Embed Size (px)
Citation preview

MEDICAL ONCOLOGY (1996) 13, 1-7
Idiotype-specific T cells in multiple myeloma: immunotherapeutic intervention?
targets for an
Q I N G YI 1. a n d A N D E R S O S T E R B O R G 2
l lmmunological Research Laboratory and Department of Medicine, and 2Department of Oncology, Karolinska Hospital, S-171 76 Stockholm, Sweden
In this paper, the results of some recent studies on idiotype-specific T cells in human multiple myeloma (MM) and monoclonal gammopathy of undetermined significance (MGUS) are dis- cussed. By using different in vitro measurements such as 3H-thymidine incorporation and ELI- SPOT assay, idiotype-specific T cells have been demonstrated in most of MM and MGUS patients. Based on the cytokine-secretion profiles, idiotype-specihc T cells were found to comprise both Thl and Th2 cells. A Thl type immunity was found preferentially in indolent disease and a Th2-1ike response predominated in advanced MM, suggesting a specific T-cell regulation of the tumor B-cell clone. The mode of T-cell recognition of id determinants on M-components has been studied. We found that idiotype-specific T cells recognized processed id determinants presented by MHC class II (HLA-DR) molecules on APC. B cells were much more efficient APC than monocytes. With the aim to induce or to amplify an idiotype-specific T-cell response, we have immunized MM patients with the autologous M-component precipitated in aluminum. Three out of the five patients showed an induction of specific cellular and humoral immunity. Nevertheless, the role for such immunity in controlling the tumor clone remains to be established.
Keywords: Multiple myeloma; T cells; idiotype; M-component.
INTRODUCTION
Monoclonal g a m m o p a t h i e s such as multiple mye- loma (MM) and monoclonal g a m m o p a t h y of un- de te rmined significance (MGUS), are lymphopro- liferative B-cell disorders. They are characterized by a proliferation of clonal B lymphocytes in var- ious stages of ma tu ra t ion and by plasma-cell in- filtration of the bone m ar row [1]. Without che- motherapy , the med ian survival of MM is less than 1 year [2]. M M patients with a low tumor burden (clinical s tage I) have a long median survi- val (> 5 years) as compared to about 2 years for those with advanced disease. Alkylating agents induce a clinical response in about 50% of MM patients and a med ian survival of about 3 years [3]. Al though p romis ing results have been repor ted with autologous [4] or allogeneic [5] bone mar row
*To whom correspondence should be addressed
or s tem cell t ransplantat ion, MM is still an almost invariably fatal disease. Thus, there is a great need for bet ter t rea tment modalit ies.
In the present paper , the results of some recent studies on tumor idiotype-specihc T-cell immuni ty in h u m a n MM and M G U S are discussed. Such cells might have an impact on the proliferation and differentiation of the mal ignant B-cell clone and might represent an interesting target for an im- munotherapeu t ic in tervent ion in MM.
CLONAL B CELLS IN MM AND MGUS
The monoclonal immunoglobul in (Ig) p roduced by the clonal B cells can usually be demons t ra ted as an M-componen t (M-protein) in p lasma and/or urine. It has unique variable regions in the heavy and light chains. B cells belonging to the tumor clone can be identified by their expression on cell
0736-0118 �9 1996 Chapman & Hall

Id-REACTIVE T CELLS IN MULTIPLE MYEOLOMA
surface of the monoclonal Ig that carries the same idiotypic (id) structures as the M-component [1]. Such monoclonal B cells are present in the bone marrow as well as in peripheral blood. The pre- sence of circulating monoclonal B cells in the peripheral blood in MM and MGUS has been confirmed by cytogenetic analysis [6], and by Southern blot analysis showing clonal rearrange- ment of Ig heavy and light chain genes in blood lymphocytes and in bone marrow plasma cells [7]. Using a highly sensitive polymerase chain reaction (PCR)-based technique, circulating clonal B lym- phocytes were detected in almost all patients with untreated MM [8].
