Embed Size (px)
Citation preview
Surg Today (2009) 39:610–614DOI 10.1007/s00595-008-3890-8
Reprint requests to: A. KumarReceived: June 24, 2008 / Accepted: September 25, 2008
Idiopathic Sclerosing Encapsulating Peritonitis — Is a Preoperative Diagnosis Possible? Report of Three Cases
AMEET KUMAR1, T.S. RAMAKRISHNAN
1,2, SAMARESH SAHU3, and K.B. MISHRA
1
Departments of 1 Surgery, 2 Orthopaedics, and 3 Radiology, Air Force Hospital, Nathu Singh Road, Kanpur Cantt, UP 208004, India
AbstractSclerosing encapsulating peritonitis (SEP) is a rare cause of intestinal obstruction that is usually diagnosed during a laparotomy; however, a preoperative diagnosis is possible. Sclerosing encapsulating peritonitis can be classifi ed as primary or idiopathic and secondary types and only about 70 cases of idiopathic type have been reported since it was fi rst described. It is characterized by a total or partial encasement of the small bowel by a thick fi brotic membrane. This report presents a series of three cases in which a diagnosis of idiopathic SEP was made preoperatively based on the clinical features and radiological fi ndings, which were confi rmed by a laparotomy and histopathology. All of the cases were successfully managed by the excision of the membrane. This report demonstrates that based on the clinical fea-tures and radiological investigations, in the absence of other plausible etiologies for intestinal obstruction, it is possible to suspect a preoperative diagnosis of SEP, thereby preventing a “surprise” fi nding during a lapa-rotomy and allowing for better management.
Key words Sclerosing encapsulating peritonitis · Abdominal cocoon · Intestinal obstruction · Preopera-tive diagnosis
Introduction
Sclerosing encapsulating peritonitis (SEP) is a rare cause of intestinal obstruction that is usually diagnosed at the time of a laparotomy; however, a preoperative diagnosis is possible. Sclerosing encapsulating peritoni-tis can be classifi ed as primary or idiopathic and second-ary types. About 70 cases of the idiopathic type have
been reported since it was fi rst described by Foo et al., who used the term abdominal cocoon to describe idio-pathic SEP.1 It is usually characterized by a total or partial encasement of the small bowel by a thick fi brotic membrane primarily in females, although it has been reported in males as well. Sclerosing encapsulating peri-tonitis is usually of unknown origin although at times it may be seen as secondary to a variety of conditions. This paper reports a series of three patients, two males and one female, who presented with symptoms of intes-tinal obstruction in which a diagnosis of idiopathic SEP was made preoperatively, and was confi rmed by a lapa-rotomy and the histopathology.
Case Reports
Case 1
A 45-year-old man was admitted to the hospital with complaints of diffuse abdominal pain, nausea, and vom-iting. He had mild upper abdominal distension but was passing fl atus. He had experienced similar episodes on two occasions in the previous two years and had been admitted elsewhere and treated conservatively; however, the details of the disease and treatment were not avail-able. There were no constitutional symptoms and he denied any history of prolonged drug use, abdominal disease, tuberculosis, or surgery. On examination, he was afebrile and his vitals were stable. On abdominal examination, there was upper abdominal distension and a soft, nontender mass, which was resonant on percus-sion occupying the epigastrium and extending to left hypochondrium. The bowel sounds were hyperactive. A rectal examination did not reveal any abnormality and the rest of systemic examination was also normal.
