocates, nonadvocates, and super advocates is summarized in Table 1. Comparisons of advocates and nonadvocates showed that the two groups were similar in age, gender, ethnicity, and years of education. However, advocates were married at a significantly greater rate than nonadvocates (x? = 5.68, p < .05). Of more interest, professionals and administrators were nominated as advocates at a greater rate than nursing staff (% = 7.30, p < .05). Similar patterns were found when comparing nonadvocates to super advocates; no differences in age, gender, ethnicity, and years of education. Super advocates were all married and came from the ranks of professional staff members.
Differences in knowledge about behavior therapy and perceived barriers to implementing behavioral innovations among advocates, nonadvocates, and super advocates are also summarized in Table 1. Results showed that advocates, compared to nonadvocates, reported significantly fewer barriers to implementing behavioral interventions. Specifically, they perceived institutional constraints (t = 2.94, p < .005) and philosophical opposition (t = 2.39, p < .05) to be less an impediment than their peers. Nonsignificant trends were found for patient dissatisfaction (t = 1.72, p < . IO). Using BIBT norms, three out of five of the average BIBT scale scores for nonadvocates are in the high range and represent staff perceptions of significant programmatic barriers (Corrigan, Kwartarini, & Pramana, 1992). None of the advocates scale scores are in the significant barrier range.
Advocates also had significantly greater knowledge of behavioral principles as measured on the BVT (t = 3.29, p < .005). Despite this difference, the average score on the BVT for advocates represented only 45% of items identified correctly. Finally, advocates seemed to be either better able to identify peers who exhibited leadership qualities or more willing to nominate these peers than nonadvocates. They reported significantly more advocates (t = 2.73, p < .OI).
Similar patterns were seen when comparing nonadvocates to super advocates; in some
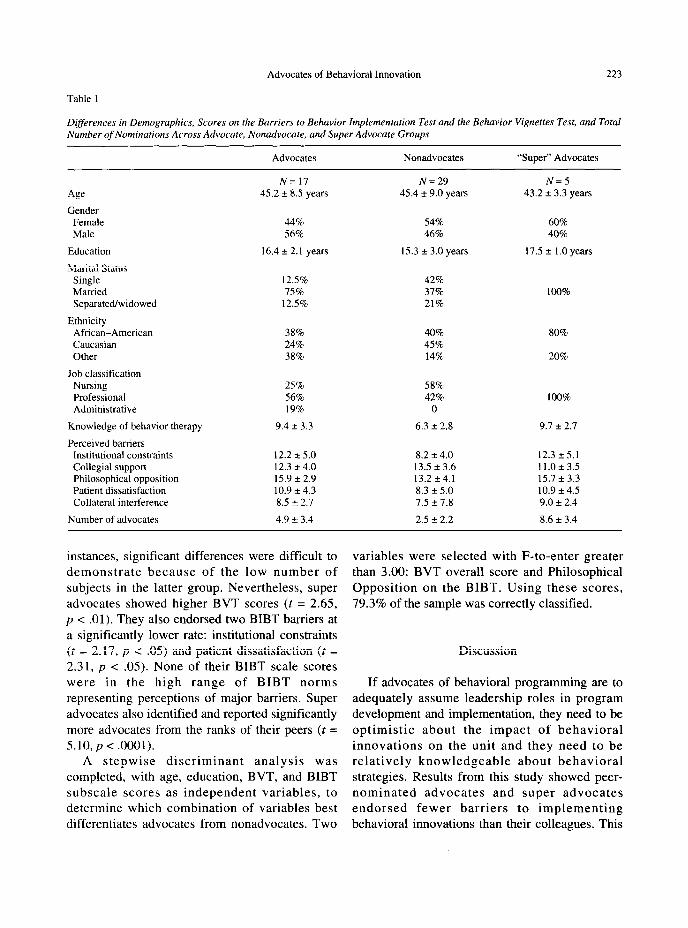
Table 1
Advocates of Behavioral Innovation 223
Differences in Demographics, Scores on the Barriers to Behavior Implementation Test and the Behavior Vignettes Test, and Total Number of Nominations Across Advocate, Nonadvocate, and Super Advocate Groups
Age
Gender Female Male
Education
Marital Status Single Married Separated/widowed
Ethnicity African-American Caucasian Other
Job classification Nursing Professional Administrative
Knowledge of behavior therapy
Perceived barriers Institutional constraints Collegial support Philosophical opposition Patient dissatisfaction Collateral interference
Number of advocates
Advocates
N= 17 45.2 + 8.5 years
44% 56%
16.4 f 2.1 years
12.5% 75%
12.5%
38% 24% 38%
25% 56% 19%
9.4 + 3.3
12.2 It 5.0 12.3 + 4.0 15.9 + 2.9 10.9 + 4.3 8.5 2 2.7
4.9 + 3.4
Nonadvocates
N=29 45.4 f 9.0 years
54% 46%
15.3 + 3.0 years
42% 37% 21%
40% 45% 14%
58% 42%
0
6.3 + 2.8
8.2 + 4.0 13.5 f 3.6 13.2 +4.1 8.3 + 5.0 7.5 + 7.8
2.5 f 2.2
“Super” Advocates
N=5 43.2 + 3.3 years
60% 40%
17.5 + 1.0 years
100%
80%
20%
100%
9.1 f 2.7
12.3 -+ 5.1 11.0 + 3.5 15.7 + 3.3 10.9 + 4.5 9.0 + 2.4
8.6 + 3.4
instances, significant differences were difficult to demonstrate because of the low number of subjects in the latter group. Nevertheless, super advocates showed higher BVT scores (t = 2.65, p < .Ol). They also endorsed two BIBT barriers at a significantly lower rate: institutional constraints (t = 2.17, p < .OS) and patient dissatisfaction (t = 2.31, p < .OS). None of their BIBT scale scores were in the high range of BIBT norms representing perceptions of major barriers. Super advocates also identified and reported significantly more advocates from the ranks of their peers (t = 5.10, p < .OOOl).
