Embed Size (px)
Citation preview
If you only have 5 minutes…PHYSICAL ASSESSMENT PEARLS
Barb Bancroft, RN, MSN, PNP
The patient history
• The most important part of any patient assessment is the patient history…
• Components of the history are numerous, but remember, since you ONLY have FIVE minutes, a detailed 2-hour history is not possible
• Pick and choose the parts of the present and past history that are relevant to their current problem
For example…
• Someone with new onset muscle aches and pains on a statin drug vs. someone who starts a statin drug but has had muscle aches and pains for 15 years
• New onset cough since the drug lisinopril was prescribed for hypertension, or has the patient had the cough for 6 years from asthma and hay fever
What is the patient telling you in his/her own words?
• “I’ve had a terrible cough for 3 weeks…”• “I can’t catch my breath…”• “I am having awful pain in my chest…”• “My head feels like it’s going to explode…”• “My ankle is swollen…”• “I’ve got this shooting pain down the back of my
leg…”• “My cat bit me and my hand is swollen…”
To characterize the “chief complaint” start with the PQRST mnemonic
• P—Precise location? Where?• Pinpoint the location? Show me…• Precipitate the problem? What were you
doing when it started?• Palliate the problem? Did anything help?
History
• Patient: “My shoulder hurts”• Nurse: “Show me where it hurts, point to where it
hurts”• Patient pointing to the shoulder joint: ”It hurts right
here…”• Nurse: “Do you know what caused your shoulder to
hurt?”• Patient: “ George hit me with a baseball bat…”
Nurse: “duh…no wonder it hurts…”
History
• Patient rubbing the area of the shoulder next to the neck: “My shoulder hurts…”
• Nurse: “Do you know what caused your shoulder to hurt?”
• Patient: “It started hurting when I smashed into the car in front of me and I slammed into the steering wheel…”
• Nurse: “uh-oh…”• Why “uh-oh?...more in a minute
To characterize the “chief complaint” start with the PQRST mnemonic
• Quality of the pain? Help them out with this one…is it deep,
burning, lancinating (shooting), cramping, crushing, vice-like, sharp, dull, explosive…
• Quantitiy of the (blood, vomit, sputum)? Is it a teaspoon (size of your first thumb joint)? Is it a cup? Quart?
Q is for quantity…
• CC—”spitting up gunk from my lungs”—chronic bronchitis (daily production of a tablespoon or more of sputum every day for at least 2 months in 2 successive years vs. bronchiectasis, a chronic, advanced inflammation with intermittent production of purulent sputum in large quantities, as much as a quart/day
To characterize the “chief complaint” start with the PQRST mnemonic
• Radiate? Where does it go? Up the jaw? Down the arm? One side of the head? To the back? Down the back of the leg? To the groin?
• Referred pain? Embryologic origins of pain
Referred pain
• Embryologic origins• The diaphragm (C3,4)• The phrenic nerve• Shared afferents with the shoulder• What causes diaphragmatic irritation?• Above and below the diaphragm
Referred pain – another example
• The ureters, kidney stones and the scrotum• Does a woman have a scrotum?
To characterize the “chief complaint” start with the PQRST mnemonic
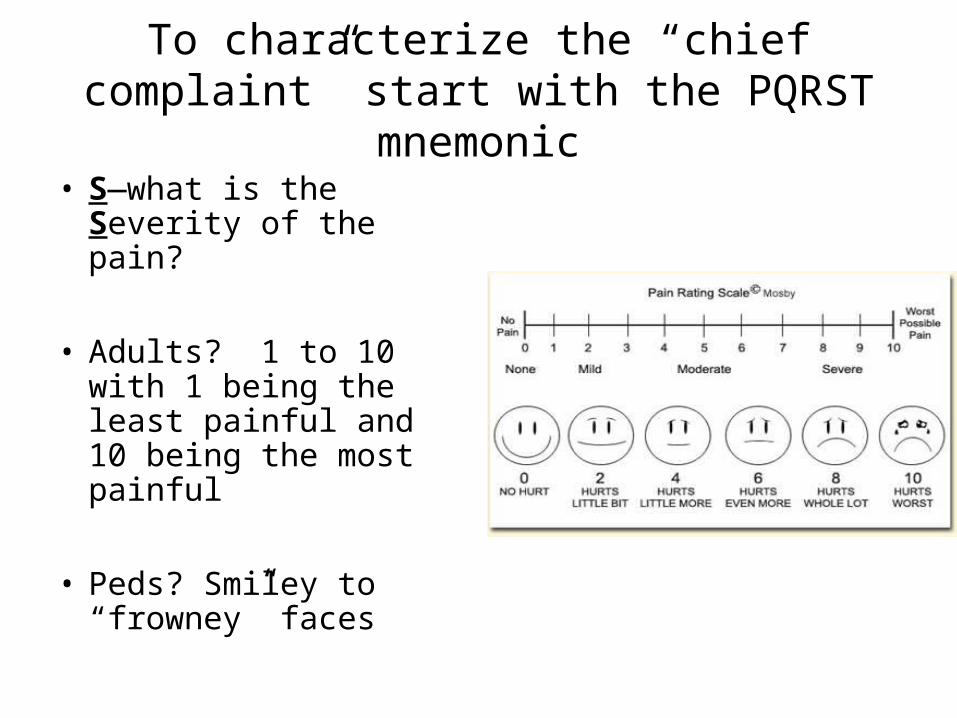
• S—what is the Severity of the pain?
• Adults? 1 to 10 with 1 being the least painful and 10 being the most painful
• Peds? Smiley to “frowney” faces
To characterize the “chief complaint” start with the PQRST mnemonic
• T—what is the Time frame or Temporal sequence?
• Clarify which symptom came first and the order in which others follow. Temporal relationships between associated symptoms are also most helpful. The simultaneous occurrence of equally intense symptoms or the development of symptoms while others regress suggest pathophysiologic mechanisms which in turn imply specific diagnoses
Time or Temporal sequence
• Did the pain last for an hour, 15 minutes, 5 minutes, or less than 5 minutes?
• Did the pain start before you vomited? After you vomited? Did the vomiting stop the pain?
• Symptoms persisting for years are unlikely to be caused by a catastrophic infection, cancer, or other illness
Temporal sequence and an ischemic stroke
• Patients may wake up with a “stroke in progress…” • You have a 4.5 hour “window” to give tissue
plasminogen activator (alteplase)…• You need to know WHEN the stroke symptoms
started?• Bed at 11? Woke up at 7 with symptoms?• Bed at 11? Woke up at 5, perfectly fine, to go to the
bathroom? Woke up again at 7 with symptoms?
The A’s…Associated symptoms , Absent symptoms or events or ALARM symptoms
• What else can you tell me about your problem? Has anything happened in your life that you think might be related to your fatigue?