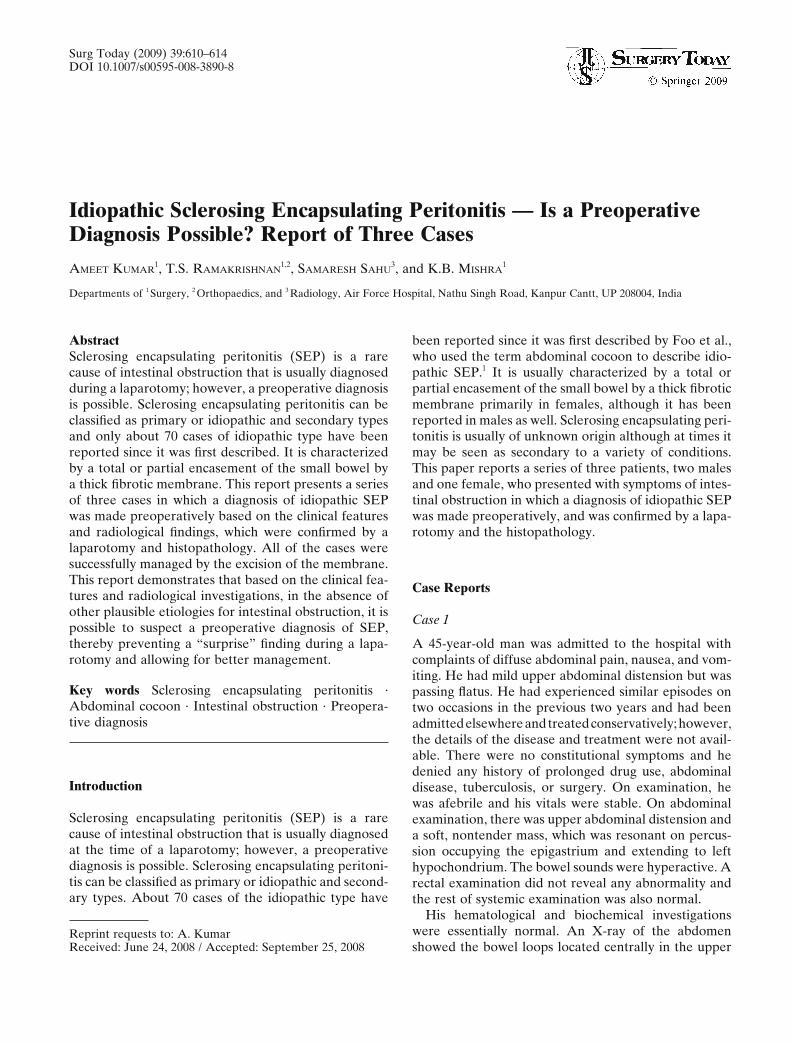
His hematological and biochemical investigations were essentially normal. An X-ray of the abdomen showed the bowel loops located centrally in the upper
A. Kumar et al.: Idiopathic Sclerosing Encapsulating Peritonitis 611
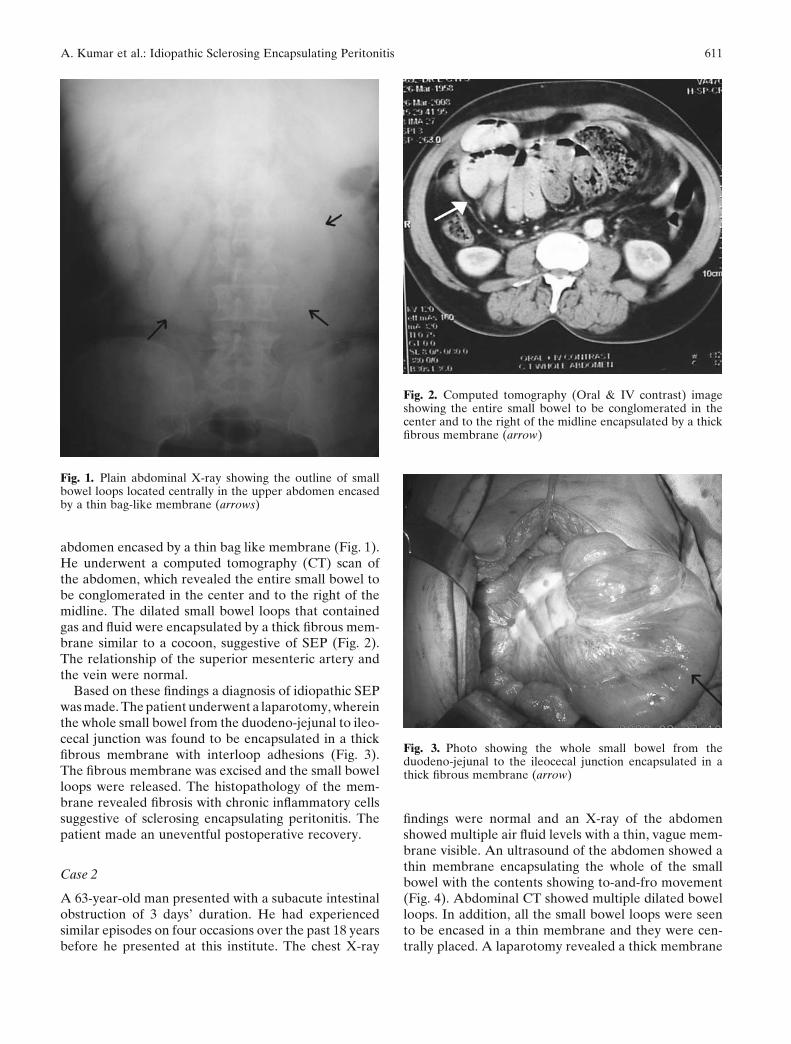
abdomen encased by a thin bag like membrane (Fig. 1). He underwent a computed tomography (CT) scan of the abdomen, which revealed the entire small bowel to be conglomerated in the center and to the right of the midline. The dilated small bowel loops that contained gas and fl uid were encapsulated by a thick fi brous mem-brane similar to a cocoon, suggestive of SEP (Fig. 2). The relationship of the superior mesenteric artery and the vein were normal.