MM could be regarded as a differentiating B-cell malignancy [9-11]. It is not yet known, however, which is the earliest cell belonging to the tumor clone. Recent studies indicate that the neoplastic event may occur in a preswitched (IgM-expres- sing) but already somatically mutated B cell, which may explain the absence of intraclonal variation in MM [12-14]. As malignancy is generally believed to result from a series of stepwise oncogenic events that take place during differentiation [15], it remains to be shown at which stage of differ- entiation the clonal B cells in MM have become fully malignant. Interestingly, it has been reported that myetoma B lymphocytes had a higher prolif- erative activity [16,17] and that they were more resistant to chemotherapy as compared to the myeloma plasma cells [18]. This is further evident in patients who had undergone autologous bone marrow transplantation where minimal residual disease (clonal B cells) remained detectable despite morphological and immunocytochemical evidence of complete remission [19]. Moreover, the pre- sence of clonal B cells in the peripheral blood was reported to be associated with a poor prog- nosis in MM [20], and in patients with MGUS a high risk of developing MM [21]. Thus, new therapeutic approaches aiming to control or eradi- cate the precursor B-cell fraction of the myeloma tumor clone are warranted.
IDIOTYPE-SPECIFIC IMMUNITY IN MURINE MYELOMA
Id structures on the surface Ig of malignant clonal B cells may be regarded as tumor-specific antigens [22], and as such, are potential targets for specific anti-id immunity [22,23]. The proliferation and differentiation of the idiotype-expressing malig- nant B cells might be regulated according to the id network hypothesis [24]. In animal studies, both antibodies (humoral response) and T cells (cellular response) regulating the growth of the myeloma clone by specific recognition of the id antigen have been described [22,23,25,26]. Immunization of
mice with soluble id § Ig protected the animals against a subsequent challenge with id +, but not id-, tumor cells [22]. Anti-id antibodies inhibited plasmacytoma cell growth as well as production of the id § Ig [26], indicating the role of idiotype- specific humoral immunity in controlling growth of tumor cells in the animal model. However, as the excess of circulating M-component may func- tion as an immunological barrier, i.e., blocking anti-id antibodies, the anti-id antibodies are less likely to be efficient effectors in vivo. T cells, on the other hand, generally recognize antigen in the form of processed peptides presented in associa- tion with major histocompatibility complex (MHC) molecules [27,28], and they may not be blocked by circulating id Ig. Thus, T cells may be more potent than antibodies in controlling the tumor B-cell clone. Indeed, this has been shown in animal studies on myeloma and lymphoma [29-31].
T CELLS IN HUMAN MM AND MGUS
Although a relatively low number of peripheral blood T cells in patients with MM and MGUS has been reported [32], the total number of T lympho- cytes was, in most studies, within the normal range [33,34]. A consistent finding was a low CD4/CD8 ratio which was most pronounced in patients with the advanced disease [33,34]. An increase in the CD4§ + subset (suppres- sor/inducer T cells) in MGUS [35] and a low number of these cells in MM [36] have been described. In addition, blood cells (probably CD8 § cytotoxic for autologous plasma cells in a SlCr-release assay [37] and increased number of CD8 + T cells with Fc receptors for the myeloma immunoglobulin isotype [38], have been reported.
The presence of activated (HLA-DR +) T cells in MM patients has been reported [39]. These T cells produced high amounts of interleukin (IL)-2 and interferon (IFN)-q and generated antiplasma cell activity in vitro after CD3 stimulation. More re- cently, the susceptibility to apoptosis in T cells of patients with MM by determining the expression on the cell surface of Fas and bcl-2 antigens was studied by the same group [40]. They found that Fas § cells were significantly higher, whereas bcl- 2 § cells were significantly lower in MM patients than in controls. The percentage of cells in spon- taneous or triggered apoptosis was higher in MM and mainly restricted to HLA-DR + T cells. These findings indicate that MM T cells have a dysregu- lated expression of Fas and bcl-2 antigens that is associated with an enhanced susceptibility to apoptosis.
Janson et al. [41] described expansions of per- ipheral blood T cells in patients with MM and MGUS. With a panel of eight monoclonal antibo-
MEDICAL ONCOLOGY (1996) 13 (1)

YI and (~STERBORG
dies covering about 25% of the T-cell-receptor (TCR) repertoire, a predominant usage of Vc~ and Vfl gene segment products within the CD4 § and CD8 § T cells was found in 40% of the patients. In some patients, up to 50% of all CD8 § or CD4 § T cells respectively were stained with one specific antibody. The functions and specificity of the expanded T cells remain to be established. The heterogeneous pattern of TCR VcdVfl expansions in patients may argue against a superantigen- driven process. A conventional antigen-driven reactivity is more likely and was also supported by an investigation [42] demonstrating in one MM patient the presence of two T-cell clones with TCRs that differed at the nucleotide level but had identical amino acid sequences. A candidate for such antigen may be the unique id structures on the tumor B-cell clone, since it has been shown in animal studies that they act as a tumor-specific antigen [22]. In chronic lymphocyte leukaemia, expanded CD8 § T cells with specific anti-tumor activity has been reported [43]. Also T-cell expan- sions with anti-tumor activity have been described [44] in solid tumors.