• My mom passed away…my husband is in Iraq…my boyfriend dumped me…all my kids have the flu”, everybody in my family has diabetes…”
• Nausea, vomiting, weight loss, blurred vision, cough…”worst headache I have every had…”
Chief complaint… “Severe chest pain for 25 minutes”—first thought? Is this an acute coronary syndrome?
• FIRST THINGS FIRST: Any patient with a suspected acute coronary syndrome should chew 160-325 mg of ASA; one simple therapy is associated with a 35-day mortality reduction exceeding 20%)
• Now, think…what structures are located in the chest and how should I go about considering this specific patient with chest pain?
Evaluation of chest pain…
• Cardiac—Acute coronary syndrome (MI, angina), pericarditis, aortic dissection, MVP
• Pulmonary—pulmonary embolism, pleuritis, pneumothorax, pneumonia
• GI—esophageal spasms, GERD, esophagitis, gall bladder
Evaluation of chest pain…
• Musculoskeletal—costochondritis, muscle strain, rib fracture (falls, or trauma, cough, cancer)
• Neurologic—herpes zoster (“band-like” pain may precede vesicular eruption)
• Psychological—panic disorder, depression• Subphrenic causes—usually subdiaphragmatic
So, use the PQRST + AA• Start with the P’s…Pinpoint the pain, what is the
precise location?• LEVINE sign…fist held over sternum is pretty
classic for angina or an MI• Swooping the hand from the back, under the
axillary region and to the front may indicate a neuropathy
• Moving the fingers up and down from the bottom of the sternum to the top may indicate heartburn/GERD
What precipitated the pain?
• Exertion? What were you doing when the chest pain started? How long did it take before the chest pain started? Shoveling snow? Raking leaves? Usually a 5-minute delay (Lag time) for cardiac pain. Did the pain start as soon as you picked up the shovel or the rake? Did you just have a fight with your boss? Did the pain start during sex?
• Digression: Can you have a heart attack during sex?
• ONLY IF YOU’RE HAVING SEX WITH SOMEONE YOU SHOULDN’T BE HAVING IT WITH!!!
• Usually NOT if it’s your same old, same old partner…
First question for any male (from 20 to 120 years old) with chest pain…(whether it’s during sex or not)
• When was your last dose of an erectile dysfunction drug?
• Sildenafil (Viagra)(24)• Tadalafil (Cialis)(36-48)• Vardenafil (Levitra)(24)
Remember…
• The combination of an ED drug with a nitrate can be deadly
• Tell the whole truth, nuttin’ but the truth!!
25
Back to the P’s
• What palliates the pain?• Stopping the activity? How long did it take
before the chest pain stopped when you ceased the activity?
• Did you put a little white pill under your tongue? If so, how many and how long did it take for the pain to stop?
• Did you take an antacid?
Quality or Quantity
• What is the Quality of the pain? Throbbing, burning, shooting, squeezing, crushing?
Radiate/Referred
• Where does it Radiate? Front, back, side, down arm, up to the jaw?
• Is it Referred pain?
Severity
• What is the severity of the pain…
• On a scale from 1-10, with 1 being the least and 10 being “outta control”—where do you rank pain on this scale?
• Angina 5 or 6• MI—9 or 10 or greater
Timing or Temporal sequence
• Temporal sequence; Timing• When did it start? • How long did it last? • How often do you experience this type of
pain?• What’s unique about the time of day and an
acute coronary syndrome?
PQRST
• Any additional symptoms? • Sweating? Nausea? Fatigue?• Dizziness? Light-headedness • Dyspnea (cardiac or respiratory)?? BNP test
(B-type natriuretic peptide—under 100 pg/mL rules out cardiac failure; greater than 500 pg/ rules in CHF)
• The feeling of impending doom…
What is the age of the patient? Sex?
• 38 y.o. female with chest pain?• Quick questions to rule OUT a myocardial infarction
in a young woman…what is her risk of having an MI at age 32?
• Family history• Diabetes• Birth control pills? Obesity? Surgical menopause?• Autoimmune disease? SLE, RA, vasculitis• Methamphetamine, cocaine, other drugs
How does coronary heart disease present in women?
• The studies on heart disease were all done in VA hospitals
• Hello?• Sexual bias? White
men, 176 pounds, 45 years old
How does coronary heart disease present in women?
• Atypical pain is more common in women than men, because of the higher prevalence among women of less common causes of ischemia, such as vasospastic and microvascular angina, and syndromes of nonischemic chest pain such as mitral valve prolapse, panic attacks, esophageal spasms
The evaluation of chest pain in women
• Heart attack warning signs for women—instead of crushing pain in the chest (40% DON’T have crushing chest pain), they may have:
• Fatigue or extreme tiredness• SOB• N & V, cold sweats• Flushing, dizziness• Jaw pain, abdominal pain, elbow pain• Flu-like symptoms• Symptoms that last for hours or days or even a
month before the myocardial infarction
What about a…
• 38 y.o. male with chest pain? Family history? Illicit drugs?
• 68 y.o. female with classic chest pain? Most likely an ACS due to age…onset of menopause?
• 58 y.o. diabetic male with sweating, nausea, hypotension and the feeling of impending doom? Assume heart attack until proven otherwise…silent ischemia due to vagal neuropathy
Medical History? How much time do you have? What is relevant to current episode?
• Allergies• Drug list—prescription, OTC, illegal• Prior surgeries or illnesses (but only if related
to this episode)• Family history• Social history (if an STD is relevant)• Smoking and drinking• Dietary history (weight loss or weight gain)
ALARM SIGNS
• Headache in the early morning vs. headache in the late afternoon when the kids get home from school
• Cough with hemoptysis and weight loss• Chest pain with nausea and diaphoresis• GERD with unexplained weight loss
How about a quick review of vital signs?
• Weight is a vital sign in the elderly• Unexplained weight loss • Consider?• Depression, hyperthyroidism, $, GI, tremor,
oral problems, swallowing, dementia, low salt/low fat diets, infection, cancer
• Weight loss and drugs
Weight gain
• Weight gain and drugs (antidepressants, antipsychotics)
• Weight gain and heart failure
Kids and growth
• Asian children? African-American children? Latino children?
• Weight and growth parameters• Premies?• Breast fed babies gain weight more slowly
Kids and growth
• Growth occurs in a step-wise pattern• Vertical growth occurs during sleep when GH
is released during the late stages of SWS• Tonsillitis, adenoiditis and growth retardation• Do kids have growing pains at night?
Vertical growth and Iron
• Iron is essential for vertical growth• Iron deficiency anemias in kids• Consider celiac disease
Temperature patterns in the elderly
• Loss of diurnal variation• May not rise as rapidly with infections or as high• A rise of greater than 3 degrees Fahrenheit within 2
hours—consider sepsis• Patients on neuroleptic drugs (dopamine blockers)—
c/o “cold”
Temperature patterns in the elderly
• Difficulty maintaining internal temperatures with extremes of ambient temperature
• “You’re not dead until you’re warm and dead.”