Based on these fi ndings a diagnosis of idiopathic SEP was made. The patient underwent a laparotomy, wherein the whole small bowel from the duodeno-jejunal to ileo-cecal junction was found to be encapsulated in a thick fi brous membrane with interloop adhesions (Fig. 3). The fi brous membrane was excised and the small bowel loops were released. The histopathology of the mem-brane revealed fi brosis with chronic infl ammatory cells suggestive of sclerosing encapsulating peritonitis. The patient made an uneventful postoperative recovery.
Case 2
A 63-year-old man presented with a subacute intestinal obstruction of 3 days’ duration. He had experienced similar episodes on four occasions over the past 18 years before he presented at this institute. The chest X-ray
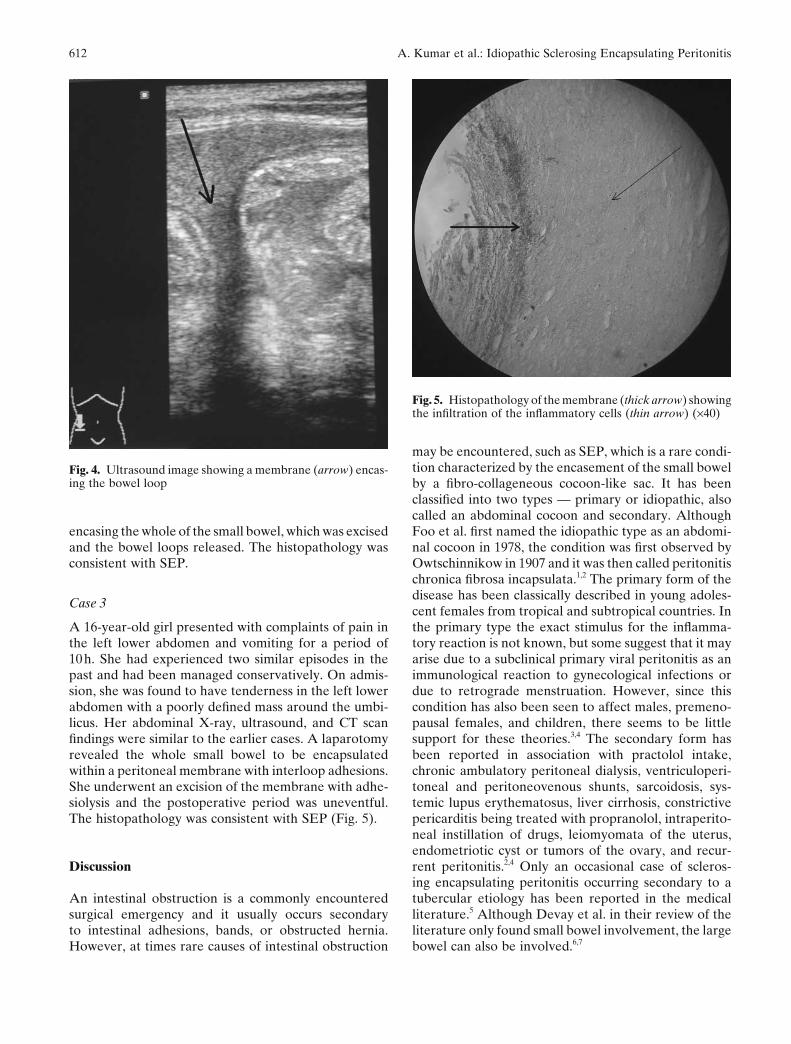
fi ndings were normal and an X-ray of the abdomen showed multiple air fl uid levels with a thin, vague mem-brane visible. An ultrasound of the abdomen showed a thin membrane encapsulating the whole of the small bowel with the contents showing to-and-fro movement (Fig. 4). Abdominal CT showed multiple dilated bowel loops. In addition, all the small bowel loops were seen to be encased in a thin membrane and they were cen-trally placed. A laparotomy revealed a thick membrane
Fig. 1. Plain abdominal X-ray showing the outline of small bowel loops located centrally in the upper abdomen encased by a thin bag-like membrane (arrows)
Fig. 2. Computed tomography (Oral & IV contrast) image showing the entire small bowel to be conglomerated in the center and to the right of the midline encapsulated by a thick fi brous membrane (arrow)
Fig. 3. Photo showing the whole small bowel from the duodeno-jejunal to the ileocecal junction encapsulated in a thick fi brous membrane (arrow)
612 A. Kumar et al.: Idiopathic Sclerosing Encapsulating Peritonitis
encasing the whole of the small bowel, which was excised and the bowel loops released. The histopathology was consistent with SEP.
Case 3
A 16-year-old girl presented with complaints of pain in the left lower abdomen and vomiting for a period of 10 h. She had experienced two similar episodes in the past and had been managed conservatively. On admis-sion, she was found to have tenderness in the left lower abdomen with a poorly defi ned mass around the umbi-licus. Her abdominal X-ray, ultrasound, and CT scan fi ndings were similar to the earlier cases. A laparotomy revealed the whole small bowel to be encapsulated within a peritoneal membrane with interloop adhesions. She underwent an excision of the membrane with adhe-siolysis and the postoperative period was uneventful. The histopathology was consistent with SEP (Fig. 5).
Discussion
