Embed Size (px)
Citation preview
If We’re Serious About Recidivism, How Can We Reduce the Gap in Service Provision?
Faye S. Taxman, Ph.D.Stephanie A. Ainsworth, M.A.Erin L. Crites, M.A.Center for Advancing Correctional Excellence (ACE!)George Mason University
Avinash Singh Bhati, Ph.D. Maxarth, LLC
James M. Byrne, Ph.D.April Pattavina, Ph.D.Department of Criminal Justice and Criminology University of Massachusetts, Lowell
Edward Banks, Ph.D. Knowledge Management Coordinator Bureau of Justice Assistance
July 26, 2011

2
Acknowledgements
•Bureau of Justice Assistance•Center for Substance Abuse Treatment•Public Welfare Foundation

3
•Client is arrested for a DWI with a BAC of .15
•Classified as low risk based on agency’s validated risk assessment instrument
•Workshop instructor states that individual should be treated as a high risk for supervision purposes based on the high BAC.

4
The REAL Problem• Lots of ways to do correctional programming, but no
set principles
• Risk and Needs are often confused
• There are no clear guidelines about assigning offenders to controls or treatment
• The guidelines can be recidivism based, if we had the data
• The RNR is complicated and hard to follow

5
Learning Objectives• Rate Your Population
▫ Identify the factors associated with offending
• Effective Interventions▫ Identify how to appropriately respond to those factors
to reduce recidivism and improve offender outcomes
• Rate Your Programs▫ Identify appropriate program options to reduce
correctional costs without jeopardizing public safety
• Town Hall Discussion
6
Rate Your Population: Factors Associated with Offending
• Empirically Based▫ Static Risk▫ Criminogenic Need>>>Dynamic Risks>>>>Linked to Criminal
Behavior Drug Dependency Criminal lifestyle
• Clinically Relevant▫ Destabilizers
Drug Abuse or Alcohol Dependence Mental Health History
▫ Stabilizers No Criminal Networks (friends & family) Stable Housing Full-Time Employment Family Support Education

7
Simplify the Criteria:
•Risk: Identify Offenders with an Extensive and Early Onset Criminal History (Static Risk Level)
•Need #1: Identify Offenders who are Drug Dependent or who Present Multiple Criminal Lifestyle Factors (Criminogenic Need Level)
•Need #2: Identify Offenders with Potential Destabilizing and Stabilizing Factors

Static RiskStep One: Know the Risk Level

9
Risk Principle: High- to Moderate-Risk offenders should be prioritized for placement in treatment and control programs• Offenders vary by level of probability of recidivism –
Static Risk
• Risk is static or unidirectional▫ Risk stays the same or increases; it can not be reduced
• Risk factors are gathered from criminal history information▫ Age at first arrest, number of prior arrests, number of
prior probation/parole events, number of probation/parole revocations, attempted/successful escapes from custody

10
Risk Level (Classification 1)
Low Risk Moderate Risk High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
53.6%
66.0%
77.2%
24.1% 52.2% 23.7%

11
Discussion
•What is the biggest struggle when considering static risk?▫For you, for your agency?
•Where does risk fall short?

Criminogenic NeedsReducing the Complexity

13
Need Principle: Criminogenic Needs should be the primary focus of treatment, control and programming
•Criminogenic Needs are dynamic factors & link with offending behavior
•Reducing criminogenic needs reduces recidivism
•Target the key ones, and consider severity

14
Contributes to Criminal Behavior
Psy
choso
cial
fun
ctio
nin
g
Antisocial PeersSubstance AbuseFamily CJ InvolvementLocation (Crime Area)Low Self ControlAntisocial Values
Criminal PersonalitySubstance Dependence
Mental HealthEmploymentEducationHousing Family Dysfunction
Criminogenic Needs
*Items in boxes are included in our data measures

15
Easily Identifiable Criminogenic Needs• Drug Dependence
▫ Early age of first use of drugs, regular use of drugs associated with offending behavior (criminogenic drugs - crack, cocaine, heroin, other opiates, methamphetamine, other amphetamines), use of criminogenic drugs at time of offense
• 3+ Criminal Lifestyle Indicators▫ Criminal Networks
Family or friends engaged in criminal activity
▫ Family Support Lack of visits, calls, or mail from children while incarcerated; receiving
financial support from family members prior to arrest
▫ Employment Not employed full time prior to arrest
▫ Education Less than a high school diploma
▫ Housing Unstable (homeless) prior to arrest
▫ Offenders who present 3+ have higher need and should be targeted for more intensive services.