IDIOTYPE-SPECIFIC T CELLS IN HUMAN MM AND MGUS
The presence of idiotype-specific T cells in the peripheral blood of patients with MM or MGUS was studied by detecting the stimulation of per- ipheral blood mononuclear cells (PBMC) culti- vated in the presence of the autologous M-compo- nents or their F(ab')2 fragments. Cell stimulation was measured as idiotype-induced incorporation of 3H-thymidine into DNA (cell proliferation) or secretion of cytokines such as IFN-% IL-2 or IL-4 [45]. The number of ceils secreting certain cyto- kines can be enumerated in an enzyme-linked immunospot (ELISPOT) assay [46].
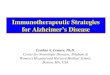
To select the optimal concentrations of M-com- ponents or their F(ab')2 fragments for the stimula- tion of T cells, PBMC were incubated with differ- ent concentrations of the antigens ranging from 0.1pgm1-1 to 10 #gm1-1. As exemplified in Fig. 1, a biphasic dose response was obtained. At low concentrations of the antigen (1-10 pg ml-1), cells from the majority of patients with monoclonal gammopathies responded while fewer cells from healthy individuals were stimulated [47]. The ex- treme low-dose response seems to be typical for id T-cell reactions. A similar pattern of id stimulation of blood lymphocytes from patients with MM and other B-cell tumors was described by measuring 3H-thymidine incorporation [48,49].
By using ELISPOT assays to enumerate IFN-v- and/or IL-2-secreting cells, idiotype-specihc T cells were detected in 90% patients with MM or with
MEDICAL ONCOLOGY (1996) 13 (1)
30
o
z
0,0001 0.001 0,01 0. l 1 10 ICO 1000 100(~
Concentration of F(ab')2 fragment of M-component (ng/ml)
Fig. 1. Stimulated numbers of IFN-3,-secreting cells/ 10 5 PBMC from a patient with MM (shaded) and a healthy individual (unshaded) after incubation with F(ab')2 fragments of the M-component from the pa- tient with MM.
MGUS [47]. Such results were confirmed in an- other of our studies in which two independent in vitro assays: a proliferation assay and an ELISPOT assay for IFN-~f and IL-2, as well as one in vivo test (delayed-type hypersensitivity [DTH]) were em- ployed [50]~ Based on the number of idiotype- induced IFN-3~- or IL-2-secreting cells, the median number of idiotype-specific T cells in the patients was calculated to be about 20/10 s PBMC, corre- sponding to 1/5000 mononuclear cells [47].
Human CD4 + T helper (Th) cells may be sub- divided into at least three subsets based on their cytokine-secretion profiles [51]. Recently, we stu- died the presence of idiotype-specific T-cell sub- sets and their relation to the tumor load in patients with MM and MGUS. An ELISPOT assay was used to identify IFN-"/-, tL-2-, or IL-4-secreting T cells after in vitro stimulation of PBMC by F(ab')2 fragments of the autologous M-component.
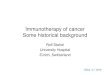
As shown in Fig. 2, the proportion of indivi- duals who had an idiotype-specific response of Thl-type (IFN-'7- and/or IL-2-secreting cells) was significantly higher in patients with indolent
80"
60
40
�9 ":: T~L a T~2 o,?';i !f~ r"2 . .Ly
Subset of Th cells
Fig. 2. Percentage of patients with MGUS (shaded), MM stage I (unshaded) or MM stage II/111 (cross- shaded) who had cells secreting cytokines that cor- responded to different Th subsets.

disease (MGUS and MM stage I) as compared to those of advanced MM (stage II/III). In contrast, cells secreting Th2 type of cytokines (IL-4) were more frequent in patients with MM stage II/HI [52]. These results indicate that a shift from an idiotype-specific T-cell response of the Thl type in early MM to a Th2 type in advanced disease may have occurred, thereby providing indirect evi- dence that idiotype-specific T cells may have a regulatory impact on the human tumor B cells. Whether the IFN-~l-secreting cells also contained CD8 + T cells cannot be ruled out by this study. Notably, both idiotype-specihc CD4 + and CD8 + T cells were suggested to be involved [48].