A stepwise discriminant analysis was completed, with age, education, BVT, and BIBT subscale scores as independent variables, to determine which combination of variables best differentiates advocates from nonadvocates. Two
variables were selected with F-to-enter greater than 3.00: BVT overall score and Philosophical Opposition on the BIBT. Using these scores, 79.3% of the sample was correctly classified.
Discussion
If advocates of behavioral programming are to adequately assume leadership roles in program development and implementation, they need to be optimistic about the impact of behavioral innovations on the unit and they need to be relatively knowledgeable about behavioral strategies. Results from this study showed peer- nominated advocates and super advocates endorsed fewer barriers to implementing behavioral innovations than their colleagues. This

224 PATRICK W. CORRIGAN. E. PAUL HOLMES and DANIEL LUCHINS
finding suggests that advocates are more likely to foresee ways in which newly developed programs can be maintained in real-world settings. Moreover, advocates and super advocates were relatively more knowledgeable about behavioral treatments. Despite the last difference, however, advocates identified less than half of tests items correctly. Expert consultants may need to be available to provide information to advocates and their colleagues as innovative programs are developed.
In many ways, staff members who were nominated as advocates were similar to their colleagues. No significant differences were found between advocates and nonadvocates in age, gender, ethnicity, or years of education. However, advocates more often came from the ranks of professionals and administrators. This finding challenges democratic notions that any person with sufficient leadership qualities could rise from the ranks to fill the advocate role. Line-level staff seem to be looking towards professionals and administrators to advocate program development.
Findings from the study suggested that subtle organizational pressures did not impede staff participation on the nomination task. Ninety-one percent of participants provided useable responses to the NCL. It was unclear whether the 9% of the sample that chose not to participate were unwilling publicly to identify advocates because they misunderstood task instructions or opposed the self-disclosure required for the task. Future research needs to examine what factors influence staff nominations of program advocates. French and Raven (1960) identified five bases of social power - legitimate, reward, coercive, referent, and expert power - which may explain organizational forces that influence line-level staff decisions. Findings from this study suggest that expert power may be one social base that affects staff nominations: i.e., line-level staff perceive professionals as having rrreded rrlrvant
knowledge to assume the role of advocate. Our results only describe staff perceptions of
who among line-level clinicians might be champions of treatment innovations. Nominated champions possess more programmatic optimism
and relatively more knowledge. However, these findings do not suggest whether identified champions manifest the managerial skills required for the task. Future research must determine whether nominated champions, in fact, can successfully lead their peers into implementing and maintaining new treatment programs.
Acknowledgements - The authors wish to express appreciation to Drs Abdul Basit and Joseph Parks for supporting data collection efforts and to Dr Stanley McCracken for a review of an earlier version of the manuscript.
References
Achilladelis, B.. Jervis, P., & Robertson, A. (1971). A Study of Succ~ess and Failure in Industrial Innovation. Sussex, England: University of Sussex Press.
Anderson, C. M., Reiss, D. _I.. & Hogarty, G. E. (1985). Schizophrenia and the Family. New York: The Guilford Press.
Anthony, W. A., Cohen, M. R., & Pierce, R. M. (1980). Instructor’s Guide to the Psychiatric Rehabilitation Practice Srries. Baltimore: University Park Press.