• The thyroid gland – myxedema coma (end-stage hypothyroidism)
• ALARM SIGN: hypothermia in a septic patient
Other temperature facts…
• Once antibiotics have been started, the finding of an unusually prolonged fever (longer than 72 hours) indicates:
1)either that the diagnosis of infection was incorrect (the patient instead has a connective tissue disorder or cancer)
2)or that the patient has one of several complications such as resistant organisms, superinfection, drug fever, or an abscess requiring surgical drainage
Drug fever—greater than 102ºF (39º C)
• Antibiotics may cause a drug fever after 5 days of administration
• Drug allergy—look for a macular rash;• Check the WBC and differential (increased
eosinophils)• If the child has been on AB for 4-5 days and
the fever goes back up, check for “bands” on the WBC for re-infection with bacteria
Drug fever
• Penicillin• Cephalosporins• Amphotericin B• Tagamet• Anticholinergics• Neuroleptic fever
Heart rate
• Unexplained tachycardia (greater than 100)—consider hyperthyroidism, dehydration, atrial fibrillation, autonomic neuropathy with the loss of the vagus nerve in diabetics (results in silent ischemia)
• Bradycardia (less than 55)—hypothyroidism, dig, beta blockers, calcium channel blockers such as verapamil/diltiazem
• Bradycardia and a fever?
Heart rate, pulses
• Important to take a pulse for at least 30 seconds for patient with an arrhythmia, but a full minute is more accurate
• With a 15-second pulse you’ll be off by 4 beats and with only a 10-second pulse you’ll be off by at least 6 beats
Heart rate in kids
• Very labile in kids; more sensitive to the effects of illness, exercise, and emotions
• 1-2 years (120)• 4-8 years (100)• 10-12 years (75)• Check radial with femoral (more valuable in older infants and
toddlers; in infants a PDA may shunt blood to the lower extremities, bypassing a severe coarctation (M>F)
Heart rate
• Beta-2 agonists for bronchodilation in asthmatics may cause tachycardia even tho’ they are beta-2 specific
• Tremor and saturation of B-2 receptor sites
Respirations
• Fever and tachypnea in the older adult—consider an acute pulmonary syndrome--pulmonary embolism or pneumonia
Rapid, deep breathing (acidosis)—KUSMAL mnemonic
• Ketones (DKA?)• Uremia• Salicylates• Metabolic (consider thyroid)• Alcohol• Lactic acidosis—CHF, sepsis
Blood pressure
• What is ideal? 120/80• May be slightly higher in the elderly to avoid
hypotension, fainting, and a broken hip (especially in diabetics on hypoglycemic meds)
• Keeping the blood pressure BELOW 140/90 prevents strokes, MIs, renal failure and DAT
• Lying down, sitting, and standing if possible
Blood pressure meds and physical assessment pearls
• Beta blockers (“olols, alols, ilols”)—cold feet, hair loss, decreased heart rate (10-15%), exercise intolerance
• Thiazide diuretics—electrolyte imbalances (especially sodium and potassium), confusion, blood sugar may rise
BP medications and physical assessment pearls
• ACE inhibitors (“prils”)—dry, hacking cough, hypoglycemia, hyperkalemia (muscle aches and pains), angioedema “Does my voice sound funny to you?”
• Calcium channel blockers (“dipines”)—peripheral edema, headaches
• Calcium channel blockers (verapamil)--constipation
In the geriatric patient…always consider medications as a possible source of their chief
complaint• Muscle aches and pains? Statins? ED drugs?• Constipation?• Burning in esophagus? Bisphosphonates? Did
a pill “stick”?• Confusion? Lots of drugs…
“Nurse, I have the worst headache, can you give me something for pain?
• P• Q• R• S• T• Associated symptoms• Absent signs and symptoms• ALARM symptoms
The many causes of headache
• Migraine• Tension• Cluster• Brain tumor (or any other space-occupying lesion, such as
subdural hematoma)• Sleep apnea (early a.m. along with carbon monoxide
poisoning, and space-occupying lesion)• Hangover• Hypertension• Caffeine withdrawal post surgery
Physical exam
• My left ankle is swollen, my right ear hurts…• RULE OF THUMB…always examine the “good”
side first• Right ear? Look at the left ear…• Left ankle? Examine the right ankle…• Neuro exam – symmetry is the rule; check
from “side-to-side”
Inspection
• In most instances, look (inspect) and feel (palpate) before you listen...exception is the abdominal exam—look, listen, and then palpate
• Inspect the area to be examined—are there lesions, lumps, bumps, pulsations, color changes
Skin
• Generalized changes—turgor (elderly—loss of extracellular water AND loss of skin elasticity), texture (coarse, dry, fine), color (increased pigmentation, decreased pigmentation, patchy (vitiligo), generalized (hemochromatosis, cyanosis, jaundice)
• Localized changes—distribution, arrangement and types of lesions
Skin
• Distribution—areas rich in keratinization such as elbows, knees, and scalp may be involved with diseases that disrupt keratinization such as psoriasis
• Moist areas—superficial fungal infections• Sun-exposed areas—skin cancers, precancerous
lesions
Skin
• Selective involvement—dermatitis under a watchband strap, areas that are taped during medical care suggest a hypersensitivity to the tape adhesive or elastic
• Arrangement of the lesions—along a dermatome (neurologic)
Skin
• Linearity of a lesion— scratching is the most common cause,
contact dermatitis (poison ivy); remember blood vessels and lymphatics run
along the long axis of the legs and arms—inflammatory lesions may produce red linear lesions
Types of skin lesions
• Papule (solid elevated lesion, less than 1 cm)—goose bumps, drug “rash”
• Plaques—larger flat elevations, extends deeper into dermis (psoriasis)
• Nodules—extend deeper into the dermis and are round, oval, or elliptical—may indicated systemic disease (malignancy)
• Wheals—edema fluid in upper dermis; pale red; small or large and frequently pruritic (hives)
Skin
• Vesicles (<0.5 cm) and bullae (> 0.5 cm)—fluid-filled elevations (lymph, blood, serum)—HSV-1, HSV-2, VZV (chickenpox, shingles)
Skin conditions
• Hyperthyroidism—fine, smooth, moist, flushed• Hypothyroidism—dry, scaly, thick• Addison’s disease—increased ACTH (w/MSH) in
primary hypoadrenalism—darkening of knuckles, freckles, areola, buccal mucosa, lips, gums (JFK)
• Fixed drug eruption—usually within 1 week of the drug and may occur up to 2 weeks after the drug is d/cd; maculopapular, erythematous, on the trunk and pressure points
• vonRecklinghausen’s disease
Skin cancers
• Squamous cell carcinoma• Basal cell carcinoma• Malignant melanoma
Cardiovascular exam
• “Do not be in a hurry to listen to the heart. The most important sounds you will hear are the words of the patient as he presents the history…” Burnside JW. Physical Diagnosis, 17th edition.
