Embed Size (px)
Citation preview
PAIN�
xxx (2014) xxx–xxx
w w w . e l s e v i e r . c o m / l o c a t e / p a i n
Identifying treatment responders and predictors of improvement aftercognitive-behavioral therapy for juvenile fibromyalgia
http://dx.doi.org/10.1016/j.pain.2014.03.0050304-3959/� 2014 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
⇑ Corresponding author. Address: Emory University School of Medicine,Children’s Healthcare of Atlanta, Aflac Cancer and Blood Disorders Center, 2015Uppergate Drive, Atlanta, GA 30322, USA. Tel.: +1 (404) 727 2712; fax: +1 (404) 7274455.
E-mail address: [email protected] (S. Sil).
Please cite this article in press as: Sil S et al. Identifying treatment responders and predictors of improvement after cognitive-behavioral therapy fonile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
Soumitri Sil a,⇑, Lesley M. Arnold b, Anne Lynch-Jordan c,d, Tracy V. Ting d,e, James Peugh c,d,Natoshia Cunningham c, Scott W. Powers c,d, Daniel J. Lovell d,e, Philip J. Hashkes f, Murray Passo g,Kenneth N. Schikler h, Susmita Kashikar-Zuck c,d
a Department of Pediatrics, Emory University School of Medicine, Aflac Cancer and Blood Disorders Center, Children’s Healthcare of Atlanta, Atlanta, GA, USAb Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati College of Medicine, Cincinnati, OH, USAc Division of Behavioral Medicine and Clinical Psychology, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USAd Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH, USAe William S. Rowe Division of Rheumatology, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USAf Pediatric Rheumatology Unit, Shaare Zedek Medical Center, Shaare Zedek, Jerusalem, Israelg Division of Rheumatology and Immunology, Medical University of South Carolina, Charleston, SC, USAh Division of Pediatric Rheumatology, University of Louisville School of Medicine, Louisville, KY, USA
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
a r t i c l e i n f o
Article history:Received 29 July 2013Received in revised form 20 February 2014Accepted 6 March 2014Available online xxxx
Keywords:Clinically meaningful changeClinical significanceCognitive-behavioral therapyTreatment respondersFunctional disabilityPain coping efficacy
a b s t r a c t
The primary objective of this study was to estimate a clinically significant and quantifiable change infunctional disability to identify treatment responders in a clinical trial of cognitive-behavioral therapy(CBT) for youth with juvenile fibromyalgia (JFM). The second objective was to examine whether baselinefunctional disability (Functional Disability Inventory), pain intensity, depressive symptoms (Children’sDepression Inventory), coping self-efficacy (Pain Coping Questionnaire), and parental pain historypredicted treatment response in disability at 6-month follow-up. Participants were 100 adolescents(11–18 years of age) with JFM enrolled in a recently published clinical trial comparing CBT to a fibromy-algia education (FE) intervention. Patients were identified as achieving a clinically significant change indisability (ie, were considered treatment responders) if they achieved both a reliable magnitude ofchange (estimated as a P7.8-point reduction on the FDI) using the Reliable Change Index, and a reductionin FDI disability grade based on established clinical reference points. Using this rigorous standard, 40% ofpatients who received CBT (20 of 50) were identified as treatment responders, compared to 28% whoreceived FE (14 of 50). For CBT, patients with greater initial disability and higher coping efficacy weresignificantly more likely to achieve a clinically significant improvement in functioning. Pain intensity,depressive symptoms, and parent pain history did not significantly predict treatment response.Estimating clinically significant change for outcome measures in behavioral trials sets a high bar but isa potentially valuable approach to improve the quality of clinical trials, to enhance interpretability oftreatment effects, and to challenge researchers to develop more potent and tailored interventions.
� 2014 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
1. Introduction of improvement in disability over 6 months for adolescents with
Cognitive-behavioral therapy (CBT) is an effective treatment forpediatric chronic pain conditions that significantly reduces func-tional disability [11,35], with 1 study demonstrating maintenance
juvenile fibromyalgia (JFM) [26]. Even with large and statisticallysignificant overall treatment effects reported in clinical trials, thereis variability in outcomes for individual patients, and not all pa-tients achieve functional improvements that are clinically mean-ingful [13]. Clinically meaningful or significant improvements areconsidered worthwhile to patients and involve a noticeable reduc-tion in symptomatology [2,7,18]. To distinguish patients whoachieve clinically significant improvements from those who donot, it is important to determine cut-off scores for outcome mea-sures that represent clinically meaningful change. Such empirically
r juve-

2 S. Sil et al. / PAIN�
xxx (2014) xxx–xxx
derived scores have the potential to significantly improve theinterpretability of treatment effects across trials and to providevaluable information to clinicians who are seeking evidence to in-form their practice [2,9,32,48].
Functional disability, as measured by the Functional DisabilityInventory (FDI) [47], is a key outcome measure in trials of behav-ioral interventions for pediatric chronic pain [30]. Although pub-lished clinical reference points have been established for the FDI[21], there are no clear established guidelines for determiningwhether statistically significant changes in the FDI are of clinicalsignificance in randomized controlled trials. Unfortunately, theprocess of determining clinical significance remains a challenge,particularly among functional health outcomes (eg, the FDI)[5,16] because of varying methods of defining clinical significance[16,48]. Estimating clinically meaningful differences has gainedsupport as a new standard for determining clinical significance oftreatment effectiveness [1,7,9,41]. Thus, estimating clinically sig-nificant changes of functional disability after treatment can be ahelpful tool for use in identifying patients who respond to treat-ment and examining patient characteristics that predict treatmentresponse.