16
What do we know about Criminogenic Needs
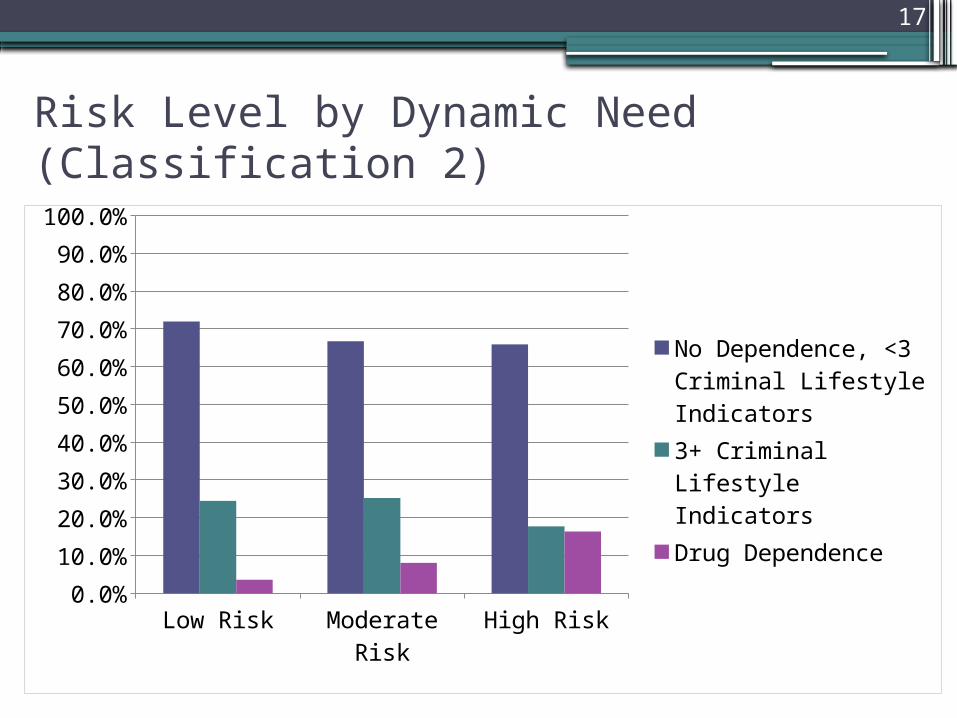
•~9% of the prison and jail sample present with drug dependence
•24.7% have 3 or more criminal lifestyle needs
17
Risk Level by Dynamic Need (Classification 2)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
No Dependence, <3 Criminal Lifestyle Indicators3+ Criminal Lifestyle IndicatorsDrug Dependence
18
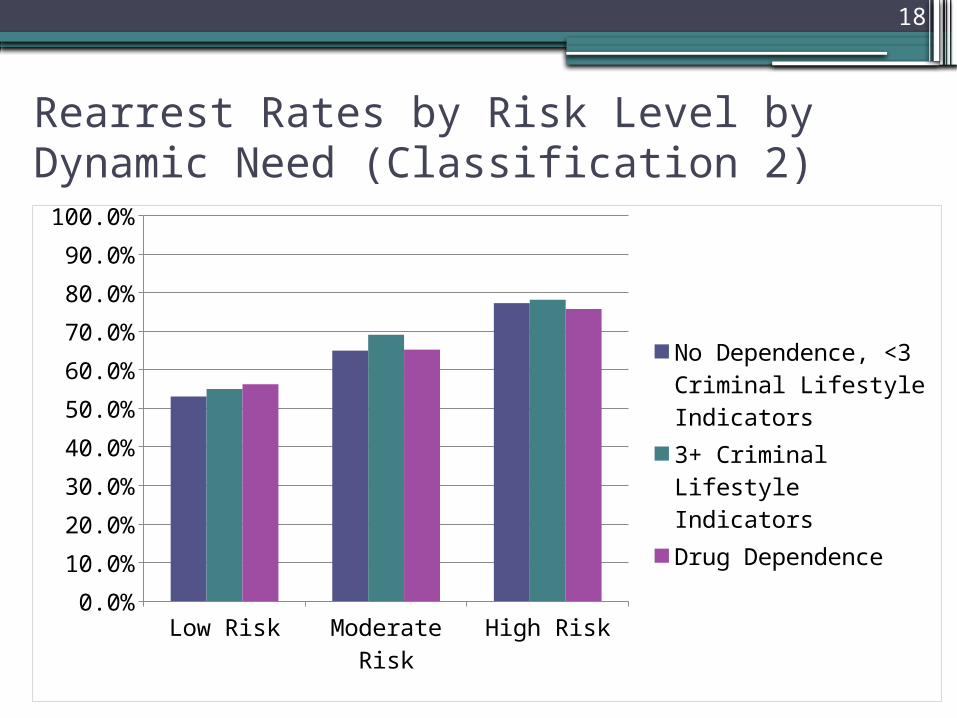
Rearrest Rates by Risk Level by Dynamic Need (Classification 2)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
No Dependence, <3 Criminal Lifestyle Indicators3+ Criminal Lifestyle IndicatorsDrug Dependence
19
BUT… there are other variables which are clinically relevant
• Drug Abuse/Alcohol Dependence▫Older age of first use, non-regular use of criminogenic
drugs, use of drugs at time of arrest, (but not criminogenic drugs)
▫Age of first drink, drinking at time of arrest, arrested because of alcohol use, disruptions to work or relationships due to alcohol use.
• Mental Health History▫Ever diagnosed with a MH disorder, ever taken
medication for mental condition, ever admitted to or stayed overnight in a mental health hospital, ever received counseling from a trained professional, ever received other mental health treatment services
20
Presence of Destabilizer
•71.3% of the prison and jail sample report drug abuse or alcohol dependence▫69% report both drug abuse and alcohol
dependence
•6.3% report a history of mental health concerns