• Family history is important (early onset heart disease, strokes, PAD; diabetes, hypertension)
• Personal history: Date of onset of heart disease, rheumatic fever as a child, coarctation, “blue baby”, poor feeder, trouble keeping up with peers in physical activity, DM, HTN
• Social history—smoking, cocaine or meth use, IV drug, dietary history
The 7 common primary heart diseases are:
• congenital • ischemic • hypertensive • valvular • pulmonary heart disease• primary disorders of the myocardium (cardiomyopathies)• pericardial diseases (pericarditis, tamponade)
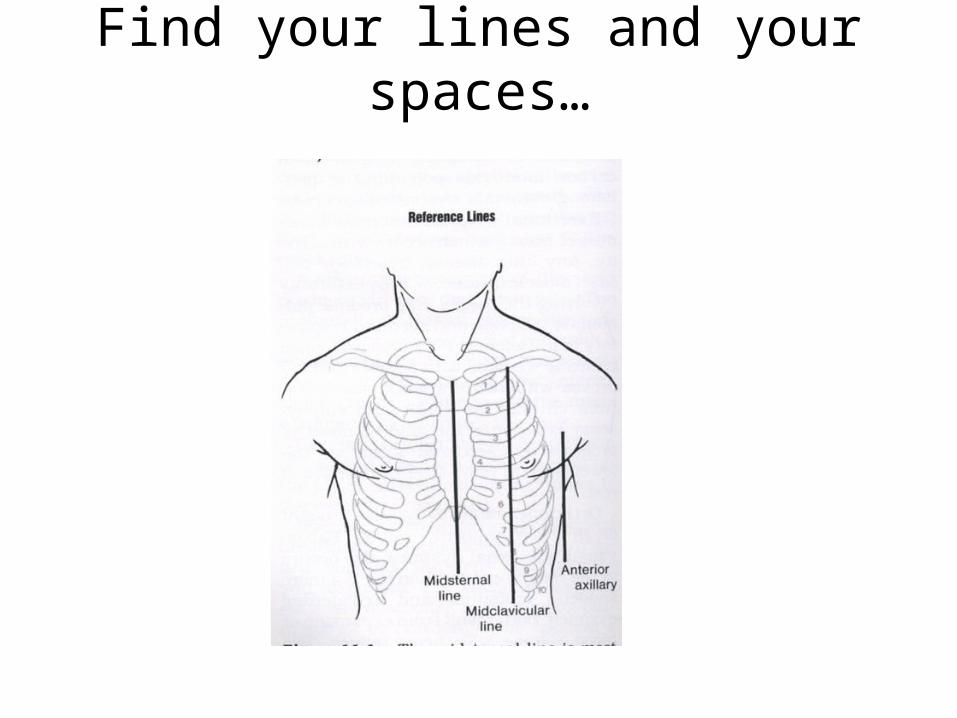
Find your lines and your spaces…
• Suprasternal notch• Clavicle (1st rib is under the clavicle)• 2nd rib, • 2nd ICS R and L• 4th ICS parasternal border• 5th ICS on L (apical area)• Epigastric area• BASE vs. APEX
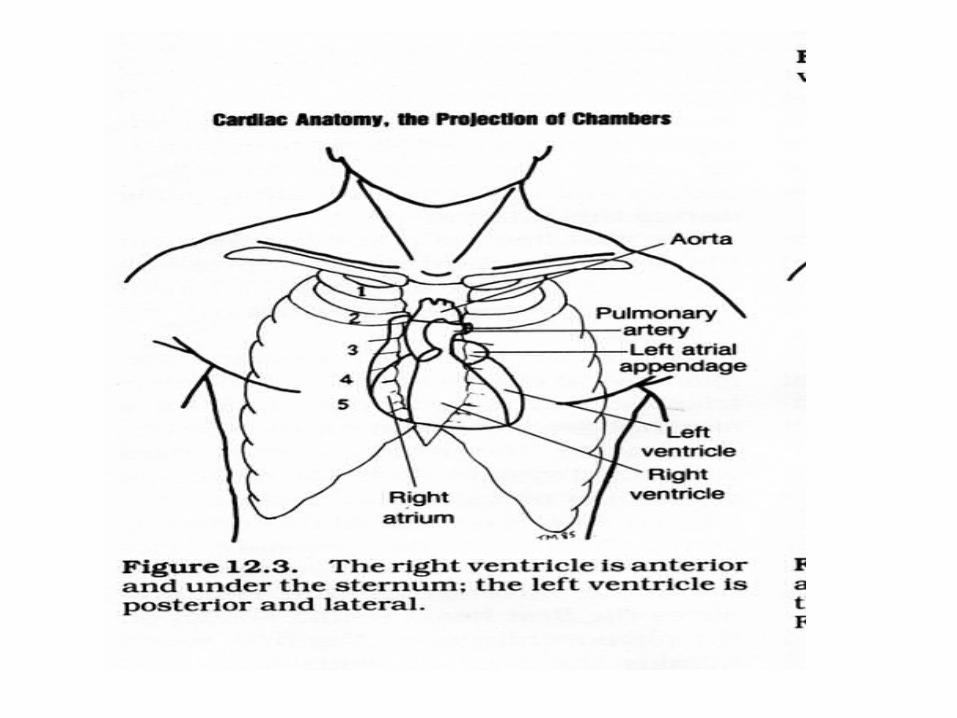
Cardiovascular exam --inspection
• Skin color, nailbeds, capillary refill (4-6 seconds is normal), ankle edema
• 5th L ICS @ MCL for apical impulse• Left 4th parasternal border for the R
ventricular area—R 4th for tricuspid• 2nd R ICS—aortic area• 2nd L ICS—pulmonic area• Suprasternal notch—pulsation?• Epigastric area—pulsation?