A few studies in adults have identified patient characteristicsthat may predict positive response to treatment. In CBT studiesof adults with chronic pain, predictors of positive treatment re-sponse included older age, higher levels of distress, depression,or disability, greater coping efficacy, and less solicitous spousebehaviors at baseline [3,43–45]. In children with chronic pain, par-ents play an integral role in the management of pain and function-ing. Specifically, family history of chronic pain may be anadditional factor to consider, given its known association with pa-tients’ greater disability [29,39,40]. To date, little is known aboutpredictors of treatment success in pediatric chronic pain.
In the current study, secondary analyses of data from our pub-lished randomized controlled trial of CBT for JFM [26] were used asan exemplar to begin the process of evaluating clinical significancefor the FDI (the primary outcome) in pediatric trials of chronicpain. The study objectives were as follows: to estimate clinicallysignificant changes in functional disability to identify treatmentresponders versus nonresponders; and to test whether patientcharacteristics at baseline (functional disability, pain intensity,depressive symptoms, coping efficacy, parent pain history) wouldpredict clinically significant treatment response in functionaldisability.
2. Methods
2.1. Patients
Participants were 100 children and adolescents aged 11 to18 years with JFM, recruited from 4 pediatric rheumatology cen-ters, who had completed a randomized clinical trial comparingCBT to an educational intervention (fibromyalgia education [FE])[26]. Children and adolescents were eligible to participate if theymet the following inclusion criteria: met the Yunus and Masi[49] JFM classification; 2) had been on stable medications for8 weeks; 3) reported average pain intensity P4 on a visual ana-logue scale of 0 to 10 cm based on 1 week of daily pain diaries;and reported at least mild disruption in daily activities becauseof JFM symptoms (ie, score >7 on the FDI). Exclusion criteria in-cluded the following: diagnosis of any other chronic rheumatic dis-ease; documented developmental delay; current symptoms ofbipolar disorder, major depressive disorder, panic disorder, or psy-chosis; or active use of opioid medications.
Institutional review board approval was obtained at each site.Parents of the participants provided written informed consent,and children and adolescents provided written assent.
Please cite this article in press as: Sil S et al. Identifying treatment responders anile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
2.2. Study procedures
After completing a comprehensive medical and psychosocialbaseline assessment that included a battery of questionnaires, eli-gible participants were randomized to receive either CBT or FE. Ineach treatment arm, participants met individually with a trained,doctoral-level therapist for 8 weekly treatment sessions in whichthe interventions were delivered using manualized protocols.CBT focused on training in active and adaptive behavioral and cog-nitive coping strategies in pain management. FE was designed toprovide educational information about fibromyalgia, its treatment,and healthy lifestyle habits with no active training or instructionfor behavior change. Sessions were well attended and the studyhad a high retention rate (88%) without any differential drop-outin the 2 treatment arms. The trial results published by Kashikar-Zuck [26] provides further details on the study treatments, studyprocedure, and primary outcomes.
2.3. Measures
The following measures were administered as part of the com-prehensive baseline assessment. Functional disability, pain inten-sity, depressive symptoms, coping self-efficacy, and parent painhistory were selected for the analyses based on evidence of theirprediction of treatment response in studies of adults with variouschronic pain conditions. Additional factors of potential interest (eg,age, medication use, duration since pain onset) were considered,but were not included in the analyses because of inconsistent pre-dictive value based on the adult pain literature as well as limitedstatistical power [3,43–45].
2.3.1. Functional disability—primary outcomeThe FDI is a well-validated, 15-item self-report instrument that
assesses children’s and adolescents’ perceived difficulty in per-forming daily activities because of their pain symptoms in home,school, recreational, and social settings [47]. This measure wasthe primary outcome used in our trial, defined as change in FDIfrom baseline to end of study (6-month follow-up), and was usedto assess clinically significant changes in functional disability out-comes in this secondary analysis [26]. Baseline FDI scores also wereused as a predictor of achieving clinically significant changes infunctioning. Participants rated how much difficulty they have per-forming each of the activities on a 5-point Likert scale (0 = no trou-ble to 4 = impossible). Total scores on the FDI ranged from 0 to 60,with higher scores indicating greater disability. For children withchronic pain, the clinical reference points include the following:0 to 12 = no/minimal disability, 13 to 29 = moderate disability,and 30 to 60 = severe disability. These clinical cut-offs were basedon a published study of the validity of the FDI in a large (n = 1300)multicenter clinical sample of youth with chronic pain [21]. TheFDI has been found to have high internal consistency, moderateto high test–retest reliability, moderate cross-informant (parent–child) reliability, and good predictive validity [4,47].
2.3.2. Average pain intensityParticipants rated their average pain intensity on a 0- to 10-cm
visual analog scale (0 ‘‘No pain’’ to 10 ‘‘Pain as bad as you can imag-ine’’) daily for 1 week. Average ratings were calculated for 1 weekat baseline and used for analyses.
2.3.3. Depressive symptomsThe Children’s Depression Inventory (CDI) is a 27-item self-
report measure used to assess baseline levels of depressive symp-toms. It has been well validated for use in children and adolescents[27]. The CDI has strong psychometric properties and is frequentlyused in pediatric pain research [6,10,22]. Participants select 1 of 3
nd predictors of improvement after cognitive-behavioral therapy for juve-

S. Sil et al. / PAIN�
xxx (2014) xxx–xxx 3
statements for each item, and total scores range from 0 to 54. Inthis study, the total raw score was used as an overall indicator ofseverity of depressive symptoms at baseline.
2.3.4. Coping self-efficacyThe coping efficacy subscale of the Pain Coping Questionnaire
(PCQ) [37] assessed overall pain coping efficacy at baseline, whichis one’s perceived ability to manage and cope with pain. The copingefficacy subscale comprises 3 items (eg, ‘‘When you are hurt or inpain for a few hours or a few days, how often do you think you cando something to change it?’’), and is part of a 39-item self-reportquestionnaire that assesses pain coping strategies in children andadolescents. Scores on the pain coping efficacy items range from1 to 5. A total score was calculated ranging from 3 to 15, such thathigher scores indicate greater initial pain coping efficacy. The PCQhas demonstrated good internal consistency (a = 0.79–0.89) insamples of children and adolescents [37] as well as good content,construct, and concurrent validity [36]. The coping efficacy sub-scale also has been shown to be sensitive to treatment effects ina prior CBT study of adolescents with JFM [24,25].
