Embed Size (px)
Citation preview
Idiopathic Unilateral Corneal Endothelial Failure in Phakic EyesAdrian Tey MBChB, MRCOphth1; Weng Lee FRCSEd(Ophth)2; Hardeep Mudhar BSc,PhD,MBBChir,FRCPath3; Francisco Figueiredo,MD,PhD,FRCOphth1
1. Department of Ophthalmology, Royal Victoria Infirmary, Newcastle, UK ; 2. Hermitage Medical Clinic, Dublin, Ireland ; 3. National Specialist Ophthalmic Pathology Service, Royal Hallamshire Hospital, Sheffield, UK
The authors have no financial interest in the subject matter of this poster
Introduction Bullous keratopathy occurs as a result of corneal endothelial cell
failure and can occur unilaterally or bilaterally. Unilateral bullous keratopathy can be Iatrogenic e.g. following
intraocular surgery, mitomycin C toxicity and laser iridotomies or as a result of pathological diseases e.g. Fuch’s endothelial dystrophy (FED), posterior polymorphous corneal dystrophy (PPD), iridoschisis, iridocorneal endothelial syndrome (ICE), pseudoexfoliation syndrome (PxF) and herpes viruses.
Purpose To describe a cohort of consecutive phakic patients with
progressive, irreversible, unilateral bullous keratopathy (BK) of undetermined aetiology.
Methods Patients presenting to the Royal Victoria Infirmary (United Kingdom
(U.K)) corneal clinic were recruited consecutively from January 1999 to July 2009.
Informed consent was obtained from all patients. Data was collected retrospectively from patient records for
demographics, thorough medical history, slit lamp ocular examination, treatment, pachymetry (Mentor) and Specular microscopy (Non contact Robo Konan, Inc) in 5 zones: central, superior, nasal, inferior and temporal zones.
All penetrating keratoplasties (where required) were performed by a single surgeon (FF) utilising standardised technique.
Corneal buttons following penetrating keratoplasty (PK) were investigated for histology, electron microscopy, immunohistochemistry (IHC) for herpes viral surface antigen, polymerase chain reaction (PCR) and in situ polymerase chain reaction (iPCR) for herpes viral DNA using established protocols1,2.
Aqueous samples were also obtained at the time of surgery for herpes viral DNA analysis.
1. Cohrs RJ, Barbour M, Gilden DH. Varicella-zoster virus (VZV) transcription during latency in human ganglia: detection of transcript mapping to genes 21,29,62, and 63 in a cDNA library enriched for VZV RNA. J. Virol 1996;70(5): 2789-27962. Lewis F. An approach to In Situ PCR manual. PE Biosystems, Foster City, CA, USA.
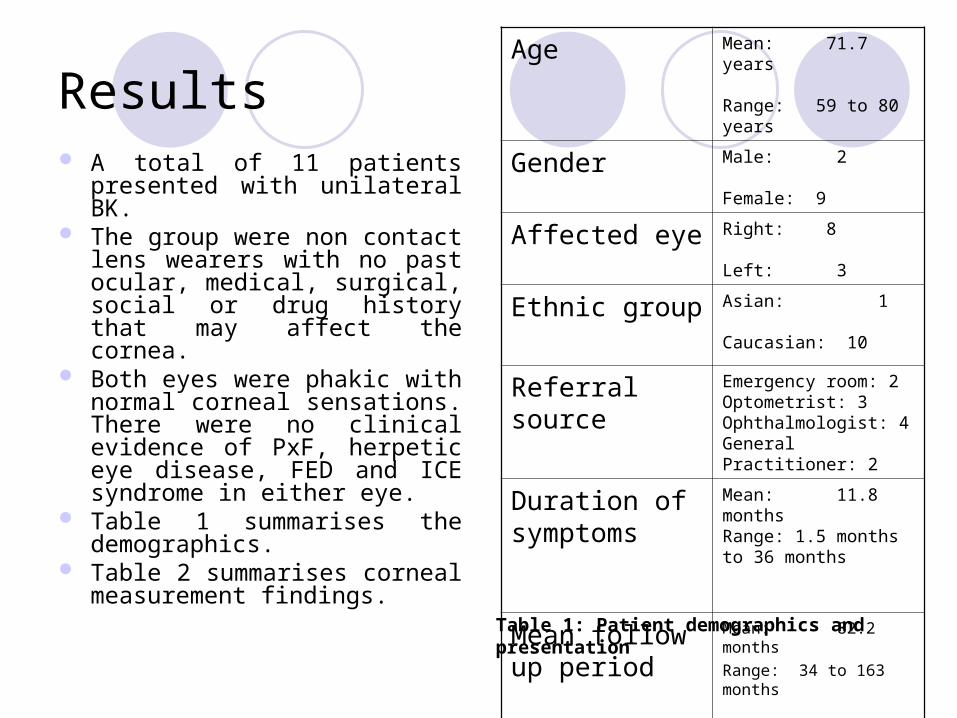
Results A total of 11 patients
presented with unilateral BK. The group were non contact
lens wearers with no past ocular, medical, surgical, social or drug history that may affect the cornea.