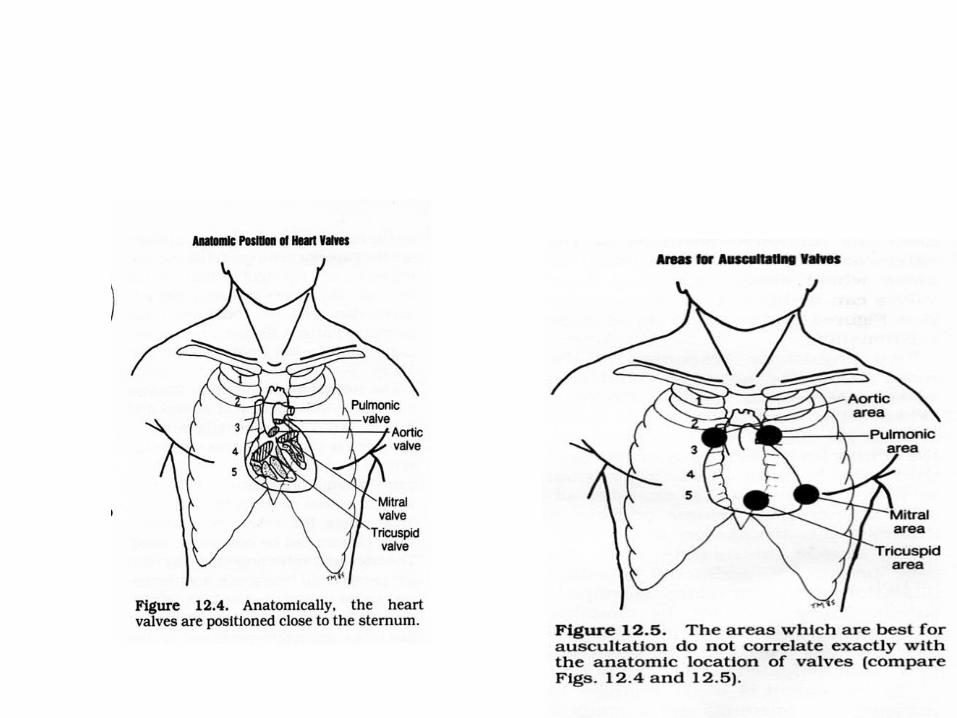
Palpation…
• The base of the heart…any thrills? Cat purring…• A thrill with a murmur means that the murmur is at
least a grade 4• Think valvular disease—aortic and pulmonic
stenosis in 2nd ICS• The 5th L ICS at the MCL The apical area—mitral stenosis
Palpation –palpating hearts and pulses since 1550 B.C. (Egyptians)
• Identify the apical impulse—should be no bigger than 1-2 cm in size; gentle, brief contraction (only present in 50% of the population—turn patient on L side to feel)—if >4 cm (LR 4.7 for a dilated heart)
• Where is it? Outside the MCL (>10 cm from the MSL)—LR for cardiomegaly is 3.4, depressed ejection fraction is 10.1, ↑LVEDV is 8.0, and increased PCWP 5.8)
• Is there a pulsation in the epigastric area? Beating up against the pads of your fingers? Beating against fingertips?
Palpation…
• Carotid pulses—carotid should be synchronous with the first heart sound (S1--lub)
• Peripheral pulses—dorsal pedalis, posterior tibial, popliteal, femoral, radial
• Radial = femoral• Abdominal aneurysms• PAD—males, diabetics, smokers, hypertensive patients
Characteristics arguing FOR the presence of peripheral vascular disease
• Absence of both pedal pulses (LR 14.9)*• Presence of any limb bruit (LR 7.3)• Presence of wounds or sores on the feet (LR 7.0)• Absence of the femoral pulse (LR 6.1)• Presence of asymmetric coolness of the foot (LR 6.1)• Unhelpful findings—atrophic skin (LR 1.7), hairless lower
limbs (LR 1.7), prolonged capillary refill time (LR 1.9)• McGee S. Evidence-Based Physical Diagnosis. WB Saunders, Co. 2001
• *LR is the Likelihood Ratio that this sign or symptom occurs with the disease or condition—the higher the LR, the greater the association
Jugular vein distention…
• The absolute best way to check the amount of volume and pressure on the right side of the heart
• Always check the R jugular vein in everyone but especially elderly pts
(direct route to heart; L veins cross the mediastinum where the aorta may compress and falsely elevate).
• If top of neck veins are elevated> 3 cm above sternal angle check for other signs of heart failure
• Hepatomegaly, peripheral edema, S3 gallop
Abdominal jugular reflex• The pressure applied over the abdomen shifts blood
into the thorax and right atrium• If the right ventricle is unable to handle this
increased load, the result is a sustained increase in JVP.
• Compression of the liver is unnecessary• Compression of the periumbilical area will suffice• Positive with a sustained increase in the JVP greater
than or equal to 4 cm.• LR ratio of 8 for detecting elevated left diastolic
pressures
Pitting edema…
• Subjective grading 1+-4+• 1+ slight pitting• 2+ deeper but no detectable distortion of
tissue• 3+ noticeably deep, extremity full and
edematous• 4+ very deep pit, dependent extremity is
grossly distorted
Peripheral edema…
• Unilateral pitting—consider occlusion of major vein
• Edema without pitting—arterial disease and occlusion
• Edema as a side effect of drugs that retain water or that are potent vasodilators—NSAIDS and Ca+ channel blockers
Now it’s time to listen--Notes on the stethoscope
• Ear plugs that fit—block out extraneous noise• Length of tubing no longer than 12”, but 8” is
ideal• Any stethoscope of a pastel color is worthless• Do not listen over clothes• The bell—LOW-pitched sounds; the diaphragm—
HIGH-pitched sounds• Quiet room—no TV; no visitors; no wives,
husbands, lovers, children; no construction
Find your lines and your spaces…
Position the patient…
• Sitting up and leaning forward—brings base of heart closer to chest wall
Murmurs of the aortic and pulmonic valves heard best in this position—high-pitched systolic sounds (aortic stenosis)
• Left lateral recumbent—best position to hear low-pitched filling sounds during diastole (mitral stenosis)
But if you only have a minute…
• …and the patient is NOT a cardiac patient—you can just listen to the apical or mitral area
• Use the bell to pick up any low-pitched murmurs
If you had two minutes and you know the following…
• #1 diseased valve of the heart? MITRAL• #2 diseased valve of the heart? AORTIC
• SO WHERE WOULD YOU LISTEN FOR EACH OF THE ABOVE?