Ayllon, T., & Azrin, N. (1968). The token economy: a moti\,ational system for therapy and rehabilitation. New York: Appleton-Century-Crofts.
Bellack. A. S., Hersen, M., & Turner, S. M. (1976). Generalization effects of social skills training with chronic schizophrenics: an experimental analysis. Behar’ioral Research and Therapy, 14,391-398.
Blair, K., & Wallace, C. (1989). Evaluation of the dissemination qf the Medication Management Module. Unpublished report available from Camarillo/UCLA Clinical Research Center, P.O. Box 6022, Camarillo, CA 9301 I-6022.
Burgelman, R. A. (1983). A process model of internal corporate venturing in the diversified major firm. Administrative Science Quarter1.y. 28, 223-244.
Corrigan, P. W., Kwartarini, W. Y., & Pramana, W. (1992) Staff perception of barriers to behavior therapy at a psychiatric hospital. Behavior Modijication, 16, 132-144.
Corrigan, P. W., MacKain, S. J., & Liberman, R. P. (in press). Skills training modules: a strategy for dissemination and utilization of a rehabilitation innovation. In J. Rothman, & E. Thomas (Eds.), Intervention research. Chicago: Hawonh Press.
Delbecq, A. L., & Mills, P. K. (1985). Managerial practices that enhance innovation. Organizational D>~namics. 14, 24-34.
Eckman. T. A., Liberman, R. P., Phipps, C. C., & Blair, K. E. Teachin& medication management skills to schizophrenic patients. Journal of Clinical Psychopharmacology (in press).
Emerson, E., & Emerson, C. (1987). Barriers to the effective implementation of habilitative behavioral programs in an institutional setting. Mental Retardation, 25, lOlL106.
Falloon. I. R. H., Boyd, J. L., & McGill, C. W. (1984). Family Care oj’.Schtophrenin. New York: Guilford.

Advocates of Behavioral Innovation 225
French, J. R. P., & Raven, B. (1960). The bases of social power. In D. Cartwright, & A. F. Zandler (Eds.), Group Dynamics (2nd ed.). Evanston, IL: Row Peterson.
Gailbraith, J. R. (1982). Designing the innovating organization. Organizational Dynamics, 10.5-25.
Heifetz, L. J., Baker, B. L., & Pease, L. A. (1981). Behavioral Vignettes Test. Cambridge, MA: Educational Projects.
Hogarty, G. E., Anderson, C. M., Reiss, D. J., et al. (1991). Family psychoeducation, social skills training, and maintenance chemotherapy in the aftercare treatment of schizophrenia. Archives of General Psychiatry, 48.340-347.
Howell, J. M., & Higgins, C. A. (1990). Champions of technological innovation. Administrative Science Quarterly, 35.317-341.
Kane, J. S., & Lawler, E. E. (1978). Methods of peer assessment. Psychological Bulletin, 85.555-586.
Liberman, R. P., & Corrigan, P. W. (in press). Designing new psychosocial treatments for schizophrenia. Psychiatry.
Liberman, R. P., Wallace, C. J., & Mueser, K. T. (1986). Social skills training for schizophrenic individuals at risk for relapse. American Journal of Psychiatry, 143,523-526.
Love, K. G. (1981). Comparison of peer assessment methods:
Reliability, validity, friendship bias, and user reaction. Joumal of Applied Psychology, 66,45 1-457.
MacKain, S. J., & Wallace, C. J. (1989). Adoptions of innovations in mental health. Unpublished report available from Camarillo/UCLA Clinical Research Center, P.O. Box 6022, Camarillo, CA 9301 l-6022.
Paul, G. L., & Lentz, R. J. (1977). Psychosocial Treatment of Chronic Mental Patients: Milieu Versus Social Learning Programs. Cambridge, MA: Harvard University Press.
Phillips, J. S., & Lord, R. G. (1986). Notes on the practical and theoretical consequences of implicit leadership theories for the future of leadership measurement. Journal of Management, 12.3141.
Rogers, E. S., Cohen, B. F., Danley, K. S., Hutchinson, D., & Anthony, W. A. (1986). Training mental health workers in psychiatric rehabilitation. Schizophrenia Bulletin, 12, 709-719.
Wallace, C. J., Liberman, R. P., MacKain, S. J., Blackwell, G., & E&man, T. A. (1992). Effectiveness and replicability of modules for teaching social and instrumental skills to the severely mentally ill. American Journal of Psychiatry, 149, 654-658.





