21
Risk and Destabilizers for Drug Dependent Individuals (Classification 3)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Drug Dependent, No DestabilizersDrug Dependent, 1 DestabilizerDrug Dependent, 2 Destabilizers
22
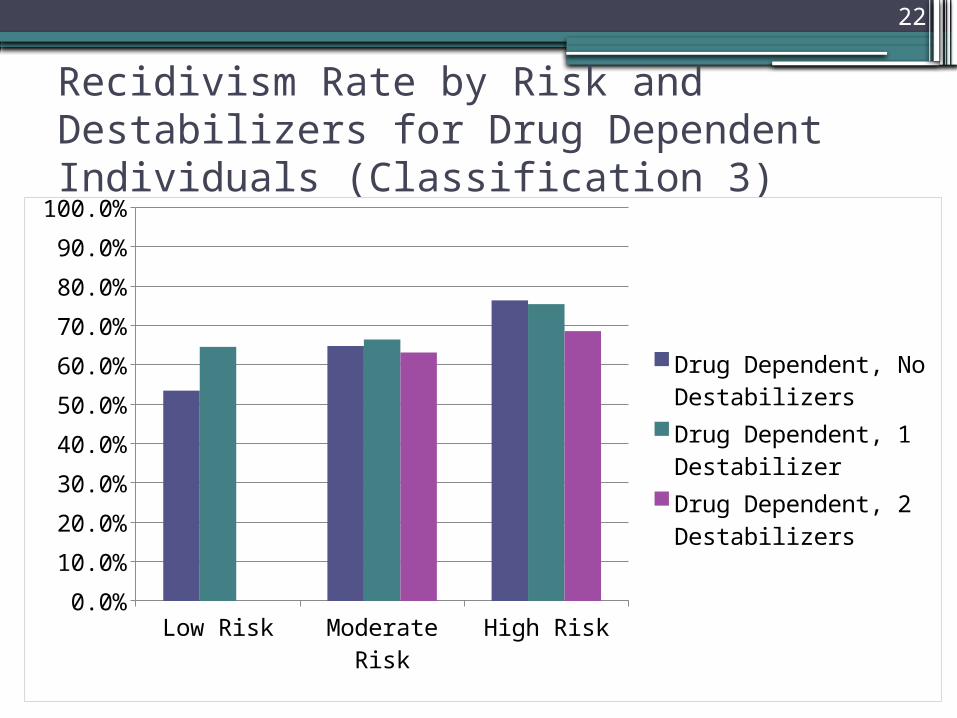
Recidivism Rate by Risk and Destabilizers for Drug Dependent Individuals (Classification 3)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Drug Dependent, No DestabilizersDrug Dependent, 1 DestabilizerDrug Dependent, 2 Destabilizers