2.3.5. Parent pain historyThe Parent Pain History Questionnaire assessed parental history
of a variety of pain conditions. Parents indicate whether they haveexperienced 12 pain conditions (eg, fibromyalgia, migraines head-aches, low back pain, shoulder/neck pain) and whether they hadsought medical treatment for each. The total number of pain con-ditions experienced as reported at baseline was used in this studyas an indicator of maternal pain history. Similar parent pain historyquestionnaires have been used in previous studies of adolescentswith JFM [23,28,40].
2.4. Statistical analysis
Two general approaches have been used to determine clinicallysignificant or meaningful differences in prior studies. Anchor-basedapproaches compare changes in outcome to another measure ofchange, often an anchor or external criterion, whereas distribu-tion-based approaches compare changes in outcome to a measureof variability (reviewed by Copay et al. [7] and Wyrwich andWolinsky [48]). In this study, clinically meaningful changes werecalculated using the framework by Jacobson et al. [19] that com-bines both anchor- and distribution-based approaches to estimateclinically significant change, which includes the following: achiev-ing a magnitude of change that is statistically reliable; and demon-strating movement from a dysfunctional to more functional rangeover the course of treatment.
For the first criterion in estimating clinical significance, a statis-tically reliable change in functional disability was establishedusing the distribution-based Reliable Change Index (RCI) approach[19,20]. The RCI is beneficial because it uses the standard error ofdifference (SEdiff) to determine whether a change in score frompre- to post-treatment is due to real change and not measurementerror. The following equation was used to calculate RCI:
RCI ¼ X1 � X2
SEdiff
where SEdiff is computed directly from the standard error of mea-surement, which is derived from the standard deviation at baselineand the scale reliability estimate. RCI values for individual patientchanges in disability were calculated, and values >1.96 were unli-kely to occur by chance and reflected an actual reliable change inscores with 95% confidence [20].
The second criterion in estimating clinical significance calls formovement in the outcome of interest from a dysfunctional to morefunctional range based on established clinical criteria. This criterion
Please cite this article in press as: Sil S et al. Identifying treatment responders anile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
is further supported by the findings of Crosby et al., who noted thatdistribution-based methods are greatly enhanced by comparing theestimated threshold value to other clinical measures to enhanceinterpretability. Therefore, the established FDI clinical referencepoints for pediatric pain patients (0–12 = no/minimal disability,13–29 = moderate disability, and 30–60 = severe disability) [21]were used to identify patients who demonstrated an improvementin the level of disability on their FDI scores from baseline to follow-up (eg, moving from the severe disability level to the moderate and/or minimal disability level; moving from the moderate disability le-vel to the minimal disability level).
To determine the characteristics that predicted a clinically sig-nificant improvement on the FDI, participants’ FDI change scoresfrom baseline to 6-month follow-up were first categorized as ‘‘reli-ably improved’’ (RCI P 1.96), ‘‘reliably declined’’ (RCI 6 �1.96), or‘‘stable’’ (�1.96 < RCI < 1.96). Similarly, the change in the severityof participants’ FDI scores from baseline to follow-up also were cat-egorized as ‘‘improved’’ (eg, FDI score moved from severe (30–60)to moderate (13–29) or from severe or moderate to minimal (0–12)level), ‘‘declined’’ (FDI score moved into higher severity level), or‘‘stable’’ (FDI score remained in same level). Participants whoachieved a clinically significant difference in functioning were clas-sified as treatment responders if they achieved a reliably improvedFDI change score and also improved the disability level of their FDIscore from baseline to follow-up. Treatment nonresponders in-cluded those who achieved a reliably improved FDI score butwhose severity category remained stable or declined, or thosewhose FDI scores were stable regardless of change in level of sever-ity. Frequencies of treatment responders’ and nonresponders’ FDIseverity at the end of the study (ie, no/minimal, moderate, or se-vere disability) were explored to further support the clinical signif-icance of change in functional disability. Binary logistic regressionanalyses were conducted to examine whether baseline disability,average pain intensity, depressive symptoms, coping efficacy, andparental pain history predicted treatment response. Given thatboth treatment arms were active interventions, analyses were con-ducted separately for CBT and FE groups to identify predictors thatwere relevant within each active intervention. In particular, sepa-rate group analyses allowed a clearer determination of which pa-tients were likely to positively respond to CBT and evaluatewhether the prediction of treatment success differed for patientswho received only fibromyalgia education.
3. Results
3.1. Sample characteristics
The final sample of 100 patients (50 in each arm) were15.02 years on average (SD = 1.75). The majority of the samplewere white (90%), female (93%), and attended regular school(86%). There were no significant differences between participantsin the CBT and FE conditions with regard to age, gender, race/eth-nicity, socioeconomic status, duration since pain onset, averagepain intensity, functional disability, depressive symptoms, schoolabsences, or type of schooling at baseline.