An intestinal obstruction is a commonly encountered surgical emergency and it usually occurs secondary to intestinal adhesions, bands, or obstructed hernia. However, at times rare causes of intestinal obstruction
may be encountered, such as SEP, which is a rare condi-tion characterized by the encasement of the small bowel by a fi bro-collageneous cocoon-like sac. It has been classifi ed into two types — primary or idiopathic, also called an abdominal cocoon and secondary. Although Foo et al. fi rst named the idiopathic type as an abdomi-nal cocoon in 1978, the condition was fi rst observed by Owtschinnikow in 1907 and it was then called peritonitis chronica fi brosa incapsulata.1,2 The primary form of the disease has been classically described in young adoles-cent females from tropical and subtropical countries. In the primary type the exact stimulus for the infl amma-tory reaction is not known, but some suggest that it may arise due to a subclinical primary viral peritonitis as an immunological reaction to gynecological infections or due to retrograde menstruation. However, since this condition has also been seen to affect males, premeno-pausal females, and children, there seems to be little support for these theories.3,4 The secondary form has been reported in association with practolol intake, chronic ambulatory peritoneal dialysis, ventriculoperi-toneal and peritoneovenous shunts, sarcoidosis, sys-temic lupus erythematosus, liver cirrhosis, constrictive pericarditis being treated with propranolol, intraperito-neal instillation of drugs, leiomyomata of the uterus, endometriotic cyst or tumors of the ovary, and recur-rent peritonitis.2,4 Only an occasional case of scleros-ing encapsulating peritonitis occurring secondary to a tubercular etiology has been reported in the medical literature.5 Although Devay et al. in their review of the literature only found small bowel involvement, the large bowel can also be involved.6,7
Fig. 4. Ultrasound image showing a membrane (arrow) encas-ing the bowel loop
Fig. 5. Histopathology of the membrane (thick arrow) showing the infi ltration of the infl ammatory cells (thin arrow) (×40)

A. Kumar et al.: Idiopathic Sclerosing Encapsulating Peritonitis 613
Clinically, patients with SEP present with attacks of colicky pain in the abdomen, nausea, and vomiting with intestinal obstruction that is subacute in nature as in the cases presented in this report.8 A soft, nontender mass on abdominal palpation is usually present. The patient may give a history of similar presentations in the past which resolved spontaneously. The diagnosis is diffi cult to establish preoperatively; however, some diagnostic radiological fi ndings have been described.