23
Risk and Destabilizers for Individuals with 3+ Criminal Lifestyle Indicators (Classification 3)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
3+ Criminal Lifestyle Indicators, No Destabilizers3+ Criminal Lifestyle Indicators, 1 Destabi-lizer3+ Criminal Lifestyle Indicators, 2 Destabi-lizers

24
Rearrest Rates by Risk and Destabilizers for Individuals with 3+ Criminal Lifestyle Indicators (Classification 3)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
3+ Criminal Lifestyle Indicators, No Destabilizers3+ Criminal Lifestyle Indicators, 1 Destabi-lizer3+ Criminal Lifestyle Indicators, 2 Destabi-lizers

25
Rearrest Rates by Risk by Need by Destabilizer (Classification 3)
No
Nee
ds, N
o Des
tabi
lizer
s
No
Nee
ds, 1
Des
tabi
lizer
No
Nee
ds, 2
Des
tabi
lizer
s
3+ C
rim
Life
styl
e In
dica
tors
, No
Des
tabi
lizer
s
3+ C
rim
Life
styl
e In
dica
tors
, 1 D
esta
biliz
er
3+ C
rim
Life
styl
e In
dica
tors
, 2 D
esta
biliz
ers
Subs
tanc
e Dep
ende
nt, N
o Des
tabi
lizer
s
Subs
tanc
e Dep
ende
nt, 1
Des
tabi
lizer
Subs
tanc
e Dep
ende
nt, 2
Des
tabi
lizer
s0.00%
10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
100.00%Low Risk
Moder-ate Risk
26
Reflection
•Does this match what you see in practice?
•What other factors are important?

27
Stabilizers
•Family Support•Educated•Full-time employment•Lack of Criminal Networks•Stable Housing
**Considered in good shape with 4+ present
• 43.6% of the combined prison and jail sample report having 4+ stabilizing indicators

28
Risk by Stabilizer for (classification 4)
Low Risk Moderate Risk High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
<4 Stabilizers
4+ Stabilizers

29
Rearrest Rates by Risk by Stabilizer for (classification 4)
Low Risk Moderate Risk
High Risk0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
<4 Stabilizers
4+ Stabilizers

So What is Responsivity?The Program Categories

31
Responsivity Principle: matching of clients to programs and supervision based on their identified risks and needs.
•Balance between supervision to respond to risk and treatment programming to address needs.
•Program setting, dosage, implementation, philosophy, and quality important influences on outcomes.

32
Program Characteristics• Restriction-restrictions (including the setting of the
program) are viewed as tools used by criminal justice agents to assist in stabilizing, monitoring, and supporting offenders in their efforts to change their behavior
• Dosage-combination of frequency, length of sessions, duration of the intervention, and length of aftercare
• Content-use of empirically supported treatment philosophies and evidence based practices.
• Fidelity-principles of effective interventions including integrity and quality (Lowencamp, Latessa, & Smith, 2009)Lowenkamp, C. T., Latesa, E. J. & Smith, P. (2008). Does correctional program quality really matter? The impact of adhering to the
principles of effective intervention. Criminology and Public Policy, 5, 575-594.