3.2. Estimating clinically significant change
The standard deviation of the FDI at baseline was 8.419(mean = 19.82), and the internal consistency of the FDI for the sam-ple was excellent (Cronbach’s a = 0.887). A baseline to follow-upFDI change score of at least 7.8 was needed to exceed the RCIcut-off value of 1.96, and corresponded to an average 40% reduc-tion in disability. To establish a statistically reliable change withthe RCI method, patients were classified as reliably improved,stable, or declined in their functional disability from baseline to
nd predictors of improvement after cognitive-behavioral therapy for juve-
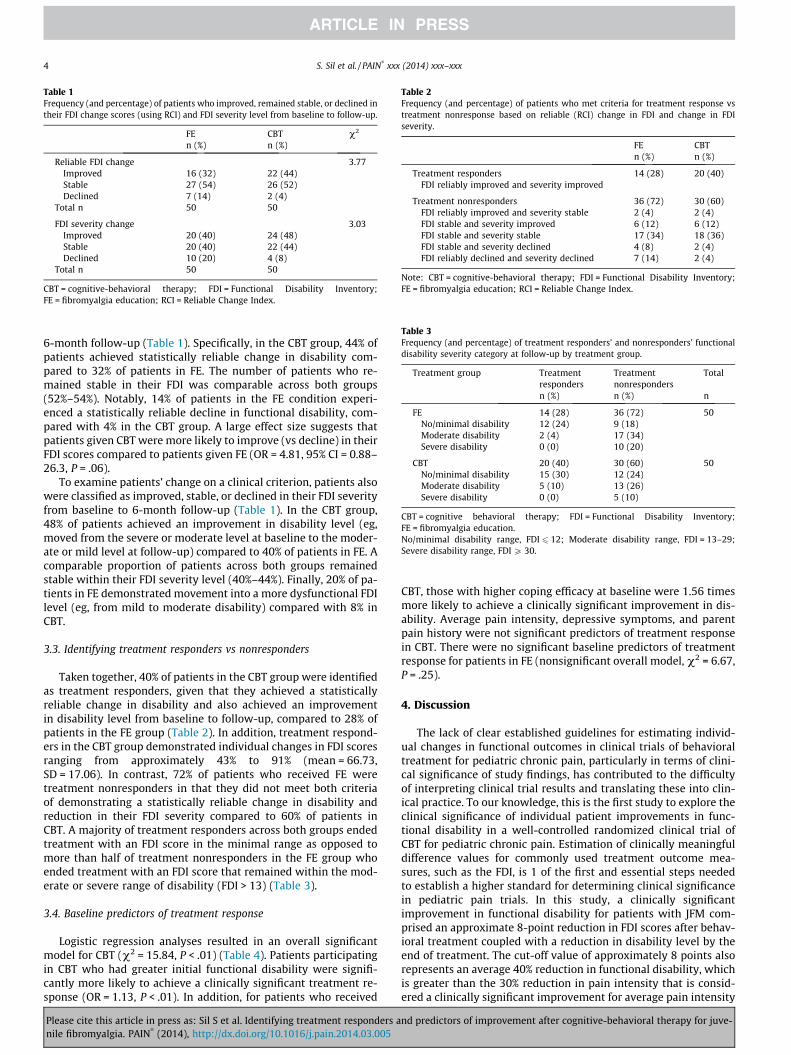
Table 1Frequency (and percentage) of patients who improved, remained stable, or declined intheir FDI change scores (using RCI) and FDI severity level from baseline to follow-up.
FE CBT v2
n (%) n (%)
Reliable FDI change 3.77Improved 16 (32) 22 (44)Stable 27 (54) 26 (52)Declined 7 (14) 2 (4)
Total n 50 50
FDI severity change 3.03Improved 20 (40) 24 (48)Stable 20 (40) 22 (44)Declined 10 (20) 4 (8)
Total n 50 50
CBT = cognitive-behavioral therapy; FDI = Functional Disability Inventory;FE = fibromyalgia education; RCI = Reliable Change Index.
Table 2Frequency (and percentage) of patients who met criteria for treatment response vstreatment nonresponse based on reliable (RCI) change in FDI and change in FDIseverity.
FE CBTn (%) n (%)
Treatment responders 14 (28) 20 (40)FDI reliably improved and severity improved
Treatment nonresponders 36 (72) 30 (60)FDI reliably improved and severity stable 2 (4) 2 (4)FDI stable and severity improved 6 (12) 6 (12)FDI stable and severity stable 17 (34) 18 (36)FDI stable and severity declined 4 (8) 2 (4)FDI reliably declined and severity declined 7 (14) 2 (4)
Note: CBT = cognitive-behavioral therapy; FDI = Functional Disability Inventory;FE = fibromyalgia education; RCI = Reliable Change Index.
Table 3Frequency (and percentage) of treatment responders’ and nonresponders’ functionaldisability severity category at follow-up by treatment group.
Treatment group Treatmentresponders
Treatmentnonresponders
Total
n (%) n (%) n
FE 14 (28) 36 (72) 50No/minimal disability 12 (24) 9 (18)Moderate disability 2 (4) 17 (34)Severe disability 0 (0) 10 (20)
CBT 20 (40) 30 (60) 50No/minimal disability 15 (30) 12 (24)Moderate disability 5 (10) 13 (26)Severe disability 0 (0) 5 (10)
CBT = cognitive behavioral therapy; FDI = Functional Disability Inventory;FE = fibromyalgia education.No/minimal disability range, FDI 6 12; Moderate disability range, FDI = 13–29;Severe disability range, FDI P 30.
4 S. Sil et al. / PAIN�
xxx (2014) xxx–xxx
6-month follow-up (Table 1). Specifically, in the CBT group, 44% ofpatients achieved statistically reliable change in disability com-pared to 32% of patients in FE. The number of patients who re-mained stable in their FDI was comparable across both groups(52%–54%). Notably, 14% of patients in the FE condition experi-enced a statistically reliable decline in functional disability, com-pared with 4% in the CBT group. A large effect size suggests thatpatients given CBT were more likely to improve (vs decline) in theirFDI scores compared to patients given FE (OR = 4.81, 95% CI = 0.88–26.3, P = .06).