Experiments in murine plasmacytoma revealed that idiotype-specihc, CD4 + T-cell clones were of both Thl and Th2 type [53]. In vivo experiments showed that both the idiotype-specific Thl and Th2 clones could protect against id § tumor devel- opment in animals. The in vitro studies demon- strated that the Thl, but not the Th2, clones were cytotoxic to id + tumor cells, even though the Th2 clones inhibited the growth of the tumor cells [54]. Taken together, these results indicate that idio- type-specific T cells of different subsets may in- hibit tumor cell growth. Alternatively, idiotype- specific T cells may provide T- to B-cell help, driving the B-cell expansion [55,56]. It may be speculated that T-cell pertubations in MM might precede the development of the expanding B-cell clone [57]. To our knowledge, there is, however, no report of in vivo tumor stimulation by specific T cells in humans, neither in MM nor in other tumors.
~d-REACTIVE T CELLS IN MULTIPLE MYEOLOMA
ANTIGEN PRESENTATION IN IDIOTYPE- INDUCED T-CELL STIMULATION
An important and unresolved question concerns the mode of T-cell recognition of id determinants on Ig. Earlier studies of animal and human sys- tems have yielded conflicting results. Idiotype- specific T cells were in some experiments shown to bind directly to id + Ig molecules [25,58], and that some of the idiotype-specihc T cells were MHC non-restricted [59,60]. More recently, ex- periments with murine plasmacytoma have de- monstrated that idiotype-specific CD4 + T-cell clones recognized only processed peptides of id determinants in the context of MHC class II mole- cules on antigen-presenting cells (APC) [28,61].
We have studied the requirements of molecules and cells involved in T-cell activation induced by F(ab')2 fragments of the autologous M-compo- nents from patients with MM and MGUS. The results showed that idiotype-induced T-cell stimu- lation required the presence of APC (monocytes and/or B cells) (Fig. 3), and was MHC class-II (HLA-DR) restricted (Fig. 4). Antigen processing and presentation were abrogated by treatment of APC with chloroquine (a lysosomotropic agent). Our study also showed that B cells were more efficient APC than monocytes because they re- quired about 1000-fold less antigen than mono- cytes [62]. However, whether MHC class I-re- stricted, CD8 + idiotype-specific T cells are also present in patients with MM or MGUS is still an open question.
c p m
cpm
2500"
1000
PBMC T ceils T§ T+M
C e l l p o p u l a t i o n
Fig. 3. Requirement of monocyte or B cells as APC. Shown is proliferation (cpm) of PBMC, T cells, T cells plus 10% autologous B cells or T cells plus 5% autologous monocytes in the presence of 1 ng ml -~ (shaded) or 10#g m1-1 (unshaded) of F(ab')2 frag- ments of the autologous M-component.
O,O! 0,1 1 10 1(%O 1000 100(30
Concentration of F(ab')2 fragment of M-component ( n g / m l )
Fig. 4. Inhibition of anti-HLA-DR antibody on the idiotype-induced cell proliferation. PBMC were incu- bated in the presence of different concentrations of the autologous F(ab')2 fragments with (unshaded) or without (shaded) the addition of 2 #g ml -~ of a mouse anti-HLA-DR antibody.
MEDICAL ONCOLOGY (1996) 13 (1)

YI and ~)STERBORG
Table 1. Enhancement of anti-id T and B cell responses and decrease in the number of CD19 § B cells in five MM patients during immunization with the autotogous M-component
Patients Anti-id Anti-id Decrease of T cells B cells CD19 § B cells
1 + + +
2 + + + 3 - - -
4 - - -
5 + + -
I N D U C T I O N / A M P L I F I C A T I O N OF ANTI - ID I M M U N I T Y I N V I V O
If idiotype-specific T cells can regulate the growth and differentiation of id + tumor B cells, a thera- peutic intervention aiming to expand such T cells with cytotoxic or suppressive effects on the tumor B-cell clone may be a rewarding approach. Active immunization using the autologous monoclonal Ig as 'vaccine' may confer resistance to tumor cell challenge in transplantable murine B-cell lympho- ma and myeloma [22,63,64]. Trials in human B-cell lymphoma [65] have revealed an induction of humoral and cell-mediated idiotype-specific re- sponse with occasional tumor regressions. How- ever, emergence of antigen (idiotype)-negative tumor variants, either spontaneously [66] or as a consequence of idiotype-specific therapy, have been reported in B-cell lymphoma [67]. From this point of view, MM may be a particularly suitable disease for an active immunotherapy, since the B- cell clone seems to be stable in terms of absence of ongoing somatic mutat ion [11,68].