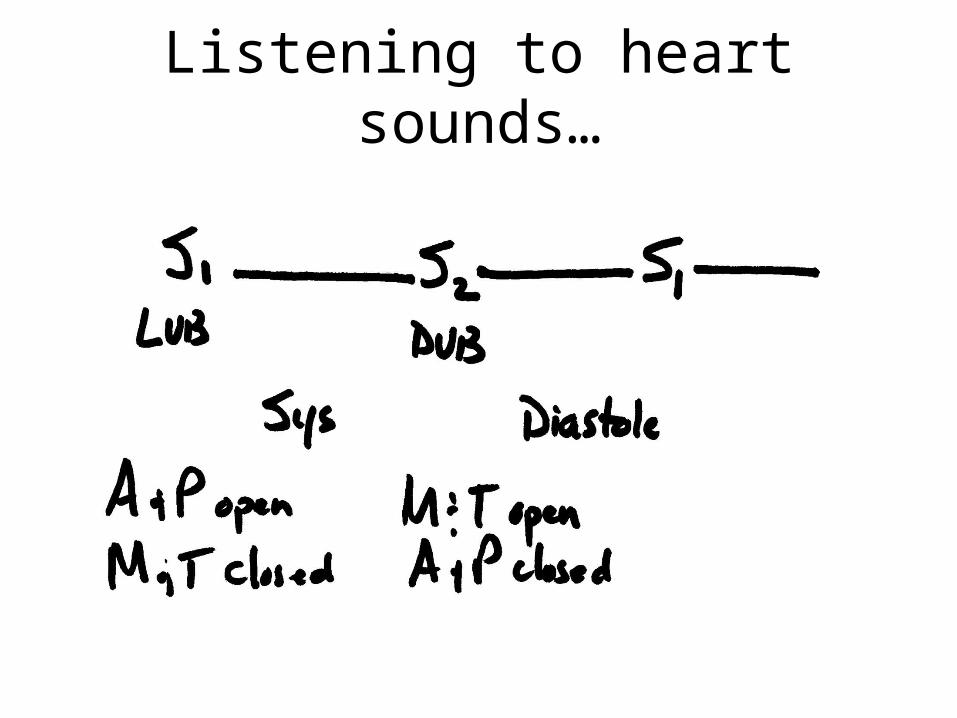
Heart sounds—S1, S2
• S1 is the closure of the mitral and tricuspid valves—the END of diastole or filling of the heart (aortic and pulmonic valves open signaling the beginning of systole)
• S2 is the closure of the aortic and pulmonic valves—the END of systole or ejecting the blood (mitral and tricuspid valves open signaling the beginning of diastole)
• Opening and closing valves are silent unless diseased
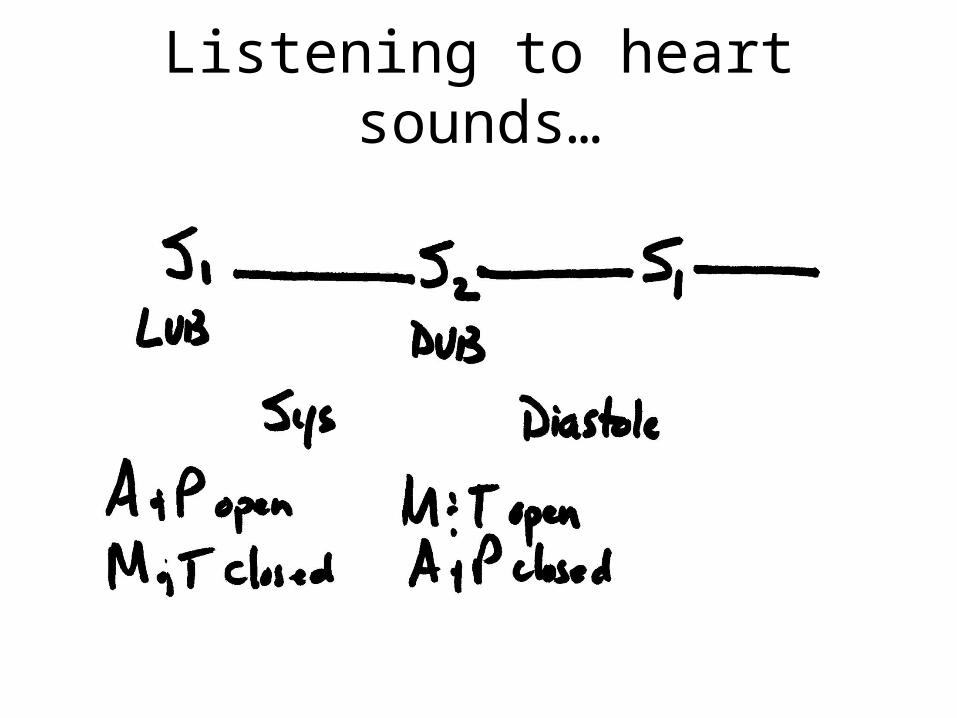
Listening to heart sounds…
So…when you hear an extra heart sound…
• First decide if it’s in systole or diastole?• Extra heart sounds can be murmurs…• 50% of all murmurs are systolic…therefore, 50% of all murmurs are diastolic. DUH…Is the murmur after the LUB? Systolic?Is the murmur after the DUB? Diastolic
Listening to heart sounds…
Characterizing a murmur…
• Timing—systole or diastole• Duration—early, mid, late, continuous in relation to
S1 and S2• Pitch—low, medium, high• Intensity—1 through 6 (4-6 usually assoc. with thrill)• Quality—descriptive (harsh, blowing, soft)• Location—where best heard• Radiation--where else is it heard
The common murmurs
• Mitral stenosis—low-pitch, mid-diastolic, apical rumble(with a healthy mitral valve you can slip three fingers through the valvular opening; with a stenotic valve it’s tough to even slip a pencil through the valvular opening)
• Mitral annular calcifications also cause an apical diastolic rumble—most common cause in elderly
• Aortic stenosis—early systolic ejection murmurREMEMBER: stenotic valves cause a murmur when the
valve is OPEN
The common murmurs
• Mitral regurgitation (insufficiency)—systolic murmur• Aortic regurgitation (insufficiency)—diastolic murmurREMEMBER: regurgitant valves cause a murmur when
the valve should be closed (mitral valve is CLOSED during systole or ejection; aortic valve is CLOSED during diastole or filling)
Functional or innocent murmurs…
• Functional or “innocent” murmurs..40-60% of all kids at some time; best heard with bell, grade I or II, no radiation, low to medium pitch, blowing, brief, 2nd L ICS parasternal border, lying down (may disappear when sitting or standing)
Causes of murmurs…
• Valvular disease• High output (increased speed or flow)—
severe anemia, thyrotoxicosis, pregnancy• Structural defects—congenital or acquired
Signs and symptoms of CHF?• Palpitations, skin color (pale, cyanotic), weak
pulses, dyspnea, nocturia, PND, orthopnea• “funny things happen in the middle of the night” • S3 gallop—early soft diastolic sound, best heard
over apex; use bell, lean patient forward; indicative of abnormal ventricular function in adults
• One-year mortality rate is higher for those with a displaced apical impulse (39% vs. 12%) or a 3rd heart sound (57% vs. 14%)
• S4? Forceful distention of noncompliant ventricles (hypertensive heart disease)
RESPIRATORY EXAM…
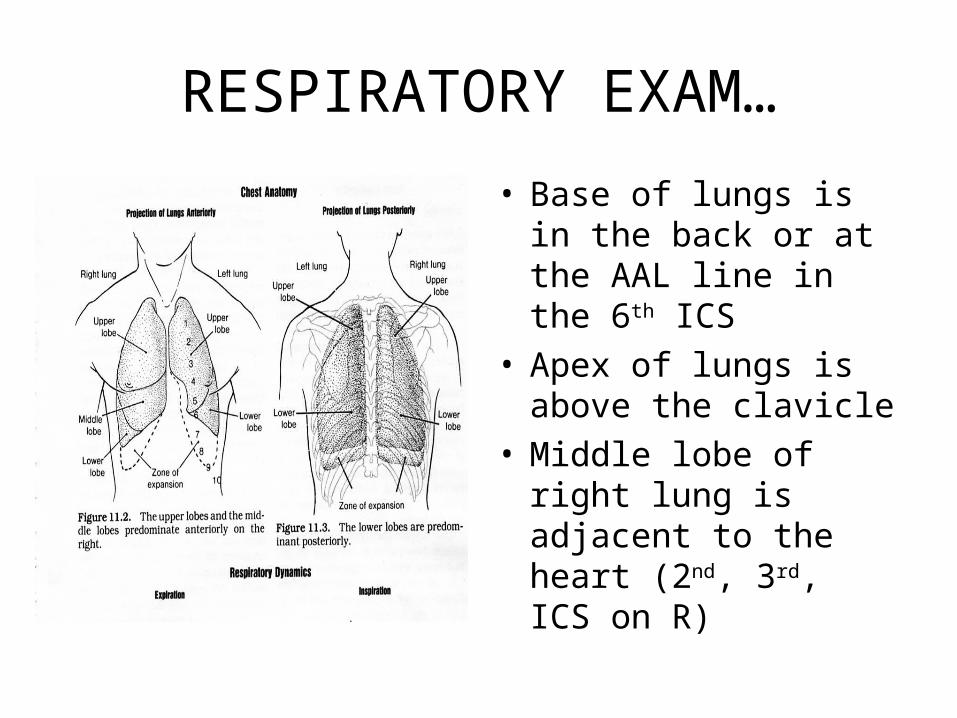
• Base of lungs is in the back or at the AAL line in the 6th ICS
• Apex of lungs is above the clavicle
• Middle lobe of right lung is adjacent to the heart (2nd, 3rd, ICS on R)