Both eyes were phakic with normal corneal sensations. There were no clinical evidence of PxF, herpetic eye disease, FED and ICE syndrome in either eye.
Table 1 summarises the demographics.
Table 2 summarises corneal measurement findings.
Age Mean: 71.7 years Range: 59 to 80 years
Gender Male: 2
Female: 9
Affected eye Right: 8
Left: 3
Ethnic group Asian: 1
Caucasian: 10
Referral source Emergency room: 2Optometrist: 3Ophthalmologist: 4General Practitioner: 2
Duration of symptoms
Mean: 11.8 months Range: 1.5 months to 36 months
Mean follow up period
Mean: 82.2 months Range: 34 to 163 months
Table 1: Patient demographics and presentation
Results
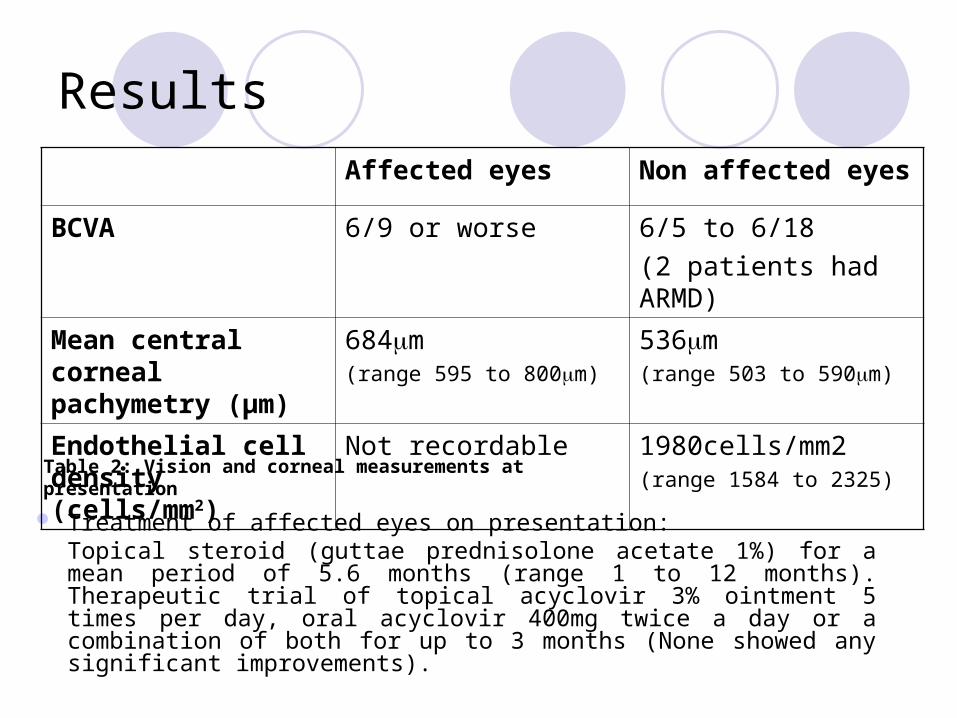
Treatment of affected eyes on presentation: Topical steroid (guttae prednisolone acetate 1%) for a mean period of 5.6 months (range 1 to 12 months). Therapeutic trial of topical acyclovir 3% ointment 5 times per day, oral acyclovir 400mg twice a day or a combination of both for up to 3 months (None showed any significant improvements).
Affected eyes Non affected eyes
BCVA 6/9 or worse 6/5 to 6/18
(2 patients had ARMD)
Mean central corneal pachymetry (µm)
684m (range 595 to 800m)
536m (range 503 to 590m)
Endothelial cell density (cells/mm2)
Not recordable 1980cells/mm2 (range 1584 to 2325)
Table 2: Vision and corneal measurements at presentation
Results 8 affected eyes eventually underwent PK. The interval from disease
onset to PK ranged from 6 to 67 months (mean 22.5 months). There were no peri-operative complications.
The PK group had a post-operative follow up of 16 to 120 months (mean 61.5 months). Table 3 summarises the post-operative course of the 8 patients.