Recently, we have completed an active immu- nization protocol in patients with previously un- treated asymptomatic MM [69]. Five stage I-III patients were repeatedly immunized with the autologous M-component precipitated in alumi- num phosphate suspension. Induction of idio- type-specific cellular immuni ty was analysed in
vi tro by an ELISPOT assay (IFN-'~- and IL-4-secret- ing cells). B cells secreting anti-id antibodies of the IgM class were also analysed. In three out of five patients, an anti-id T-cell response was amplified 1.9- to 5-fold during the immunization. The num- ber of B cells secreting anti-id antibodies also increased in these patients, and two of the three patients had a gradual decrease of blood CD19 + B cells (Table 1). However, the induced T-cell re- sponse was transient, and it was eliminated dur- ing repeated immunizations. These results indi- cate that it may be possible to augment an idio- type-specific immuni ty in v ivo in MM patients. Further studies are warranted to optimize the
MEDICAL ONCOLOGY (1996) 13 (1)
immunizat ion schedule in order to achieve a long-lasting T-cell immuni ty against id determi- nants on the tumor clone.
Id immunizat ion may also be used in allogeneic bone marrow transplantation. Kwak and cowor- kers [70] immunized an HLA-identical sibling marrow donor with the patient's(recipient's) M- component, and showed that idiotype-specihc T- cell immuni ty was successfully transferred to the recipient. Also in this experiment, the transferred anti-id T-cell immuni ty was transient (< 60 days), indicating that booster immunizations of the reci- pient may be required to maintain the anti-tumor immunity.
REFERENCES
1 Mellstedt, H., Holm, G. and Bj6rkholm, M. (1984) Multiple myeloma, Waldenstr6m's macroglobulinemia, and benign monodonal gammopathy: characteristics of the B cell done, immunoregulatory cell populations and clinical implications. Adv. Cancer Res. 41, 257-89.
20sgood , E.E. (1960) The survival time of patients with plasmacytic myeloma. Cancer Chemther. Rep. 9, 1-10.
3 Alexanian, R., Haut, A., Khan, A.U. et al. (1969) Treatment for multiple myeloma. Combination chemotherapy with different melphalan close regimens. JAMA 208, 1680-85.
4 Harousseau, J.-L., Attal, M., Divine, M. et al. (1995) Auto- logous stem cell transplantation after first remission induc- tion treatment in multiple myeloma: a report of the French registry on autologous transplantation in multiple myeloma. Blood 85, 3077-85.
5 Gahrton, G., Tura, S., Ljungman, P. et al. (1991) Allogeneic bone marrow transplantation in multiple myeloma. N. Engl. J. Med. 325, 1267-73.
6 MacKenzie, M.R. and Lewis, J.P. (1985) Cytogenetic evi- dence that the malignant event in multiple myeloma occurs in a precursor lymphocyte. Cancer Genet. Cytogenet. 17, 13-20.
7 Berenson, J., Wong, R., Kirn, K. et al. (1987) Evidence of peripheral blood B lymphocyte but not T lymphocyte involvement in multiple myeloma. Blood 70, 1550-3.
8 Billadeau, D., Quam, L., Thomas, W. et al. (1992) Detection and quantitation of malignant ceils in the peripheral blood of multiple myeloma patients. Blood 80, 1818-24.
90sterborg, A., Steinitz, M., Lewin, N. et al. (1991) Establish- ment of idiotype bearing B-lymphocyte clones from a patient with monoclonal gammopathy. Blood 78, 2642-9.
10 Bergui, L., Schena, M., Gaidano, G. et al. (1989) Interleukin 3 and interleukin 6 synergistically promote the prolifera- tion and differentiation of malignant plasma cell precur- sors in multiple myeloma. J. Exp. Med. 170, 613-8.
11 Takishita, M., Kosaka, M., Goto, T. et al. (1994) Cellular origin and extent of clonal involvement in multiple mye- loma: genetic and phenotypic studies. Br. J. Haematol. 87, 73542.
12 BiUadeau, D., Ahmann, G., Greipp, P. et al. (1993) The bone marrow of multiple myeloma patients contains B cell populations at different stages of differentiation that are clonally related to the malignant plasma cell. J. Exp. Med.