Conventional radiographs may show evidence of a small-bowel obstruction, with dilated bowel loops and air-fl uid levels in erect abdominal radiographs. A barium meal follow-through study also may help sometimes in revealing this condition by showing a conglomeration of multiple bowel loops that appear to adhere to each other with a suspected sac-like structure surrounding them. On sonography, the small-bowel loops are encased in a thick membrane made visible by minimal ascites. In the appropriate clinical setting, recognition of the entire dilated small bowel at the center of the abdomen and encased within a thick fi bro-collageneous mem-brane as though it were in a cocoon on abdominal CT is diagnostic of sclerosing encapsulating peritonitis.9 Stafford-Johnson et al. described peritoneal thickening with associated calcifi cation, peritoneal enhancement, small bowel tethering, and loculated fl uid collections as the most common signs which are useful in making an accurate diagnosis of sclerosing encapsulating peritoni-tis on CT scans.10
In a case of small-bowel obstruction, an internal hernia that causes a localized collection of small-bowel loops with symptoms of obstruction must be considered in the differential diagnosis of SEP. Transmesenteric and paraduodenal hernias are the most common types of internal hernias. Contrast-enhanced CT fi ndings may allow for an accurate diagnosis in most cases. The main features of an internal hernia on imaging are the central location of the small bowel, evidence of small-bowel obstruction, clustering of the bowel loops, and displace-ment of and a mass effect on adjacent organs. In addi-tion, the mesenteric vessels are stretched, displaced, crowded, and engorged.11 No membrane-like sac can be detected in patients with internal hernias. Sclerosing encapsulating peritonitis may be confused with congeni-tal peritoneal encapsulation, which is characterized by a thin accessory peritoneal sac surrounding the small bowel. This asymptomatic condition is generally found incidentally during unrelated surgery and does not fi t with the clinical or imaging fi ndings in the current patients. The peritoneal membrane in this condition is attached to the ascending and descending colon later-ally, the transverse mesocolon cranially, and the poste-rior parietal peritoneum caudally. The membrane has two openings, one as the intestine enters at about the duodeno-jejunal junction and the other as it leaves at
the ileocecal junction. The relative position of the viscera is normal. Peritoneal encapsulation is probably an embryological abnormality. The accessory perito-neal sac may be derived from the peritoneum of the yolk-sac as it is withdrawn rather rapidly into the abdominal cavity with the small bowel behind it during the 12th week of gestation.12
In a review of the pertinent literature, most authors confi rm the diagnosis during a laparotomy. However, as observed in the current cases, it is possible to entertain a preoperative diagnosis of SEP. The clues to a preop-erative diagnosis are:
1. Attacks of colicky pain abdomen, nausea and vomit-ing with intestinal obstruction that is subacute in nature
2. The absence of other plausible etiologies for the intestinal obstruction
3. A history of similar episodes in the past that resolved spontaneously
4. A soft, non-tender mass on abdominal palpation5. Radiological fi ndings, particularly a CT scan of
abdomen which shows the entire dilated small bowel at the center of the abdomen and encased within a thick fi bro-collageneous membrane as though it were in a cocoon
A preoperative diagnosis prevents a “surprise” fi nding during a laparotomy and thus results in better manage-ment of the case.13
Surgery remains the cornerstone in the management of SEP. A careful dissection and excision of the thick sac with the release of the small intestine leads to com-plete recovery and rarely a resection of adherent bowel loops is required.8,14,15 However, these features are only true of the idiopathic type. In the secondary type, the whole peritoneal cavity is often obliterated by dense adhesions. The visceral and parietal peritoneums are thickened with a shortened small bowel encased in a rigid tube. There is usually no plane of cleavage between the membrane and the bowel, thus making the release of the bowel loops extremely diffi cult; the potential for iatrogenic complications is high in such cases.6,16
The prognosis of idiopathic SEP after surgery tends to be excellent and no recurrence has been described. Only one patient in the literature who had presented with long-standing symptoms and weight loss died post-operatively after a subclavian vein thrombosis due to intravenous hyperalimentation.1
Conclusion
Idiopathic SEP is a rare cause of intestinal obstructions and is seldom diagnosed preoperatively. However, clues to a preoperative diagnosis are recurrent episodes of

614 A. Kumar et al.: Idiopathic Sclerosing Encapsulating Peritonitis
incomplete intestinal obstruction combined with rele-vant imaging fi ndings and lack of other plausible etio-logies. Abdominal CT scans can help in the early recognition of the disease. Surgery is the optimal treat-ment modality for idiopathic SEP via the surgical release of the cocoon membrane, and it can normally be accom-plished with minimal morbidity.