To examine patients’ change on a clinical criterion, patients alsowere classified as improved, stable, or declined in their FDI severityfrom baseline to 6-month follow-up (Table 1). In the CBT group,48% of patients achieved an improvement in disability level (eg,moved from the severe or moderate level at baseline to the moder-ate or mild level at follow-up) compared to 40% of patients in FE. Acomparable proportion of patients across both groups remainedstable within their FDI severity level (40%–44%). Finally, 20% of pa-tients in FE demonstrated movement into a more dysfunctional FDIlevel (eg, from mild to moderate disability) compared with 8% inCBT.
3.3. Identifying treatment responders vs nonresponders
Taken together, 40% of patients in the CBT group were identifiedas treatment responders, given that they achieved a statisticallyreliable change in disability and also achieved an improvementin disability level from baseline to follow-up, compared to 28% ofpatients in the FE group (Table 2). In addition, treatment respond-ers in the CBT group demonstrated individual changes in FDI scoresranging from approximately 43% to 91% (mean = 66.73,SD = 17.06). In contrast, 72% of patients who received FE weretreatment nonresponders in that they did not meet both criteriaof demonstrating a statistically reliable change in disability andreduction in their FDI severity compared to 60% of patients inCBT. A majority of treatment responders across both groups endedtreatment with an FDI score in the minimal range as opposed tomore than half of treatment nonresponders in the FE group whoended treatment with an FDI score that remained within the mod-erate or severe range of disability (FDI > 13) (Table 3).
3.4. Baseline predictors of treatment response
Logistic regression analyses resulted in an overall significantmodel for CBT (v2 = 15.84, P < .01) (Table 4). Patients participatingin CBT who had greater initial functional disability were signifi-cantly more likely to achieve a clinically significant treatment re-sponse (OR = 1.13, P < .01). In addition, for patients who received
Please cite this article in press as: Sil S et al. Identifying treatment responders anile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
CBT, those with higher coping efficacy at baseline were 1.56 timesmore likely to achieve a clinically significant improvement in dis-ability. Average pain intensity, depressive symptoms, and parentpain history were not significant predictors of treatment responsein CBT. There were no significant baseline predictors of treatmentresponse for patients in FE (nonsignificant overall model, v2 = 6.67,P = .25).
4. Discussion
The lack of clear established guidelines for estimating individ-ual changes in functional outcomes in clinical trials of behavioraltreatment for pediatric chronic pain, particularly in terms of clini-cal significance of study findings, has contributed to the difficultyof interpreting clinical trial results and translating these into clin-ical practice. To our knowledge, this is the first study to explore theclinical significance of individual patient improvements in func-tional disability in a well-controlled randomized clinical trial ofCBT for pediatric chronic pain. Estimation of clinically meaningfuldifference values for commonly used treatment outcome mea-sures, such as the FDI, is 1 of the first and essential steps neededto establish a higher standard for determining clinical significancein pediatric pain trials. In this study, a clinically significantimprovement in functional disability for patients with JFM com-prised an approximate 8-point reduction in FDI scores after behav-ioral treatment coupled with a reduction in disability level by theend of treatment. The cut-off value of approximately 8 points alsorepresents an average 40% reduction in functional disability, whichis greater than the 30% reduction in pain intensity that is consid-ered a clinically significant improvement for average pain intensity
nd predictors of improvement after cognitive-behavioral therapy for juve-

Table 4Logistic regression analyses to identify baseline predictors of clinically significant treatment response.
Baseline predictor Fibromyalgia education Cognitive-behavioral therapy
b OR (95% CI) Wald v2 b OR (95% CI) Wald v2
Functional disability (FDI) 0.10 1.10 (0.99–1.22) 3.40 0.12 1.13 (1.03–1.23) 7.05**
Average pain intensity (VAS) �0.40 0.67 (0.38–1.16) 2.03 �0.25 1.29 (0.77–2.16) 0.91Depressive symptoms (CDI) 0.05 1.05 (0.93–1.18) 0.65 �0.01 1.01 (0.91–1.13) 0.06Coping efficacy (PCQ) 0.31 1.37 (0.88–2.13) 1.92 0.45 1.56 (1.01–2.43) 3.97*
Parent pain history 0.17 1.19 (0.88–1.61) 1.20 �0.03 1.03 (0.85–1.25) 0.09
CDI = Children’s Depression Inventory; CI = confidence interval: FDI = Functional Disability Inventory; PCQ = Pain Coping Questionnaire; VAS = visual analogue scale.* p < 0.05.** p < 0.01.
S. Sil et al. / PAIN�
xxx (2014) xxx–xxx 5
[14,31]. Although there is no direct comparison for clinically mean-ingful differences on the FDI, integrating a statistically reliablechange and change on a clinical criterion is, by far, more conserva-tive and clearly sets a higher bar for defining ‘‘improvement’’ com-pared to traditional group mean differences. In fact, group meandifferences often result in large and statistically significant treat-ment effects in behavioral trials, including the primary trial find-ings of Kashikar-Zuck [26], often with moderate sample sizes(numbers typically range from 30 to 80) [35]. With the more con-servative approach of examining clinical significance, the resultsfrom the current study continue to support the primary trial find-ings that CBT is beneficial in the treatment of JFM; however, the ef-fects are less robust because of power limitations. To advance theevidence base for behavioral interventions for pediatric chronicpain, it is critical for researchers to consider clinical significancerather than statistical significance as a primary outcome. By doingso, clinical trials that are powered based on clinical significancewill be able to more fully capture meaningful changes in patients’functional outcomes.