.178, 1023-31. 13 Bakkus, M.H., van Riet, I., Camp, B.V. et al. (1994) Evi-
dence that the clonogenic cell in multiple myeloma origi- nates from a pre-switched but somatically mutated B cell. Br. J. Haemtol. 87, 68-74.
14 Vescio, R.A., Cao, J., Hong, C.H. et aL (1995) Myeloma !g

6
heavy chain V region sequences reveal prior antigenic selection and marked somatic mutation but not intraclonal diversity. J. Irnmunol. 155, 2487-97.
15 Fearon, E.R. and Vogelstein, B. (1990) A genetic mode for colorectal tumorigenesis. Cell 61, 759-67.
16 Mellstedt, H., Killander, D. and Pettersson, D. (1977) Bone marrow kinetic studies on three patients with myeloma- tosis: indications for malignant proliferation within both the plasma cell and lymphoid cell compartments. Acta Med. Stand. 202, 413-7.
17 Chan, C:S., Wormsley, S.B., Pierce, L.E. et al. (1990) B-cell surface phenotypes of proliferating myeloma cells: target antigen for immunotherapy. Am. J. Hematol. 33, 101-9.
18 Pilarski, L.M. and Belch, A.R. (1994) Circulating monoclo- nal B cells expressing P glycoprotein may be a reservoir of multidrug-resistant disease in multiple myeloma. Blood 83, 724-36.
19 Corradini, P., Voena, C., Astolh, M. et al. (1995) High-dose sequential chemoradiotherapy in multiple myeloma: resi- dual tumor cells are detectable in bone marrow and per- ipheral blood cell harvests and after autografting. Blood 85, 1596-1602.
20 Osterborg, A., Nilsson, B., Bjo~kholm, M. et al. (1987) Blood clonal B cell excess at diagnosis in multiple myeloma. Relation to prognosis. Eur. J. Haematol. 38, 173-8.
21 Isaksson, E., Bj6rkholm, M., Holm, G. et al. (1996) Blood clonal B-cell excess in patients with monoclonal gammo- pathy of undetermined signihcance (MGUS): association with malignant transformation. Br. J. Haematol. 92, 71-6.
22 Lynch, R.G., Graff, R.J., Sirisinha, S. et al. (1972) Myeloma proteins as tumor-specific transplantation antigens. Proc. Natl. Acad. Sci. USA 69, 1540-4.
23 Stevenson, F.K., George, A.J.T. and Glennie, M.J. (1990) Anti-idiotypic therapy of leukemias and lymphomas. Chem. Immunol. 48, 126-66.
24 Jerne, N.K. (1974) Towards a network theory of the immune system. Ann. Immunol. (Inst. Pasteur), 125C, 373-89.
25 Lynch, R.G. (1987) Immunoglobulin-specihc suppressor T cells. Adv. Immunol. 40, 135-51.
26 Mahony, J., Bose, A., Cowdrey, D. et al. (1981) A mono- clonal antiidiotypic antibody to MOPC 315 IgA inhibits the growth of MOPC 315 myeloma cells in vitro. J. lmmunol. 126, 113-7.
27 Germain, R.N. (1994) MHC-dependent antigen processing and peptide presentation: providing ligands for T lympho- cyte activation. Cell 76, 287-99.
28 Bogen, B., Malissen, B. and Haas, W. (1986) Idiotype- specihc T cell clones that recognize syngeneic immunoglo- bulin fragments in the context of class II molecules. Eur. J. Immunol. 16, 1373-8.
29 Daley, M.J., Gebel, H.M. and Lynch, R.G. (1978) Idiotype- specific transplantation resistance to MOPC-315: abroga- tion by post-immunization thymectomy. J. ImmunoL 120, 1620-4.
30 Flood, P.M., Philipps, C., Taupier, M.A. et al. (1980) Reg- ulation of myeloma growth in vitro by idiotype-specihc T lymphocytes. J. ImmunoL 124, 424-30.
31 Hornung, R.L., Longo, D.L., Bowersox, O.C. et al. (1995) Tumor antigen-specific immunization of bone marrow transplantation donors as adoptive therapy against estab- Lished tumor. J. Natl Cancer Inst. 87, 1289-96.
32 Bergman, L., Mitrou, P.S., Kelker, W. et al. (1985) T-cell subsets in malignant lymphomas and monoclonal gammopathies. Scand. J. Haematol. 34, 170-6.