Thoracic disease—7 common symptoms signify thoracic disease
• Cough* (see next slide)• Sputum production• Hemoptysis—expectoration of blood or blood-
stained material• Chest pain—chest wall, pleura (“catch”)(sensitive to
sudden changes in pressure such as a spontaneous pneumothorax), heart, great vessels, trachea, and esophagus can all cause chest pain
Cough?
• Anywhere from the larynx to the distal bronchi…• Immediate coughing? Chemical irritation from
fumes, aspirated food or fluid can cause immediate coughing…
• The fluid from a cough can be mucus from inflammation (bronchitis—80% viral), pus from infection, or transudated plasma fluid from CHF; interstitial lung disease can also cause a cough
Thoracic disease—7 common symptoms signify thoracic disease
• Sputum production• Hemoptysis—expectoration of blood or blood-
stained material• Chest pain—chest wall, pleura (“catch”)(sensitive to
sudden changes in pressure such as a spontaneous pneumothorax), heart, great vessels, trachea, and esophagus can all cause chest pain
Thoracic disease—7 common symptoms signify thoracic disease
• Dyspnea—difficult or labored breathing; metabolic (acidosis*), hematologic (anemia), pulmonary (asthma, pneumonia, PE), cardiac (orthopnea, PND)
• Stridor— coarse “crowing” due to obstruction of the upper airway—emergency and may require immediate airway management
• Wheezing—high-pitched, whistling sound due to airway narrowing
Inspection
• AP diameter• Increased in COPD due to air trapping—
frequently assume a typical posture; they sit in a chair slightly inclined forward, with hands and elbows on their knees to help brace for maximum inspiratory effort
• Child with asthma
Palpation…
• Respiratory excursion• Tactile fremitus—”99” “99”, Mickey Mouse,
Mickey Mouse decreased fremitus—excess air in lungs increased fremitus—presence of solid mass
or fluids• Position of the trachea
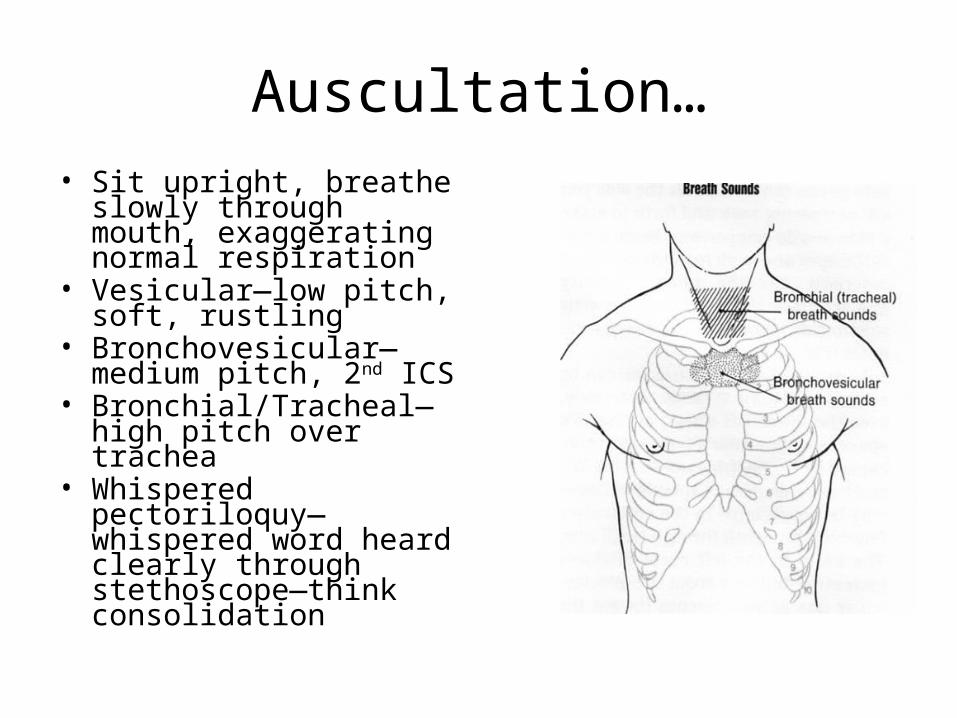
Auscultation…• Sit upright, breathe slowly
through mouth, exaggerating normal respiration
• Vesicular—low pitch, soft, rustling
• Bronchovesicular—medium pitch, 2nd ICS
• Bronchial/Tracheal—high pitch over trachea
• Whispered pectoriloquy—whispered word heard clearly through stethoscope—think consolidation
Ausculation for adventitious sounds…• Crackles (fine)-early or late inspiratory? Early—re-opening of closed alveoli (obstructive pulmonary
disease—chronic bronchitis, asthma, emphysema) Late—fluid at base of lungs (pneumonia, pulmonary
edema)** • **Late inspiratory basilar crackles are very common in the
very old patient—aging process, not disease (only heard with a few deep breaths—re-expanding alveoli in bed-ridden adults, elderly, persons just aroused from sleep)
• Crackles don’t clear with coughing
Adventitious sounds…
• Rhonchi in the bronchi—loud, snoring sounds, may clear with coughing;
• Bronchitis—heard throughout cycle, more prominent on expiration
• Wheezing—high-pitched whistle; edema of airways
The one-airway hypothesis
• Allergic rhinitis• Hay fever• Asthma• TREAT THE NOSE!