Mean BCVA of grafted eye: 6/18 (range 6/6 to hand movements) Two patients with age related macular degeneration accounted for poor BCVAs of hand movements.
Complications: Controlled secondary glaucoma - 3, Endothelial rejection - 1, Grafts failed - 4 ( 3 primary failure, 1 due to
fungal infection) Only one patient required multiple PKs (2 regrafts). Two patients have since deceased and 1 was discharged back to
the care of the district general hospital.

Table 3: Penetrating Keratoplasty (PK) group
PatientGraftnumber
Post-op follow
up (months)
Duration onset
to PK(months)
Graft Failure / rejection
episodes
Donor endotheliu
m(cells/mm2)
A123
1202116
6126147
Graft failureFungal infection
2600 2500
B 1 108 30 No 2500
C 1 72 28 No 2400
D 1 63 19 Graft failure 2600
E 1 91 10 Graft failure 2600
F 1 74 13 No 2400
G 1 21 67Endothelial rejection x
12800
H 1 29 7 No Not recorded
Results
In the non PK group (n = 3), mean central pachymetry of affected eyes increased by 9.8% to 793m (range 715m to 857m). One patient opted for amniotic membrane transplant for symptomatic BK instead of PK in view of her advanced age related macular degeneration.
Results
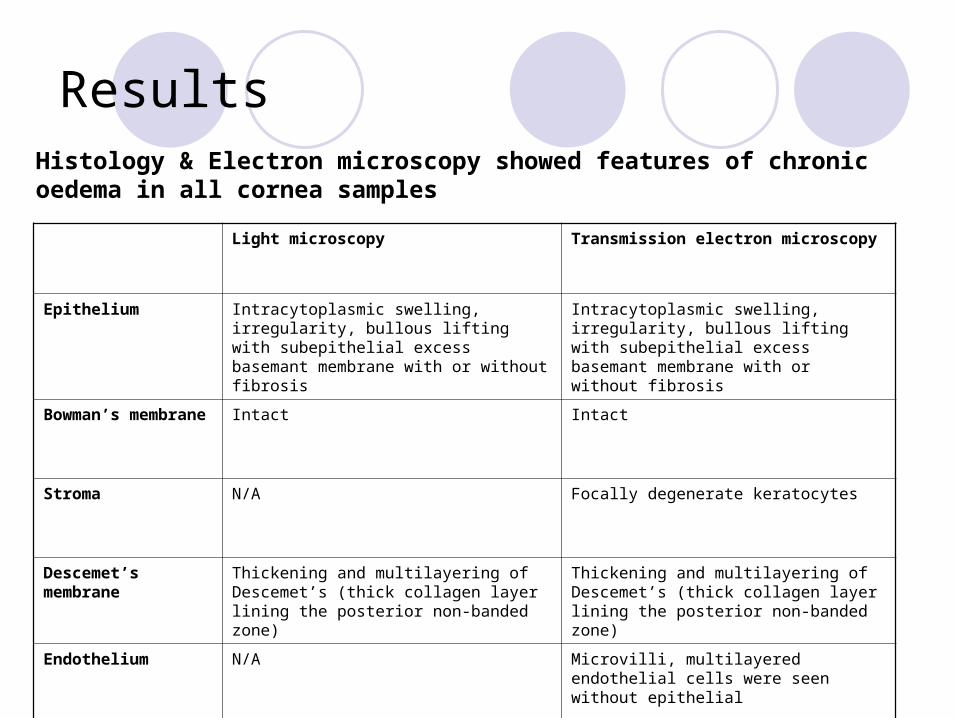
Light microscopy Transmission electron microscopy
Epithelium Intracytoplasmic swelling, irregularity, bullous lifting with subepithelial excess basemant membrane with or without fibrosis
Intracytoplasmic swelling, irregularity, bullous lifting with subepithelial excess basemant membrane with or without fibrosis
Bowman’s membrane Intact Intact
Stroma N/A Focally degenerate keratocytes
Descemet’s membrane
Thickening and multilayering of Descemet’s (thick collagen layer lining the posterior non-banded zone)
Thickening and multilayering of Descemet’s (thick collagen layer lining the posterior non-banded zone)
Endothelium N/A Microvilli, multilayered endothelial cells were
seen without epithelial differentiation
Histology & Electron microscopy showed features of chronic oedema in all cornea samples
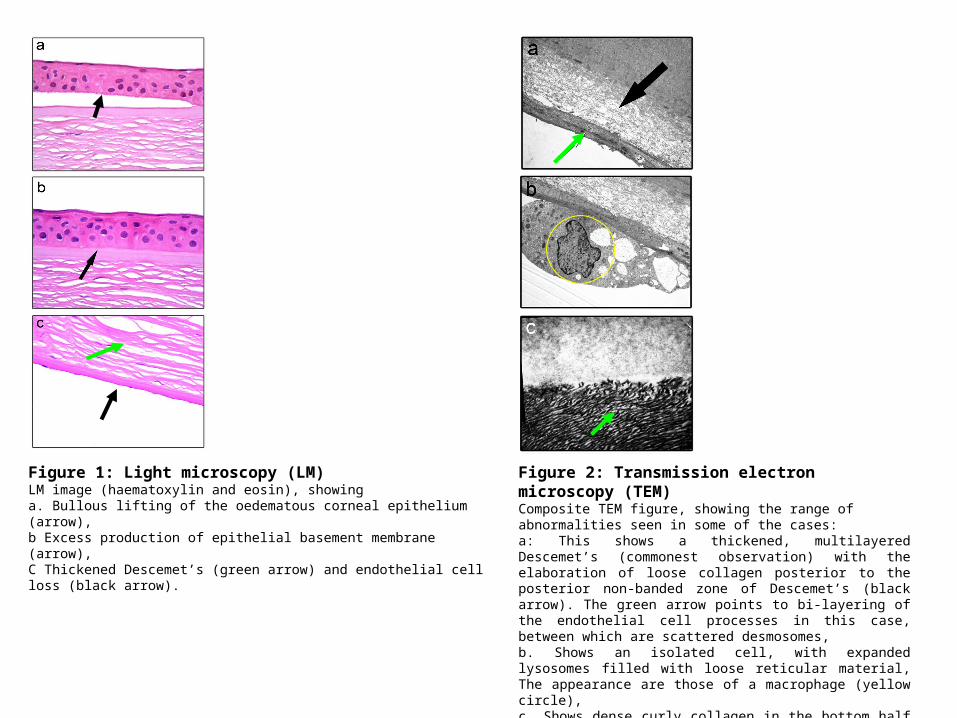
Figure 1: Light microscopy (LM)LM image (haematoxylin and eosin), showing a. Bullous lifting of the oedematous corneal epithelium (arrow), b Excess production of epithelial basement membrane (arrow),C Thickened Descemet’s (green arrow) and endothelial cell loss (black arrow).