33 Mellstedt, H., Holm, G., Pettersson, D. et al. (1982) T cells in monoclonal gammopathies. Scand. J. Haematol. 29, 57-64.
34 San Miguel, J.F., Caballero, M.D. and Gonzalez, M. (1985) T-cell subpopulations in patients with monoclonal gam- mopathies: essential monoclonal gammopathy, multiple myeloma, and Waldenstrom macroglobullnemia. Am. J. Hematol. 20, 267-73.
Id-REACTIVE T CELLS IN MULTIPLE MYEOLOMA
35 Shapira, R., Froom, P., Kinarty, A. el al. (1989) Increase in the suppressor-inducer T cell subset in multiple myeloma and monoclonal gammopathy of undetermined significance. Br. J. Haernatol. 71, 223-5.
36 Serra, H.M., Mant, M.J., Ruether, B.A. et al. (1988) Selec- tive loss of CD4+CD45R + T cells in peripheral blood of multiple myeloma patients. J. Clin. Immunol. 8, 259-65.
37 Paglieroni, T. and MacKenzie, M.R. (1979) In vitro cytotoxic response to human myeloma plasma cells by peripheral blood leukocytes from patients with multiple myeloma and benign monoclonal gammopathy. Blood 54, 226-37.
38 Hoover, R.G., Hickman, S., Gebel, H.M. et al. (1981) Expansion of Fc receptor-bearing T lymphocytes in pa- tients with immunoglobulin G and immunoglobulin A myeloma. J. Clin. Invest. 67, 308-11.
39 Massaia, M., Attisano, C., Peola, S. et al. (1993) Rapid generation of antiplasma cell activity in the bone marrow of myeloma patients by CD3-activated T cells. Blood 82, 1787-97.
40 Massaia, M., Borrione, P., Attisano, C. et al. (1995) Dysre- gulated Fas and Bcl-2 expression leading to enhanced apoptosis in T ceils of multiple myeloma patients. Blood 85, 3679-87.
41 Janson, C.H., Grunewald, J., Osterborg, A. et al. (1991) Predominant T cell receptor V gene usage in patients with abnormal clones of B cells. Blood 77, 1776-80.
42 Moss, P.A.H., Gillespie, G., Frodsham, P. et al. (1994) Clonal populations of CD4 and CD8 T cells in patients with paraproteinaemia and myeloma. Blood 84 (suppl. 1), 177a (abstr.).
43 Farace, F., Orlanducci, F., Dietrich, P-Y. et al. (1994) T cell repertoire in patients with B chronic lymphocytic leukemia. J. Immunol. 153, 4281-90.
44 Sensi, M.L. and Parmiani, G. (1995) Analyses of TCR usage in human tumors: a new tool for assessing tumor specific immune responses. Immunol. Today 16, 588-95.
45 Hecht, T.T., Longo, D.L. and Matis, L.A. (1983) The rela- tionship between immune interferon production and pro- liferation in antigen-specific, MHC-restricted T cell lines and clones. [. Immunol. 131, 1049-55.
46 Czerkinsky, C.C. , Andersson, G., Ekre, H.P. et al. (1988) Reverse ELISPOT assay for clonal analysis of cytokine production. I. Enumeration of gamma-interferon-secreting cells. J. Immunol. Meth. 110, 29-36.
47 Yi, Q., Bergenbrant, S., Osterborg, A. et al. (1993) T-cell stimulation induced by idiotypes on monoclonal immuno- globulins in patients with monoclonal gammopathies. Scand. J. Immunol. 38, 529-34.
48 Osterborg, A., Masucci, M., Bergenbrant, S. et al. (1991) Generation of T cell clones binding F(ab~)2 fragments of the idiotypic immunoglobulin in patients with monoclonal gammopathy. Cancer Immunol. Immunother. 34, 157-62.
49 Holm, G., Bergenbrant, S., Lefvert, A.K., Yi, Q. etal. (1991) Anti-idiotypic immunity as a potential regulator in myelo- ma and related diseases. Ann. N Y Acad. Sci. 636, 178-83.
Osterborg, A., Yi, Q., Bergenbrant, S. et aL (1995) Idiotype- specific T cells in multiple myeloma stage I: an evaluation by four different functional tests. Br. J. HaematoL 89, 110-6.
Romagnani, S. (1991) Human TH1 and TH2 subsets: doubt no more. Immunol. Today 12, 256-7.
Yi, Q., Osterborg, A., Bergenbrant, S. et al. (1995) Idiotype- reactive T-cell subsets and tumor load in monodonal gammopathies. Blood 86, 3043-9.