Apical TB
• Who’s at risk?• What are the cardinal symptoms of TB?• Where should you listen with your
stethoscope?• Sputum cytology for “red snappers”
Pulmonary embolism
• Early morning—7:30 is the most common time
• Risk factors for DVT—stasis, endothelial damage, hypercoagulation (Virchow’s triad)(Aging—1% rule)
• Ask about recent travel—especially long trips— “economy class syndrome”
The abdomen
• The pathophysiologic mechanisms producing symptoms and signs of abdominal diseases
• Pain• Dysfunction• GI bleeding• Systemic symptoms (anorexia, weight loss, fever)• Signs of organ decompensation• Hollow organ obstruction• Peritoneal irritation
GI and GU exam
• Divide the abdomen into 4 quadrants?
• RUQ—what’s in it?• LUQ—what’s in it?• RLQ—what’s in it?• LLQ—what’s in it?
Location, location, location• RUQ—LIVER, gallbladder, high
appendix, leaking peptic ulcer, pleurisy, second and third portion of the duodenum
• LUQ—stomach, duodenum (1st portion),aorta (ruptured aneurysm), pancreas, kidney, spleen, subdiaphragmatic processes
• RLQ– appendix, ovary, ileum, kidney, peritoneal inflammation
• LLQ—colon, pelvic processes, peritoneal inflammation from other areas
Inspection of the abdomen
• Venous engorgement • Peristalsis• Umbilicus• Scars• Petechiae, purpura• Spider angiomas• Skin color
Inspection of the distended abdomen
• The 6 F’s• Fluid (ascites, ileus)• Fat (fat is symmetrical)• Flatus (post prandial? No bowel sounds?)• Feces—yikes! Obstipation, constipation• Fetus—”I can’t believe I’m pregnant!• Fibroid (or other tumor)--asymmetrical
Auscultation of the abdomen
• Auscultate before palpating the abdomen• Listen for bowel sounds• Where should you listen?• Small bowel peristalsis with high pitched
frequent gurgle sounds vs. large bowel rumbles
• Listen for an abdominal bruit
The Acute Abdomen—quick checklist—who’s at risk?
• Acute cholecystitis• Acute appendicitis• Gall stones• Kidney stones• Ectopic pregnancy• Intestinal obstruction• Acute pancreatitis• Splenic rupture• Perforated peptic ulcer• Ruptured abdominal aneurysm• Above the diaphragm—MI, pneumonia
Palpation
• Light palpation• Deep palpation• Palpation for the liver at the right costal
margin—if you think you’re feeling the liver? You are…LR 233.4
• Palpation for the spleen at the left costal margin
• Murphy’s sign for cholecystitis. OUCH.• Midline structures
Evaluation of the patient with the acute abdomen
• General appearance and position of the patient
• Vital signs—assess quickly for signs of hypovolemic shock—pulse (supine tachycardia), BP (postural hypotension greater than 20 mm Hg decrease in systolic BP—if the patient can stand; or supine hypotension with systolic BP less than 95 mm Hg)
Evaluation
• While obtaining a history, palpate the abdomen; if it exhibits board-like rigidity with involuntary guarding, or you have palpated and/or observed a palpable, pulsating mass (just slightly to the left of the umbilicus), call your ever-so-friendly surgeon for immediate consultation
• A note about the abdominal exam in the elderly—may not have “board-like” rigidity even with a catastrophic event in the abdomen (muscle mass/rectus abdominis)
The appendix
• Acute appendicitis is at most a 5-day disease• Anorexia followed by periumbilical crampy pain,
occasional nausea and low-grade fever• Pain then migrates to the right iliac region and
becomes progressively more intense• CT scan is the usual method of diagnosis today
but if you don’t have one…• Rebound tenderness—hop off the bed, pop ‘em
on the bottom of the feet
The kidney…retroperitoneal space
• CVA tenderness• Acute pyelonephritis• Glomerulonephritis• Palpation? Polycystic kidney disease (PKD)
The ovaries
• The ovary should not be palpable in a postmenopausal women
• 14 grams to 5 grams• If palpable in a 62-year old women—refer!
The two-minute neuro exam
• Repeat after me…red ball, clock, tennis shoe (I will ask you those 3 items in a few minutes)
• Stand with feet together, arms out, palms up, eyes closed—check for swaying/unsteadiness, arm drifting (pronator drift)
---checks cerebellar function, subtle hemiparesis
• Push one arm down--proprioception
The two-minute neuro exam
• With eyes closed, ask patient to touch nose with outstretched hand—can the patient light on an object? any tremors
---checking cerebellar function• Ask patient to walk across room and back—
gait? Arm swing? Involuntary movements? Wide-based? Stiff-legged? (cerebellar, basal ganglia, corticospinal tract)
The two-minute neuro exam
• Sit on exam table and check DTRs• S1,2 (Achilles); L3,4 (patellar); C5,6 (Biceps),
C7,8 (Triceps)• Hyperreflexia? Hyporeflexia? Areflexia?• Check Babinski response (Adams HP, Corbette JJ, Dellyer WE. A quick neurologic
exam. Patient Care 2000 (Feb. 15), 161-74.
The Achille’s reflex
• 50% of the elderly population have lost their Achille’s reflex
• Symmetrical loss?• Unilateral loss with shooting pain down the
leg? Herniated disc at L-4,5
Reflex chart
The two-minute neuro exam—cranial nerves
• Clench teeth (CN V)--symmetry• Close eyes tightly—check for asymmetry, facial weakness---checks CN VII (facial nerve)• Open eyes and follow movement with finger—eyes eyes
track? ---checking CNIII, IV, VI, • Light reflex/follow finger to nose (CNII, III)• Optic fundus (CN II)• KKK, pant like dog (CNIX, X)• Shrug shoulders (Xi)• Stick tongue out (XII)
Argyl-Robertson pupil
• Prostitute’s pupil• It will accommodate, but not react
Unequal pupils
• Pupil chart—mm• Tape it to a tongue blade and you whip it out
of your pocket when necessary
The two-minute neuro exam—mental status
• The Time and Change test• Clock with hands• 3 Quarters, 7 dimes, and 7 nickels• What time is it?• Please make change in the amount of one dollar• Rules OUT dementia; 93% negative predictive value…• What were those three things I asked you to
remember?
Thank you.
• Barb Bancroft, RN, MSN, PNP• CPP Associates, Inc.• Chicago, IL • [email protected]• www.barbbancroft.com