33
Intensive Daily
Restrictions
Punishment Only
Moderate Daily
Restrictions
Low Daily Restrictions
Low
M
od
era
te
H
igh
Liberty Restrictions by Risk LevelR
isk
Leve
l

34
• Identify promising correctional programs supported by the literature
• Meta-analytic techniques are the strongest evidence since they summarize the literature
• ACE! “collaboratory” to identify and code systematic reviews to identify known effect sizes
• To date Aos, Miller, and Drake (2006) have identified multiple promising programs including: CBT-based programs, adult drug courts, and Therapeutic Communities followed by aftercare.
Aos, S., Miller, M., & Drake, E. (2006). Evidence-Based Public Policy Options to Reduce Future Prison Construction, Criminal Justice Costs and Crime Rates. Olympia: Washington State Institute for Public Policy.
Content

35
Expected Reductions in Recidivism• Programs:
▫ CBT and CBT based programs (6.8%-31.2%)a
▫ Therapeutic Communities (5.3% no aftercare to 6.9% with aftercare) a
▫ Specialized Courts (10.7% drug courts) a
▫ Sex Offender Treatment▫ Intensive Manualized Drug Treatment▫ Half Back Programs▫ Outpatient Drug Treatment
• Supervision Tools▫ Electronic Monitoring▫ Motivational Interviewing▫ Drug Testing▫ Intensive Supervision (17.9%-21.9% when paired with treatment)a
Aos, S., Miller, M., & Drake, E. (2006). Evidence-Based Public Policy Options to Reduce Future Prison Construction, Criminal Justice Costs and Crime Rates. Olympia: Washington State Institute for Public Policy.

36
Program Categories• Category A: Intensive daily restrictions on behavior with 3+ hours a day in
a setting; deals with High Risk and Substance Abuse Dependent or 3+ Criminogenic Needs.
• Category B: Moderate daily restrictions on behavior with services multiple times a week; deals with High Risk with <3 Criminogenic Needs
• Category C: Low daily restrictions on behavior with multiple times a month services; deals with Moderate Risk with Drug Dependence or 3+ Criminogenic Needs
• Category D: Weekly restrictions on behavior; for Moderate Risk with Drug Use or Alcohol Dependence and Low Risk with 3+ Criminogenic Needs or Drug Dependence
• Category E: Weekly restrictions on behavior for Low Risk with Drug Use or Alcohol Dependence
• Category F: Punishment only for Low Risk with <3 Criminogenic Needs
37
Program Category A
• Includes individuals classified as high risk with drug dependence or 3+ criminal lifestyle factors.
• Approximately 4.7% of the sample
• Programs include: ▫ CBT-3 or more hours per day, 5 days per week, for at least 90 days, plus
aftercare.▫ Therapeutic community- 3 or more hours per day, 5 or more days per week,
for at least 9 months, in a highly structured environment, plus community based reentry services and tapered aftercare.
▫ Specialized court- 3 hours per day, five days a week, at least 12 months.▫ Intensive manualized drug treatment-at least 3 hours per day, five days a
week, at least 9 months.▫ Sex offender treatment-at least 3 hours daily, combining intensive individual
and group counseling as appropriate. ▫ Half-back programs-at least 3 hours per day.
• Supervision tools: used to manage compliance and address public safety.

38
Program Category B• Includes individuals classified as high risk with <3 criminogenic needs
• Approximately 9.3% of the sample
• Programs include:▫ CBT based programming-one or more hours at least 2-4 times weekly,
lasting about 90 days, followed by aftercare.▫ Specialized court-lasting at least 12 months.▫ Intensive manualized drug treatment-2 or more hours session, 3 or more
days per week, at least 9 months. ▫ Sex offender treatment-at least 2 hours per session, at least 3 days a
week, combining intensive individual and group counseling as appropriate.
▫ Work release—behavior restricted when not engaged in employment-related activities outside of the facility.
▫ Educational, vocational, or employment-2-4 days a week for at least 2 hours each session .
• Supervision tools used to manage compliance and address public safety (lower levels of restriction from A).