Acknowledgments. The authors thank Dr. Arijit Sen MD (Pathology), Department of Pathology, Air Force Hospital, Kanpur, India, for providing valuable clinical support.
References
1. Foo KT, Rauff A, Foong WC, Sinniah R. Unusual small intestinal obstruction in adolescent girls: the abdominal cocoon. Br J Surg 1978;65:427–30.
2. Sahoo SP, Gangopadhyay AN, Gupta DK, Gopal SC, Sharma SP, Dash RN. Abdominal cocoon in children: a report of four cases. J Pediatric Surg 1996;31:987–8.
3. Yoon YW, Chung JP, Park HJ, Cho HG, Chon CY, Park IS, et al. A case of abdominal cocoon. J Korean Med Science 1995;10:220–5.
4. Wig JD, Goenka MK, Nagi B, Vaphei K. Abdominal cocoon in a male: a rare cause of intestinal obstruction. Trop Gastroenterol 1995;16:31–3.
5. Lalloo S, Krishna D, Maharajh J. Abdominal cocoon associated with tuberculous pelvic infl ammatory disease. Br J Radiol 2002;75:174–6.
6. Devay AO, Gomceli I, Korukluoglu B, Kusdemi A. An unusual and diffi cult diagnosis of intestinal obstruction: the abdominal cocoon. Case report and review of the literature. World J Emerg Surg 2006;1:8.
7. Choi JH, Kim JH, Kim JJ, Jin SY, Choi DL. Large bowel obstruc-tion caused by sclerosing peritonitis: Contrast-enhanced CT fi nd-ings. Br J Radiol 2004;77:344–6.
8. Kumar M, Deb M, Parshad R. Abdominal cocoon: report of a case. Surg Today 2000;30:950–3.
9. Hur J, Kim KW, Park MS, Yu JS. Abdominal cocoon: preopera-tive diagnostic clues from radiologic imaging with pathologic cor-relation. Am J Roentgenol 2004;182:639–41.
10. Stafford-Johnson DB, Wilson TE, Francis IR, Swartz R.CT appearance of sclerosing peritonitis in patients on chronic ambu-latory peritoneal dialysis. J Comput Assist Tomogr 1998;22:295–9.
11. Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging fi ndings in 17 patients with emphasis on CT criteria. Radiology 2001;218:68–74.
12. Sayfan J, Adam YG, Reif R. Peritoneal encapsulation in child-hood: case report, embryologic analysis, and review of literature. Am J Surg 1979;138:725–7.
13. Serafi midis C, Katsarolis I, Vernadakis S, Rallis G, Giannopoulos G, Legakis N, et al. idiopathic sclerosing encapsulating peritonitis (or abdominal cocoon). BMC Surg 2006;6:3.
14. Hamaloglu E, Altun H, Ozdemir A, Ozenc A. The abdominal cocoon: a case report. Dig Surg 2002;19:422–4.
15. Deeb LS, Mourad FH, El-Zein YR, Uthman SM. Abdominal cocoon in a man. Preoperative diagnosis and Literature review. J Clin Gastroenterol 1998;26:148–50.
16. Kaushik R, Punia RPS, Mohan H, Attri AK. Tuberculous abdom-inal cocoon — a report of 6 cases and review of the literature. World J Emerg Surg 2006;1:18.





