Estimating clinically meaningful change is a novel approachthat has been used to establish clinically significant changes inpain intensity in a few studies of adults with chronic pain[13–15,31,38], and is just starting to generalize to other pain-related health outcomes in adults [33,41,46]. Comparing CBT toan educational intervention (FE) that provided support and educa-tion (as opposed to a wait list or standard care control typicallyused in clinical trials of CBT for chronic pain) further contributedto the more rigorous and conservative method of estimating clini-cal significance in this study. For patients who received CBT, 40%were treatment responders, of which the majority (75%) achieveda clinically significant improvement in functional disability that re-sulted in no/minimal disability. Notably, this is a similar responserate compared to studies in adults with fibromyalgia who re-sponded positively to CBT (38%) [44] and is somewhat higher com-pared to the response of adult patients with chronic pain whoachieved clinically significant improvements in disability afterAcceptance and Commitment Therapy (ACT) (25%) [46]. In con-trast, only 28% of patients in FE positively responded to treatment,and 20% actually declined in their functioning. This decline may re-flect the natural course of change over 6 months that occurs whenpatients receive no direct training in coping skills to manage pain.In addition, approximately 35% of patients in both groups demon-strated stable FDI scores that remained within the same severitylevel over time. Minor fluctuations in FDI scores that do not meetthe threshold value and do not cross severity levels may reflect lesswillingness or openness by patients to participate in treatment,and indicate the need for additional or more intensive educationregarding the goals and benefits of behavioral intervention. Theseindividual patterns of change often are not evident in clinical trialfindings that focus on evaluating group mean differences, butprovide meaningful information about patients’ response to behav-ioral interventions. Information about the likelihood of an individ-ual patient’s response to an intervention can guide clinicians in
Please cite this article in press as: Sil S et al. Identifying treatment responders anile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
clinical decision making and potentially lead to improved patientcare. Although the estimation of clinical significance has not yetbeen fully explored in the pediatric chronic pain literature, thisstudy provides preliminary evidence and a rationale to supportthe use of this approach as a method of evaluating clinical signifi-cance and improving interpretability of treatment effects acrosspediatric pain trials.
Our second objective was to use the results to better under-stand individual patient characteristics that predicted clinicallysignificant treatment response in functional disability after behav-ioral treatment. The findings suggest that patients with greaterfunctional disability at baseline were more likely to achieve a clin-ically significant change in disability, which may reflect a greateropportunity to improve their functioning with treatment. In addi-tion, patients with initial high levels of coping efficacy were 1.6times more likely to respond positively to CBT. A high initial copingself-efficacy may represent a protective factor that helps patientsto be receptive to and harness more adaptive coping strategies inresponse to pain. In contrast, those with lower coping efficacy be-fore starting treatment may be in an early stage of readiness tochange their behavior and coping. Consequently, they may notadopt or use the coping strategies taught during treatment as reg-ularly or effectively to manage pain, or may require a longer dura-tion of psychological intervention before meaningful changes arenoted. As such, patients with lower coping efficacy may benefitfrom tailored treatments that better match their needs. For exam-ple, these patients may benefit from CBT that is modified to includea motivational interviewing approach to enhance patients’ willing-ness to engage in behavior change before the onset of teachingadaptive coping skills to manage pain. Moving forward, under-standing patients’ cognitive appraisals of pain (eg, catastrophicthinking) as well as their pain beliefs may also be important to as-sess [24,42], to guide the development of tailored interventionsthat can enhance coping efficacy and improve daily functioning.
In contrast, baseline levels of pain intensity, depressive symp-toms, and parent pain history were not predictive of a clinicallysignificant treatment response, despite their evidence in the adultchronic pain literature [3,43]. This may suggest that adolescents’response to treatment may be influenced by a more complex inter-action of factors that incorporates the context of the family andparental responses to pain [34], such as marked catastrophic think-ing coupled with parental overprotection [17]. Additional researchin this area is warranted to examine how the interaction of child,parent, and family responses to pain influences treatment responsein adolescents.
The interpretation of study findings should be considered with-in the context of a few limitations. First, clinically meaningfulchange was calculated using Jacobson’s framework for definingand estimating clinical significance, which includes establishing astatistically reliable change in the outcome of interest and move-ment of the outcome from a dysfunctional to more functional level[19]. A variety of well-supported approaches to estimatingclinically meaningful differences are available and have been
nd predictors of improvement after cognitive-behavioral therapy for juve-

6 S. Sil et al. / PAIN�
xxx (2014) xxx–xxx
commonly used in past studies [1,7,8,12]. Future studies might usealternative approaches to establish clinical significance, and it willbe important to examine whether similar estimates are found. Inaddition, it is not clear whether these findings will be generalizableto other pain conditions. Finally, the number of constructs exam-ined in predicting improvement in functional disability was lim-ited because of the sample size of each treatment group. It islikely that, with a larger sample and greater statistical power, addi-tional predictors might have emerged as significant predictors oftreatment response. Future examination of additional variables,such as adolescent and parental pain beliefs, catastrophic thinking,readiness and motivation to change, and acceptance is warrantedto understand their potential in predicting treatment response.
These limitations notwithstanding, the estimation of clinicalsignificance for functional disability for adolescents with fibromy-algia begins the process of establishing an important referencepoint for clinicians and researchers interested in interpreting treat-ment effects using a common metric for measuring patients’ func-tional disability. Future studies may consider establishing clinicalsignificance for outcome measures, such as disability or pain inten-sity, for pediatric chronic pain patients in real-world clinical set-tings, to clarify whether these clinically meaningful changestranslate into clinical practice. Researchers evaluating the use ofCBT may also need to consider how to make treatment effects morepowerful by adding new components to treatment or using moretailored approaches based on patient needs (eg, motivational inter-viewing for those who show more reluctance to incorporate behav-ioral changes, or combining physical exercise training/behavioralactivation for those who are very sedentary). Finally, future clinicaltrials can build on this approach to establish clearer standards forestimating clinical significance, improve interpretability of treat-ment outcomes across pediatric pain trials, and guide the develop-ment of more powerful tailored interventions to match patientneeds and result in greater patient improvements.
Conflict of interest statement
The authors have no conflicts of interest, financial or otherwise,related to this study.