Lauritzsen, G.F. and Bogen, B. (1991) Idiotype-specific, major histocompatibility complex restricted T cells are of both Thl and Th2 type. Scand. J. Immunol. 33, 647-56.
Lauritzsen, G.F., Weiss, S. and Bogen, B. (1993) Anti-tumor activity of idiotype-specihc, MHC-restricted Thl and Th2 clones in vitro and in vivo. Scand. [. Immunol. 37, 77-85.
Clark, E.A. and Ledbetter, J.A. (1994) How B and T cells talk to each other. Nature 367, 425-8.
MEDICAL O N C O L O G Y (1996) 13 (1)
50
51
52
53
54
55

YI and OSTERBORG
56 Hilbert, D.M., Shen, M-Y., Rapp, U.R. et al. (1995) T cells induce terminal differentiation of transformed B cells to mature plasma cell tumors. Proc. Natl. Acad. Sci. USA 92, 649-53.
57 Paglieroni, T., Caggiano, V. and MacKenzie, M. (1992) Abnormalities in immune regulation precede the develop- ment of multiple myeloma. Am. J. Hematol. 40, 51-5.
58 Dianzani, U., Pileri, A., Boccadoro, M. et aI. (1988) Acti- vated idiotype-reactive cells in suppressor/cytotoxic sub- populations of monoclonal gammopathies: correlation with diagnosis and disease status. Blood 72, 1064-8.
59 Bottomly, K. and Mosier, D.E. (1981) Antigen-specihc help- er T cells required for dominant idiotype expression are not H-2 restricted. J. Exp. Med. 154, 411-21.
60 Parra, C.C., Lima, M.S., Gazzinelli, G. etal. (1988) Immune responses during human Schistosomiasis Mansoni. XV. Anti-idiotypic T cells can recognize and respond to anti- SEA idiotypes directly. J. Immunol. 140, 2401-5.
61 Yamamoto, H., Araki, K., Bitoh, S. et al. (1987) Cytotoxic T lymphocyte clone recognizing self idiotype: its regulatory role in antibody production. Eur. J. Immunol. 17, 719-22.
62 Yi, Q., Holm, G. and Lefvert, A.K. (1996) Idiotype-induced T cell stimulation requires antigen presentation in associa- tion with HLA-DR molecules. Clin. Exp. Immunol. 104, 359- 650.
63 George, A.J.T., Folkard, S.G., Hamblin, T.J. et al. (1988) Idiotypic vaccination as a treatment for a B cell lymphoma. J. Immunol. 141, 2168-74.
64 Kwak, L.W., Campbell, M. and Levy, R. (1991) Idiotype
7
vaccination post-bone marrow transplantation for B-cell lymphoma: initial studies in a murine model. Cancer Detec. Prev. 15, 323-5.
65 Kwak, L.W., Campbell, M., Czerwinski, D.K. et al. (1992) Induction of immune responses in patients with B-cell lymphoma against the surface-immunoglobulin idiotype expressed by their tumors. N. Engl. J. Med. 327, 1209-15.
66 Raffeld, M., Necker, L., Longo, D.L. et al. (1985) Sponta- neous alteration of idiotype in a monoclonal B-cell lym- phoma: Escape from detection by anti-idiotype. N. Engl. J. Med. 312, 1653-8.
67 Maloney, D.G., Brown, S., Czerwinski, D.K. et al. (1992) Monoclonal anti-idiotype antibody therapy of B-cell lym- phoma: the addition of a short course of chemotherapy does not interfere with the antitumor effect nor prevent the emergence of idiotype-negative variant cells. Blood 80, 1502-10.
68 Bakkus, M.H.C., Heirman, C., van Riet, I. et al. (1992) Evidence that multiple myeloma Ig heavy chain VDJ genes contain somatic mutations but show no intraclonal variation. Blood 80, 2326-35.
69 Bergenbrant, S., Yi, Q., Osterborg, A. et al. (1996) Modula- tion of anti-idiotypic immune response by immunization with the autologous M-component protein in multiple myeloma patients. Br. J. Haematol. 92, 840-6.
70 Kwak, L.W., Taub, D.D., Duffey, P.L. et al. (1995)Transfer of myeloma idiotype-specihc immunity from an actively immunised marrow donor. Lancet 345, 1016-20.
MEDICAL O N C O L O G Y (1996) 13 (1)