39
Program Category C• Includes individuals classified as moderate risk with drug dependence or
3+ criminogenic needs
• Approximately 18.8% of the sample
• Programs include:▫ CBT based programming-1+hours per week, lasting about 90 days.▫ Educational, vocational, or employment programs that include activities
once per week for 1+hours each session. ▫ Specialized court-1+ hours per session weekly, lasting at least 6 months,
could be supported by more frequent group treatment sessions as needed.▫ Manualized drug treatment-1+ hours per session, weekly extends for 6
months and could be supported by more frequent group substance abuse sessions as needed.
▫ Sex offender treatment-2+ hours, at least weekly and combining intensive individual and group counseling as appropriate.
• Supervision tools used to manage compliance and address public safety (lower levels of restriction from B).

40
Program Category D• Includes individuals classified as moderate risk with drug use
or alcohol dependence and low risk with 3+ criminogenic needs or drug dependence
• Approximately 23.5% of the sample.
• Programs include:▫ Outpatient drug treatment-at least 1 hour/week on a weekly
basis, which may be supported by attendance at group substance abuse treatment sessions or at self-help groups.
▫ Substance abuse group counseling at least weekly. ▫ CBT based programming-one hour/week lasting about 90 days.▫ Educational, vocational, or employment programs that include
activities once per week for around 1 hour each session.
• Supervision tools used to manage compliance and address public safety (lower levels of restriction from C).

41
Program Category E• Includes individuals classified as moderate risk with no substance use or
criminogenic needs (with stabilizers) or low risk with drug use or alcohol dependence.
• Approximately 37.4% of the sample.
• Programs include:▫ Substance abuse group counseling 2-3 times per month, as needed. ▫ Psycho-educational services.▫ Drug/alcohol abuse/use education.▫ CBT based programming-one hour about 2-3 times per month, and over the
course of at about 90 days ▫ Educational, vocational, or employment programs that include activities as
needed. ▫ Referrals for treatment services or community educational/vocational,
literacy, ESL or other such programs with no or limited requirments for attendance
• Supervision tools used to manage compliance and address public safety (lower levels of restriction from D).

42
Program Category F
• Includes individuals classified as low risk with <3 criminogenic needs.
• Approximately 6.2% of the sample.
• Includes fines, community service, restitution, shock incarceration, and other criminal justice sanctions with the sole purpose of being punitive and retributive.
• Likely to include some form of supervision, but with no additional services to assist the offender in managing criminogenic needs.

43
A B C D E F0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Low RiskModerate RiskHigh Risk
Percent of Program Category within Static Risk Level

44
A B C D E F0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Low RiskModerate RiskHigh Risk
Percent Rearrested by Program Category and Static Risk Level-Actual Rates with No Programming

45
Discussion
•Do the program categories clarify the differences seen in risk levels?
•Questions?
46
Next Steps
•Establish expected reductions in recidivism following appropriate program placement.
•Expanding data to include pre-trial, diversion, and probation samples using SCPS data.
•Pilot model with data from multiple jurisdictions.
•Model can be used at the individual or jurisdictional level.
47
Faye S. Taxman, Ph.D.University ProfessorCenter for Advancing Correctional Excellence
(ACE!)Criminology, Law and Society George Mason University10519 Braddock Road Suite 1900Fairfax, VA 22032
Stephanie A. Ainsworth, M.A.Graduate Research AssistantCenter for Advancing Correctional Excellence
(ACE!)Criminology, Law and Society George Mason University10519 Braddock Road Suite 1900Fairfax, VA 22032
Erin L. Crites, M.A.Graduate Research AssistantCenter for Advancing Correctional Excellence
(ACE!)Criminology, Law and Society George Mason University10519 Braddock Road Suite 1900Fairfax, VA 22032
Avinash Singh Bhati, Ph.D. Maxarth, LLC 509 Cedar Spring St.,Gaithersburg, MD 20877
James M. Byrne, Ph.D.ProfessorDepartment of Criminal Justice and
Criminology University of Massachusetts, Lowell1 University Avenue,Lowell, MA 01854
April Pattavina, Ph.D.Associate ProfessorDepartment of Criminal Justice and
Criminology University of Massachusetts, Lowell1 University Avenue,Lowell, MA 01854
Edward Banks, Ph.D. Knowledge Management Coordinator Bureau of Justice Assistance810 Seventh Street NW., Fourth FloorWashington, DC 20531