Acknowledgements
We thank the following additional members of the JuvenileFibromyalgia Clinical Trial Research Team: Judy Bean (CincinnatiChildren’s Hospital), Dr. T. Brent Graham (Vanderbilt UniversitySchool of Medicine), Drs. Steven Spalding, Gerard Banez, and Mar-garet M. Richards-Mauze (Cleveland Clinic Lerner School of Medi-cine). We also thank study coordinators Raegan Malblanc MA,Sonya Crook, RN, Megan Johnston, MA, and Emily Verkamp,MSW. This study was funded by the National Institutes of Arthritisand Musculoskeletal and Skin Diseases (NIAMS) grantR01AR050028 (S.K.-Z.).
References
[1] Beaton DE, Boers M, Wells GA. Many faces of the minimal clinically importantdifference (MCID): a literature review and directions for future research. CurrOpin Rheumatol 2002;14:109–14.
[2] Birnie KA, McGrath PJ, Chambers CT. When does pain matter? Acknowledgingthe subjectivity of clinical significance. PAIN� 2012;153:2311–4.
[3] Blanchard EB, Lackner JM, Gusmano R, Gudleski GD, Sanders K, Keefer K,Krasner S. Prediction of treatment outcome among patients with irritablebowel syndrome treated with group cognitive therapy. Behav Res Ther2006;44:317–37.
[4] Claar RL, Walker LS. Functional assessment of pediatric pain patients:psychometric properties of the functional disability inventory. PAIN�
2006;121:77–84.[5] Clancy CM, Eisenberg JM. Outcomes research: measuring the end results of
health care. Science 1998;282:245–6.
Please cite this article in press as: Sil S et al. Identifying treatment responders anile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
[6] Conte P, Walco G, Kimura Y. Temperament and stress response in childrenwith juvenile primary fibromyalgia syndrome. Arthritis Rheum2003;48:2923–30.
[7] Copay AG, Subach BR, Glassman SD, Polly DW, Schuler TC. Understanding theminimum clinically important difference: a review of concepts and methods.Spine J 2007;7:541–6.
[8] Crosby RD, Kolotkin RL, Williams GR. Defining clinically meaningful change inhealth-related quality of life. J Clin Epidemiol 2003;56:395–407.
[9] Dworkin RH, Turk DC, McDermott MP, Peirce-Sandner S, Burke LB, Cowan P,Farrar JT, Hertz S, Raja SN, Rappaport BA, Rauschkolb C, Sampaio C.Interpreting the clinical importance of group differences in chronic painclinical trials: IMMPACT recommendations. PAIN� 2009;146:238–44.
[10] Eccleston, Crombez G, Scotford A, Clinch J, Connell H. Adolescent chronic pain:patterns and predictors of emotional distress in adolescents with chronic painand their parents. PAIN� 2004;108:221–9.
[11] Eccleston C, Palermo TM, Williams ACdC, Lewandowski A, Morley S.Psychological therapies for the management of chronic and recurrent pain inchildren and adolescents. Cochrane Database Syst Rev 2013:1–84.
[12] Eisen S, Ranganathan G, Seal P, Spiro III A. Measuring clinically meaningfulchange following mental health treatment. J Behav Health Serv Res2007;34:272–89.
[13] Farrar JT, Portenoy RK, Berlin JA, Kinman JL, Strom BL. Defining the clinicallyimportant difference in pain outcome measures. PAIN� 2000;88:287–94.
[14] Farrar JT, Pritchett YL, Robinson M, Prakash A, Chappell A. The clinicalimportance of changes in the 0 to 10 numeric rating scale for worst, least, andaverage pain intensity: analyses of data from clinical trials of duloxetine inpain disorders. J Pain 2010;11:109–18.
[15] Farrar JT, Young Jr JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance ofchanges in chronic pain intensity measured on an 11-point numerical painrating scale. PAIN� 2001;94:149–58.
[16] Ferguson R, Robinson A, Splaine M. Use of the Reliable Change Index toevaluate clinical significance in SF-36 outcomes. Qual Life Res2002;11:509–16.
[17] Guite JW, McCue RL, Sherker JL, Sherry DD, Rose JB. Relationships among pain,protective parental responses, and disability for adolescents with chronicmusculoskeletal pain: the mediating role of pain catastrophizing. Clin J Pain2011;27:775–81.
[18] Hays RD, Woolley JM. The concept of clinically meaningful difference inhealth-related quality-of-life research. Pharmacoeconomics 2000;18:419–23.
[19] Jacobson NS, Roberts LJ, Berns SB, McGlinchey JB. Methods for defining anddetermining the clinical significance of treatment effects: description,application, and alternatives. J Consult Clin Psychol 1999;67:300.
[20] Jacobson NS, Truax P. Clinical significance. J Consult Clin Psychol1991;59:12–9.
[21] Kashikar-Zuck S, Flowers SR, Claar RL, Guite JW, Logan DE, Lynch-Jordan AM,Palermo TM, Wilson AC. Clinical utility and validity of the Functional DisabilityInventory (FDI) among a multicenter sample of youth with chronic pain. PAIN�
2011;15:1600–7.[22] Kashikar-Zuck S, Goldschneider KR, Powers SW, Vaught MH, Hershey AD.
Depression and functional disability in chronic pediatric pain. Clin J Pain2001;17:341–9.
[23] Kashikar-Zuck S, Lynch AM, Slater S, Graham TB, Swain NF, Noll RB. Familyfactors, emotional functioning, and functional impairment in juvenilefibromyalgia syndrome. Arthritis Rheum 2008;59:1392–8.
[24] Kashikar-Zuck S, Sil S, Lynch-Jordan AM, Ting TV, Peugh J, Schikler KN, HashkesPJ, Arnold LM, Passo M, Richards-Mauze MM, Powers SW, Lovell DJ. Changes inpain coping, catastrophizing, and coping efficacy after cognitive-behavioraltherapy in children and adolescents with juvenile fibromyalgia. J Pain2013;14:492–501.