Figure 2: Transmission electron microscopy (TEM)Composite TEM figure, showing the range of abnormalities seen in some of the cases:a: This shows a thickened, multilayered Descemet’s (commonest observation) with the elaboration of loose collagen posterior to the posterior non-banded zone of Descemet’s (black arrow). The green arrow points to bi-layering of the endothelial cell processes in this case, between which are scattered desmosomes, b. Shows an isolated cell, with expanded lysosomes filled with loose reticular material, The appearance are those of a macrophage (yellow circle), c. Shows dense curly collagen in the bottom half of the image( green arrow), posterior to the non-banded Descemet’s above.
Results
No virus particles, exfoliation material or guttae were identified. Post-PK (regrafts) corneal buttons showed features of chronic
bullous keratopathy, secondary to chronic endothelial cell loss, with a thickened, multilayered Descemet’s. There were no specific features within the failed grafted tissue that exposed the aetiology of the original corneal disease.
Herpes viral studies on post-PK corneal buttons were negative for all samples. In addition, aqueous humour PCR confirmed absence of any herpes viruses (HSV, VZV and CMV)
Conclusions
Despite extensive investigations and long term follow up, the aetiology of BK for this group of patients remained elusive and remains a diagnostic challenge.
Medical treatment was not beneficial. PK appears to offer a limited prognosis as 2 patients developed early graft endothelial failure and 1 patient required 2 further transplants due to fungal keratitis after the initial PK.
Features of chronic inflammatory component was seen in 2 cases, however, all other cases showed no inflammation and therefore the interpretation of inflammation playing a role is speculative.
Whilst some cases harboured some pathological changes that were reminiscent of CHED and PPD, non of the cases fitted neatly into a distinct diagnostic category.
We speculate that the clinical entity we observed may yet represent previously unreported and currently unknown pathology.












![[ 1 ] - Isleworth and Syon School to Aadi Mudhar (11B), Harry Wells (10E), Quinn Goodliffe (8F) and Cade Nation (9E) for bringing their characters to life with such aplomb. Audience](https://img.pdfslide.net/doc/110x75/5abd2e097f8b9a567c8ea74d/-1-isleworth-and-syon-to-aadi-mudhar-11b-harry-wells-10e-quinn-goodliffe.jpg)
