[25] Kashikar-Zuck S, Swain NF, Jones BA, Graham TB. Efficacy of cognitive-behavioral intervention for juvenile primary fibromyalgia syndrome. JRheumatol 2005;32:1594–602.
[26] Kashikar-Zuck S, Ting TV, Arnold LM, Bean J, Powers SW, Graham TB, PassoMH, Schikler KN, Hashkes PJ, Spalding S, Lynch-Jordan AM, Banez G, RichardsMM, Lovell DJ. Cognitive behavioral therapy for the treatment of juvenilefibromyalgia: a multisite, single-blind, randomized, controlled clinical trial.Arthritis Rheum 2012;64:297–305.
[27] Kovacs M. Children’s Depression Inventory. North Tonawanda (NY): Multi-Health Systems, 1992.
[28] Lester N, Lefebvre JC, Keefe FJ. Pain in young adults: I. Relationship to genderand family pain history. Clin J Pain 1994;10:282–9.
[29] Lynch AM, Kashikar-Zuck S, Goldschneider KR, Jones BA. Psychosocialrisks for disability in children with chronic back pain. J Pain2006;7:244–51.
[30] McGrath PJ, Walco GA, Turk DC, Dworkin RH, Brown MT, Davidson K, EcclestonC, Finley GA, Goldschneider K, Haverkos L, Hertz SH, Ljungman G, Palermo T,Rappaport BA, Rhodes T, Schechter N, Scott J, Sethna N, Svensson OK, Stinson J,von Baeyer CL, Walker L, Weisman S, White RE, Zajicek A, Zeltzer L. Coreoutcome domains and measures for pediatric acute and chronic/recurrent painclinical trials: PedIMMPACT recommendations. J Pain 2008;9:771–83.
[31] Mease PJ, Spaeth M, Clauw DJ, Arnold LM, Bradley LA, Russell IJ, Kajdasz DK,Walker DJ, Chappell AS. Estimation of minimum clinically importantdifference for pain in fibromyalgia. Arthritis Care Res 2011;63:821–6.
[32] Morley S, Williams A, Eccleston C. Examining the evidence of psychologicaltreatments for chronic pain: time for a paradigm shift? PAIN�
2013;154:1929–31.
nd predictors of improvement after cognitive-behavioral therapy for juve-

S. Sil et al. / PAIN�
xxx (2014) xxx–xxx 7
[33] Morley S, Williams A, Hussain S. Estimating the clinical effectiveness ofcognitive behavioural therapy in the clinic: evaluation of a CBT informed painmanagement programme. PAIN� 2008;137:670–80.
[34] Palermo TM, Chambers CT. Parent and family factors in pediatric chronic painand disability: an integrative approach. PAIN� 2005;119:1–4.
[35] Palermo TM, Eccleston C, Lewandowski AS, Williams AC, Morley S.Randomized controlled trials of psychological therapies for management ofchronic pain in children and adolescents: an updated meta-analytic review.PAIN� 2010;148:387–97.
[36] Rapoff MA. Pediatric measures of pain. Arthritis Rheum 2003;49:S90–5.[37] Reid GJ, Gilbert CA, McGrath PJ. The Pain Coping Questionnaire: preliminary
validation. PAIN� 1998;76:83–96.[38] Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically
important changes in chronic musculoskeletal pain intensity measured on anumerical rating scale. Eur J Pain 2004;8:283–91.
[39] Schanberg LE, Anthony KK, Gil KM, Lefebvre JC, Kredich DW, Macharoni LM.Family pain history predicts child health status in children with chronicrheumatic disease. Pediatrics 2001;108:E47.
[40] Schanberg LE, Keefe FJ, Lefebvre JC, Kredich DW, Gil KM. Social context of painin children with juvenile primary fibromyalgia syndrome: parental painhistory and family environment. Clin J Pain 1998;14:107–15.
[41] Schmidt S, Grossman P, Schwarzer B, Jena S, Naumann J, Walach H. Treatingfibromyalgia with mindfulness-based stress reduction: results from a 3-armedrandomized controlled trial. PAIN� 2011;152:361–9.
Please cite this article in press as: Sil S et al. Identifying treatment responders anile fibromyalgia. PAIN
�(2014), http://dx.doi.org/10.1016/j.pain.2014.03.005
[42] Sil S, Kashikar-Zuck S. Understanding why cognitive–behavioral therapy is aneffective treatment for adolescents with juvenile fibromyalgia. Int J ClinRheumatol 2013;8:213–9.
[43] Sinclair V, Wallston K. Predictors of improvement in a cognitive-behavioralintervention for women with rheumatoid arthritis. Ann Behav Med2001;23:291–7.
[44] Thieme K, Turk DC, Flor H. Responder criteria for operant and cognitive–behavioral treatment of fibromyalgia syndrome. Arthritis Care Res2007;57:830–6.
[45] Turk DC, Okifuji A, Sinclair JD, Starz TW. Interdisciplinary treatment forfibromyalgia syndrome: clinical and statistical significance. Arthritis Rheum1998;11:186–95.
[46] Vowles KE, Witkiewitz K, Sowden G, Ashworth J. Acceptance and commitmenttherapy for chronic pain: evidence of mediation and clinically significantchange following an abbreviated interdisciplinary program of rehabilitation. JPain 2014;15:101–13.
[47] Walker LS, Greene JW. The functional disability inventory: measuring aneglected dimension of child health status. J Pediatr Psychol 1991;16:39–58.
[48] Wyrwich KW, Wolinsky FD. Identifying meaningful intra-individual changestandards for health-related quality of life measures. J Eval Clin Pract2000;6:39–49.
[49] Yunus MB, Masi AT. Juvenile primary fibromyalgia syndrome. A clinical studyof thirty-three patients and matched normal controls. Arthritis Rheum1985;28:138–45.
nd predictors of improvement after cognitive-behavioral therapy for juve-